Croup Syndrome
Laryngotracheobronchitis and Acute Epiglottitis
Chapter Objectives
After reading this chapter, you will be able to:
• List the anatomic alterations of the lungs associated with inspiratory stridor (croup) syndrome.
• Describe the causes of inspiratory stridor (croup) syndrome.
• List the cardiopulmonary clinical manifestations associated with inspiratory stridor (croup) syndrome.
• Describe the general management of inspiratory stridor (croup) syndrome.
• Describe the clinical strategies and rationales of the SOAPs presented in the case studies.
Key Terms
Introduction
The word croup is a general term used to describe the inspiratory, barking or brassy sound associated with a partial upper airway obstruction. In other words, croup is actually a clinical sign (objective data) or a clinical manifestation—that is, the “barking or brassy sound” associated with a partial upper airway obstruction. Clinically, the inspiratory barking sound heard in a patient with a partial upper airway obstruction is called inspiratory stridor.
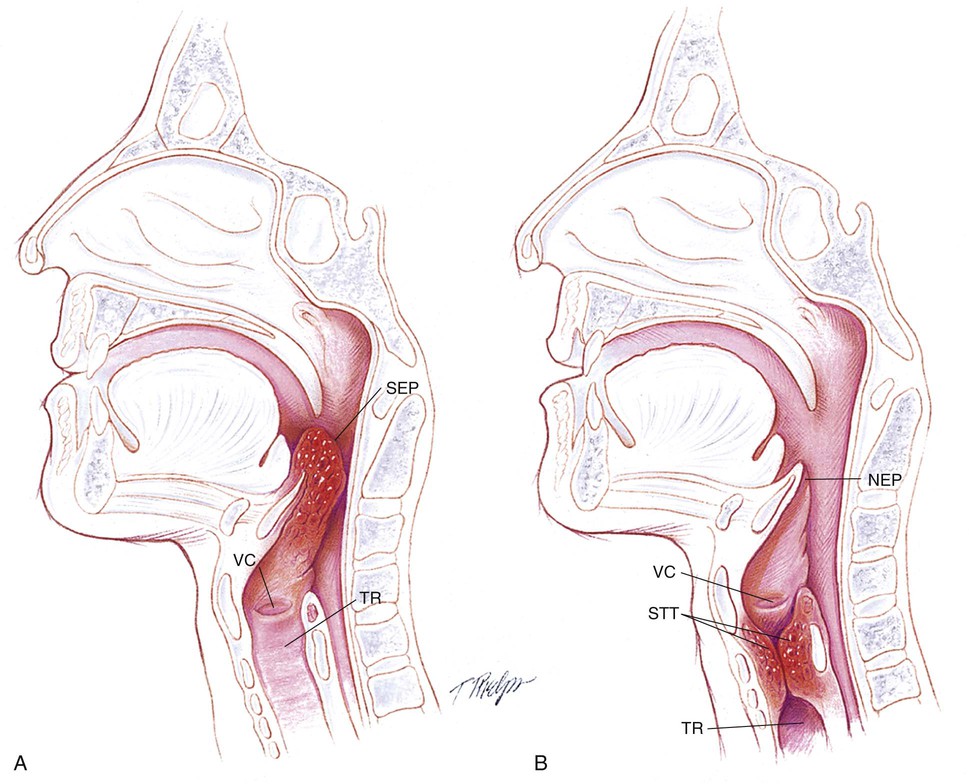
Most experts use the term croup and laryngotracheobronchitis (LTB)—which is a subglottic airway obstruction—interchangeably. Acute epiglottitis—which is a supraglottic airway obstruction—is regarded as an entirely separate disease entity (Figure 41-1). Historically, this is probably a result, in part, of the fact that the inspiratory stridor (i.e., the croup sound) associated with a patient with LTB is usually a loud and high-pitched brassy sound, whereas the inspiratory stridor associated with a patient with acute epiglottis is often lower in pitch, muffled, or even absent.
