Chapter 10
Microbial Infection
Introduction
Host–parasite relationship is determined by the interaction between host factors and the infecting microorganisms. Outcome of any microbial infection depends on the interaction between the host and the parasite. The relationship of existence between the host and parasite may be (1) symbiosis, (2) commensalism or (3) disease process:
• Symbiosis describes a situation where both the microorganisms and host species live together with mutual benefit. There is an element of symbiosis in the relationship between the human host and the gut flora.
• Commensalism is an association in which only the microorganism derives benefit, without causing any injury to the host. Most human microbes are commensals.
• Disease is caused by certain microorganisms known as pathogens. Microorganisms vary in their ability to cause disease in humans.
Types of Microorganisms
Microorganisms may be of the following types:
1. Saprophytes: These are free-living microorganisms that live on dead or decaying organic matter. They are usually present in soil and water. They are generally unable to invade the living body.
2. Parasites: These are microorganisms that live on a living host and derive nutrition from the host without any benefit to the host and causes harm to the infected host.
3. Commensals: These are microorganisms that live on a living host without causing any injury to the host. Most human microbes are commensals.
4. Pathogens: A microorganism capable of causing disease, especially if it causes disease in immunocompetent people, is called as a pathogen. These pathogens, however, represent a very small proportion of the microbial species.
5. Opportunistic pathogens: A microbe that is capable of causing disease only in immunocompromised people is known as opportunistic pathogen. These organisms can cause disease only if one or more of the usual defence mechanisms of humans are reduced or altered by accident, by intent (e.g., surgery) or by an underlying metabolic disorder or an infectious disease (e.g., AIDS).
Infection
This is a process when an organism enters the body, increases in number and causes damage to the host. All infections do not invariably result in the disease.
The term infection has more than one meaning: (1) the presence of microbes in the body and (2) the symptoms of the disease. The presence of microbes in the body does not always result in symptoms of the disease. Bacteria cause symptoms of disease by two main mechanisms: (1) production of toxins, both endotoxin and exotoxin and (2) production of inflammation.
The words virulence and virulent are derived from the Latin word virulentus, meaning ‘full of poison.’ The term virulentus is derived from the Latin words virus (poison) and lentus (fullness), and, in turn, the term virus may be related to the Sanskrit word visham, meaning ‘poison.’ The virulence of a microbe is determined by virulence factors, such as capsules, exotoxins or endotoxins (Table 10-1).
Table 10-1
Important Bacterial Surface Virulence
| Virulence Factors | Bacteria |
|
Capsule |
|
| Polysaccharide capsule | Streptococcus pneumoniae Klebsiella pneumoniae Haemophilus pneumonia Salmonella Typhi Neisseria meningitidis |
| Polypeptide capsule | Bacillus anthracis |
| Pili protein | Escherichia coli |
| Protein A | Staphylococcus aureus |
| M protein | Streptococcus pyogenes |
| V and W proteins | Yersinia pestis |

The diseases that can be spread from one person to another are called communicable diseases. Most microbial infections are communicable diseases. Three epidemiological terms are often used to describe infection: endemic, epidemic and pandemic.
• Endemic: The infection that occurs at a persistent, usually low level in a certain geographical area is called endemic.
• Epidemic: The infection that occurs at a much higher rate than usual is known as epidemic.
• Pandemic: Infection that spreads rapidly over large areas of the world is known as a pandemic.
Types of Infections
Infections may be of the following types:
• Primary infection: This condition denotes an initial infection with an organism in a host.
• Re-infection: This condition denotes subsequent infection with the same organism in the same host.
• Secondary infection: This condition denotes an infection with a new organism in a host whose body resistance is already lowered by a pre-existing infectious disease.
• Cross-infection: This condition denotes an infection with a new organism from another host or another external source in a patient who is already suffering from a disease.
• Nosocomial infection: Cross-infections acquired in hospitals are called hospital-acquired, hospital-associated or nosocomial infections.
• Iatrogenic infection: This condition denotes a physician-induced infection as a result of therapy with drugs or investigation procedures.
• Sub-clinical infection: Inapparent clinical infections are called sub-clinical infections.
• Latent infections: This denotes a condition in which some organisms may remain in a latent or hidden stage in host and subsequently they multiply to produce clinical disease when host resistance is lowered.
Stages of Pathogenesis of Infections
Infectious diseases are complex. The outcome of infection depends on a variety of factors of the microbe and host as follows:
1. The ability of the organism to break host barriers and evade destruction by innate local and tissue host defences.
2. The ability of the organism to replicate, spread, establish infection and cause disease.
3. The ability of the organism to transmit to a new susceptible host.
4. The innate and adaptive immunologic ability of the host to control and eliminate the invading microorganism.
The infection process involves the following stages: (1) transmission of infection, (2) entry of the organisms and evasion of the local defences, (3) adherence to cell surfaces, (4) growth and multiplication of the bacteria at the site of adherence, (5) manifestations of disease and (6) termination of disease.
Transmission of Infection
There are three important components that play an important role in successful transmission of microbial diseases. These are (1) sources, (2) mode of transmission and (3) susceptible host.
Sources of Infection
Sources of microbial infections are human, animal, plant, soil or inanimate matter in which organisms usually live, multiply and cause the infections with or without overt clinical manifestations. Humans are usually the common reservoirs of many of the microbial infections. Animals are reservoirs of zoonotic infections, such as plague (e.g., rats), rabies (e.g., dogs), cysticercosis (e.g., pigs), etc.
