Blood Supply and Lymphatic Drainage of the Head and Neck
BLOOD SUPPLY OF HEAD AND NECK
The blood supply of head and neck consists of an arterial supply and venous drainage and carried out by the arteries and veins, respectively. The medical students must know the location of larger blood vessels of the head and neck because these vessels may become compromised due to disease process or during surgical procedures. The blood vessels also spread infection to head and neck. Further, they may also spread cancer cells from a malignant tumor to distant sites (metastasis) and at a faster rate than lymph vessels. The blood vessels are less numerous than lymph vessels yet the veins usually parallel the lymph vessels.
ARTERIAL SUPPLY
The arteries that supply the head and neck are subclavian and common carotid arteries (Fig. 16.1). The main arteries of the head and neck are right and left common carotid arteries, each of which divides into (a) an external carotid artery and (b) an internal carotid artery. The external carotid artery supplies structures external to the head and greater part of the neck. The internal carotid artery supplies structures within the cranial cavity and the orbit. The common carotid, external carotid, and internal carotid together form the carotid system of arteries. The carotid system of arteries forms the major source of arterial blood supply to the head and neck.

SUBCLAVIAN ARTERIES
The subclavian artery is so called because it is located beneath the clavicle. It is the main source of blood supply to the upper limb and hence called artery of the upper limb. However, the subclavian artery also supplies considerable part of the thoracic wall, head, neck, and brain through its branches.
Origin (Fig. 16.2)
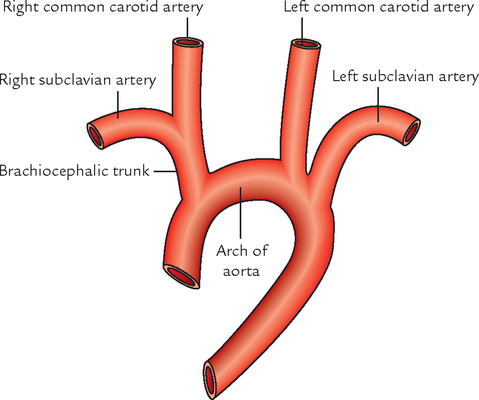
1. The right subclavian artery arises from the brachiocephalic trunk behind the right sternoclavicular joint at the root of neck.
2. The left subclavian artery arises from the arch of aorta in the thorax. It runs upwards on the left mediastinal pleura and makes groove on the left lung and enters the neck by passing behind the left sternoclavicular joint.
N.B. Based on their origin, the right subclavian artery has only cervical part whereas the left subclavian artery has thoracic as well as cervical parts. The cervical part extends from sternoclavicular joint to the outer border of the first rib.
Course (Fig. 16.3)
In the neck, both the arteries pursue a similar course.

On each side, the subclavian artery arches laterally across the anterior surface of the cervical pleura onto the first rib posterior to the scalenus anterior muscle. At the outer border of 1st rib, it ends by becoming axillary artery.
Parts
On each side, the subclavian artery is divided into three parts by the scalenus anterior muscle (Fig. 16.3). These are:
1. The common carotid artery, internal jugular vein, vagus nerve, vertebral vein, phrenic nerve, sternocleidomastoid, sternothyroid, and sternohyoid muscles.
2. Thoracic duct (only on the left side), cardiac branches of the vagus and sympathetic trunk; and ansa cervicalis (encircling the subclavian artery), and phrenic nerve on the left side only.
1. Apex of lung covered by the cervical pleura and suprapleural membrane.
2. Lower trunk of the brachial plexus and scalenus medius muscle.
N.B. The second part forms the summit of the arch of the subclavian artery and rises 1.5–2.5 cm above the level of the clavicle. It emerges through the gap between scalenus anterior and scalenus medius muscle along with lower trunk of the brachial plexus.
Branches of the Subclavian Artery (Fig. 16.5)
The subclavian artery usually gives off four branches. All of them arise from first part with the exception of costocervical trunk, which on the right side arises from the second part.

Vertebral Artery
The vertebral artery is one of the principal arteries which supplies the brain.
It is the first and largest branch of the first part of the subclavian artery (Fig. 16.6).

Origin, Course, and Termination
The vertebral artery arises from the upper aspect of the first part of the subclavian artery, runs vertically upwards to enter the foramen transversarium of the transverse process of C6. Then it passes through the foramen transversaria of the upper six cervical vertebrae.
After emerging from the foramen transversarium of C1, it winds backwards around the lateral mass of the atlas and enters the cranial cavity through foramen magnum.
In the cranial cavity, it unites with the vertebral artery of the opposite side at the lower border of the pons to form the basilar artery.
Parts (Fig. 16.6)
The vertebral artery is divided into four parts, viz.
1. First (cervical) part—extends from origin to foramen transversarium of C6 vertebra. This part lies in the scalenovertebral triangle.
2. Second (vertebral) part—lies within the foramen transversaria of upper six cervical vertebrae.
3. Third (suboccipital) part—extends from foramen transversarium of C1 vertebra to the foramen magnum of skull. This part lies within the suboccipital triangle.
4. Fourth (intracranial) part—extends from foramen magnum to the lower border of the pons.
Branches
In the neck (cervical branches)
1. Spinal branches: They arise from the second (vertebral) part and enter the vertebral canal through intervertebral foramina to supply the upper five or six cervical segments of the spinal cord.
2. Muscular branches: They arise from the first and third parts of the vertebral artery. Those from the first part, supply deep muscles of the neck and those from the third part, supply the muscles of the suboccipital triangle.
In the cranial cavity (cranial branches)
They arise from the 4th part. These are:
Subclavian steal syndrome (Fig. 16.7): If there is obstruction of the subclavian artery proximal to the origin of vertebral artery, some amount of blood from opposite vertebral artery will pass in a retrograde fashion to the subclavian artery of the affected side through the vertebral artery of that side to provide the collateral circulation to the upper limb on the side of lesion. Thus there occurs a sort of stealing of blood of brain by the subclavian artery of the affected side. Hence, the name subclavian steal syndrome.