In addition, some sources refer to LTB as a subglottic croup and to acute epiglottitis as a supraglottic croup. In essence, these phrases (subglottic croup versus supraglottic croup) simply mean that the inspiratory stridor sound originates from either the subglottic area (i.e., in LTB) or the supraglottic area (i.e., in acute epiglottitis).
Thus, in view of the confusing nature of the term croup and the two types of partial upper airway disorders—LTB and acute epiglottis—for clarity, the phrase inspiratory stridor will always be used in place of the term croup throughout this chapter.
Anatomic Alterations of the Upper Airway
Laryngotracheobronchitis
Because laryngotracheobronchitis can affect the lower laryngeal area, trachea, and occasionally the bronchi, the term laryngotracheobronchitis is used as a synonym for “classic” subglottic obstruction (see Figure 41-1, B). Pathologically, LTB is an inflammatory process that causes edema and swelling of the mucous membranes. Although the laryngeal mucosa and submucosa are vascular, the distribution of the lymphatic capillaries is uneven or absent in this region. Consequently, when edema develops in the upper airway, fluid spreads and accumulates quickly throughout the connective tissues, which causes the mucosa to swell and the airway lumen to narrow. The inflammation also causes the mucous glands to increase their production of mucus and the cilia to lose their effectiveness as a mucociliary transport mechanism.
Because the subglottic area is the narrowest region of the larynx in an infant or small child, even a slight degree of edema can cause a significant reduction in cross-sectional area of the airway. The edema in this area is further aggravated by the rigid cricoid cartilage, which surrounds the subglottic trachea and prevents external swelling as fluid engorges the laryngeal tissues. The edema and swelling in the subglottic region decrease the ability of the vocal cords to abduct (move apart) during inspiration. This further reduces the cross-sectional area of airway in this region.
Acute Epiglottitis
Acute epiglottitis is a life-threatening emergency. In contrast to LTB, epiglottitis is an inflammation of the supraglottic region, which includes the epiglottis, aryepiglottic folds, and false vocal cords (see Figure 41-1, A). Epiglottitis does not involve the pharynx, trachea, or other subglottic structures. As the edema in the epiglottis increases, the lateral borders curl and the tip of the epiglottis protrudes posteriorly and inferiorly. During inspiration the swollen epiglottis is pulled (or sucked) over the laryngeal inlet. In severe cases, this may completely block the laryngeal opening. Clinically, the classic finding is a swollen, cherry-red epiglottis, severe respiratory distress and drooling.
The major pathologic or structural changes associated with inspiratory stridor are as follows:
Etiology and Epidemiology
Laryngotracheobronchitis
The parainfluenza viruses cause most cases of LTB, with type 1 being the most common, type 3 less common, and type 2 infrequent. LTB also may be caused by influenza A and B, respiratory syncytial virus (RSV), herpes simplex virus, Mycoplasma pneumoniae, rhinovirus, and adenoviruses. LTB is primarily seen in children 6 months to 5 years of age, with peak prevalence in the second year of life. Boys are affected slightly more often than girls. The onset of LTB is slow (i.e., symptoms progressively increase over 24 to 48 hours), and it is most common during the fall and winter. A brassy or barking cough is commonly present. The child's voice is hoarse, and the inspiratory stridor is typically loud and high in pitch. The patient usually does not have a fever, drooling, swallowing difficulties, or a toxic appearance.
Acute Epiglottitis*
Acute epiglottitis is a bacterial infection that is almost always caused by Haemophilus influenzae type B. It is transmitted via aerosol droplets. Since 1985, when vaccinations with H. influenzae type B vaccine became widespread, the number of reported cases of epiglottitis has decreased by over 95%. H. influenzae type B, however, is still responsible for 75% of the epiglottitis cases. Other causes of epiglottitis include aspiration of hot liquid and trauma from repeated intubation attempts.