The sources of infections may be endogenous and exogenous:
• Endogenous sources: The source of infection is the normal bacterial flora present in the human body. These bacteria are usually non-pathogenic but in certain situations become pathogenic and cause infections at different sites in the same host. For example, Escherichia coli present as normal flora of the intestine may cause urinary tract infection in the same host. Similarly, viridans streptococci present as a part of the normal flora of the mouth may cause infective endocarditis.
• Exogenous sources: The source of infection is from outside the host’s body. Most of the microbial infections are exogenous in nature. The exogenous sources include the following:
1. Humans: Humans are the most common sources of infections caused by the microorganisms. They may be either patients or carriers. The patient suffering from an active infection is an important source of infection to others.
A carrier is a person who harbours pathogenic microorganisms without showing any signs and symptoms of disease. Carriers are also important sources of infections. A carrier may be (1) healthy carrier, (2) convalescent carrier, (3) temporary carrier and (4) chronic carrier.
a. Healthy carrier is the host who harbours the microorganism without ever suffering from the disease caused by that microorganism.
b. Convalescent carrier is the host who continues to harbour the microorganism even after recovering from the clinical disease caused by the same pathogen.
c. Temporary carrier is the host who harbours the microorganism up to 6 months after recovering from the disease caused by the same pathogen.
d. Chronic carrier is the host who harbours the microorganism for many years after recovering from the clinical disease caused by the same pathogen.
2. Animals: Animals are also important sources of infection for humans. The symptomatic as well as asymptomatic animals can transmit infections to humans. Asymptomatic animals act as a reservoir of human infections. These are called as reservoir hosts. Infections transmitted from animals to humans are called zoonotic infections.
The examples of zoonotic infections include bacterial (e.g., plague, anthrax, bovine tuberculosis, etc.), viral (e.g., rabies, Japanese encephalitis, etc.), fungal (e.g., dermatophytic infections) and parasitic (e.g., toxoplasmosis, cysticercosis, hydatid disease, etc.).
3. Insects: Insects, such as mosquitoes, ticks, mites, flies, fleas and lice may transmit a wide variety of microorganisms to the humans (Table 10-2). The diseases transmitted by the insects are collectively referred to as arthropod-borne diseases and the insects transmitting these pathogens are called vectors. Insect vectors may transmit the infection in two ways: mechanical transmission and biological transmission.
a. Mechanical vectors: Insects (e.g., domestic flies) carry enteric bacteria (Salmonella typhi, Shigella spp., etc.) mechanically on their legs, wings and surface of the body and transfer them to food.
b. Biological vectors: These are the vectors in which the microorganisms multiply or undergo a part of their life cycle before being transmitted to humans. Rat flea and female Anopheles mosquitoes are the examples of biological vectors that transmit plague and malaria, respectively, to humans by biting.
Insects, besides acting as vectors, also act as reservoir hosts (e.g., ticks in relapsing fever).
4. Food: Food items contaminated with pathogens also act as source of infection and cause diarrhoea, dysentery, food poisoning and gastroenteritis.
5. Water: Water contaminated with microorganisms also acts as a source of infection and transmits water-borne diseases, such as leptospirosis, cholera, dysentery, hepatitis A infection, etc.
Table 10-2
Microbial Diseases Transmitted by Insects
| Organism | Disease | Reservoir | Insect |
|
Bacteria |
|||
| Yersinia pestis | Plague | Rodents, especially rats | Rat fleas |
| Francisella tularensis | Tularaemia | Rabbits and other rodents | Ticks |
| Borrelia recurrentis | Relapsing fever | Humans | Lice |
| Borrelia burgdorferi | Lyme disease | Rodents and deer | Ixodes ticks |
| Rickettsia rickettsii | Rocky mountain spotted fever | Dogs, rodents, and ticks | Ticks |
| Rickettsia prowazekii | Epidemic typhus | Humans | Lice |
| Ehrlichia chaffeensis | Ehrlichiosis | Deer and rodents | Ticks |
|
Parasites |
|||
| Leishmania spp. | Leishmaniasis | Humans, dogs, and wild canine | Sandfly (Phlebotomus) |
| Trypanosoma spp. | Trypanosomiasis | Humans, armadillos, antelope, and cattle | Reduviid bug, tsetse fly |
| Plasmodium spp. | Malaria | Humans | Anopheles mosquitoes |
| Wuchereria bancrofti and Brugia malayi | Filaria | Humans | Mosquitoes (Culex, Aedes, Mansonia spp.) |
|
Viruses |
|||
| Japanese encephalitis virus | Japanese encephalitis | Birds | Culex tritaeniorhynchus mosquitoes |
| West Nile virus | West Nile fever | Birds | Culex mosquitoes |
| Chikungunya virus | Chikungunya | Humans and monkeys | Aedes aegypti mosquitoes |
| Dengue virus | Dengue | Humans | Aedes aegypti mosquitoes |
| Kyasanur forest disease virus | Kyasanur forest disease | Forest birds and small mammals | Tick |
| Yellow fever virus | Yellow fever | Monkeys and humans | Aedes aegypti mosquitoes |

Methods of Transmission
Microbial pathogens causing various infectious diseases are transmitted from one host to another by many ways: (1) contact, (2) inoculation, (3) ingestion, (4) inhalation and (5) vectors (Table 10-3).