Internal Thoracic Artery (Internal Mammary Artery)
The internal mammary artery arises from the inferior aspect of the first part of the subclavian artery opposite the origin of thyrocervical trunk. It passes downwards and medially in front of the cupola of the cervical pleura and enters the thorax behind the sternoclavicular joint.
In the thorax, it passes vertically downwards, about 1.25 cm away from the lateral border of the sternum, up to the level of the 6th intercostal space, where it divides into two terminal branches: musculophrenic and superior epigastric arteries (for details see Textbook of Anatomy: Upper Limb and Thorax, Vol. I by Vishram Singh).
Thyrocervical Trunk
It is the short, wide branch of the subclavian artery.
Branches (Fig. 16.5)
Inferior thyroid artery:
It ascends along the medial border of scalenus anterior and just below transverse process of C7 vertebra, it turns medially in front of the vertebral artery and posterior to vagus nerve, sympathetic trunk, and common carotid artery to reach the posterior surface of the lateral lobe of the thyroid gland. Then it descends to the lower pole of the thyroid lobe and divides into ascending and descending glandular branches.
In addition to glandular branches to thyroid gland it also gives the following branches:
1. Ascending cervical artery passes upwards in front of the transverse processes of cervical vertebrae along the medial side of the phrenic nerve and acts as a guide to this nerve. It supplies prevertebral muscles and sends spinal branches to the vertebral canal along the spinal nerves.
2. Inferior laryngeal artery accompanies the recurrent laryngeal nerve to the larynx and supplies the mucous membrane of the larynx below the vocal cord and muscles of the larynx.
3. Tracheal, pharyngeal, and esophageal branches to trachea, pharynx, and esophagus, respectively.
Transverse cervical artery:
It passes laterally and upwards across the scalenus anterior to reach the posterior triangle, where it lies in front of the trunks of the brachial plexus. Here, it further divides into superficial and deep branches. The superficial branches ascend beneath the trapezius and anastomoses with the superficial division of the descending branch of the occipital artery.
The deep branch courses deep to the levator scapulae and takes past in the scapular anastomosis.
Suprascapular artery:
It passes laterally across the scalenus anterior to lie in front of the third part of the subclavian artery and of brachial plexus. Now it passes behind the clavicle to reach the suprascapular notch of the scapula, where it passes above the suprascapular ligament to enter the suprascapular fossa and takes part in the formation of arterial anastomosis around the scapula.
Costocervical Trunk (Fig. 16.8)

