Forceps and vacuum
Forceps
Describe different parts of forceps and classify forceps.
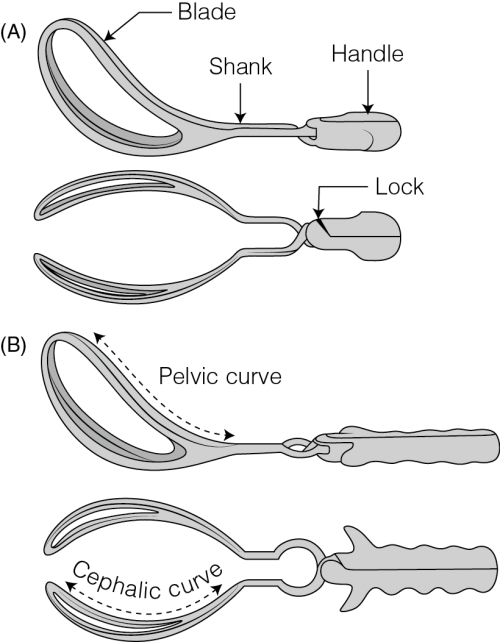
Forceps is a paired metal instrument used to assist vaginal delivery; they are identified as left (lower and applied on the left side of the pelvis and fetal head) and right (applied on the right side of the pelvis and fetal head). Different parts of each side are handle, lock shank and blade (Fig. 43.1A). Blades are curved and each blade has two curves. The lateral curve is designed to conform to the fetal head and is called cephalic curve. The vertical curve corresponds to the axis of the birth canal and is called as the pelvic curve (Fig. 43.1B). Blades are fenestrated to allow firmer grip over the fetal head without crushing or compressing it. Moreover, when assembled the tips never meet and the distance between tips is 2.5 cm and the distance at the centre is 7.5 cm. Shank is the portion that is between the blade and the handle. It is the length of the shank that determines the type of forceps. It is about 5 cm in outlet forceps and 7.5 cm or more in low forceps. Lock is devised to articulate with the fellow forceps. It is located on the shank at its junction with the handle. It is in the form of a socket that compliments with the one similarly located on opposite shank. The articulation is usually referred as English lock.
There are three types of forceps:
(1) Traction forceps short or long (pull required: 18 kg in primi, 14 kg in multi)
(2) Rotation forceps – Not used in modern obstetrics
(3) For special use – Piper’s forceps (long forceps with minimal pelvic curve) for after coming head in breech
Acog classification of forceps
| Type of instrument | Criteria for application |
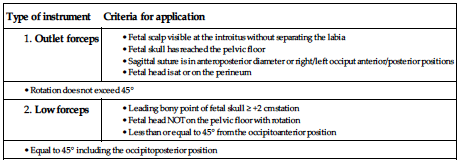
Mid and high forceps are not used in modern obstetrics.
What are the indications, prerequisites for forceps delivery?
Maternal indications
■ Undue delay in second stage (those with occiptioposterior, on epidural)
■ Exhaustion following prolonged labour
■ Maternal distress – maternal tachycardia, dehydration, ketoacidosis and pyrexia
■ To cut short normal second stage (prophylactic forceps) as in heart disease, preeclampsia, anaemia, previous LSCS
Fetal indications
■ Fetal distress/nonreassuring status in the second stage of labour
■ Cord prolapse – in the second stage of labour
■ Abruptio placenta – in the second stage of labour
■ Breech presentation – for delivery of aftercoming head
■ Prophylactic application – delivery of a preterm baby by providing a protective cage to the fetal head in preventing intracranial damage
Prerequisites
■ Bladder and bowel should be emptied
■ Usually episiotomy is given prior to application of blades or while applying traction (after local infiltration with lignocaine)
■ Cervix should be fully dilated
■ Membranes should be ruptured
■ Station of the head should be +2 or +3
■ Head is fully rotated (sagittal suture in AP diameter of the outlet)
Describe the forceps application.
