Thoracic Duct, Azygos and Hemiazygos Veins, and Thoracic Sympathetic Trunks
THORACIC DUCT
The thoracic duct is the largest lymphatic vessel (trunk or great lymph channel) which drains lymph from most of the body into the bloodstream. The lymph in the thoracic duct is milky-white in appearance because it contains a product of fat digestion (chyle) from the intestine. The duct appears beaded due to the presence of numerous valves in its lumen.
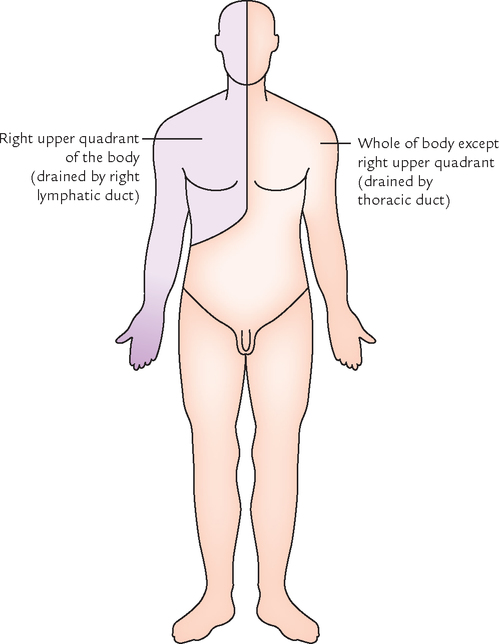
Area of drainage: The thoracic duct drains the lymph from all the parts of the body except the (a) right side of the head and neck, (b) right side of the chest wall, (c) right lung, (d) right side of the heart, and (e) right surface of the liver.
N.B. Thoracic duct drains lymph from whole of the body except the right upper quadrant of the body which is drained by the right lymphatic duct (Fig. 23.1).
Extent: The thoracic duct extends to the upper end of cisterna chyli on the posterior abdominal wall at the lower border of T12 vertebra to the junction of left internal jugular and left subclavian veins at the root of the neck.
Measurements: The measurements of the thoracic duct are as follows:
Width of lumen: 5 mm (at the ends but narrow in the middle).
FORMATION, COURSE, AND TERMINATION (Fig. 23.2)
The duct begins in the abdomen at the lower border of T12 vertebra, as a continuation of cisterna chyli (lying in front of the bodies of L1 and L2 vertebrae) and enters the thorax through the aortic opening of the diaphragm. It then ascends in the posterior mediastinum to the right of midline on the front of vertebral bodies. On reaching the T5 vertebra, it crosses the midline from right to left side and enters the superior mediastinum to run along the left border of the esophagus and reaches the root of the neck.

At the root of neck it arches laterally at the level of C7 vertebra—in front of vertebral system (e.g., vertebral artery and vertebral vein) and left cervical sympathetic trunk and behind the carotid system (e.g., left common carotid artery, left internal jugular vein, and left vagus nerve). The summit of arch lies 3–4 cm above the clavicle. Finally, the duct descends in front of the first part of left subclavian artery and finally terminates by opening into the junction of left subclavian and left internal jugular veins.
N.B. The thoracic duct begins in abdomen, courses through thorax and terminates in the neck.
RELATIONS (Fig. 23.3)
The relations of thoracic duct are as follows:

A At the aortic orifice of the diaphragm
| Anterior: | Median arcuate ligament of diaphragm. |
| Posterior: | T12 vertebra. |
| To the right: | Azygos vein. |
| To the left: | Aorta. |
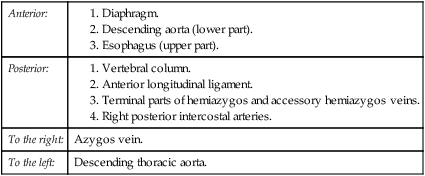
B In the posterior mediastinum
| Anterior: | |
| Posterior: | |
| To the right: | Azygos vein. |
| To the left: | Descending thoracic aorta. |
| Anterior: | |
| Posterior: | Vertebral column. |
| To the right: | Edge of esophagus. |
| To the left: | Left lung and pleura. |
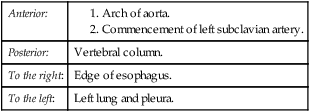
D In the root of the neck (Fig. 23.3)
| Anterior: | Carotid sheath containing left common carotid artery, left internal jugular vein, and left vagus nerve. |
| Posterior: |

TRIBUTARIES
The tributaries of the thoracic duct are as follows (Fig. 23.4):

Efferent from lower six intercostal lymph nodes of both sides.
1. A pair of the ascending lymph trunks which drains lymph from the upper lumbar lymph nodes (para-aortic lymph nodes).
2. A pair of the descending lymph trunks which drain lymph from the posterior intercostal lymph nodes of upper six spaces.
3. Lymph vessels from the posterior mediastinal lymph nodes.
Development
There are three stages in the development of the thoracic duct (Fig. 23.5).