Course and Termination
The artery arches backwards above the cupola of the pleura and on reaching the neck of the first rib it terminates by dividing into ascending deep cervical artery and ascending superior (highest) intercostal artery.
Deep cervical artery passes backwards between the transverse process of C7 vertebra and neck of the first rib. It then ascends between the semispinalis capitis and semispinalis cervicis and anastomoses with the deep division of the descending branch of the occipital artery.
Superior (highest) intercostal artery descends in front of the neck of the first two ribs and gives rise to posterior intercostal arteries to the first two intercostal spaces.
Dorsal Scapular Artery
It arises from the third part of the subclavian artery (but may be the deep branch of the transverse cervical artery). As a direct branch of the subclavian artery, it passes laterally and backwards between the trunks of brachial plexus to reach underneath the levator scapulae. Now it descends along the medial border of the scapula in company with dorsal scapular nerve deep to rhomboids and takes part in the formation of arterial anastomosis around the scapula.
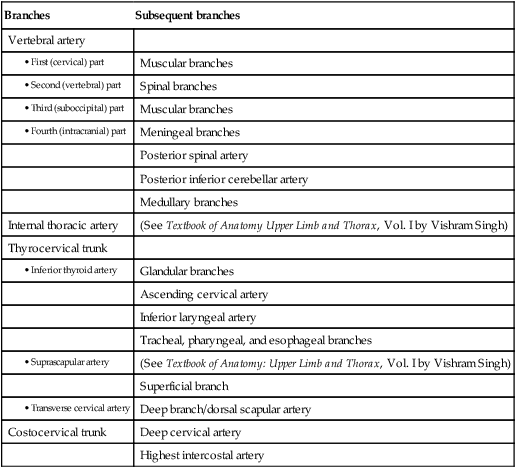
The branches of subclavian artery and their subsequent branches are summarized in Table 16.1.
Table 16.1
Summary of branches of the subclavian artery and their subsequent branches
| Branches | Subsequent branches |
| Vertebral artery | |
| Muscular branches | |
| Spinal branches | |
| Muscular branches | |
| Meningeal branches | |
| Posterior spinal artery | |
| Posterior inferior cerebellar artery | |
| Medullary branches | |
| Internal thoracic artery | (See Textbook of Anatomy Upper Limb and Thorax, Vol. I by Vishram Singh) |
| Thyrocervical trunk | |
| Glandular branches | |
| Ascending cervical artery | |
| Inferior laryngeal artery | |
| Tracheal, pharyngeal, and esophageal branches | |
| (See Textbook of Anatomy: Upper Limb and Thorax, Vol. I by Vishram Singh) | |
| Superficial branch | |
| Deep branch/dorsal scapular artery | |
| Costocervical trunk | Deep cervical artery |
| Highest intercostal artery |
COMMON CAROTID ARTERIES
There are two common carotid arteries: right and left. They are the chief arteries of the head and neck.
Origin (Fig. 16.1)
The right common carotid artery arises in neck from brachiocephalic trunk (innominate artery) behind the sternoclavicular joint.
The left common carotid artery arises in thorax (superior mediastinum) directly from the arch of aorta. It ascends to the back of left sternoclavicular joint and enters the neck.
Course, Termination, and Relations
In the neck, both arteries (right and left) have similar course. Each artery runs upwards from sternoclavicular joint to the upper border of the lamina of thyroid cartilage (opposite the disc between the 3rd and 4th cervical vertebrae), where it terminates by dividing into internal and external carotid arteries. The internal carotid artery is considered as a continuation of common carotid artery. They are named as internal and external because the former supplies structures within the skull and latter supplies structures outside the skull.
Each common carotid artery lies in front of transverse processes of lower four cervical vertebrae under the cover of anterior border of the sternocleidomastoid muscle.
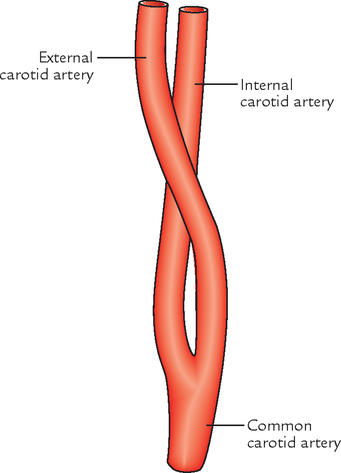
External Carotid Artery (Fig. 16.9)
It is one of the two terminal branches of the common carotid artery and supplies the structures external to the head and in front of the neck.
Course and Relations
The external carotid artery extends upwards from the level of upper border of the lamina of the thyroid cartilage to a point behind the neck of the mandible, where it terminates in the substance of the parotid gland by dividing into the superficial temporal and maxillary arteries.
The external carotid artery has a slightly curved course so that it is anteromedial to the internal carotid artery in its lower part and anterolateral to the internal carotid artery in its upper part (Fig. 16.9).
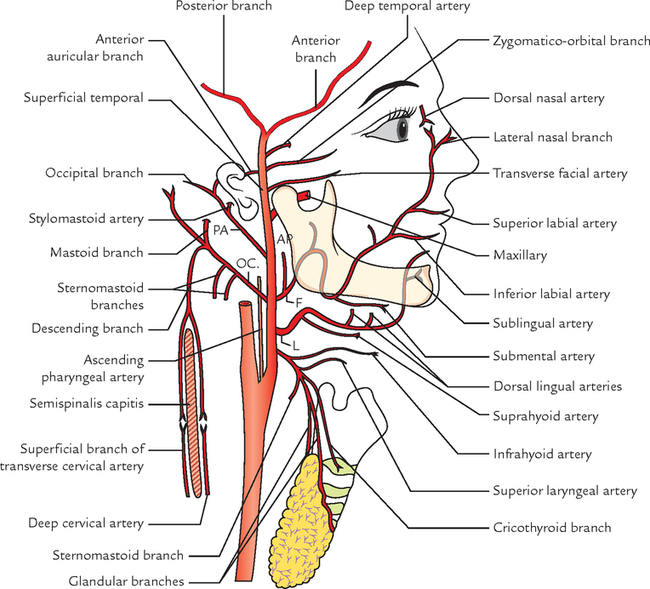
Branches (Fig. 16.10)
The external carotid artery gives rise to eight branches as follows:

The first three arteries arise from anterior aspect, next two from posterior aspect, and next one from medial aspect. The last two are terminal branches.
The branches of the external carotid artery are eight in number (Mnemonic – the term EXTERNAL consists of 8 letters: 1, 2, 3, 4, 5, 6, 7, 8, which correspond to the number of branches of the external carotid artery).
1. Superior thyroid artery: It arises from the front of external carotid artery just below the tip of the greater cornu of the hyoid bone. It runs downwards and forwards, parallel and superficial to the external laryngeal nerve to reach the upper pole of the thyroid gland, which it supplies.
Branches (Fig. 16.11)
(a) Infrahyoid branch, which anastomoses with its fellow of opposite side.
(b) Sternomastoid branch to the sternomastoid muscle.
(c) Superior laryngeal artery accompanies the internal laryngeal nerve, passes deep to the thyrohyoid muscle and pierces the thyrohyoid membrane to supply the larynx.
(d) Cricothyroid branch, passes across the cricothyroid ligament and anastomoses with its counterpart of the opposite side.
(e) Glandular branches to the thyroid gland; one of which anastomoses with its fellow of the opposite side along the upper border of the isthmus of the thyroid gland.
2. Lingual artery: It arises from the front of the external carotid artery opposite the tip of the greater cornu of the hyoid bone. It is the main artery to supply blood to the tongue. It may arise in common with the facial artery (linguofacial trunk).
It is divided into three parts by the hyoglossus muscle, viz.
(a) First part lies in the carotid triangle and forms a characteristic loop with convexity upwards above the greater cornu. The loop is crossed superficially by the hypoglossal nerve. The loop permits free movement of the hyoid bone.
(b) Second part lies deep to the hyoglossus muscle along the upper border of the hyoid bone.
(c) Third part (also called arteria profunda linguae) or deep lingual artery first runs upwards along the anterior border of the hyoglossus muscle and then forwards on the undersurface of the tongue, where it anastomoses with its fellow of opposite side.
(a) From first part—suprahyoid branch. It anastomoses with its fellow of opposite side.
(b) From second part—dorsal linguae branches usually two in number, to the dorsum of tongue and tonsil.
(c) From third part—sublingual artery, to the sublingual gland.
3. Facial artery (formerly called external maxillary artery): It arises from the front of the external carotid artery just above the tip of the greater cornu of the hyoid bone.
It is divided into two parts—cervical and facial:
(a) Cervical part of the facial artery ascends deep to the digastric and stylohyoid muscles, passes deep to the ramus of mandible where it grooves the posterior border of the submandibular gland. Then it makes S-shaped bend, first bending down (with convexity upwards) over the submandibular gland, and then up (with convexity downwards) over the base of the mandible.
(b) Facial part of the facial artery begins where the facial artery winds around the lower border of the body of the mandible at the anteroinferior angle of the masseter. (It has already been described on ![]() page 63).
page 63).
From the cervical part (branches in the neck)
(a) Ascending palatine artery arises near the origin of facial artery, ascends, and accompanies the levator palati, passes over the upper border of the superior constrictor and supplies mainly the palate.
(b) Tonsillar artery (main artery of tonsil) pierces the superior constrictor and ends in the tonsil.
(c) Glandular branches supply the submandibular gland.
(d) Submental artery, a large artery which runs forwards on the mylohyoid muscle in company with mylohyoid nerve. It supplies the mylohyoid muscle and submandibular and sublingual salivary glands.
4. Occipital artery: It arises from the posterior aspect of the external carotid artery at the same level as the facial artery. It runs backwards and upwards under cover of lower border of the posterior belly of digastric muscle superficial to internal carotid artery, internal jugular vein, and last four cranial nerves, crosses the apex of the posterior triangle. Then it runs deep to the mastoid process grooving the lower surface of the temporal bone medial to the mastoid notch. It crosses the superior oblique and semispinalis capitis and apex of suboccipital triangle to reach underneath the trapezius muscle, which it pierces 2.5 cm away from the midline and comes to lie just lateral to the greater occipital nerve. It supplies most of the back of the scalp.
(a) Sternomastoid branches are usually two in number. They run downwards and backwards, and supply the sternocleidomastoid. The upper one accompanies the spinal accessory nerve and lower one is hooked by the hypoglossal nerve.
(b) Mastoid branch enters the cranial cavity through mastoid foramen and supplies mastoid air cells.
(c) Meningeal branches enter the cranial cavity through jugular foramen and hypoglossal canal to supply dura mater of posterior cranial fossa.
(d) Muscular branches supply adjoining muscles.
(e) Auricular branch (occasional) supplies the cranial surface of the auricle.
(f) Descending branch divides into superficial and deep branches. The superficial branch anastomoses with the superficial branch of transverse cervical artery and deep branch anastomoses with the deep cervical artery—a branch of the costocervical trunk of subclavian artery on the superficial and deep surfaces of the semispinalis capitis, respectively.
• The hypoglossal nerve hooks the occipital artery under its site of origin.
• The upper sternomastoid branch of occipital artery accompanies the spinal accessory nerve and the lower sternomastoid branch crosses the hypoglossal nerve.
• Occipital artery crosses the apical part of the posterior triangle.
5. Posterior auricular artery: It arises from the posterior aspect of the external carotid artery a little above the occipital artery. It crosses superficial to the stylohyoid muscle. It runs upwards and backwards parallel to the occipital artery along the upper border of the posterior belly of digastric muscle and deep to the parotid gland. Then it becomes superficial and lies on the base of mastoid process behind the ear which it supplies.
(a) Stylomastoid artery enters the stylomastoid foramen to supply middle ear, mastoid air cells, and facial nerve.
(b) Auricular branch supplies both cranial and lateral surfaces of the auricle.
(c) Occipital branch, supplies scalp above and behind the auricle.
