Periodontal Diseases

Learning Outcomes
On completion of this chapter, the student will be able to achieve the following objectives:
1. Pronounce, define, and spell the Key Terms.
2. Discuss the periodontium, including:
• Name and describe the structures and tissues of the periodontium.
• Describe the prevalence of periodontal disease.
3. Identify systemic factors that may cause periodontal disease.
4. Discuss the causes and risk factors of periodontal disease.
5. Identify and describe the two basic types of periodontal disease and explain the significance of plaque and calculus in periodontal disease.
6. List the seven basic case types and signs and symptoms of periodontal disease.
Definition and Prevalence of Periodontal Disease
This chapter presents the scientific basis of periodontal disease. It includes:
• The relationship of periodontal disease and several systemic diseases
• The causes of periodontal disease
• Risk factors for periodontal disease
Chapter 55 (Periodontics) presents the role of the dental assistant in the clinical practice of periodontics, including the periodontal examination, charting, instruments, surgical and non-surgical techniques, and laser techniques.
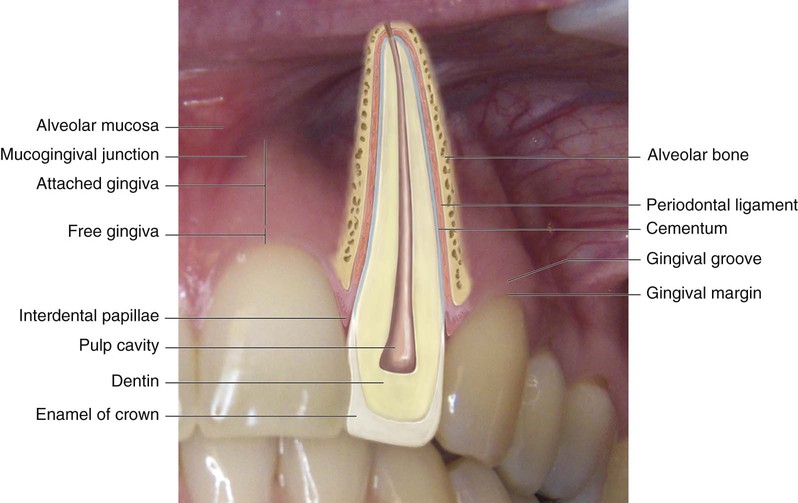
Periodontal disease is an infectious disease process that involves inflammation of the structures of the periodontium (Table 14-1). The periodontium is made up of structures that surround, support, and are attached to the teeth (Fig. 14-1). Periodontal disease causes a breakdown of the periodontium, resulting in loss of tissue attachment and destruction of alveolar bone.
TABLE 14-1
Structures of the Periodontium
| Name | Description |
| Gingivae | Commonly referred to as gums. This mucosa covers the alveolar process of the jaws and surrounds the necks of the teeth. |
| Epithelial attachment | Tissue at the base of the sulcus where the gingiva attaches to the tooth. |
| Sulcus | Space between the tooth and the free gingiva. |
| Periodontal ligaments | Dense connective fibers that connect the cementum covering the root of the tooth with the alveolar bone of the socket wall. |
| Cementum | Covers the root of the tooth. The primary function of the cementum is to anchor the tooth to the bony socket with attachments of the periodontal ligaments. |
| Alveolar bone | Bone that supports the tooth in its position within the jaw. The alveolar socket is the cavity in the bone that surrounds the tooth. |
From Robinson D, Bird D: Essentials of dental assisting, ed 4, St Louis, 2007, Saunders.
Periodontal diseases are the leading cause of tooth loss in adults. Almost 75 percent of American adults have some form of periodontal disease, and most are unaware of the condition. Almost all adults and many children have calculus on their teeth. Fortunately, with early detection and treatment of periodontal disease, most people can keep their teeth for life.
Periodontal Disease and Systemic Health
Periodontal science has proven a relationship with several systemic diseases, including coronary artery disease, diabetes, and stroke, as well as delivery of low-birth-weight infants. This relationship is not likely to affect everyone, but certainly affects many. In these patients, periodontal infection is thought to be a risk factor for systemic disease just as high cholesterol is a risk factor for coronary heart disease (Box 14-1). Chronic inflammation appears to do harm to the entire body.
Cardiovascular Disease
Individuals with periodontal disease have a greater incidence of coronary heart disease. This results in an increased occurrence of strokes and heart attacks. Individuals with severe periodontal disease have 3 times the risk for stroke and 3.6 times the risk for coronary heart disease when compared with individuals without periodontal disease. Studies show that oral bacteria can easily spread into the bloodstream, attach to fatty plaques in the coronary arteries, and contribute to clot formation and heart attacks.