Epiglottitis has no clear-cut geographic or seasonal incidence. Although acute epiglottitis may develop in all age groups (neonatal to adulthood), it most often occurs in children 2 to 6 years of age. Boys are affected more often than girls. The onset of epiglottitis is usually abrupt. Although the initial clinical manifestations are usually mild, they progress rapidly over a 2- to 4-hour period. A common scenario includes a sore throat or mild upper respiratory problems that quickly progresses to a high fever, lethargy, and difficulty in swallowing and handling secretions. The child usually appears pale and septic. As the supraglottic area becomes swollen, breathing becomes noisy, the tongue is often thrust forward during inspiration, and the child may drool. Compared with LTB, the inspiratory stridor is usually softer and lower in pitch. A cough is usually absent with acute epiglottitis. The voice and cry are usually muffled rather than hoarse. Older children commonly complain of a sore throat during swallowing. Acute epiglottitis in adults is typically seen in patients with neck trauma (e.g., blunt force neck injury or aspiration of hot liquid), in those who have been intubated repeatedly, and in drug abuse (crack cocaine) cases.
The general history and physical findings of LTB and epiglottitis are compared and contrasted in Table 41-1.
TABLE 41-1
General History and Physical Findings of Laryngotracheobronchitis (LTB) and Epiglottitis
| LTB | Epiglottitis | |
| Age | 6 months–5 years (with the peak prevalence in the second year) | 2–6 years |
| Onset | Usually slow or gradual (24–48 hours) | Abrupt (2–4 hours) |
| Fever | Absent | Present |
| Drooling | Absent | Present |
| Radiograph findings | Haziness in subglottic area,“pencil point” or “steeple point” | Haziness in supraglottic area, “thumb sign” |
| Inspiratory stridor | High-pitched, brassy, loud sound | Low-pitched and muffled, or absent |
| Cough | Present (barking or brassy cough) | Absent |
| Hoarseness | Present | Absent |
| Swallowing difficulty | Absent | Present |
| White blood count | Normal (viral—parainfluenza viruses 1, 2, and 3; influenza A and B; respiratory syncytial virus) | Elevated (bacterial—Haemophilus influenza type B) |
Overview of the Cardiopulmonary Clinical Manifestations Associated with Laryngotracheobronchitis and Epiglottitis
The following clinical manifestations result from the pathologic mechanisms caused (or activated) by an Upper Airway Obstruction—the major anatomic alteration of the lungs associated with laryngotracheobronchitis (LTB) and epiglottitis (see Figure 41-1). It should also be noted that an “upper airway” obstruction is not one of the major clinical scenarios discussed in Chapter 9.
Clinical Data Obtained at the Patient's Bedside
The Physical Examination
Increased Respiratory Rate (Tachypnea)
Several pathophysiologic mechanisms operating simultaneously may lead to an increased ventilatory rate:
• Increased stimulation of peripheral chemoreceptors
• Increased temperature (seconday to infection)
Increased Heart Rate (Pulse) and Blood Pressure
Inspiratory Stridor
Under normal circumstances the slight narrowing of the upper (extrathoracic) airway that naturally occurs during inspiration is insignificant. Because the upper airway is relatively small in infants and children, however, even a slight degree of edema may become significant, particularly at the level of the cricoid cartilage. Thus when the cross-section of the upper airway is reduced because of the edema, the child will generate stridor during inspiration, when the upper airway naturally becomes smaller. It also should be noted that if the edema becomes severe, the patient may generate both inspiratory and expiratory stridor.
Cyanosis
Intermittent coughing spells may produce intermittent cyanosis as secretions obstruct an already limited airway.