6. Ascending pharyngeal artery: It is a slender artery that arises from the medial aspect of the external carotid artery near its lower end. It runs vertically upwards between the side wall of the pharynx and internal carotid artery up to the base of the skull.
(a) Pharyngeal and prevertebral branches to corresponding muscles.
(b) Meningeal branches, which traverse foramina in the base of the skull.
(c) Inferior tympanic, which supplies medial wall of tympanic cavity.
(d) Palatine branches, which accompany levator veli palatini to the palate.
7. Superficial temporal artery: It is the smaller but more direct terminal branch of the external carotid artery. It begins behind the neck of the mandible deep to the upper part of the parotid gland. It runs vertically upwards crossing the root of zygoma in front of the tragus where its pulsation can be felt.
About 5 cm above the zygoma, it divides into anterior and posterior branches, which supply the temple and scalp.
(a) Transverse facial artery runs forwards across the masseter below the zygomatic arch.
(b) Anterior auricular branch, supplies the lateral surface of auricle and external auditory meatus.
(c) Zygomatico-orbital artery runs forwards along the upper border of zygomatic arch between two layers of temporal fascia and reaches the lateral angle of the eye.
(d) Middle (deep) temporal artery runs on the temporal fossa deep to temporalis muscle and supplies temporalis muscle and fascia.
(e) Anterior (frontal) and posterior (parietal) terminal branches.
The anterior branch supplies the muscles and skin of the frontal region. It is very tortuous and anastomoses with the branches of the ophthalmic artery. The posterior branch supplies skin and the auricular muscles.
8. Maxillary artery: It is the larger terminal branch of the external carotid artery (see ![]() Chapter 10,
Chapter 10, ![]() page 136).
page 136).
Internal Carotid Artery
The internal carotid artery is one of the two terminal branches of the common carotid artery but it is more direct. It is considered as an upward continuation of the common carotid artery. It supplies structures inside the skull and in the orbit. It is the principal artery to supply the brain and eye.
It begins as the upper border of the lamina of thyroid cartilage at the level of the disc between C3 and C4 vertebrae and runs upwards to reach the base of the skull, where it enters the carotid canal in the petrous temporal bone. It emerges in the cranial cavity by passing through the upper part of the foramen lacerum. In the cranial cavity, it enters the cavernous sinus and pursues a tortuous course before it ends below the anterior perforated substance of the brain by dividing into the anterior and middle cerebral arteries.
Parts
For the sake of convenience, the course of the internal carotid artery is divided into the following four parts:
1. Cervical part: It ascends vertically upwards from its origin to the base of the skull to reach the lower end of carotid canal and lies on the front of transverse process of upper cervical vertebrae. In the neck, the internal carotid artery is enclosed in the carotid sheath along with the internal jugular vein and vagus nerve.
The lower part of the artery is superficial and located in the carotid triangle. The upper part is deeply located and lies deep to the posterior belly of digastric muscle, styloid process with structures attached to it, and parotid gland.
At the upper end, the internal jugular vein lies posterior to the internal carotid artery. Here the last four cranial nerves (glossopharyngeal, vagus, accessory, and hypoglossal) lie between the internal jugular vein and internal carotid artery.
In the neck, the internal carotid artery gives no branches.
2. Petrous part: The internal carotid artery enters the petrous part of the temporal bone in a carotid canal. It first runs upwards and then turns forwards and medially at the right angle. It emerges at the apex of petrous temporal bone in the posterior wall of foramen lacerum, and passes through its upper part to enter the cranial cavity.
(a) Caroticotympanic branches to middle ear, which anastomose with the anterior and posterior tympanic arteries.
(b) Pterygoid branch (small and inconstant) enters the pterygoid canal and anastomoses with the greater palatine artery.
3. Cavernous part: This part lies within the cavernous sinus. From foramen lacerum, the internal carotid artery ascends and enters the cavernous sinus. In the sinus, it passes forwards along the side of sella turcica in the floor and medial wall of the sinus. Here it lies outside the endothelial lining of the sinus and related to the abducent nerve inferolaterally.
In the anterior part of the sinus, the artery ascends and pierces the dural roof of the sinus between the anterior and middle clinoid processes to reach underneath the cerebrum.
(a) Cavernous branches to the trigeminal ganglion.
(b) Superior and inferior hypophyseal arteries to the hypophysis cerebri (pituitary gland).
4. Cerebral part: This part lies at the base of the brain. After emerging from the roof of the cavernous sinus, the artery turns backwards in the subarachnoid space along the roof of the cavernous sinus and lies below the optic nerve.
Finally it turns upwards by the side of the optic chiasma and reaches the anterior perforated substance of the brain located at the beginning of the stem of lateral sulcus of the cerebral hemisphere. Here it ends by dividing into anterior and middle cerebral arteries.
The branches of cerebral part of the internal carotid artery are described in detail in ![]() Chapter 29,
Chapter 29, ![]() page 407. The branches of internal carotid artery are summarized in Table 16.2.
page 407. The branches of internal carotid artery are summarized in Table 16.2.
Table 16.2
Summary of branches of the internal carotid artery
| Part | Branches |
| Cervical part | No branches |
| Petrous part | 1. Caroticotympanic branches |
| 2. Pterygoid branch | |
| Cavernous part | 1. Cavernous branches |
| 2. Superior and inferior hypophyseal arteries | |
| Cerebral part | 1. Ophthalmic artery |
| 2. Anterior choroidal artery | |
| 3. Posterior communicating artery Terminal branches | |
| 4. Anterior cerebral artery | |
| 5. Middle cerebral artery |
Carotid siphon: The U-shaped bend formed by the internal carotid artery while passing through and above the cavernous sinus is called carotid siphon. It probably dampens down the pulsations of the artery. The carotid siphon is an important feature to be seen in cerebral angiography.
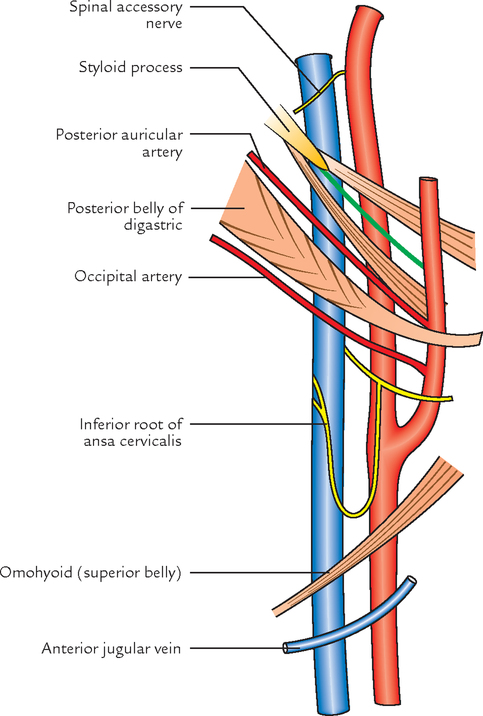
The structures passing between the external and internal carotid arteries are as follows (Fig. 16.12):