Stage I: In this stage, network of lymph channels is seen in front of the thoracic part of the vertebral column.
Stage II: In this stage, two longitudinal lymph channels appear, in the network of lymph channels, one on the left and another on the right with a number of cross communications.
Stage III: In this stage, the cross communication appears opposite the T5 vertebra, right longitudinal channel below this cross communication and left longitudinal channel above this cross communication persists and form the thoracic duct. All the other parts disappear.
AZYGOS VEIN (Fig. 23.6)
The azygos vein is present only on the right side in the upper part of the posterior abdominal wall and the posterior mediastinum. It connects the inferior vena cava with the superior vena cava. It is provided with valves and may appear tortuous.
The functions of azygos vein are as follows:
1. It drains venous blood from the thoracic wall and upper lumbar region.
2. It forms an important collateral channel connecting the superior vena cava and inferior vena cava.
FORMATION
The formation of azygos vein is variable. It is formed in one of the following ways:
1. Formed by the union of right subcostal and right ascending lumbar vein at the level of T12 vertebra (common).
2. Arises from the posterior aspect of the inferior vena cava (IVC) near the renal veins.
3. As a continuation of right subcostal vein.
4. Occasionally, it may arise from right renal or right first lumbar vein.
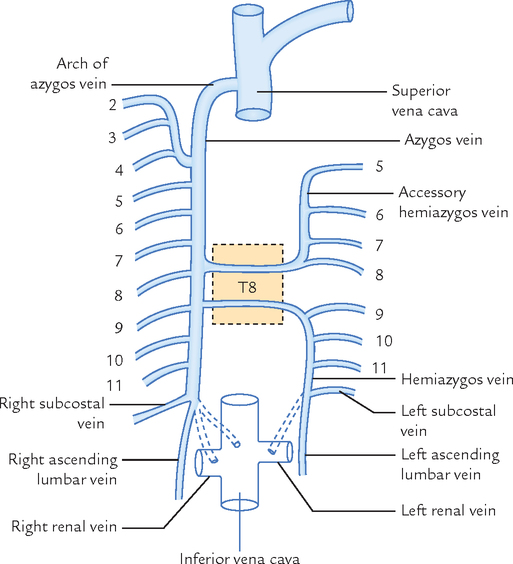
COURSE AND TERMINATION
The azygos vein after formation ascends up and leaves the abdomen by passing through the aortic opening of the diaphragm and enters the posterior mediastinum. There it ascends vertically lying in front of vertebral column up to the level of T4 vertebra, where it arches forwards above the hilum of the right lung to terminate in the superior vena cava at the level of the 2nd costal cartilage.

