Introduction to Thorax and Thoracic Cage
The thorax is the upper part of trunk, which extends from root of the neck to the abdomen. In general usage, the term chest is used as a synonym for thorax. The cavity of trunk is divided by the diaphragm into an upper part called thoracic cavity and the lower part called the abdominal cavity. The thoracic cavity contains the principal organs of respiration–the lungs, which are separated from each other by bulky and movable median septum – the mediastinum. The principal structures in the mediastinum are heart and great vessels.
THORACIC CAGE
The thorax is supported by a skeletal framework called thoracic cage. It provides attachment to muscles of thorax, upper extremities, back, and diaphragm. It is osteocartilaginous and elastic in nature. It is primarily designed for increasing or decreasing the intrathoracic pressure so that air is sucked into lungs during inspiration and expelled from lungs during expiration—an essential mechanism of respiration.
FORMATION OF THORACIC CAGE (Fig. 14.1)

| Anteriorly: | by sternum (breast bone). |
| Posteriorly: | by 12 thoracic vertebrae and intervening intervertebral discs. |
| Laterally: | by 12 pairs of ribs and associated 12 pairs of |
| each side: | costal cartilages. |
The rib cage is formed by sternum, costal cartilages, and ribs attached to the thoracic vertebrae.
The ribs articulate as follows:
1. Posteriorly—all the ribs articulate with the thoracic vertebrae.
(a) the upper seven ribs (1st–7th) articulate with the side of sternum through their costal cartilages.
(b) The next three ribs (e.g., 8th, 9th, and 10th) articulate with each other through their costal cartilages.
(c) The lower two ribs (e.g., 11th and 12th) do not articulate and anterior ends of their costal cartilages are free.
N.B. The costal cartilages of 7th, 8th, 9th, and 10th ribs form a sloping costal margin.
SHAPE OF THORACIC CAGE (Fig. 14.2)
The thoracic cage resembles a truncated cone with its narrow end above and broad end below. The narrow upper end is continuous above with root of neck from which it is partly separated on either side by the suprapleural membranes. The broad lower end is completely separated from abdominal cavity by the diaphragm, but provides passage to structures like, aorta, esophagus, and inferior vena cava.
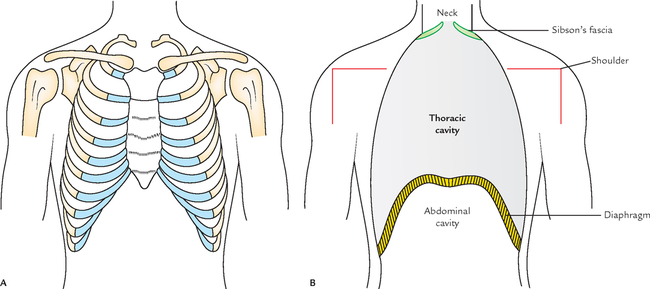
The diaphragm is dome shaped with its convexity directed upwards. Thus, the upper abdominal viscera lies within the thoracic cage and are protected by it.
In life, the upper end of thorax appears broad due to the presence of shoulder girdle made up of clavicles and scapulae and associated scapular musculature.
N.B. The thoracic cavity is actually much smaller than one assumes because the upper narrow part of thoracic cage appears broad (vide supra) and lower broad part of thoracic cage is encroached by the abdominal viscera due to dom-eshaped diaphragm.
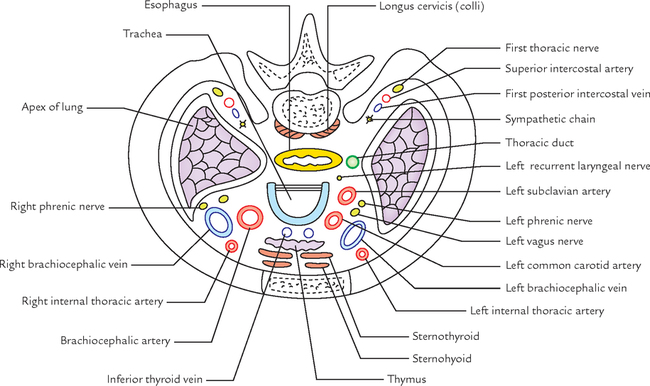
TRANSVERSE SECTION OF THORAX
In transverse section, the adult thorax is kidney shaped with transverse diameter more than the anteroposterior diameter (Fig. 14.3B, C). This is because the ribs are placed obliquely in adults.
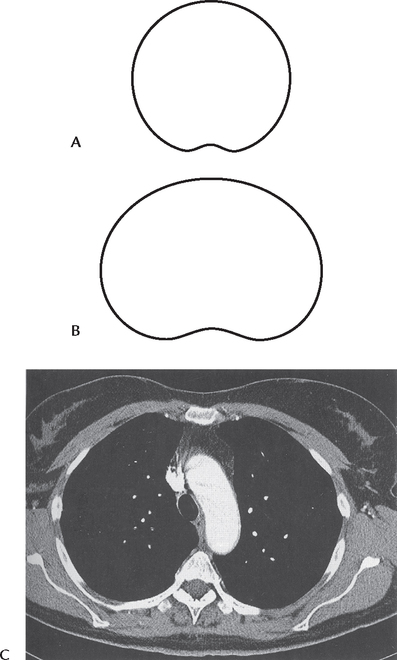
In transverse section, the thorax of infants below the age of two years is circular with equal transverse and anteroposterior diameter (Fig. 14.3A). This is because the ribs are horizontally placed.
The transverse sections of thorax in adult and infant are compared in Table 14.1.
Table 14.1
Comparison of thoracic cavity as seen in transverse sections of the thorax in adult and infant
| Thoracic cavity in adult | Thoracic cavity in infant |
| Kidney shaped | Circular |
| Ribs obliquely placed | Ribs horizontally placed |
| Transverse diameter can be increased by thoracic breathing (Hence respiration is thoraco-abdominal) | Transverse diameter cannot be increased by thoracic breathing (Hence respiration is purely abdominal) |
SUPERIOR THORACIC APERTURE (THORACIC INLET)
The thoracic cavity communicates with the root of the neck through a narrow opening called superior thoracic aperture or thoracic inlet.
N.B. The superior thoracic aperture is called thoracic outlet by the clinicians because important arteries and T1 spinal nerves emerge from thorax through this aperture and enter the neck and upper limbs.
Anatomists refer to the superior thoracic aperture as thoracic inlet because air and food enter the thorax through trachea and esophagus, respectively.
Boundaries (Fig. 14.4)