VEINS
The major veins draining the head and neck are subclavian, internal jugular, external jugular, and anterior jugular veins (Fig. 16.13). The internal jugular vein is the principal vein of the head and neck region for it drains the brain as well as most of the other tissues of the head and neck. The external jugular vein drains only a portion of extracranial tissues.

The valves in the lumen are mostly absent in the veins draining head and neck area, unlike in the rest of the body. This leads to two-way flow of blood dictated by local pressure changes. For this reason, infections in the head and neck area can lead to serious complications.
SUBCLAVIAN VEIN
It is the continuation of axillary vein and extends from the outer border of the first rib to the medial border of the scalenus anterior, where it joins the internal jugular vein to form brachiocephalic vein (Fig. 16.13). The subclavian vein is principally the vein of the upper limb.
The subclavian vein forms an arch across the pleura at a level below the arch of the subclavian artery. The two arches are separated from each other by the scalenus anterior.
It seldom rises above the level of the clavicle and possesses a pair of valves about 2 cm from its termination.
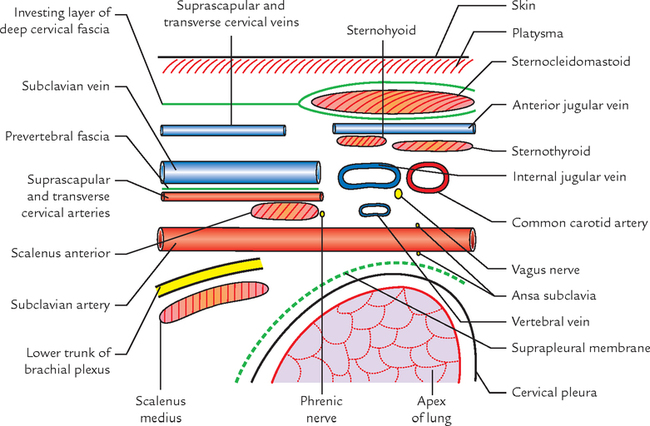
Relations (Fig. 16.14)
In front: Clavicle and subclavius muscle.

Behind: Subclavian artery with intervening scalenus anterior muscle and phrenic nerve.

INTERNAL JUGULAR VEIN
The internal jugular vein is usually the largest vein in the neck. It begins as the direct continuation of the sigmoid sinus at the base of the skull below the jugular foramen and descends vertically downwards to end behind the sternal end of the clavicle by joining the subclavian vein to form the brachiocephalic vein. The internal jugular vein drains brain and most of the tissues of the head and neck (Fig. 16.15).

N.B. The right internal jugular vein is usually larger than the left because it drains the blood from the larger superior sagittal sinus, c.f. the left internal jugular vein drains blood from the smaller inferior sagittal sinus.
Special Features
1. It presents two dilatations:
• First, at its commencement, which lies in the jugular fossa of the temporal bone. It is known as superior bulb and is related to the floor of the middle ear.
• Second, close to its termination, which lies in the lesser supraclavicular fossa between the sternal and clavicular heads of sternocleidomastoid. It is known as inferior bulb and is guarded by a pair of valves.
2. It is vertically applied to the lateral side of the internal and common carotid arteries, enclosed with them and the vagus nerve in the facial sheath called carotid sheath.
3. The deep cervical lymph nodes lie along its entire course.
4. It is remarkably constant in position and can be marked on the surface by a vertical line extending from midpoint between the tip of the mastoid process and the angle of the mandible, to the sternoclavicular joint.
N.B. At the lower end, both the internal jugular veins (right and left) tend to shift to the right, so that the right comes to lie further lateral to the right common carotid artery while the left tends to overlap the left common carotid artery.
Relations
From above downwards, these are (Fig. 16.16) as follows:
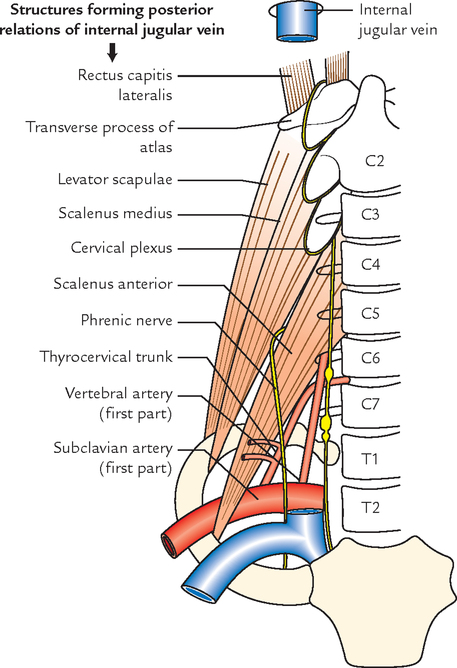
2. Transverse process of atlas.
4. Scalenus medius and cervical plexus.
5. Scalenus anterior and phrenic nerve.
6. Thyrocervical trunk and first part of vertebral artery.
7. First part of the subclavian artery.
8. Thoracic duct on the left side.
9. The sternocleidomastoid overlaps the upper part and covers the lower part of the vein.
Superficial (anterolateral; Fig. 16.17):
Tributaries (Fig. 16.15)
1. Inferior petrosal vein—is usually the first tributary and joins the internal jugular vein immediately below the jugular foramen.
In addition to the above mentioned tributaries, the right lymphatic duct on the right side and thoracic duct on the left side, usually open into internal jugular vein or into the junction between the internal jugular vein and the subclavian vein.
N.B. In the upper part of the neck internal jugular vein may communicate with the external jugular vein by an oblique jugular vein across the anterior border of sternocleidomastoid muscle.
The anterior jugular and external jugular veins are described in detail in ![]() Chapter 4.
Chapter 4.
CAROTID SHEATH
The carotid sheath extends from the base of the skull above to the arch of the aorta below. At the upper end it is attached to the margins of carotid canal and the jugular fossa.
The upper part of the carotid sheath contains internal carotid artery, internal jugular vein, and last four cranial nerves (Fig. 16.18). Medial to it lies pharynx, lateral to it lies styloid apparatus, anterior to it lies infratemporal fossa, and posterior to it lies cervical sympathetic trunk on the prevertebral fascia.