Anterio-Posterior Neck Radiograph
• “Steeple point” or “pencil point” narrowing of the upper airway (LTB)
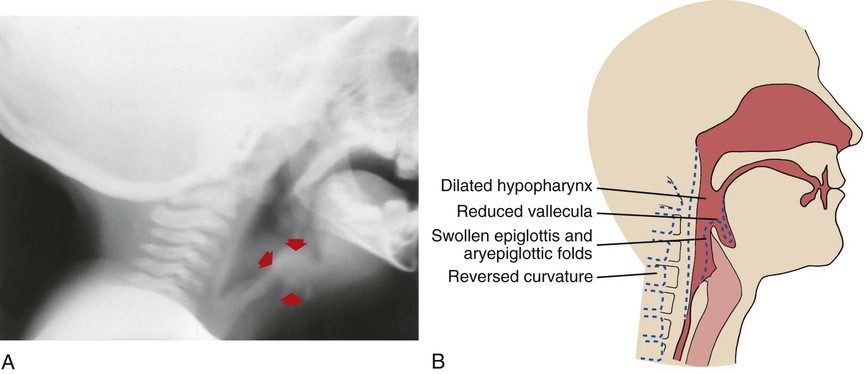
Although the diagnosis of epiglottitis or LTB can generally be made on the basis of the patient's clinical history, radiologic examinations are helpful. A lateral neck radiograph is usually done first to rule out the diagnosis of epiglottitis. Once this film is read as negative, an AP neck is ordered to define the degree of subglottic edema. When the patient has acute epiglottitis, a white haziness is evident in the supraglottic area. In addition, the epiglottitis often appears on a lateral neck radiograph as the classic “thumb sign.” The epiglottis is swollen and rounded, giving it an appearance of the distal portion of a thumb (see Figure 41-2). Figure 41-3 shows an infant with new onset leukemia and epiglottitis.

When the patient has LTB, a white haziness is demonstrated in the subglottic area; the AP neck will show the classic “pencil point” or “steeple point” narrowing at the level of the cricoid cartilage (see Figure 41-4). It is also important to mention that a barky cough associated with partial airway obstruction can be caused by a foreign object in the airway—a not-so-infrequent cause in toddlers. Generally, the lateral and AP neck are helpful screens to suggest laryngoscopy in these cases.

General Management of Laryngotracheobronchitis and Epiglottitis*
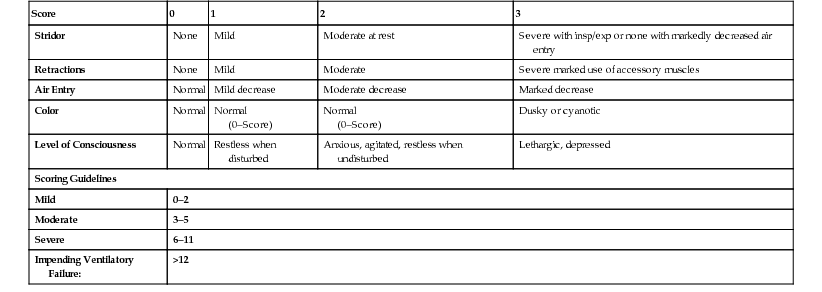
There are a number of excellent LTB scoring systems available that allow the respiratory therapist to objectively assess and treat the patient. The typical LTB score table measures the patient's stridor, retractions, air movement, color and level of consciousness (Table 41-2).
TABLE 41-2
LTB Scoring System
| Score | 0 | 1 | 2 | 3 |
| Stridor | None | Mild | Moderate at rest | Severe with insp/exp or none with markedly decreased air entry |
| Retractions | None | Mild | Moderate | Severe marked use of accessory muscles |
| Air Entry | Normal | Mild decrease | Moderate decrease | Marked decrease |
| Color | Normal | Normal (0–Score) | Normal (0–Score) | Dusky or cyanotic |
| Level of Consciousness | Normal | Restless when disturbed | Anxious, agitated, restless when undisturbed | Lethargic, depressed |
| Scoring Guidelines | ||||
| Mild | 0–2 | |||
| Moderate | 3–5 | |||
| Severe | 6–11 | |||
| Impending Ventilatory Failure: | >12 | |||
Early recognition of epiglottitis may save a patient's life; it is a true airway emergency. Once the diagnosis is suspected or confirmed by the lateral neck radiograph, examination or inspection of the pharynx and larynx is only to be done in the operating room under general anesthesia with a fully trained team. Under no circumstances should the mouth or throat be examined outside the operating room (even though depression of the tongue may reveal a bright red epiglottis and confirm the diagnosis) unless personnel and equipment are available to rapidly intubate or tracheostomize the patient. The patient usually maintains their limited airway by sitting up and leaning forward with their chin protruding—laying the patient down for examination will cause complete airway obstruction within minutes. The patient with a confirmed diagnosis of acute epiglottitis should be intubated immediately!