1. Contact: Transmission of microorganisms from person to person occurs by direct or indirect contact. Transmission by direct contact occurs through the acts of touching, kissing, sex, etc. The diseases transmitted by direct contact include common cold, staphylococcal infections and sexually transmitted infections (e.g., gonorrhoea, syphilis, AIDS, etc.). The term contagious disease was used earlier for the disease acquired by direct contact.
Microorganisms can also be transmitted by indirect contact through inanimate objects, such as clothings, handkerchief, toys, etc., called fomites. Influenza, tuberculosis and certain superficial fungal infections are examples of diseases transmitted by fomites.
2. Inoculation: Infections can be transmitted by inoculation of microorganisms directly into tissues of the host. For example, tetanus is transmitted by direct inoculation of Clostridium tetani spores present in soil to the injured tissues in the host. These spores then germinate to vegetative forms of bacteria and migrate along the neural tissues to cause tetanus. Similarly, rabid dogs through their act of biting inoculate rabies virus directly to host tissue and cause rabies in humans.
Iatrogenic infection occurs following the use of un-sterile syringes and equipment in a hospital. Hepatitis B and C and HIV infections are the examples of iatrogenic infections caused by use of contaminated syringes and that of contaminated blood and blood products.
3. Ingestion: Ingestion of water and food contaminated with microorganisms can transmit a wide variety of microbial infections. For example, food poisoning caused by Bacillus cereus is transmitted by rice contaminated with bacterial spores that survive boiling. Cholera, typhoid, food poisoning, hepatitis A, poliomyelitis and many parasitic infections are the other examples of diseases transmitted by ingestion of contaminated food and water.
4. Inhalation: Infections are transmitted by inhalation of droplet nuclei that are discharged into the air by coughing, sneezing or talking. Respiratory pathogens are shed into the environment by patients in secretions from the nose or throat during coughing, sneezing or talking. Small droplets (less than 0.1 mm in diameter) become airborne as minute particles or droplet nuclei (1–10 μm in diameter), whereas large droplets fall down to the ground.
Measles, influenza, whooping cough, tuberculosis, aspergillosis, etc. are few examples of infectious diseases acquired by inhalation.
5. Vectors: Mosquitoes, flies, fleas, ticks, mite and lice are the vectors that transmit many diseases as mentioned earlier.
Table 10-3
Different Modes of Transmission
| Modes of Transmission | Disease | Causative Agents |
|
Human to human |
||
| Direct contact | Gonorrhoea | Neisseria gonorrhoeae |
| Indirect contact | Dysentery | Shigella dysenteriae |
| Blood-borne | Syphilis | Treponema pallidum |
| Trans-placental | Congenital syphilis | Treponema pallidum |
|
Nonhuman to human (animal origin) |
||
| Direct contact | Cat-scratch disease | Bartonella henselae |
| Lyme disease | Borrelia burgdorferi | |
| Through animal excreta | Haemolytic uraemic syndrome | Enterohemorrhagic Escherichia coli (EHEC) |
| Handling of fomites | Skin infection | Staphylococcus aureus |
| Soil borne | Tetanus | Clostridium tetani |
| Water borne | Legionnaire disease | Legionella pneumophila |

Susceptible Host
The infective agent enters the body by four main routes: (1) genital tract, (2) respiratory tract, (3) gastrointestinal tract and (4) skin. The pathogens can be transmitted either as vertical or horizontal transmission.
Vertical transmission: Certain bacteria (Treponema pallidum), viruses (rubella and cytomegalovirus) and parasites (Toxoplasma gondii) can be transferred from mother to foetus by a process called vertical transmission (Table 10-4). The organisms can be transmitted vertically by three ways:
1. across the placenta,
2. within birth canal during birth and
3. through breast milk.
Table 10-4
Vertical Transmission of Microbial Agents
| Modes of Transmission | Organism | Disease |
|
Breast milk |
||
| Bacteria | Staphylococcus aureus | Skin or oral infection |
| Viruses | Human T-cell leukaemia virus | Asymptomatic |
Cytomegalovirus Human immunodeficiency virus (HIV) |
Asymptomatic infection | |
|
During passage through birth canal |
||
| Bacteria | Group B streptococcus | Neonatal sepsis and meningitis |
| Neisseria gonorrhoeae | Conjunctivitis | |
| Chlamydia trachomatis | Pneumonia or conjunctivitis | |
| Viruses | HIV | Asymptomatic infection |
| Hepatitis B virus | Hepatitis B | |
| Herpes simplex virus-2 | Skin or CNS infection; sepsis | |
|
Transplacental |
||
| Bacteria | Listeria monocytogenes | Neonatal sepsis and meningitis |
| Treponema pallidum | Congenital syphilis | |
| Viruses | Cytomegalovirus | Congenital abnormalities |
| Parvovirus B19 | Hydrops fetalis | |
| Parasite | Toxoplasma gondii | Congenital toxoplasmosis |

Table 10-4 summarises a list of diseases transmitted vertically.
Horizontal transmission: Unlike vertical transmission, horizontal transmission occurs from person to person and is not from mother to offspring (Fig. 10-1).

Fig. 10-1 Schematic diagram showing horizontal and vertical transmission of infections.
Entry of Organisms and Evasion of Local Defences
Skin, mucus, ciliated epithelium and secretions containing antibacterial substances (e.g., lysozyme) are the natural barriers of the human and animal hosts that prevent microbial entry. However, these barriers are sometimes broken (e.g., a break in the skin, an ulcer in the intestine, or a tumour, etc.), thereby allowing the entry of microbes into the host (Table 10-5). On entry, the microbes spread through blood circulation to other sites in the body (Fig. 10-2).