The lower part of carotid sheath contains common carotid artery, internal jugular vein, and vagus nerve.
STYLOID APPARATUS
The styloid apparatus consists of styloid process and structures attached to it.
The structures attached to styloid process (Fig. 16.19) are:

The five elongated structures attached to styloid process resemble the reins of a chariot. Two of these reins (ligaments) are non-adjustable, whereas the remaining three reins (muscles) are adjustable, with each being controlled by separate cranial nerve, e.g., stylohyoid, stylopharyngeus, and styloglossus are supplied by 7th, 9th, and 12th cranial nerves, respectively.
STYLOID PROCESS
The styloid process is long, slender, pointed bony process projecting anteroinferiorly from the inferior aspect of the temporal bone. Its length is variable, ranging from 2–3 mm to an average of 2.5 cm.
Its proximal part (tympanohyal) is ensheathed by the tympanic plate, while its muscles and ligaments are attached to its distal part (stylohyal). Its relation in vivo is important:
MUSCLES
Stylohyoid Muscle
It is a slender muscle extending from posterior surface of the styloid process to the hyoid bone at the junction between its body and greater cornu (for details see ![]() Chapter 9). It helps in controlling movements of the hyoid bone.
Chapter 9). It helps in controlling movements of the hyoid bone.
Styloglossus Muscle
It extends from anterior surface of the tip of the styloid process and adjoining part of the stylohyoid ligament to the side of the tongue. It pulls the tongue upwards and backwards (for details see ![]() Chapter 9).
Chapter 9).
Stylopharyngeus Muscle
It extends from medial side of the base of the styloid process to the posterior border of the lamina of the thyroid cartilage. It helps to elevate the larynx during swallowing and phonation (for details see ![]() Chapter 14).
Chapter 14).
LYMPHATIC DRAINAGE OF THE HEAD AND NECK
The knowledge of lymphatic drainage of the head and neck is extremely important because the cancers arising in this region have predictable patterns of spread through the chains of lymph nodes in the neck, which help the surgeons to remove the desired lymph nodes. The lymph nodes and other lymphoid tissues in the head and neck are often inflamed and produce swellings, which are examined by physicians in day-to-day practice. All the lymph from the region of head and neck drains into deep cervical lymph nodes either (a) directly from the tissues or (b) indirectly after passing through the outlying groups of lymph nodes.
The efferents from deep cervical nodes form the jugular trunk, which on the right side drains into the right lymphatic duct and on the left side into the thoracic duct. The right lymphatic duct and thoracic duct generally empty into the junction of the subclavian and internal jugular veins on their respective sides.
LYMPH NODES
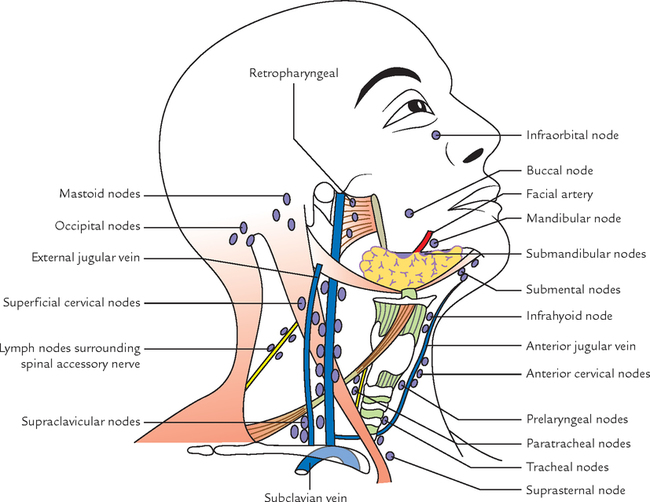
Out of total 800 lymph nodes in the body, about 300 lymph nodes are located in the region of the head and neck only. The lymph nodes in the region of the head and neck are broadly classified into two groups: peripheral and terminal (Fig. 16.20).
PERIPHERAL LYMPH NODES
Peripheral lymph nodes (also called outlying lymph nodes). They are usually found in groups, which are arranged in outer and inner circles (Fig. 16.21):
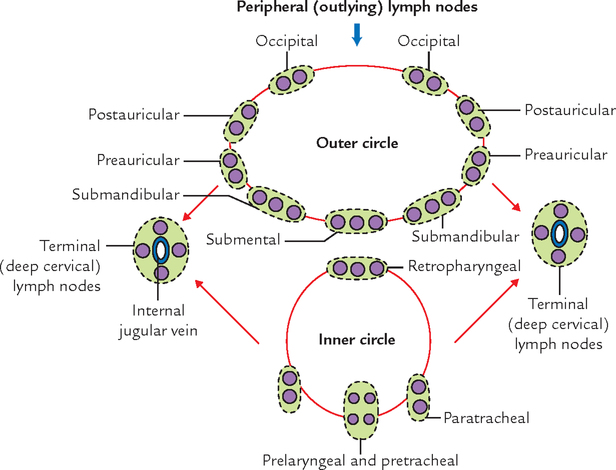
1. Outer circle: It is formed by lymph node groups, which form the pericervical or cervical collar at the junction of the head and neck (craniocervical junction) and extends from chin in front to the occiput behind. They include submental, submandibular, superficial parotid (preauricular), mastoid (postauricular), and occipital nodes.
Outlying extensions of lymph node groups of pericervical collar:
(a) Facial nodes: These are extensions of submandibular nodes and include:
• a small buccal node lying on the lateral surface of the buccinator along the facial vein.
• a small mandibular node which is frequently present where facial vessels cross the lower border of the mandible.
(b) Superficial cervical nodes: They are situated superficial to sternomastoid (upper part) along the external jugular vein. These are the extensions of parotid nodes.
(c) Anterior cervical nodes: They are situated along the anterior jugular vein. One member of this group frequently lies in the suprasternal space (suprasternal node). They are extensions of submental lymph nodes.
2. Inner circle: The inner circle is formed by following lymph node groups, which lie deep to the investing layer of deep cervical fascia (Fig. 16.21):
(a) Infrahyoid nodes: These lie in front of thyrohyoid membrane.
(b) Prelaryngeal nodes: These are situated in front of the conus elasticus or cricothyroid membrane.
(c) Pretracheal lymph nodes: These lie in front of trachea below the isthmus of thyroid gland.
3. Paratracheal nodes: These nodes flank the trachea and esophagus on either side along the recurrent laryngeal nerves.
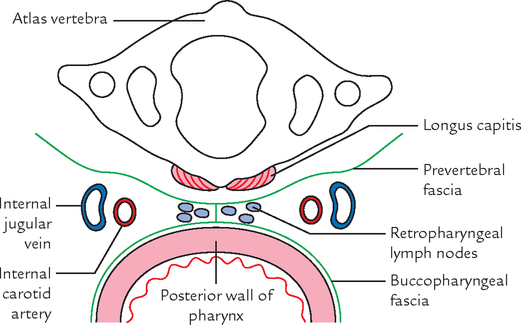
4. Retropharyngeal lymph node: These lie posterior to pharynx and in front of prevertebral fascia in the retropharyngeal space (Fig. 16.22).
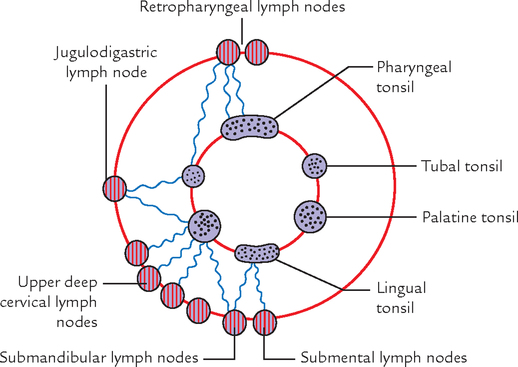
Deep to inner circle, there is a submucosal ring of aggregated masses of lymphoid tissue called tonsils, which surround the commencement of air and food passages. These together constitute the Waldeyer’s lymphatic ring (Fig. 16.23). The lymph from lymphoid tissue of this ring drains into pericervical chain and deep cervical chain, which constitutes the external ring of Waldeyer.
TERMINAL LYMPH NODES
These are deep cervical lymph nodes that lie along and around the internal jugular vein, some within the carotid sheath and some on the surface of the sheath, under cover of sternocleidomastoid.
For the convenience of description deep cervical lymph nodes are divided into upper and lower groups (superior and inferior deep cervical nodes), though there is no clear demarcation between them:
1. Superior group of deep cervical lymph nodes: They lie above the omohyoid. One lymph node of this group is situated below the posterior belly of digastric between the angle of the mandible and anterior border of the sternocleidomastoid in the triangle formed by posterior belly of digastric, facial vein, and internal jugular vein. It is called jugulodigastric node.
It drains the lymph primarily from the palatine tonsil. Therefore it is also termed lymph node of the tonsil. When enlarged due to pathology in the palatine tonsil, it is easily palpable behind and below the angle of the mandible.
2. Lower group of deep cervical lymph nodes: One of the lymph nodes of this group lies above the intermediate tendon of omohyoid posterior to the internal jugular vein. It is called jugulo-omohyoid lymph node. Since this lymph node drains lymph primarily from the tongue, it is termed lymph node of the tongue. This node lies deep to sternocleidomastoid, and therefore, can be palpated only if enlarged considerably.
Some nodes of this group extend into the supraclavicular fossa and are related to brachial plexus and subclavian vessels. These are termed supraclavicular lymph nodes (Virchow’s lymph nodes). The left supraclavicular lymph nodes are clinically important because they are common site of metastasis from malignant disease (cancer) of the stomach. The testicular and esophageal cancers can also metastasize in these nodes. The Virchow’s lymph nodes are often palpable in cancer stomach. One or two lymph nodes of this group lie in contact with accessory nerve at a higher level in the posterior triangle.
 Chief arteries of the head and neck Chief arteries of the head and neck |
Right and left common carotid arteries |
| Chief veins of the head and neck |
Right and left internal jugular veins |
| All the branches of subclavian artery (generally) arise from its first part except |
Costocervical trunk on the right side which arises from second part of that side |
| Largest branch of the first part of the subclavian artery |
Vertebral artery |
| Shortest branch of the subclavian artery |
Thyrocervical trunk |
| Most superficial part of the subclavian artery |
Third part |
| Most constant pulse in the body |
Carotid pulse |
| Anesthetist’s artery |
Superficial temporal artery |
| All the lymph node groups of pericervical collar are paired except |
Submental group of lymph nodes which is unpaired |
| Lymph node of tonsil |
Jugulodigastric lymph node |
| Lymph node of tongue |
Jugulo-omohyoid lymph node |