TRIBUTARIES
The tributaries of the azygos vein are as follows:
1. Lower 7th right posterior intercostal veins except first.
2. Right superior intercostal vein (formed by union of 2nd, 3rd, and 4th right posterior intercostal veins).
3. Hemiazygos vein (at the level of T7 or T8 vertebra).
4. Accessory hemiazygos vein (at the level of T8 or T9 vertebra).
7. Right ascending lumbar vein.
8. Esophageal veins with the exception of those at its lower end.
In case of obstruction of SVC, it serves as the main collateral channel to shunt the blood from the upper half of the body to IVC (for details see Clinical correlation on ![]() p. 285.
p. 285.
HEMIAZYGOS VEIN (Fig. 23.6)
The hemiazygos vein (syn. inferior hemiazygos vein) lies on the left side only and corresponds to the lower part of the azygos vein (i.e., mirror image of the lower part of the azygos vein).
COURSE AND TERMINATION
It pierces the left crus of the diaphragm and ascends vertically in front of the left side of the vertebral column up to the level of T8 vertebra. At T8 vertebra it turns to the right and crosses in front of the vertebral column posterior to the aorta, esophagus and thoracic duct to terminate in the azygos vein.
ACCESSORY HEMIAZYGOS VEIN
The accessory hemiazygos vein (syn. superior hemiazygos vein; Fig. 23.6) lies on the left side only and corresponds to the upper part of the azygos vein (i.e., mirror image of the upper part of the azygos vein).
COURSE AND TERMINATION
The accessory hemiazygos vein begins at the medial end of left 4th or 5th intercostal space and descends to the left side of the vertebral column. At the level of T8 vertebra, it turns to the right passes in front of the vertebral column posterior to the aorta, esophagus and thoracic duct to terminate in the azygos vein.
N.B. Sometimes the terminal parts of hemiazygos and accessory hemiazygos veins join together to form a common trunk which crosses across the vertebral column to open into the azygos vein.
THORACIC SYMPATHETIC TRUNKS (Fig. 23.7)
The thoracic sympathetic trunk is a ganglionated chain situated on either side of the vertebral column. Superiorly it is continuous with the cervical sympathetic chain at the thoracic inlet and inferiorly with the lumbar sympathetic chain after passing behind the medial arcuate ligament of the diaphragm.
COURSE AND RELATIONS
The sympathetic chain descends in front of the neck of the 1st rib, head of 2nd–10th ribs and along the bodies of T11 and T12 vertebrae, in front of posterior intercostal nerve and vessels, passes behind the medial arcuate ligament to become continuous with the lumbar sympathetic trunk.
GANGLIA
Initially, each thoracic sympathetic trunk has 12 ganglia corresponding to the 12 thoracic spinal nerves. The first ganglion commonly fuses with the inferior cervical sympathetic ganglia to form the cervico-thoracic/stellate ganglion. The second ganglion also may occasionally fuse with the first ganglion. Thus there are usually 11 ganglia in the thoracic sympathetic trunk; sometimes there may be only 10 ganglia (vide supra). Each ganglion lies at the level of the corresponding intervertebral disc and is connected to the corresponding spinal nerve by white and grey ramus communicans.
BRANCHES
The branches of thoracic sympathetic trunks are divided into two groups: medial and lateral.
A Medial branches
The medial branches supply the viscera. They are as follows:
1. The medial branches from 1st to 5th ganglia consist of postganglionic fibres and are distributed to the heart, great vessels, lungs, and esophagus through the following plexuses:
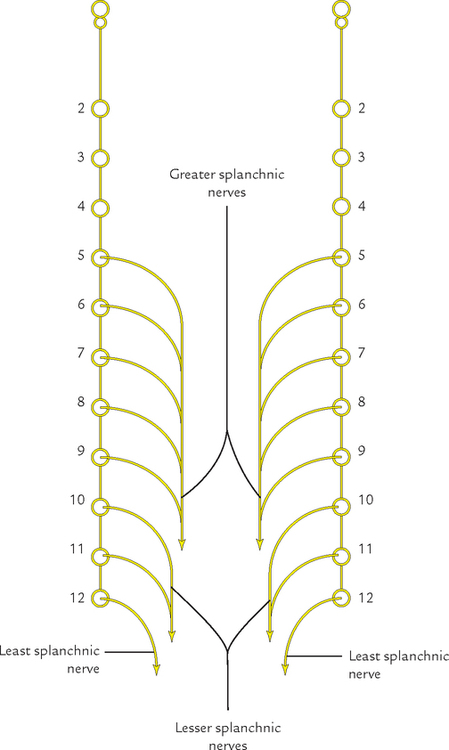
2. Medial branches from 5th to 12th thoracic ganglia consist of preganglionic fibres and from three splanchnic nerves as follows:
(a) Greater splanchnic nerve: It is formed by the preganglionic fibres arising from 5th to 9th ganglia. It descends obliquely on the vertebral bodies, pierces the corresponding crus of diaphragm and terminates mainly in the celiac ganglion. Partly it also terminates in the aorticorenal ganglion and the suprarenal gland.
(b) Lesser splanchnic nerve: It is formed by the preganglionic fibres from 10th and 11th ganglia. It course is obliquely similar to the greater splanchnic nerve, pierces the corresponding crus of diaphragm and terminates in the celiac ganglion.
(c) Least (lowest) splanchnic nerve: It is also called renal nerve. This tiny nerve arises from the 12th thoracic ganglion and may even be absent. It descends obliquely as greater and lesser splanchnic nerves, pierces either the crus or passes behind the medial arcuate ligament of diaphragm and terminates in the renal plexus.
B Lateral branches
The lateral branches supply limbs and body wall. Their supply is pilomotor, sudomotor, and vasomotor to the skin of these regions.
The preganglionic fibres arise from the lateral horns of spinal segments and enter the sympathetic ganglion via white rami communicantes of the spinal nerve. The preganglionic fibres from the ganglion re-enter the spinal nerve via grey rami communicantes and supply the corresponding dermatome of the upper limb and the body wall.
 Largest lymphatic channel in the body Largest lymphatic channel in the body |
Thoracic duct |
| Chylothorax |
Accumulation of chyle in the pleural cavity |
| Chylocele |
Accumulation of chyle in the tunica vaginalis |
| Renal nerve |
Least splanchnic nerve |
| Commonest cause of damage of thoracic duct at the root of the neck |
Block dissection of the neck |
| Largest collateral channel connecting superior and inferior vena cavae |
Azygos vein |
| Largest splanchnic nerve |
Greater splanchnic nerve |
| Most posterior intercostal veins drain into |
Azygos venous system |

A 50-year-old male visited the hospital and complained of swelling of the scrotum associated with periodic fever and passage of milky urine. On examination, the doctor found that scrotum as a whole was enlarged. The scrotal skin was thickened mainly at the bottom. On aspiration of scrotum a milky fluid came out. He was diagnosed as a case of chylocele and chyluria.