Please refer to Chapter 72 of Holland and Brews Manual of Obstetrics for answer.
List the complications of forceps.
Maternal complications of forceps
Fetal complications of forceps
What is trial forceps and what is failed forceps?
Please refer to Chapter 72 of Holland and Brews Manual of Obstetrics for answer.
Vacuum
Describe ventouse (vacuum extraction), also write about the indications and contraindications of vacuum delivery.
Ventouse (the French word for soft cup) is the instrument used to let the scalp to be drawn into the cup by creating negative suction and then applying the traction to effect delivery. This is one of the frequently practiced instrumental vaginal delivery and is referred as vacuum extraction or ventouse delivery. The instrument unit used is vacuum extractor or ventouse.
Vacuum extraction can be used as an alternative to forceps delivery and has advantages over it by being applicable even when the cervix is not fully dilated and fetal head is not favourably rotated as autorotation is possible in vacuum delivery.
The components of vacuum delivery system are:
■ The metal cups (different sizes 40, 50, 60 mm are available) (Fig. 43.2) that are narrower at the rim than the rest of cup. This is to accommodate expanded fetal scalp tissue or a silastic vacuum cup (Fig. 43.3)
■ Glass trap bottle with manometer
■ Chain attached to the cup which passes through the tubing and attaches to a cross-bar and handle used for traction
■ Suction apparatus (usually electric suction in these days) (Fig. 43.4)



Indications for vacuum delivery
They are similar to forceps delivery except the contraindications for vacuum (given below).
Maternal indications
Fetal indications
■ Fetal distress/nonreassuring status in the second stage of labour
■ Cord prolapse – in the second stage of labour
■ Abruptio placenta – in the second stage of labour
■ Prophylactic application – delivery of a preterm baby by providing a protective cage to the fetal head in preventing intracranial damage
Contraindications for vacuum delivery
■ Breech presentation – for delivery of aftercoming head
■ Preterm baby/low birthweight babies to avoid intracranial haemorrhage
■ Fetal invasive monitoring (scalp blood sampling)
■ Maternal exhaustion/hypotonic uterine action – Vacuum extractor needs maternal efforts to supplement the traction effect
Describe the conduct of vacuum delivery and its complications.
Prerequisites for vacuum extraction
Conduct of vacuum extraction
Knowledge of the position of fetal head and occiput along with suture lines in the patient is necessary to place the cup at the pivotal point, the point of cranial flexion. When correctly placed, the vacuum cup is positioned centrally over it. It is better to choose the largest cup that can be introduced comfortably. When properly applied, the edge of a 60 mm cup should be 30 mm behind the anterior fontanelle in the midline over the sagittal suture so that the posterior fontanelle is covered (Fig. 43.5A and B).

It should be emphasized that the cervical rim or vaginal wall are not included in the cup. When using rigid cups, it is recommended that the vacuum be created gradually by increasing the suction by 0.2 kg/cm2 every 2 min until a negative pressure of 0.8 kg/cm2 is reached. The metal cups help in creating chignon, an induced caput succedaneum, which forms a holding link between the instrument and the baby. Wait for 2 min for the formation of chignon. With soft cups, no chignon is formed and hence negative pressure can be increased to 0.8 kg/cm2 over as little as 1 min.
Traction should be made intermittently coinciding with the uterine contractions and supplemented by maternal expulsive efforts. When applied the traction should be sustained during the pains, and the direction of pull should correspond to the axis of the birth canal. The pull should be at right angles to the cup to prevent the cup from slipping.
Traction is relaxed in between the pains and the suction force reduced temporarily. Limit unintended cup detachments to no more than 2 or 3 with soft silicone cups or 1 or 2 with rigid metal cups. Delivery is usually effected with 4–6 pulls given over a period of 15–20 min. Once the head is delivered, suction is released and the cup slips off.