Table 10-5
Routes of Entry of Microbial Pathogens
| Portal of Entry | Bacteria | Virus | Fungi |
| Skin and mucus membrane | Clostridium tetani, Leptospira | Hepatitis B virus (HBV), human immunodeficiency virus (HIV) | Dermatophytes |
| Respiratory tract | Streptococcus pneumoniae, Neisseria meningitidis, Haemophilus influenzae, Mycobacterium tuberculosis | Rhinovirus, RSV (respiratory syncytial virus), Epstein–Barr virus, influenza virus | Cryptococcus neoformans, Histoplasma capsulatum, Pneumocystis jirovecii |
| Gastrointestinal tract | Shigella spp., Salmonella spp., Vibrio spp. | Hepatitis A or E virus, poliovirus | Candida albicans |
| Genital tract | Neisseria gonorrhoeae, Treponema pallidum | HIV, human papilloma virus | Candida albicans |


Fig. 10-2 Schematic diagram showing various stages of infection process.
Factors Predisposing to Microbial Pathogenicity
Pathogenicity is the capacity of a pathogen species to cause disease, whereas virulence is used to describe the sum of disease causing properties of a population (strain) within the species. Pathogens can be distinguished from their avirulent counterparts by the presence of specific genes or gene clusters in the genome known as pathogenicity islands.
Virulence is a measure of a microbe’s ability to cause disease. It is a quantitative measure of pathogenicity and is measured by the number of organisms required to cause disease. It means that a highly virulent microbe requires fewer organisms to cause disease than a less virulent one; hence it is directly dependent on the infectious dose of the organism.
The 50% lethal dose (LD50) is the number of organisms required to kill half of the hosts, whereas 50% infectious dose (ID50) is the number of microbes needed to cause infection in half of the hosts. The infectious dose of an organism required to cause disease varies among the pathogenic bacteria.
Bacteria cause diseases by four main mechanisms: (1) adhesions, (2) invasion of tissues followed by inflammation, (3) toxin production and (4) immunopathogenesis.
Table 10-6 summarises a list of bacteria with their virulence factors. The virulence depends upon following factors:
Table 10-6
Bacterial Virulence Factors
| Organism | Virulence Factors |
| Staphylococcus aureus | Coagulase, protein A |
| Streptococcus pyogenes | M protein |
| Streptococcus pneumoniae | Capsular polysaccharide |
| Enterococcus faecalis | Cytolysin, biofilm formation |
| Neisseria gonorrhoeae | Pili, opacity-associated proteins (Opa), IgA proteases |
| Neisseria meningitidis | Capsular polysaccharide |
| Bacillus anthracis | Capsule, oedema factor, lethal factor, protective antigen |
| Listeria monocytogenes | Internalin |
| Escherichia coli | Heat-labile and heat-stable enterotoxins, pili |
| Haemophilus influenzae | Capsular polysaccharide |
| Vibrio cholerae | Cholera toxin |
| Mycobacterium tuberculosis | Mycolic acid cell wall |
Adhesions: Adherence of bacteria to body surface is the most important event in the pathogenesis of disease. Once bacteria enter the body of the host, they must adhere to the cells of a tissue surface. If they do not adhere, they will be swept away by mucus and other fluids that bathe the tissue surface.
Bacterial adherence to the cell surface is mediated by specialised molecules. The various molecules that mediate adherence to the cell surface are called adhesins. These adhesins allow the bacteria to adhere to the surface of human cell, thereby promoting their ability to cause disease. Microorganisms that lack this mechanism are non-pathogenic. Bacterial adhesins can be divided into two major groups: pili (fimbriae) and non-pilus adhesins (afimbrial adhesins).
Pili: These are the main mechanisms by which bacteria adhere to human cells. They are the fibres that extend from the bacterial surfaces and mediate attachment of bacteria to specific receptor on the host cells. The pili of many Gram-negative bacteria bind directly to sugar residues that are part of glycolipids or glycoproteins on the host cells. They also act as a protein scaffold to which another more specific adhesive protein is affixed.
The pili of the Gram-negative bacteria have been classified into five different types and are extremely important in the pathogenesis of infections caused by them. Further antigenic variation in the actual structural pilin protein can be an important source of antigenic diversity for the pathogen.
Most E. coli strains that cause pyogenic nephritis produce an adhesin protein known as P-pili (pyelonephritis-associated pili) encoded by pap genes. Many of these adhesin proteins are present at the tip of the pili that bind specific receptors on the surface of the urinary bladder. The binding prevents the bacteria from being washed away from the urinary bladder by the flushing action of the urine.
Similarly, the pili of Neisseria gonorrhoeae mediate the attachment of the organism by binding to oligosaccharide receptors on epithelial cells of the urethra. The gonococci utilise pili as primary adhesins and opacity-associated proteins (Opa) as secondary adhesins to cells. These Opa proteins intercede adherence to polymorphonuclear cells. A part of gonococci survive subsequent phagocytosis by these cells. In organ cultures of uterine (fallopian) tube, the gonococci affix to the microvilli of non-ciliated cells and emerge to activate engulfment by these cells. These gonococci develop intracellularly and drift to the sub-epithelial space by an unexplained action.