| Anteriorly: | Superior border of manubrium sterni. |
| Posteriorly: | Anterior border of the superior surface of the body of T1 vertebra. |
| Laterally (on each side): | Medial border of first rib and its cartilage. |
The upper end of anterior boundary lies 1.5 inches below the upper end of posterior boundary because first rib slopes downwards and forwards from its posterior end to anterior end (Fig. 14.5). Therefore, plane of thoracic inlet slopes (directed) downwards and forwards with an obliquity of about 45°. The upper border of manubrium sterni lies at the level of upper border of T3 vertebra (Fig. 14.6).
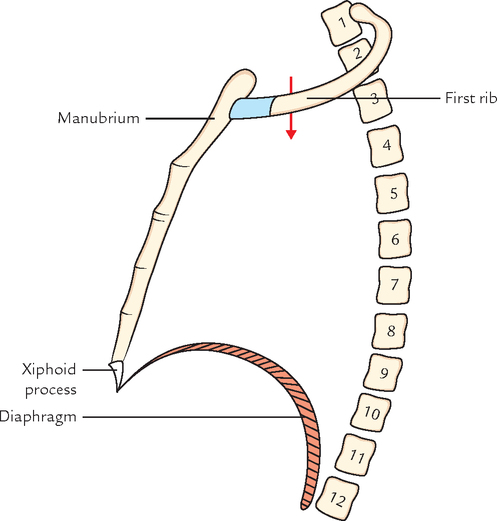

N.B. Due to downward and forward inclination of thoracic inlet, the apex of lung with the overlying pleura projects into the root of the lung.