After the diagnosis is established, the general management of LTB and acute epiglottitis is as follows:
Supplemental Oxygen
Because hypoxemia and significant work of breathing is associated with both LTB and epiglottitis, supplemental oxygen may be required. Oxygen therapy should be started when the patient's SpO2 is under 92% (see Oxygen Therapy Protocol, Protocol 32-1).
Racemic Epinephrine
Aerosolized racemic epinephrine is administered to children with LTB based on the LTB Scoring System (see Table 41-2). Using the patient’s LTB score, the administration of racemic epinephrine protocol is as follows:
• 3–5: Consider racemic epinephrine
• >6: Administer racemic epinephrine 0.5 mL in 3 mL normal saline
This adrenergic agent is used for its vasoconstriction effect on mucosal edema and is recognized as an effective and safe aerosol decongestant for in-hospital use (see Aerosolized Medication Protocol, Protocol 32-4).
Corticosteroids
Corticosteroids, such as dexamethasone, have been shown to reduce the severity and duration of LTB, and are generally given when the patient presents with moderate to severe symptoms (see Appendix II).
Antibiotic Therapy
Because acute epiglottitis is almost always caused by H. influenzae type B, appropriate antibiotic therapy is part of the treatment plan. Ceftriaxone (Rocephin) and Ampicillin/sulbactam (Unasyn) often are prescribed to cover the most common organisms that cause acute epiglottitis.
Endotracheal Intubation or Tracheostomy
In the patient with a suspected acute epiglottitis, the examination or inspection of the pharyngeal and laryngeal areas is only to be performed in the operating room with a trained surgical team in attendance. This is because the epiglottis may obstruct completely in response to even the slightest touch or supine positioning during inspection. The physician, nurse, and respiratory therapist should not leave the patient's bedside until the endotracheal tube is secured. If the patient is anxious, restless, or uncooperative, restraints and sedation may be needed to prevent accidental extubation. After intubation, the patient should be transferred to the intensive care unit (ICU) and placed on continuous positive airway pressure (CPAP) or pressure support ventilation. Mechanical ventilation must be provided if paralysis is used to protect the airway in an uncooperative patient (see Mechanical Ventilation and Weaning Protocol, Protocol 32-5).
Case Study 1 Laryngotracheobronchitis
Admitting History and Physical Examination
An 18-month-old boy had a mild viral upper respiratory infection and some hoarseness. At 10 PM on the third day of his illness, he rapidly developed a brassy cough and high-pitched inspiratory stridor. He became moderately dyspneic. The child was restless and appeared frightened. Rectal temperature was 37° C. The mother claimed that the child was “blue” on two occasions during a coughing episode. She was going to take the child to the emergency room, but the grandmother suggested that she try steam inhalation first. Accordingly, the child was taken to the bathroom, where the hot shower was turned on full force. The child was comforted by the grandmother and urged to breathe slowly and deeply. As the bathroom became filled with steam, the respiratory distress abated and within a few minutes the child was free of stridor, breathing essentially normally. The next day the same symptoms recurred, and the patient was taken to the emergency department.
Cough and inspiratory stridor were noted. Vital signs were: blood pressure 90/60, pulse 160 beats/min, respiratory rate 32 breaths/min. The room air SpO2 was 94%. The patient's inspiratory stridor (croup) score was 7. The AP neck radiograph showed narrowing of the subglottic airway. The respiratory therapist documented the following assessment and plan.
Respiratory Assessment and Plan
S Mother reports patient had cough and inspiratory stridor.
O Confirms above. Lungs clear except for stridor and tracheal breath sounds throughout. Vital signs: BP: 90/60, P: 160/min, RR 32/min. Pallor noted. SpO2 94% on room air. Inspiratory stridor (croup) score of 7. Soft tissue radiograph of neck suggests laryngotracheobronchitis.