Nonplus adhesins: These include glycocalyx and other adhesins present on the bacterial surfaces. Glycocalyx is a polysaccharide ‘slime layer’ secreted by some strains of bacteria that mediates strong adherence to certain structures, such as catheters, prosthetic implants and heart valves. For example, the glycocalyx of Staphylococcus epidermidis and that of certain viridans streptococci allows the bacteria to adhere strongly to the endothelium of the heart valve. The matrix formed by these adhesins forming proteins is called a biofilm.
The biofilms are important in pathogenesis because they protect the bacteria by host defence and antibiotics. The biofilms facilitate colonisation of bacteria, especially of surgical appliances, such as artificial valve or indwelling catheters. Streptococcus pyogenes makes use of non-pilus adhesins (such as lipoteichoic acid, protein F and M protein) to bind to epithelial cells. Recently, it has been shown that certain strains of E. coli and Shigella spp. have surface proteins called curli, which help in the binding of bacteria to the host endothelium as well as to extracellular proteins.
Invasiveness
Invasiveness refers to the ability of an organism to invade the host cells after establishing infection. ‘Invasion’ is the term commonly used to describe the entry of bacteria into host cells, implying an active role for the organisms and a passive role for the host cells. For many disease-causing bacteria, invasion of the host’s epithelium is central to the infectious process. Some bacteria (e.g., Salmonella spp.) invade tissues through the intracellular junctions in the cytoplasm. Some bacteria (e.g., Shigella spp.) multiply within host cells, whereas other bacteria do not.
Shigella spp. initiate infection process by adhering to host cells in the small intestine. There are multiple proteins, including the invasion plasmid antigens (IpA-D) that contribute to the process. Once inside the cells, the shigellae either are lysed or escape from the phagocytic vesicle, where they multiply in the cytoplasm.
Other bacteria (e.g., Yersinia species, N. gonorrhoeae, Chlamydia trachomatis) invade specific types of host’s epithelial cells and may subsequently enter the tissue. Once inside the host cell, they may remain enclosed in a vacuole composed of host cell membrane, or the vacuole membrane may dissolve and bacteria may disperse within the cell and from one cell to another.
Invasion of tissues followed by inflammation is enhanced by many factors, which include: (1) enzymes, (2) antiphagocytic factors, (3) biofilms, (4) inflammation and (5) intracellular survival.
1. Enzymes: Invasion of bacteria is enhanced by many enzymes. Many species of bacteria produce enzymes that are not intrinsically toxic but do play important roles in the infectious process. Some of these enzymes are discussed as follows:
a. Hyaluronidases and collagenase: Hyaluronidases and collagenase are the enzymes that hydrolyse hyaluronic acid and degrade collagen, respectively; thereby allowing the bacteria to spread through subcutaneous tissues.
Hyaluronidases are produced by many bacteria (e.g., staphylococci, streptococci and anaerobes) and aid in their spread through tissues. For example, hyaluronidase produced by S. pyogenes degrades hyaluronic acid in the subcutaneous tissue, thereby facilitating the organism to spread rapidly.
Clostridium perfringens produces the proteolytic enzyme collagenase, which degrades collagen (the major protein of fibrous connective tissue), and promotes the spread of infection in tissue.
b. Coagulase: Staphylococcus aureus produces the enzyme coagulase, which in association with blood factors coagulates the plasma. Coagulase contributes to the formation of fibrin walls around staphylococcal lesions, which protects bacteria from phagocytosis by walling off the infected area. The enzyme also causes deposition of fibrin on the surfaces of individual staphylococci, which may help protect them from phagocytosis or from destruction within phagocytic cells.
c. Streptokinase (fibrinolysin): Many haemolytic streptococci produce enzyme streptokinase, which activates a proteolytic enzyme of plasma. This enzyme is then able to dissolve coagulated plasma and thereby possibly aids in the rapid spread of streptococci through tissues. Streptokinase has been used in the treatment of acute myocardial infarction to dissolve fibrin clots.
d. IgA1 proteases: Certain pathogenic bacteria produce enzymes IgA1 proteases that split IgA1 at specific proline–threonine or proline–serine bonds in the hinge region and inactivate its antibody activity. IgA1 protease is an important virulence factor of the pathogens, such as N. gonorrhoeae, Neisseria meningitidis, Haemophilus influenzae, and Streptococcus pneumoniae. Production of IgA1 protease allows the pathogens to inactivate the primary antibody found on mucosal surfaces and thereby facilitates the attachment of these bacteria to the mucous membrane.
2. Antiphagocytic factors: Many bacterial pathogens are rapidly killed once they are ingested by polymorphonuclear cells or macrophages. Some pathogens evade phagocytosis or leukocyte microbicidal mechanisms by several anti-phagocytic factors; the most important being (1) capsule, (2) cell wall proteins, (3) cytotoxins and (4) surface antigens.
a. Capsule: The capsule surrounding bacteria, such as S. pneumoniae (Fig. 10-3) and N. meningitidis, is the most important anti-phagocytic factor. It retards the phagocytosis of bacteria by preventing the phagocytes from adhering to the bacteria.
b. Cell wall proteins: The cell wall proteins, such as the protein A and protein M, of S. aureus and S. pyogenes especially are anti-phagocytic. For example, protein A of S. aureus binds to IgG and prevents the activation of complement. M protein of S. pyogenes is anti-phagocytic.
c. Cytotoxins: Certain bacteria produce cytotoxins that interfere with chemotaxis or killing of phagocytes. For example, S. aureus produces haemolysins and leukocidins that lyse and damage RBCs and WBCs.
d. Surface antigens: Surface antigens of bacteria, such as Vi antigen of S. typhi and K antigen of E. coli make the bacteria resistant to phagocytosis and lytic activity of complement.