DIAPHRAGM OF SUPERIOR THORACIC APERTURE (SUPRAPLEURAL MEMBRANE/SIBSON’S FASCIA)
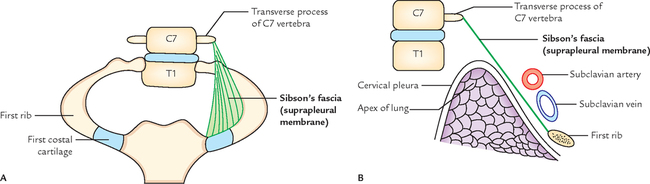
The part of thoracic inlet, on either side, is closed by a dense fascial sheet called suprapleural membrane or Sibson’s fascia, or diaphragm of superior thoracic aperture. It is tent-shaped.
Attachments and Relations (Fig. 14.7)
The apex of Sibson’s fascia is attached to the tip of transverse process of C7 vertebra, and its base is attached to the inner border of first rib and its costal cartilage. Its superior surface is related to the subclavian vessels and its inferior surface is related to cervical pleura, covering the apex of the lung.
Functions
The functions of Sibson’s fascia are as follows:
1. It protects the underlying cervical pleura, beneath which lies the apex of the lung.
2. It resists the intrathoracic pressure during respiration. As a result, the root of neck is not puffed up and down during respiration.
N.B. Morphologically, Sibson’s fascia represents the spread out degenerated tendon of scalenus minimus (or pleuralis) muscle.
Structures Passing Through Thoracic Inlet (Fig. 14.8)
1. Right and left internal thoracic arteries.
2. Brachiocephalic trunk/artery.
1. Right and left vagus nerves.
2. Left recurrent laryngeal nerve.
3. Right and left phrenic nerves.
INFERIOR THORACIC APERTURE (THORACIC OUTLET)
The inferior thoracic aperture is broad and surrounds the upper part of the abdominal cavity. The large musculoaponeurotic diaphragm attached to the margins of thoracic outlet separates the thoracic cavity from the abdominal cavity.
DIAPHRAGM OF INFERIOR THORACIC APERTURE (Fig. 14.9)
The thoracic outlet is closed by a large dome-shaped flat muscle called diaphragm. Since it separates thoracic cavity from abdominal cavity, it is also termed thoraco-abdominal diaphragm.
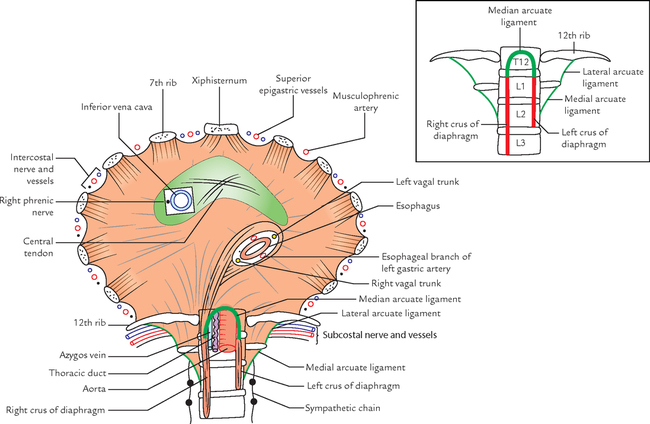
The diaphragm is the principal muscle of respiration. It is dome shaped and consists of peripheral muscular part, and central fibrous part called central tendon.
Origin
The origin of the diaphragm is divided into three parts, viz.
Sternal part: It consists of two fleshy slips, which arise from the posterior surface of the xiphoid process.
Costal part: On each side, it consists of six fleshy slips, which arise from the inner surface of lower six ribs near their costal cartilages.
Vertebral part: This part arises by means of (a) right and left crura of diaphragm and (b) five arcuate ligaments.
• Right crus: It is a vertical fleshy bundle, which arises from the right side of anterior aspects of the upper three lumbar vertebrae and intervening intervertebral discs.
• Left crus: It is vertical fleshy bundle, which arises from the left side of anterior aspects of upper two lumbar vertebrae and the intervening intervertebral discs.
The medial margins of the crura are tendinous.
• Median arcuate ligament is an arched fibrous band stretching between the upper ends of two crura.
• Medial arcuate ligament is the thickened upper margin of the psoas sheath. It extends from the side of the body of L2 vertebra to the tip of the transverse process of L1 vertebra.
• Lateral arcuate ligament is the thickened upper margin of fascia covering the anterior surface of the quadratus lumborum. It extends from the tip of transverse process of L1 vertebra to the 12th rib.
N.B. The right crus is attached to more number of vertebrae because the right side diaphragm has to contract on the massive liver.
Insertion
From circumferential origin (vide supra), the muscle fibres converge towards the central tendon and insert into its margins.
The features of the central tendon are as follows:
1. It is trifoliate in shape, having (a) an anterior (central) leaflet, and (b and c) two tongue-shaped posterior leaflets. It resembles an equilateral triangle. The right posterior leaflet is short and stout, whereas the left posterior leaflet is thin and long.
2. It is inseparably fused with the fibrous pericardium.
3. It is located nearer to the sternum than to the vertebral column.
Surfaces and Relations
The superior surface of diaphragm projects on either side as dome or cupola into the thoracic cavity. Depressed area between the two domes is called central tendon. The superior surface is covered by endothoracic fascia and is related to the bases of right and left pleura on the sides and to the fibrous pericardium in the middle.
The inferior surface of diaphragm is lined by the diaphragmatic fascia and parietal peritoneum.
Openings of the Diaphragm
The openings of diaphragm are classified into two types: (a) major openings and (b) minor openings.
Major Openings
There are three named major openings, viz.
The location, shape, and vertebral levels of these openings are presented in Table 14.2.
Table 14.2
Location, shape, and vertebral level of three major openings of the diaphragm
| Opening | Location | Shape | Vertebral level |
| Vena caval opening | In the central tendon slightly to the right of median plane between the central and right posterior leaflets | Quadrangular or square | T8 (body) |
| Esophageal opening | Slightly to the left of median plane (The fibres of right crus split around the opening and act like pinch cock) | Oval or elliptical | T10 (body) |
| Aortic opening | In the midline behind the median arcuate ligament | Circular or round | T12 (lower border of the body) |