A LTB, moderate (history and inspiratory stridor).
P Notify the physician. Start Aerosolized Medication Protocol (med. neb. treatment with racemic epinephrine per protocol).
Discussion
Home remedies sometimes do work. Any parent who has had a child with LTB will find this scenario familiar. What may not be as widely recognized is that sometimes inhalation of warm or cool mist may improve this syndrome. When this approach failed, the parents were wise to bring their son to the emergency department for prompt vasoconstrictive therapy and oral steroids. This resulted in prompt improvement.
Case Study 2 Acute Epiglottitis
Admitting History and Physical Examination
A 2-year-old girl whose parents had an objection to routine infant and childhood immunizations appeared quite well in the evening and was put to bed at the usual time. She woke up 2 hours later, and her parents were immediately aware that she was in serious respiratory distress. She was feverish, sitting up in bed, drooling, unable to speak or cry, and breathing noisily. The parents wrapped the child in warm blankets and drove her to the emergency department of the nearest hospital.
On inspection, the child demonstrated a puffy face, drooling, inspiratory stridor, and cyanotic nail beds. At this time, she was placed on a 4 L/min nasal cannula. The emergency physician looked at the girl and listened to her chest but did not examine her mouth. Respiratory rate was 36 breaths/min, blood pressure was 80/50, and pulse was 140 beats/min. The rectal temperature was 103.6° F (39.8° C). The physician ordered a lateral soft-tissue radiograph of the neck, but while waiting for the radiograph, the child became increasingly dyspneic and more cyanotic. Her SpO2 on 4 L/min nasal cannula was 88%. At this time, the following respiratory SOAP note was charted.
Respiratory Assessment and Plan
S Mother states that patient is in severe respiratory distress.
O RR 36/min, BP 80/50, P 140 regular. T 103.6° F (39.8° C). Child's face puffy, drooling. Inspiratory stridor (worsening). Nail beds cyanotic. On a 4 L/min nasal cannula: SpO2 88%. Soft tissue x-ray exam of neck pending.
A • Probable acute epiglottitis. No history of foreign body aspiration (general history).
• Impending acute ventilatory failure (SpO2 history, drooling, inspiratory stridor, and cyanosis)
P STAT page for anesthesiologist and ENT surgeon. Up-regulate the Oxygen Therapy Protocol (a non-rebreather with 100% oxygen [FIO2 1.0] if tolerated).
While the emergency page for the anesthesiologist and the ENT surgeon went out, a nonrebreathing oxygen mask was immediately “lightly” held to the child's face by the respiratory therapist. As soon as the physicians arrived (after about 10 minutes), the child was taken to the operating room. The surgeon stood by to perform an emergency tracheostomy while the anesthesiologist attempted to intubate the child.
Fortunately, the anesthesiologist was successful in spite of an enlarged, cherry-red epiglottis partially obstructing the larynx. As soon as the endotracheal tube was in place, the child relaxed and soon went to sleep. She was admitted to the intensive care unit (ICU), sedated, and placed on +5 cm H2O continuous positive airway pressure (CPAP). IV ceftriaxone was administered. She was extubated the next day when she demonstrated a leak around her ET tube. She was discharged on the third hospital day. A throat culture taken in the OR was positive for H. influenzae (type B). She was discharged on a 7-day course of oral cefdinir (Omnicef).
Discussion
Acute epiglottitis is a life-threatening condition. The key point to remember is to refrain from examining the throat until a staff member qualified in pediatric intubation is nearby. Such manipulation is often unsuccessful, and unless qualified assistance is at hand, the child may asphyxiate. The treatment suitably selected here was placement of a nonrebreathing oxygen mask while the appropriate team was assembled. Typical of this disease is its abrupt onset, and once the airway is secured and antibiotics given, the symptoms and danger subside. Maintaining the intubated airway until a leak is heard is key to survival. In cases of acute epiglottitis, H. influenzae type B will grow from blood cultures, whereas airway or respiratory tract cultures will grow non-typeable H. influenza.