A list of intracellular pathogens is given in Table 10-7.

Fig. 10-3 Schematic diagram showing inhibition of phagocytosis by the capsule of S. pneumoniae.
Table 10-7
Intracellular Pathogens
| Organism | Examples |
| Bacteria | Mycobacterium spp. Listeria monocytogenes Brucella spp. Legionella pneumophila Francisella spp. Yersinia pestis Salmonella Typhi Shigella dysenteriae Rickettsia Chlamydia |
| Viruses | All viruses |
| Parasites | Leishmania spp. Trypanosoma cruzi Plasmodium spp. Babesia spp. Toxoplasma gondii Cryptosporidium parvum Microsporidium spp. |
| Fungus | Histoplasma capsulatum |
3. Biofilms: The biofilm is an aggregate of interactive bacteria attached to a solid surface or to each other and encased in an exopolysaccharide matrix. Biofilms consist of single cells and micro-colonies of bacteria, all found together in a highly hydrated, predominantly anionic exopolymer matrix. This is distinct from planktonic or free-living bacterial growth, in which interactions of the microorganisms do not occur. Biofilms form a slimy coat on solid surfaces and occur throughout the nature. A single species of bacteria may be involved, or more than one species may co-aggregate to form a biofilm. Fungi, including yeasts, are occasionally involved.
Biofilms are important in human infections that are persistent and difficult to treat. A few such infections include:
a. S. epidermidis and S. aureus infections of central venous catheters;
b. eye infections that occur with contact lenses and intraocular lenses;
c. infections in dental plaque and
d. Pseudomonas aeruginosa airway infections in cystic fibrosis patients.
Biofilm confers an inherent resistance to anti-microbial agents, whether these anti-microbial agents are anti-biotics, disinfectants or germicides. The mechanisms of resistance are:
a. delayed penetration of anti-microbial agent through the biofilm matrix;
b. altered growth rate of biofilm organisms;
c. other physiological changes due to biofilm mode of growth.
4. Inflammation: Inflammation is an important host defence induced by the presence of bacteria in the body. It is of two types: pyogenic and granulomatous. Pyogenic inflammation is the host defence seen primarily against pyogenic or pus-producing bacteria, such as S. pyogenes. It typically consists of neutrophils and the production of specific antibodies and elevated level of complement. Granulomatous inflammation is the host defence seen primarily against intracellular granuloma-producing bacteria, such as Mycobacterium tuberculosis, Mycobacterium leprae, etc. The response consists of production of macrophages and CD4+ T cells.
5. Intracellular survival: A few mechanisms that are suggested for intracellular survival of bacteria include (1) inhibition of phagolysosome fusion, (2) resistance to action of lysosomal enzymes and (3) adaptation to cytoplasmic replication as follows:
a. Bacteria (such as Chlamydia, M. tuberculosis) that interfere with the formation of phagolysosomes in a phagocyte can survive intracellularly and evade host defence process. These bacteria live within cells and are protected from attack by macrophages and neutrophils. The bacteria that do not interfere with the formation of phagolysosomes are otherwise killed inside the phagocytes.
b. Presence of capsular polysaccharide in Mycobacterium lepraemurium and mycoside in M. tuberculosis makes these bacteria resistant to action of lysosomal enzymes.
c. Certain bacteria, such as rickettsiae, escape from the phagosome into the cytoplasm of the host cell before the fusion of phagosome with lysosome takes place and hence continue to remain intracellular.
Toxin Production
Toxins produced by bacteria are generally classified into two groups: exotoxins and endotoxins.
1. Exotoxins: Exotoxins are heat-labile proteins that are produced by several Gram-positive and Gram-negative bacteria. These are bacterial products, which are secreted into tissues and directly harm tissues or trigger destructive biological activities (Fig. 10-4). The genes coding for these proteins are frequently encoded on plasmid or on bacteriophage DNA. Some important toxins encoded by plasmids are tetanus toxin of C. tetani and heat-labile and heat-stable toxins of enterotoxigenic E. coli. Toxins encoded by bacteriophage DNA are cholera toxins, diphtheria toxins and botulinum toxin.
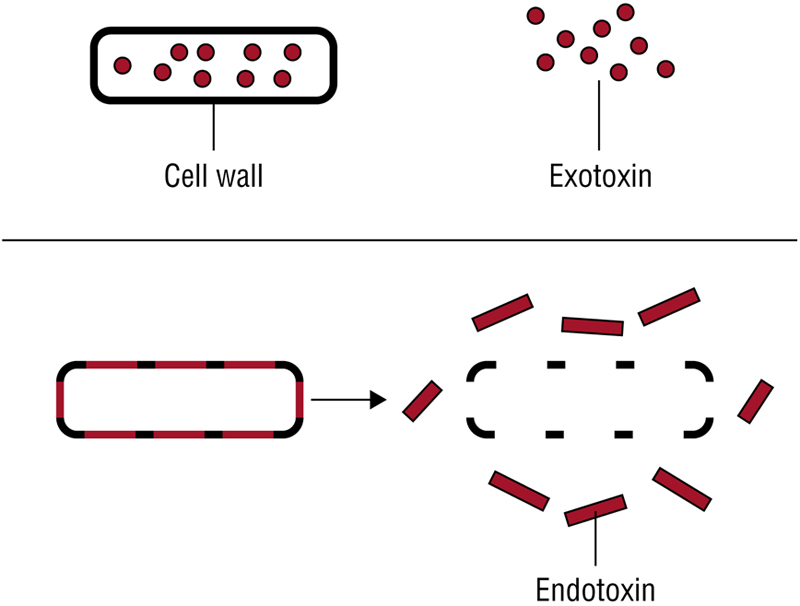
Fig. 10-4 Schematic diagram showing release of exotoxin and endotoxin.