The structure passing through three major opening of diaphragm are listed in Table 14.3.

Minor Openings
These are unnamed. Structures passing through these openings are as follows:
1. Superior epigastric vessels pass through the gap (space of Larry) between the muscular slips arising from xiphoid process and 7th costal cartilage.
2. Musculophrenic artery passes through the gap between the slips of origin from 7th to 8th ribs.
3. Lower five intercostal nerves and vessels (i.e., 7th–11th) pass through gaps between the adjoining costal slips.
4. Subcostal nerves and vessels pass deep to the lateral arcuate ligament.
5. Sympathetic chain passes deep to the medial arcuate ligament.
6. Greater, lesser, and least splanchnic nerves pass by piercing the crus of diaphragm on the corresponding side.
Nerve Supply
The phrenic nerves are both motor and sensory. The right phrenic nerve provides motor innervation to the right half of the diaphragm up to the right margin of esophageal opening, and left phrenic nerve provides motor innervation to the left half of the diaphragm up to the left margin of the esophageal opening.
The phrenic nerves provide sensory innervation to the central tendon of the diaphragm, and pleura and peritoneum related to it.
The intercostal nerves supply the peripheral parts of the diaphragm.
Arterial Supply
The diaphragm is supplied by the following arteries:
1. Superior phrenic arteries (also called phrenic arteries) from thoracic aorta.
2. Inferior phrenic arteries, from the abdominal aorta.
3. Pericardiophrenic arteries, from the internal thoracic arteries.
4. Musculophrenic arteries, the terminal branches of the internal thoracic arteries.
5. Superior epigastric arteries, the terminal branches of the internal thoracic arteries.
6. Lower five intercostal and subcostal arteries from the aorta.
Actions of Diaphragm
The diaphragm acts to subserve the following functions:
1. Muscle of inspiration: The diaphragm is the main/principal muscle of respiration. When it contracts, it descends and increases the vertical diameter of the thoracic cavity (for details see ![]() Page 223).
Page 223).
2. Muscle of abdominal staining: The contraction of diaphragm along with contraction of muscles of anterior abdominal wall raises the intra-abdominal pressure to evacuate the pelvic contents (voluntary expulsive efforts, e.g., micturition, defecation, vomiting, and parturition).
3. Muscle of weight lifting: By taking deep breath and closing the glottis, if possible to raise the intra-abdominal pressure to such an extent that it will help support the vertebral column and prevent its flexion. This assists the postvertebral muscles in lifting the heavy weights.
4. Thoraco-muscular pump: The descent of diaphragm decreases the intrathoracic pressure and at the same time increases the intra-abdominal pressure. This pressure change compresses the inferior vena cava, and consequently its blood is forced upward into the right atrium.
5. Sphincter of esophagus: The fibres of the right crus of diaphragm subserve a sphincteric control over the esophageal opening.
Development
The diaphragm develops in the region of neck from the following four structures (Fig. 14.10):
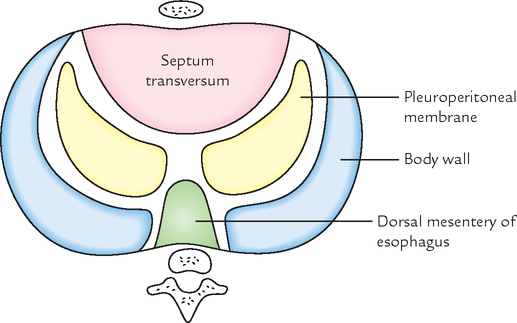
1. Septum transversum, ventrally.
2. Pleuroperitoneal membranes at the sides.
• Central tendon of diaphragm develops from septum transversum.
• Domes of diaphragm develop from pleuroperitoneal membrane.
• Part of diaphragm around the esophagus develops from the dorsal mesentery of esophagus.
• Peripheral part of diaphragm, develops from the body wall.
For details of development, consult any textbook of Embryology.
N.B. The musculature of diaphragm develops from 3rd, 4th, and 5th cervical myotomes (C3, C4, C5), hence it receives its motor innervations from C3, C4, and C5 spinal segments (i.e., phrenic nerve). Later, when diaphragm descends from the neck to its definitive position (i.e., thoraco-abdominal junction), its nerve supply is dragged down. This explains the long course of the phrenic nerve.
The various types of congenital diaphragmatic hernias are as follows:
1. Posterolateral hernia (commonest congenital diaphragmatic hernia; Fig. 14.11): In this condition, there is herniation of abdominal contents into the thoracic cavity, which compress the lung and heart. The herniation occurs through the gap (pleuroperitoneal hiatus) between the costal and vertebral origins of the diaphragm called foramen of Bochdalek. The gap remains due to failure of closure of pleuroperitoneal canal. It occurs commonly on the left side (for details see Clinical and Surgical Anatomy, 2nd edition by Vishram Singh).