Preterm/Low Birth Weight
Preterm birth is defined as birth that follows a pregnancy that is shorter than 37 weeks; low birth weight is defined as less than 5.5 pounds. Preterm birth and low birth weight are the two most significant predictors of the health and survival of an infant. Other risk factors such as smoking, alcohol use, and drug use also contribute to preterm low-birth-weight (PLBW) infants. Women with severe periodontal disease have 7 times the risk for PLBW babies compared with women with little or no periodontal disease. This association may be linked to particular biochemicals that are produced with periodontal disease, such as prostaglandin E2, which may create hormones that cause early uterine contraction and labor.
Respiratory Disease
Individuals with periodontal disease may be at increased risk for respiratory infection. It appears that bacteria that have colonized in the mouth may alter the respiratory epithelium, leaving it more susceptible to pneumonia. In addition, in patients who already have chronic bronchitis, emphysema, or chronic obstructive pulmonary disease, existing conditions may be aggravated by inhalation of bacteria from the mouth into the lungs. These bacteria multiply in the respiratory tract and cause infection.
Causes of Periodontal Disease
Dental Plaque
Plaque is a soft mass of bacterial deposits that covers tooth surfaces. When the plaque layer is thin, it is not visible, but it stains pink when a disclosing agent (erythrosine stain) is applied (staining plaque is discussed further in Chapter 15). If it is not removed, plaque will continue to build up and will appear as a sticky white material (Fig. 14-2).

Although plaque is the primary factor causing periodontal disease, type of bacteria, length of time bacteria are left undisturbed on the teeth, and patient response to bacteria are all critical factors in the risk for periodontal disease. Plaque cannot be removed simply by rinsing the mouth. Bacteria in dental plaque cause inflammation by producing enzymes and toxins that destroy periodontal tissues and lower host defenses.
Calculus
Calcium and phosphate salts in the saliva form calculus, which is commonly called “tartar.” Calculus is a hard, stonelike material that attaches to the tooth surface. The surface of calculus is porous and rough and provides an excellent surface on which additional plaque can grow. Calculus can penetrate into the cementum on root surfaces. It cannot be removed by the patient and must be removed by the dentist or the dental hygienist with the use of scaling instruments. Regular, effective plaque control measures can minimize or eliminate the buildup of calculus. Plaque control measures are discussed in Chapter 15.
Calculus is usually divided into supragingival and subgingival types, even though these types often occur together.
Supragingival Calculus
Supragingival calculus is found on the clinical crowns of the teeth, above the margin of the gingiva. It is readily visible as a yellowish-white deposit that may darken over time (Fig. 14-3).

Supragingival calculus occurs frequently near the openings of Wharton's ducts (on the lingual surfaces of the lower anterior teeth) and Stensen's ducts (on the buccal surfaces of the maxillary molars).
Subgingival Calculus
Subgingival calculus forms on root surfaces below the gingival margin and can extend into the periodontal pockets. It can be dark green or black. The color is caused by stain that results from subgingival bleeding.
Unlike supragingival calculus, the location of subgingival calculus is not site specific. It is found throughout the mouth. Subgingival calculus provides a reservoir for bacteria and endotoxins. Subgingival calculus covered by plaque can cause greater disease than can be produced by plaque alone.
Other Risk Factors
A vast majority of periodontal diseases begin as inflammation caused by an accumulation of bacterial plaque. However, periodontal diseases may be triggered by other factors such as malocclusion, some medications (such as those used for control of blood pressure), and serious nutritional deficiencies.
Disease-causing bacteria are necessary for periodontal disease to occur, but they are not totally responsible for destruction of the periodontium. Other risk factors alter the body's response to bacteria that are present in the mouth. Risk factors involved will determine the onset, degree, and severity of periodontal disease. This is why there is a great deal of variability in the susceptibility of individuals to periodontal disease and in successful outcomes of treatment.
Periodontal disease results from the complex interaction of bacterial infection and risk factors. As the number of risk factors increases, the patient's susceptibility to periodontal disease also increases (Table 14-2).