A 67-year-old man was keeping quite well until he suddenly developed weakness in his limbs on the right side. This lasted for about 12 hours and then improved spontaneously and he recovered completely after 24 hours. His family physician thought that he may have a transient ischemic attack of brain (cerebral stroke). He was referred to a neurocentre by his family physician for thorough check-up by a neurosurgeon. On examination, the surgeon heard a bruit at the level of origin of common carotid artery on the left side. The color Doppler ultrasound scan revealed more than 75% narrowing of the internal carotid artery at its origin. A carotid angiogram confirmed this narrowing.
1. At what level does the common carotid terminate by dividing into internal and external carotid arteries?
3. What are the main relations at the bifurcation of common carotid artery?
4. Why does a patient develop signs of a cerebral stroke if there is formation of atheroma in the internal carotid artery?
1. At the level of upper border of lamina of the thyroid cartilage.
2. It is a noise of blood flow produced when it passes through a narrowed vessel.
3. The common carotid artery is present in the carotid sheath containing internal jugular vein laterally and vagus nerve between and behind the artery and vein. The cervical sympathetic chain lies behind the carotid sheath on prevertebral fascia.
4. A portion of atheroma gets detached, and enters the middle cerebral artery and blocks it. This leads cerebral ischemia. Consequently, the patient develops the signs of cerebral stroke.