2. Retrosternal hernia: It occurs through the gap between the muscular slips of origin from xiphisternum and 7th costal cartilage (space of Larry or foramen of Morgagni). It is more common on the right side. Thus hernial sac usually lies between pericardium and right pleura. Usually it causes no symptoms in the infants, but in later age, the patients complain of discomfort and dysphagia (difficulty in swallowing).
3. Paraesophageal hernia: In this condition, there is defect in the diaphragm to the right and anterior to the esophageal opening. The anterior wall of the stomach rolls upwards in the hernial sac through this defect, until it becomes upside down in the thoracic cavity. An important feature of paraesophageal hernia is that the normal relationship of gastroesophageal junction in relation to diaphragm is not disturbed.
The acquired diaphragmatic hernias may be either traumatic or hiatal (sliding).
1. Traumatic hernia: It may occur due to an open injury to the diaphragm by the penetrating wounds or closed injury to the diaphragm in road traffic accidents leading to sudden severe increase in the intra-abdominal pressure.
2. Hiatal (sliding) hernia (Fig. 14.12): This is the commonest of all the internal hernias. In sliding hernia, the gastroesophageal junction and cardiac end of stomach slides up into the thoracic cavity, but only anterolateral portion of the herniated stomach is covered by peritoneum, therefore the stomach itself is not within the hernial sac. The hiatal hernia is caused by the weakness of the diaphragmatic muscle surrounding the esophageal opening and increased intra-abdominal pressure. This may cause regurgitation of acid contents of stomach into the esophagus leading to peptic esophagitis. The patient complains of heart burn. The sliding hernia is usually associated with short esophagus.

 Principal muscle of respiration/most important muscle of inspiration Principal muscle of respiration/most important muscle of inspiration |
Diaphragm |
| Commonest congenital diaphragmatic hernia |
Posterolateral hernia/herniation through foramen of Bochdalek |
| Commonest of all the internal hernias |
Acquired hiatal (sliding) hernia |
| Superior thoracic aperture is called by clinicians as |
Thoracic outlet |
| Diaphragm receives its motor innervations from C3, C4, and C5 spinal segments (phrenic nerve) because |
Musculature of diaphragm develops from 3rd, 4th, and 5th cervical myotomes in the region of the neck |


A male infant was brought to the hospital having markedly labored respiration and cyanosis. The heart sounds were displaced and there was an apparent dextrocardia. The left side of the chest was dull (flat) to percussion and had diminished breath sounds. The abdomen was characteristically scaphoid (i.e., boat shaped). The X-ray chest revealed the presence of bowel, spleen, and portions of the liver within thorax. A diagnosis of congenital posterolateral (Bochdalek) hernia of diaphragm was made.
1. Tell the congenital defect of diaphragm that leads to posterolateral hernia of Bochdalek.
2. Posterolateral (Bochdalek) hernia is common on which side—right or left?
3. What are the different types of congenital diaphragmatic hernia?
4. Which is the commonest congenital hernia of the diaphragm? Give its incidence.
1. Congenital gap between the vertebral and costal origins of the diaphragm due to failure of closure of pleuro-peritoneal canal.
2. It is three to five times more common on the left side.
3. (a) Posterolateral hernia, (b) retrosternal hernia, and (c) congenital paraesophageal or rolling hernia.
4. Posterolateral hernia of Bochdalek. Its incidence is 1:2000 births.