TABLE 14-2
Common Risk Factors for Periodontal Disease
| Risk Factor | Rationale |
| Smoking | Smokers have greater loss of attachment, bone loss, periodontal pocket depths, calculus formation, and tooth loss. Periodontal treatments are less effective in smokers than in nonsmokers. |
| Diabetes mellitus | Diabetes is a strong risk factor for periodontal disease. Individuals with diabetes are 3 times more likely to have attachment and bone loss. Persons who have their diabetes under control have less attachment and bone loss than do those with poor control. |
| Poor oral hygiene | Lack of good oral hygiene increases the risk of periodontal disease in all age groups. Excellent oral hygiene greatly reduces the risk of severe periodontal disease. |
| Osteoporosis | An association has been reported between alveolar bone loss and osteoporosis. Women with osteoporosis have increased alveolar bone resorption, attachment loss, and tooth loss compared with women without osteoporosis. Estrogen deficiency also has been linked to decreases in alveolar bone. |
| HIV/AIDS | Increased gingival inflammation is noted around the margins of all teeth. Often, patients with HIV/AIDS develop necrotizing ulcerative periodontitis (NUP). |
| Stress | Psychological stress is associated with depression of the immune system, and studies show a link between stress and periodontal attachment loss. Research is ongoing to identify the link between psychological stress and periodontal disease. |
| Medications | Some medications, such as tetracycline and nonsteroidal anti-inflammatory drugs (NSAIDs), have a beneficial effect on the periodontium, and others have a negative effect. Decreased salivary flow (xerostomia) can be caused by more than 400 medications, including diuretics, antihistamines, antipsychotics, antihypertensive agents, and analgesics. Antiseizure drugs and hormones such as estrogen and progesterone can cause gingival enlargement. |
| Local factors | Overhanging restorations, subgingival placement of crown margins, orthodontic appliances, and removable partial dentures also may contribute to the progression of periodontal disease. |
Types of Periodontal Disease
The term periodontal disease includes both gingivitis and periodontitis, and these two basic forms of periodontal disease each has a variety of forms. It is important for the dental assistant to have a clear understanding of the characteristics of the healthy periodontium, which will serve as a foundation from which signs of disease can be identified. You may wish to review the appearance of healthy oral tissues as presented in Chapter 10.
Gingivitis
Gingivitis is inflammation of the gingival tissue. It may be the most common human disease and is one of the easiest to treat and control. Areas of redness and swelling characterize gingivitis, and the gingiva tends to bleed easily. In addition, there may be changes in gingival contour and loss of tissue adaptation to the teeth (Table 14-3).
TABLE 14-3
Clinical Gingival Characteristics in Health and Disease
| Characteristic | Health | Disease |
| Color | Uniformly pale pink with or without generalized dark brown pigmentation | Bright red Dark red, blue-red Pink if fibrotic |
| Consistency | Firm, resilient | Soft, spongy, dents easily when pressed with probe Bleeds readily to probing |
| Surface texture | Free gingival—smooth Attached—stippled | Loss of stippling, shiny Fibrotic with stippling Nodular Hyperkeratotic |
| Contour | Gingival margin is 1–2 mm above CEJ in fully erupted teeth. Marginal gingiva is knife-edge, flat; follows a curved line around the tooth and fits snugly around the tooth Papilla is pointed and pyramidal; fills interproximal spaces | Irregular margins from edema, fibrosis, clefting, and/or festooning. May be rounded, rolled, or bulbous; therefore more coronal to CEJ. May show recessions so that the anatomical root is exposed Bulbous, flattened, blunted, cratered |
| Size | Free marginal gingiva is near CEJ and adheres closely to the tooth | Enlarged from excess fluid in tissues or fibrotic from the formation of excess collagen fibers. Free marginal gingiva may be highly retractable with air |
| Probing depth | 0–4 mm; no apical migration of JE | More than 4 mm with or without apical migration of JE |
CEJ, Cementoenamel junction; JE, junctional epithelium.
From Darby ML, Walsh MM: Dental hygiene: theory and practice, ed 3, St Louis, 2010, Saunders.
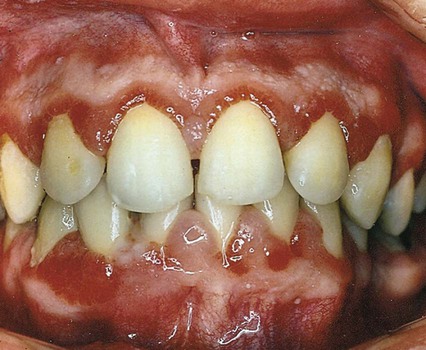
Gingivitis is found only in the epithelium and in gingival connective tissues. No tissue recession or loss of connective tissue or bone is associated with gingivitis (Fig. 14-4). Other types of gingivitis are associated with puberty, pregnancy, and the use of birth control medications (Box 14-2 and Fig. 14-5). Orthodontic appliances tend to retain bacterial plaque and food debris, resulting in gingivitis (Fig. 14-6). Instruction regarding proper home care is a critical part of orthodontic treatment (see Chapter 60).