Exotoxins show the following features:
a. Exotoxins are good antigens; they induce the synthesis of protective antibody called antitoxins. Some of these antitoxins are useful in the treatment of botulism, tetanus and other diseases. Exotoxins treated with formaldehyde or acid or heat can be converted into toxoid. The toxoids lack toxicity but retain antigenicity. Hence, these are used in protective vaccines.
b. Exotoxins are some of the most toxic substances known. They are highly potent even in minute amounts. Botulinum toxin is the most potent one, and it has been estimated that 3 kg of botulinum toxin can kill all persons in the world. Similarly, the fatal dose of tetanus toxin for a human is estimated to be less than 1 |ULg.
c. Many toxins have a dimeric A–B subunit structure. Diphtheria toxin, tetanus toxin, cholera toxins and the enterotoxin of E. coli are some of the examples of exotoxins that have an A–B subunit structure. A is the active subunit that possesses the toxic activity, and B is the binding subunit that is responsible for the binding of exotoxin to specific receptors of the membrane of human cell (Fig. 10-5).

Fig. 10-5 Schematic diagram showing mode of action of exotoxin.
d. These toxins are very specific in their mechanism of action and act at specific sites of a tissue. The biochemical targets of A–B toxin include ribosomes, transport mechanisms and intracellular signalling (cyclic adenosine monophosphate, CAMP; G protein production); all these cause diarrhoea, loss of neuronal functions or even death.
The exotoxins have specific pharmacological activities and do not produce fever, unlike endotoxins.
Superantigens: Superantigens are special group of toxins. These molecules activate T-cell nonspecifically by binding simultaneously to a T-cell receptor and major histocompatibility complex class II (MHC II) molecules on another cell, without requiring antigen. Non-specific activation of T cells results in a life-threatening autoimmune-like response by producing a large amount of interleukins, such as IL-1 and IL-2. Furthermore, stimulation of T cells by superantigen can also lead to the death of activated T cell, resulting in loss of specific T-cell clones and that of their immune response. Staphylococcal enterotoxin (toxic shock syndrome toxin) of S. aureus and erythrogenic toxin of type A or C of S. pyogenes are examples of superantigens.
2. Endotoxins: The term endotoxin was coined in 1893 by Pfeiffer to distinguish the class of toxic substances released after lysis of bacteria from the toxic substances (exotoxins) secreted by bacteria.
Endotoxins show the following properties:
a. They are produced by Gram-negative bacteria, but not by Gram-positive bacteria.
b. They are lipopolysaccharide (LPS) components of the outer membrane of Gram-negative bacteria. These form an integral part of the cell wall unlike exotoxins, which are actively released from the cells.
c. The genes that encode the enzymes that produce the LPS are present on the bacterial chromosome, but not on plasmids or bacteriophage DNA, which usually encodes the exotoxins.
d. They are heat stable, and they are released from the bacterial cell surface by disintegration of the cell wall.
e. They are weakly antigenic and do not induce, or poorly induce, protective antibodies. Hence, their action is not neutralised by the protective antibodies.
f. They cannot be toxoided.
g. All endotoxins usually produce the same generalized effect of fever and shock. The lipid A protein of LPS is responsible for endotoxin activities (Table 10-8).
Table 10-8
Mechanisms of Endotoxin-Mediated Toxicity
| Clinical Features | Mechanism |
| Fever | Interleukin-1 |
| Inflammation | Activation of alternative pathway of complement (C3a, C5a) |
| Disseminated intra-vascular coagulation (DIC) | Activation of Hageman factor |
| Shock (hypo-tension) | Bradykinin, nitric oxide |
| Leucopoenia, thrombocytopaenia, decreased peripheral circulation, and perfusion to organs | Secondary to DIC |
Endotoxic shock: Endotoxins at low concentration induce a protective response, such as fever, vasodilation, and activation of immunity and inflammatory response. However, endotoxins at very high concentration, as seen in blood of patients with Gram-negative bacterial sepsis, cause a syndrome of endotoxic shock. Endotoxic shock is characterised by fever, leucopoenia, thrombocytopaenia, sudden fall of blood pressure, circulatory collapse and sudden death. This is because high concentration of endotoxin can activate the alternative pathway of complement and cause vasodilatation and capillary leakage, resulting in high fever, hypertension and shock. It also causes activation of blood coagulation pathway, leading to disseminated intra-vascular coagulation. Endotoxins are not destroyed by autoclaving; hence infusion of sterile solution containing endotoxins can cause serious illness.
Table 10-9 summarises differences between exotoxins and endotoxins.
Table 10-9
Differences Between Endotoxins and Exotoxins
| Feature | Endotoxin | Exotoxin |
| Nature | Lipopolysaccharide | Protein (polypeptide) |
| Source | Gram-negative bacterial cell wall | Gram-positive bacteria and some Gram-negative bacteria |
| Location of genes | Chromosome | Plasmid or bacteriophage |
| Nature of secretion | Not secreted by the bacterial cell | Actively secreted by the bacteria |
| Release of toxin | Cell lysis | Filtration of bacterial cultures |
| Heat stability | Highly stable (withstand even 100°C for an hour) | Heat-labile, destroyed mostly at 60°C |
| Mode of action | Mediated by interleukins (IL-1) and tumour necrosis factor | Mostly enzyme-like action |
| Effect | Non-specific (fever, shock, etc.) | Specific pharmacological effect |
| Tissue affinity | No | Specific affinity for certain tissues |
| Diseases | Gram-negative bacterial sepsis, meningococcemia | Botulism, diphtheria, and staphylococcal toxic shock syndrome |
| Fatal dose | Only large doses are fatal | Small doses (even a few micrograms) are fatal |
| Antigenicity | Poorly antigenic | Highly antigenic |
| Neutralisation by antibodies | Ineffective | Neutralised by specific antibodies |
| Vaccine | No effective vaccine | Specific toxoids are available |
Plasmids: Plasmids are extra-chromosomal DNA materials and some of them carry specific genes responsible for drug resistance or virulence factors. Plasmids can be transferred from one bacterium to other bacteria through conjugation. Thus, certain bacterial virulence characteristics may be solely dependent on the presence or absence of the plasmid inside the cell. E. coli colonisation of intestinal mucosa through surface antigen and enterotoxin production by E. coli and S. aureus are the examples of plasmid-borne virulence characteristics.
In modern era antibiotic resistance is a major concern in treating bacterial infections. The main reason for the raise in antibiotic resistance is plasmids carrying genes for antibiotic resistance. These plasmids can be easily transferred among bacteria.
Bacteriophages: In Corynebacterium diphtheriae virulence is due to diphthteria toxin. The gene responsible for diphthteria toxin production is not an integral part of the Corynebacterium genome but it is acquired through lysogenic conversion from a beta or other tox+ corynephages.
Communicability: The survival and distribution of the parasite in a community mainly depends on its ability to spread from one host to another and it is called as communicability. Virulence and communicability are two different entities and they need not be correlating to each other. In some cases a highly virulent organism may kill its host thereby hindering its existence in the community.
Generally, intestinal and respiratory infections have high communicability, because these pathogens spread among a community through the secretory materials of the infected individuals. However, in certain infections human act as a dead end host, thereby interrupting the communicability of the pathogen. Thus, only the pathogen strain with high degrees of virulence and communicability is able to cause epidemic and pandemic diseases.
Immunopathogenesis
In certain diseases, the symptoms are caused not by the organism itself, but due to immune response to the presence of organisms. For example, immune complexes deposited in the glomerulus of the kidney cause post-streptococcal glomerulonephritis. Antibodies that are produced against the M proteins of S. pyogenes cross-react with joint, heart and brain tissues producing disease manifestations of rheumatic fever.
Similarly, the host immune response is an important cause of disease symptoms in patients suffering from syphilis caused by T. pallidum, Lyme disease caused by Borrelia and other diseases.
Manifestations of Disease
Diseases caused by various pathogenic as well as opportunistic pathogens cause a variety of clinical manifestations in infected human hosts. Many of these manifestations are caused either due to the inflammation or toxin production by the bacteria.
Termination of Disease
Termination of an infectious disease may occur by resolution or continuation of the disease. This depends on a complex interaction of host immunity with pathogens and host response to treatment with specific anti-microbial agents.
Stages of an Infectious Disease
There are four discrete stages of an infectious disease, which are as follows:
Incubation period: This denotes the time interval between the entry of infective agent and the onset of clinical manifestations of disease. During this period, the infective agent after reaching the selective tissue undergoes multiplication.
Prodrome period: It is the time during which only non-specific symptoms of disease occur.
Specific illness period: The time during which the characteristic features of disease occur.
Recovery period: The time during which symptoms resolve and health is restored.
Not all the cases that recover become free of organism. Some become chronic carriers and act as sources of infection for others. Though some cases may not develop infection, they can act as a link in the transmission of infection. This is called sub-clinical infection.
Study questions
1. Define and discuss various forms of infection.
2. Discuss the entry of the organisms and evasion of the local defences in a host.
3. Describe transmission of microbial infections.
4. Describe growth and multiplication of the bacteria at the site of adherence.
5. Discuss various types of toxins produced by bacteria. Add a note on biological effects of toxins in humans.
6. Short notes:
a. Biofilms
b. Vertical transmission
c. Biological activity of endotoxin
d. Rabbit pyrogenicity test
e. Immunopathogenesis.
Online study material
Multiple Choice Questions
1. The infection that occur at a much higher rate than usual is known as
A. Sporadic
B. Endemic
C. Endemic
D. Pandemic
2. The organisms can be transmitted vertically by all the following ways except
A. Sexual contact
B. Through the placenta
C. Within the birth canal
D. Through breast milk
3. Endotoxins can be detected in intravenous fluid by
A. Dien test
B. Limuls lysate test
C. Rideal–Walker test
D. Chick–Martin test
4. For adherence, S. pyogenes makes use of all the following adhesins except
A. Lipoteichoic acid
B. Protein F
C. M protein
D. Pili
5. All the following are the examples of superantigens except
A. Staphylococcal toxic shock syndrome toxin
B. Enterotoxin of E. coli
C. S. pyogenes erythrogenic toxin A
D. S. pyogenes erythrogenic toxin C
Keys: 1. C; 2. A; 3. B; 4. D; 5. B