Gingivitis is painless and often remains unrecognized until a dental professional emphasizes its importance. Improved daily oral hygiene practices may reverse gingivitis.
 1
1 Periodontitis
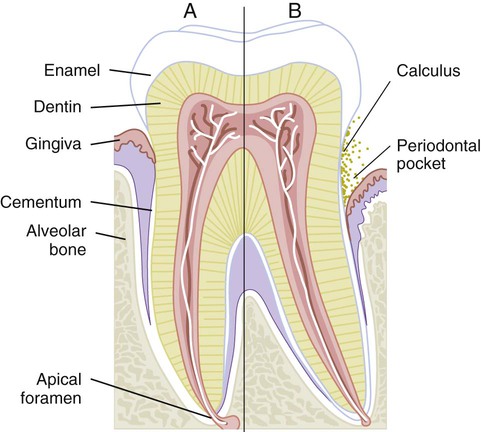
Periodontitis is inflammation of the supporting tissues of the teeth. The inflammatory process progresses from the gingiva into the connective tissue and alveolar bone that support the teeth (Fig. 14-7). The connective tissue attachment at the base of a periodontal pocket is destroyed as the disease progresses.
At one time, it was believed that periodontitis progressed slowly and at a constant rate. All individuals were thought to be equally susceptible to periodontitis. This is no longer true. The current view of periodontitis is that the disease can take several forms, all of which are infections caused by groups of microorganisms living in the oral cavity. All forms of periodontal disease appear to be related to changes in the many types of bacteria found in the oral cavity.
Description of Periodontal Disease
Periodontal disease is described in terms of disease severity and how much of the mouth is affected:
• If less than 30% of sites in the mouth are affected, the disease is considered localized
• If more than 30% of sites in the mouth are affected, the disease is considered generalized (Fig. 14-8)

The severity of the disease is determined by assessment of the amount of lost attachment, as follows:
On the basis of disease severity and the amount of tissue destruction that has occurred by the time of examination (Box 14-3), the American Academy of Periodontology has identified seven basic case types of periodontal disease.
▪ Eye to the Future
Traditionally, nonsurgical examination of the sulcus has been limited to the use of explorers and radiographs. Perioscopy is a new procedure in which a miniature dental endoscope is used, along with video, lighting, and magnification technology. It enables the operator to look into a deep subgingival pocket to explore the gingival sulcus and to determine the precise location of root deposits, granulation tissue, caries, and root fractures. The goal of periodontal therapy is to get the root surfaces as clean as possible so that tissues can heal; now, with the use of the perioscope, the operator can actually see any remaining calculus that might have been missed. In addition, the perioscope enables the operator and the patient to look at defects (magnified up to 46 times) on the enamel and cementum and identify initial decay and/or cracks that were previously camouflaged.
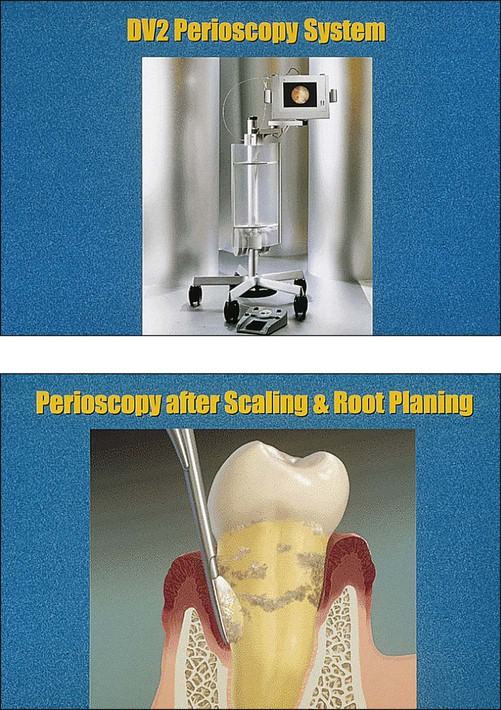
A miniature camera is attached to a tiny probe and then is gently placed into the sulcus. Images are immediately displayed on a chairside video screen for the operator and patient to see.
To maintain sterility, a disposable sterile sheath is placed around the perioscope before each patient use. There is very little discomfort during the procedure, and often, the patient does not require the use of local anesthesia. This device may one day become a new standard of care in the diagnosis and treatment of patients with periodontal disease worldwide. ▪
Pageburst Integrated Resources
As part of your Pageburst Digital Book, you can access the following Integrated Resources:
