6
Intracellular and Extracellular Fluid Compartments and Edema
A frequent problem in treating seriously ill patients is maintaining adequate fluids in one or both of the intracellular and extracellular compartments. As discussed in Chapter 39 and in this chapter, the relative amounts of extracellular fluid distributed between the plasma and interstitial spaces are determined mainly by the balance of hydrostatic and colloid osmotic forces across the capillary membranes.
The distribution of fluid between intracellular and extracellular compartments, in contrast, is determined mainly by the osmotic effect of the smaller solutes—especially sodium, chloride, and other electrolytes—acting across the cell membrane. The reason for this is that the cell membranes are highly permeable to water but relatively impermeable to even small ions such as sodium and chloride. Therefore, water moves across the cell membrane rapidly and the intracellular fluid remains isotonic with the extracellular fluid.
In the next section, we discuss the interrelations between intracellular and extracellular fluid volumes and the osmotic factors that can cause shifts of fluid between these two compartments.
Basic Principles of Osmosis and Osmotic Pressure
The basic principles of osmosis and osmotic pressure were presented in Chapter 4. Because cell membranes are relatively impermeable to most solutes but are highly permeable to water (ie, they are selectively permeable), whenever there is a higher concentration of solute on one side of the cell membrane, water diffuses across the membrane toward the region of higher solute concentration. Thus, if a solute such as sodium chloride is added to the extracellular fluid, water rapidly diffuses from the cells through the cell membranes into the extracellular fluid until the water concentration on both sides of the membrane becomes equal. Conversely, if a solute such as sodium chloride is removed from the extracellular fluid, water diffuses from the extracellular fluid through the cell membranes and into the cells. The rate of diffusion of water is called the rate of osmosis.
In Table 6-1, we note the approximate osmolarity of the various osmotically active substances in plasma, interstitial fluid, and intracellular fluid. About 80% of the total osmolarity of the interstitial fluid and plasma is due to sodium and chloride ions, whereas for intracellular fluid almost half the osmolarity is due to potassium ions and the remainder is divided among many other intracellular substances.
Table 6-1
Osmolar Substances in Extracellular and Intracellular Fluids
| Plasma (mOsm/L H2O) | Interstitial (mOsm/L H2O) | Intracellular (mOsm/L H2O) | |
| Na+ | 142 | 139 | 14 |
| K+ | 4.2 | 4.0 | 140 |
| Ca++ | 1.3 | 1.2 | 0 |
| Mg++ | 0.8 | 0.7 | 20 |
| Cl− | 106 | 108 | 4 |

|
24 | 28.3 | 10 |
 ,
,

|
2 | 2 | 11 |

|
0.5 | 0.5 | 1 |
| Phosphocreatine | 45 | ||
| Carnosine | 14 | ||
| Amino acids | 2 | 2 | 8 |
| Creatine | 0.2 | 0.2 | 9 |
| Lactate | 1.2 | 1.2 | 1.5 |
| Adenosine triphosphate | 5 | ||
| Hexose monophosphate | 3.7 | ||
| Glucose | 5.6 | 5.6 | |
| Protein | 1.2 | 0.2 | 4 |
| Urea | 4 | 4 | 4 |
| Others | 4.8 | 3.9 | 10 |
| Total (mOsm/L) | 299.8 | 300.8 | 301.2 |
| Corrected osmolar activity (mOsm/L) | 282.0 | 281.0 | 281.0 |
| Total osmotic pressure at 37°C (mmHg) | 5441 | 5423 | 5423 |

As shown in Table 6-1, the total osmolarity of each of the three compartments is about 300 mOsm/L, with that of the plasma being about 1 mOsm/L greater than that of the interstitial and intracellular fluids. The slight difference between plasma and interstitial fluid is caused by the osmotic effects of the plasma proteins, which maintain about 20 mmHg greater pressure in the capillaries than in the surrounding interstitial spaces, as discussed in Chapter 39.
Corrected Osmolar Activity of the Body Fluids
At the bottom of Table 6-1 are shown corrected osmolar activities of plasma, interstitial fluid, and intracellular fluid. The reason for these corrections is that cations and anions exert interionic attraction, which can cause a slight decrease in the osmotic “activity” of the dissolved substance.
Osmotic Equilibrium Is Maintained Between Intracellular and Extracellular Fluids
Large osmotic pressures can develop across the cell membrane with relatively small changes in the concentrations of solutes in the extracellular fluid. As discussed earlier, for each milliosmole concentration gradient of an impermeant solute (one that will not permeate the cell membrane), about 19.3 mmHg of osmotic pressure is exerted across the cell membrane. If the cell membrane is exposed to pure water and the osmolarity of intracellular fluid is 282 mOsm/L, the potential osmotic pressure that can develop across the cell membrane is more than 5400 mmHg. This demonstrates the large force that can move water across the cell membrane when the intracellular and extracellular fluids are not in osmotic equilibrium. As a result of these forces, relatively small changes in the concentration of impermeant solutes in the extracellular fluid can cause large changes in cell volume.
Isosmotic, Hyperosmotic, and Hypoosmotic Fluids
The terms isotonic, hypotonic, and hypertonic refer to whether solutions will cause a change in cell volume. The tonicity of solutions depends on the concentration of impermeant solutes. Some solutes, however, can permeate the cell membrane. Solutions with an osmolarity the same as the cell are called iso-osmotic, regardless of whether the solute can penetrate the cell membrane.
The terms hyperosmotic and hypoosmotic refer to solutions that have a higher or lower osmolarity, respectively, compared with the normal extracellular fluid, without regard for whether the solute permeates the cell membrane. If a cell is placed in a hypertonic solution having a higher concentration of impermeant solutes, water will flow out of the cell into the extracellular fluid causing it to shrink. If a cell is placed into a hypotonic solution that has a lower concentration of impermeant solutes (<282 mOsm/L), water will diffuse into the cell, causing it to swell. Highly permeating substances, such as urea, can cause transient shifts in fluid volume between the intracellular and extracellular fluids, but given enough time, the concentrations of these substances eventually become equal in the two compartments and have little effect on intracellular volume under steady-state conditions.
Osmotic Equilibrium Between Intracellular and Extracellular Fluids Is Rapidly Attained
The transfer of fluid across the cell membrane occurs so rapidly that any differences in osmolarities between these two compartments are usually corrected within seconds or, at the most, minutes. This rapid movement of water across the cell membrane does not mean that complete equilibrium occurs between the intracellular and extracellular compartments throughout the whole body within the same short period. The reason for this is that fluid usually enters the body through the gut and must be transported by the blood to all tissues before complete osmotic equilibrium can occur. It usually takes about 30 minutes to achieve osmotic equilibrium everywhere in the body after drinking water.
Volume and Osmolality of Extracellular and Intracellular Fluids in Abnormal States
Some of the different factors that can cause extracellular and intracellular volumes to change markedly are excess ingestion or renal retention of water, dehydration, intravenous infusion of different types of solutions, loss of large amounts of fluid from the gastrointestinal tract, and loss of abnormal amounts of fluid by sweating or through the kidneys.
One can calculate both the changes in intracellular and extracellular fluid volumes and the types of therapy that should be instituted if the following basic principles are kept in mind:
1. Water moves rapidly across cell membranes; therefore, the osmolarities of intracellular and extracellular fluids remain almost exactly equal to each other except for a few minutes after a change in one of the compartments.
2. Cell membranes are almost completely impermeable to many solutes, such as sodium and chloride; therefore, the number of osmoles in the extracellular or intracellular fluid generally remains constant unless solutes are added to or lost from the extracellular compartment.
With these basic principles in mind, we can analyze the effects of different abnormal fluid conditions on extracellular and intracellular fluid volumes and osmolarities.
Effect of Adding Saline Solution to the Extracellular Fluid
If isotonic saline is added to the extracellular fluid compartment, the osmolarity of the extracellular fluid does not change; therefore, no osmosis occurs through the cell membranes. The only effect is an increase in extracellular fluid volume (Figure 6-1A).
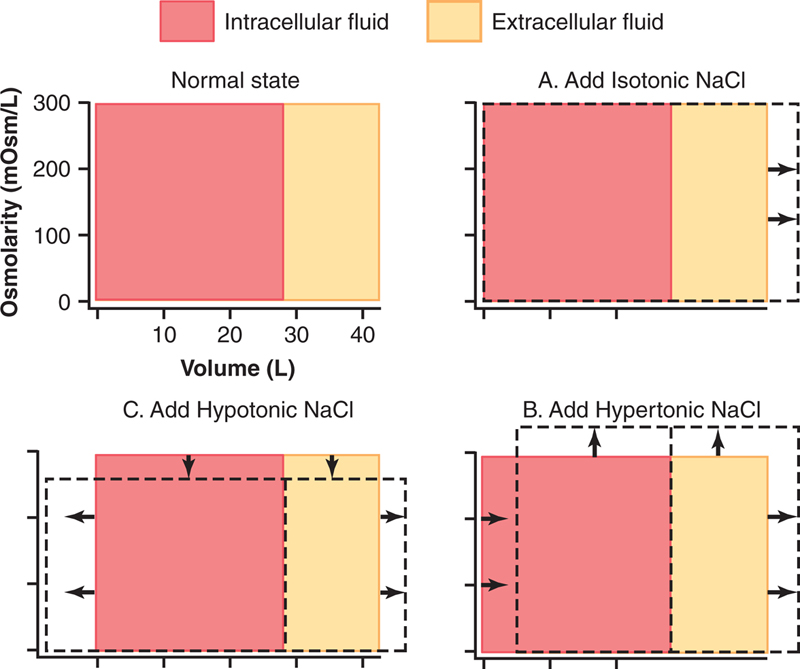
Figure 6-1 Effect of adding (A) isotonic, (B) hypertonic, and (C) hypotonic solutions to the extracellular fluid after osmotic equilibrium. The normal state is indicated by the solid lines, and the shifts from normal are shown by the shaded areas. The volumes of intracellular and extracellular fluid compartments are shown in the abscissa of each diagram, and the osmolarities of these compartments are shown on the ordinates.
If a hypertonic solution is added to the extracellular fluid, the extracellular osmolarity increases and causes osmosis of water out of the cells into the extracellular compartment (see Figure 6-1B). Again, almost all the added sodium chloride remains in the extracellular compartment and fluid diffuses from the cells into the extracellular space to achieve osmotic equilibrium. The net effect is an increase in extracellular volume (greater than the volume of fluid added), a decrease in intracellular volume, and a rise in osmolarity in both compartments.
If a hypotonic solution is added to the extracellular fluid, the osmolarity of the extracellular fluid decreases and some of the extracellular water diffuses into the cells until the intracellular and extracellular compartments have the same osmolarity (see Figure 6-1C). Both the intracellular and the extracellular volumes are increased by the addition of hypotonic fluid, although the intracellular volume increases to a greater extent.
Clinical Abnormalities of Fluid Volume Regulation: Hyponatremia and Hypernatremia
A measurement that is readily available to the clinician for evaluating a patient’s fluid status is the plasma sodium concentration. Plasma osmolarity is not routinely measured, but because sodium and its associated anions (mainly chloride) account for more than 90% of the solute in the extracellular fluid, plasma sodium concentration is a reasonable indicator of plasma osmolarity under many conditions. When plasma sodium concentration is reduced more than a few milliequivalents below normal (about 142 mEq/L), a person is said to have hyponatremia. When plasma sodium concentration is elevated above normal, a person is said to have hypernatremia.
Causes of Hyponatremia: Excess Water or Loss of Sodium
Decreased plasma sodium concentration can result from loss of sodium chloride from the extracellular fluid or addition of excess water to the extracellular fluid (Table 6-2). A primary loss of sodium chloride usually results in hyponatremia and dehydration and is associated with decreased extracellular fluid volume. Conditions that can cause hyponatremia as a result of loss of sodium chloride include diarrhea and vomiting. Overuse of diuretics that inhibit the ability of the kidneys to conserve sodium and certain types of sodium-wasting kidney diseases can also cause modest degrees of hyponatremia. Finally, Addison disease, which results from decreased secretion of the hormone aldosterone, impairs the ability of the kidneys to reabsorb sodium and can cause a modest degree of hyponatremia.
Table 6-2
Abnormalities of Body Fluid Volume Regulation: Hyponatremia and Hypernatremia
| Abnormality | Cause | Plasma Na+ Concentration | Extracellular Fluid Volume | Intracellular Fluid Volume |
| Hyponatremia—dehydration | Adrenal insufficiency; overuse of diuretics | ↓ | ↓ | ↑ |
| Hyponatremia—overhydration | Excess ADH (SIADH); bronchogenic tumors | ↓ | ↑ | ↑ |
| Hypernatremia—dehydration | Diabetes insipidus; excessive sweating | ↑ | ↓ | ↓ |
| Hypernatremia—overhydration | Cushing disease; primary aldosteronism | ↑ | ↑ | ↓ |

ADH, antidiuretic hormone; SIADH, syndrome of inappropriate ADH.
Hyponatremia can also be associated with excess water retention, which dilutes the sodium in the extracellular fluid, a condition that is referred to as hyponatremia—overhydration. For example, excessive secretion of antidiuretic hormone, which causes the kidney tubules to reabsorb more water, can lead to hyponatremia and overhydration.
Consequences of Hyponatremia: Cell Swelling
Rapid changes in cell volume as a result of hyponatremia can have profound effects on tissue and organ function, especially the brain. A rapid reduction in plasma sodium concentration, for example, can cause brain cell edema and neurological symptoms, including headache, nausea, lethargy, and disorientation. If plasma sodium concentration rapidly falls below 115–120 mmol/L, brain swelling may lead to seizures, coma, permanent brain damage, and death. Because the skull is rigid, the brain cannot increase its volume by more than about 10% without it being forced down the neck (herniation), which can lead to permanent brain injury and death.
When hyponatremia evolves more slowly over several days, the brain and other tissues respond by transporting sodium, chloride, potassium, and organic solutes, such as glutamate, from the cells into the extracellular compartment. This response attenuates osmotic flow of water into the cells and swelling of the tissues (Figure 6-2).

Figure 6-2 Brain cell volume regulation during hyponatremia. During acute hyponatremia, caused by loss of Na+ or excess H2O, there is diffusion of H2O into the cells (1) and swelling of the brain tissue (indicated by the dashed lines). This process stimulates transport of Na+, K+, and organic solutes out of the cells (2), which then causes water diffusion out of the cells (3). With chronic hyponatremia, the brain swelling is attenuated by the transport of solutes from the cells.
Transport of solutes from the cells during slowly developing hyponatremia, however, can make the brain vulnerable to injury if the hyponatremia is corrected too rapidly. When hypertonic solutions are added too rapidly to correct hyponatremia, this intervention can outpace the brain’s ability to recapture the solutes lost from the cells and may lead to osmotic injury of the neurons that is associated with demyelination, a loss of the myelin sheath from nerves. This osmotic-mediated demyelination of neurons can be avoided by limiting the correction of chronic hyponatremia to less than 10–12 mmol/L in 24 hours and to less than 18 mmol/L in 48 hours. This slow rate of correction permits the brain to recover the lost osmoles that have occurred as a result of adaptation to chronic hyponatremia.
Hyponatremia is the most common electrolyte disorder encountered in clinical practice and may occur in up to 15–25% of hospitalized patients.
Causes of Hypernatremia: Water Loss or Excess Sodium
Increased plasma sodium concentration, which also causes increased osmolarity, can be due to either loss of water from the extracellular fluid, which concentrates the sodium ions, or excess sodium in the extracellular fluid. Primary loss of water from the extracellular fluid results in hypernatremia and dehydration. This condition can occur from an inability to secrete antidiuretic hormone, which is needed for the kidneys to conserve water. As a result of lack of antidiuretic hormone, the kidneys excrete large amounts of dilute urine (a disorder referred to as “central” diabetes insipidus), causing dehydration and increased concentration of sodium chloride in the extracellular fluid. In certain types of renal diseases, the kidneys cannot respond to antidiuretic hormone, causing a type of “nephrogenic” diabetes insipidus. A more common cause of hypernatremia associated with decreased extracellular fluid volume is simple dehydration caused by water intake that is less than water loss, as can occur with sweating during prolonged, heavy exercise.
Hypernatremia can also occur when excessive sodium chloride is added to the extracellular fluid. This often results in hypernatremia—overhydration because excess extracellular sodium chloride is usually associated with at least some degree of water retention by the kidneys as well. For example, excessive secretion of the sodium-retaining hormone aldosterone can cause a mild degree of hypernatremia and overhydration. The reason that the hypernatremia is not more severe is that the sodium retention caused by increased aldosterone secretion also increases the secretion of antidiuretic hormone and causes the kidneys to also reabsorb greater amounts of water.
Thus, in analyzing abnormalities of plasma sodium concentration and deciding on proper therapy, one should first determine whether the abnormality is caused by a primary loss or gain of sodium or a primary loss or gain of water.
Consequences of Hypernatremia: Cell Shrinkage
Hypernatremia is much less common than hyponatremia, and severe symptoms usually occur only with rapid and large increases in the plasma sodium concentration above 158–160 mmol/L. One reason for this phenomenon is that hypernatremia promotes intense thirst and stimulates secretion of antidiuretic hormone, which protect against a large increase in both plasma and extracellular fluid sodium, as discussed in Chapter 80. However, severe hypernatremia can occur in patients with hypothalamic lesions that impair their sense of thirst, in infants who may not have ready access to water, in elderly patients with altered mental status, or in persons with diabetes insipidus.
Correction of hypernatremia can be achieved by administering hypoosmotic sodium chloride or dextrose solutions. However, it is prudent to correct the hypernatremia slowly in patients who have had chronic increases in plasma sodium concentration because hypernatremia also activates defense mechanisms that protect the cell from changes in volume. These defense mechanisms are opposite to those that occur for hyponatremia and consist of mechanisms that increase the intracellular concentration of sodium and other solutes.
Edema: Excess Fluid in the Tissues
Edema refers to the presence of excess fluid in the body tissues. In most instances, edema occurs mainly in the extracellular fluid compartment, but it can involve intracellular fluid as well.
Intracellular Edema
Three conditions are especially prone to cause intracellular swelling: (1) hyponatremia, as discussed earlier; (2) depression of the metabolic systems of the tissues; and (3) lack of adequate nutrition to the cells. For example, when blood flow to a tissue is decreased, the delivery of oxygen and nutrients is reduced. If the blood flow becomes too low to maintain normal tissue metabolism, the cell membrane ionic pumps become depressed. When the pumps get depressed, sodium ions that normally leak into the interior of the cell can no longer be pumped out of the cells and the excess intracellular sodium ions cause osmosis of water into the cells. Sometimes this process can increase intracellular volume of a tissue area—even of an entire ischemic leg, for example—to two to three times normal. When such an increase in intracellular volume occurs, it is usually a prelude to death of the tissue.
Intracellular edema can also occur in inflamed tissues. Inflammation usually increases cell membrane permeability, allowing sodium and other ions to diffuse into the interior of the cell, with subsequent osmosis of water into the cells.
Extracellular Edema
Extracellular fluid edema occurs when excess fluid accumulates in the extracellular spaces. There are two general causes of extracellular edema: (1) abnormal leakage of fluid from the plasma to the interstitial spaces across the capillaries and (2) failure of the lymphatics to return fluid from the interstitium back into the blood, often called lymphedema. The most common clinical cause of interstitial fluid accumulation is excessive capillary fluid filtration.
Factors that Can Increase Capillary Filtration
To understand the causes of excessive capillary filtration, it is useful to review the determinants of capillary filtration discussed in Chapter 39. Mathematically, capillary filtration rate can be expressed as follows:

where Kf is the capillary filtration coefficient (the product of the permeability and surface area of the capillaries), Pc is the capillary hydrostatic pressure, Pif is the interstitial fluid hydrostatic pressure, πc is the capillary plasma colloid osmotic pressure, and πif is the interstitial fluid colloid osmotic pressure. From this equation, one can see that any one of the following changes can increase the capillary filtration rate:
• increased capillary filtration coefficient
• increased capillary hydrostatic pressure
• decreased plasma colloid osmotic pressure
Summary of Causes of Extracellular Edema
A large number of conditions can cause fluid accumulation in the interstitial spaces by abnormal leaking of fluid from the capillaries or by preventing the lymphatics from returning fluid from the interstitium back to the circulation. The following is a partial list of conditions that can cause extracellular edema by these two types of abnormalities:
I. increased capillary pressure
A. excessive kidney retention of salt and water
1. acute or chronic kidney failure
2. mineralocorticoid excess
B. high venous pressure and venous constriction
1. heart failure
2. venous obstruction
3. failure of venous pumps
(a) paralysis of muscles
(b) immobilization of parts of the body
(c) failure of venous valves
C. decreased arteriolar resistance
1. excessive body heat
2. insufficiency of sympathetic nervous system
3. vasodilator drugs
II. decreased plasma proteins
A. loss of proteins in urine (nephrotic syndrome)
B. loss of protein from denuded skin areas
1. burns
2. wounds
C. failure to produce proteins
1. liver disease (eg, cirrhosis)
2. serious protein or caloric malnutrition
III. increased capillary permeability
A. immune reactions that cause release of histamine and other immune products
B. toxins
C. bacterial infections
D. vitamin deficiency, especially vitamin C
E. prolonged ischemia
F. burns
IV. blockage of lymph return
A. cancer
B. infections (eg, filarial nematodes)
C. surgery
D. congenital absence or abnormality of lymphatic vessels
Edema Caused by Heart Failure
One of the serious and most common causes of edema is heart failure. In heart failure the heart fails to pump blood normally from the veins into the arteries, which raises venous pressure and capillary pressure, causing increased capillary filtration. In addition, the arterial pressure tends to fall, causing decreased excretion of salt and water by the kidneys, which causes still more edema. Also, blood flow to the kidneys is reduced in persons with heart failure and this reduced blood flow stimulates secretion of renin, causing increased formation of angiotensin II and increased secretion of aldosterone, both of which cause additional salt and water retention by the kidneys. Thus, in persons with untreated heart failure, all these factors acting together cause serious generalized extracellular edema.
In patients with left-sided heart failure, but without significant failure of the right side of the heart, blood is pumped into the lungs normally by the right side of the heart but cannot escape easily from the pulmonary veins to the left side of the heart because this part of the heart has been greatly weakened. Consequently, all the pulmonary vascular pressures, including pulmonary capillary pressure, rise far above normal, causing serious and life-threatening pulmonary edema. When left untreated, fluid accumulation in the lungs can rapidly progress, causing death within a few hours.
Edema Caused by Decreased Kidney Excretion of Salt and Water
Most sodium chloride added to the blood remains in the extracellular compartment, and only small amounts enter the cells. Therefore, in kidney diseases that compromise urinary excretion of salt and water large amounts of sodium chloride and water are added to the extracellular fluid. Most of this salt and water leaks from the blood into the interstitial spaces, but some remains in the blood. The main effects of this are (1) widespread increases in interstitial fluid volume (extracellular edema) and (2) hypertension because of the increase in blood volume, as explained in Chapter 44. As an example, in children who have acute glomerulonephritis, in which the renal glomeruli are injured by inflammation and therefore fail to filter adequate amounts of fluid, serious extracellular fluid edema also develops; along with the edema severe hypertension usually develops.
Edema Caused by Decreased Plasma Proteins
Failure to produce normal amounts of proteins or leakage of proteins from the plasma causes the plasma colloid osmotic pressure to fall. This leads to increased capillary filtration throughout the body and extracellular edema.
One of the most important causes of decreased plasma protein concentration is loss of proteins in the urine in certain kidney diseases, a condition referred to as nephrotic syndrome. Multiple types of renal diseases can damage the membranes of the renal glomeruli, causing the membranes to become leaky to the plasma proteins and often allowing large quantities of these proteins to pass into the urine. When this loss exceeds the ability of the body to synthesize proteins, a reduction in plasma protein concentration occurs. Serious generalized edema occurs when the plasma protein concentration falls below 2.5 g/100 mL.
Cirrhosis of the liver is another condition that causes a reduction in plasma protein concentration. Cirrhosis means development of large amounts of fibrous tissue among the liver parenchymal cells. One result is failure of these cells to produce sufficient plasma proteins, leading to decreased plasma colloid osmotic pressure and the generalized edema that goes with this condition.
Another way liver cirrhosis causes edema is that the liver fibrosis sometimes compresses the abdominal portal venous drainage vessels as they pass through the liver before emptying back into the general circulation. Blockage of this portal venous outflow raises capillary hydrostatic pressure throughout the gastrointestinal area and further increases filtration of fluid out of the plasma into the intraabdominal areas. When this occurs, the combined effects of decreased plasma protein concentration and high portal capillary pressures cause transudation of large amounts of fluid and protein into the abdominal cavity, a condition referred to as ascites.
Safety Factors that Normally Prevent Edema
Even though many disturbances can cause edema, usually the abnormality must be severe before serious edema develops. The reason the abnormality must be severe is that three major safety factors prevent excessive fluid accumulation in the interstitial spaces: (1) low compliance of the interstitium when interstitial fluid pressure is in the negative pressure range, (2) the ability of lymph flow to increase 10- to 50-fold, and (3) wash down of interstitial fluid protein concentration, which reduces interstitial fluid colloid osmotic pressure as capillary filtration increases.
Safety Factor Caused by Low Compliance of the Interstitium in the Negative Pressure Range
Interstitial fluid hydrostatic pressure in most loose subcutaneous tissues of the body is slightly less than atmospheric pressure, averaging about −3 mmHg. This slight suction in the tissues helps hold the tissues together. Figure 6-3 shows the approximate relations between different levels of interstitial fluid pressure and interstitial fluid volume, as extrapolated to the human being from animal studies. Note that in Figure 6-3 as long as the interstitial fluid pressure is in the negative range small changes in interstitial fluid volume are associated with relatively large changes in interstitial fluid hydrostatic pressure. Therefore, in the negative pressure range, the compliance of the tissues, defined as the change in volume per millimeter of mercury pressure change, is low.
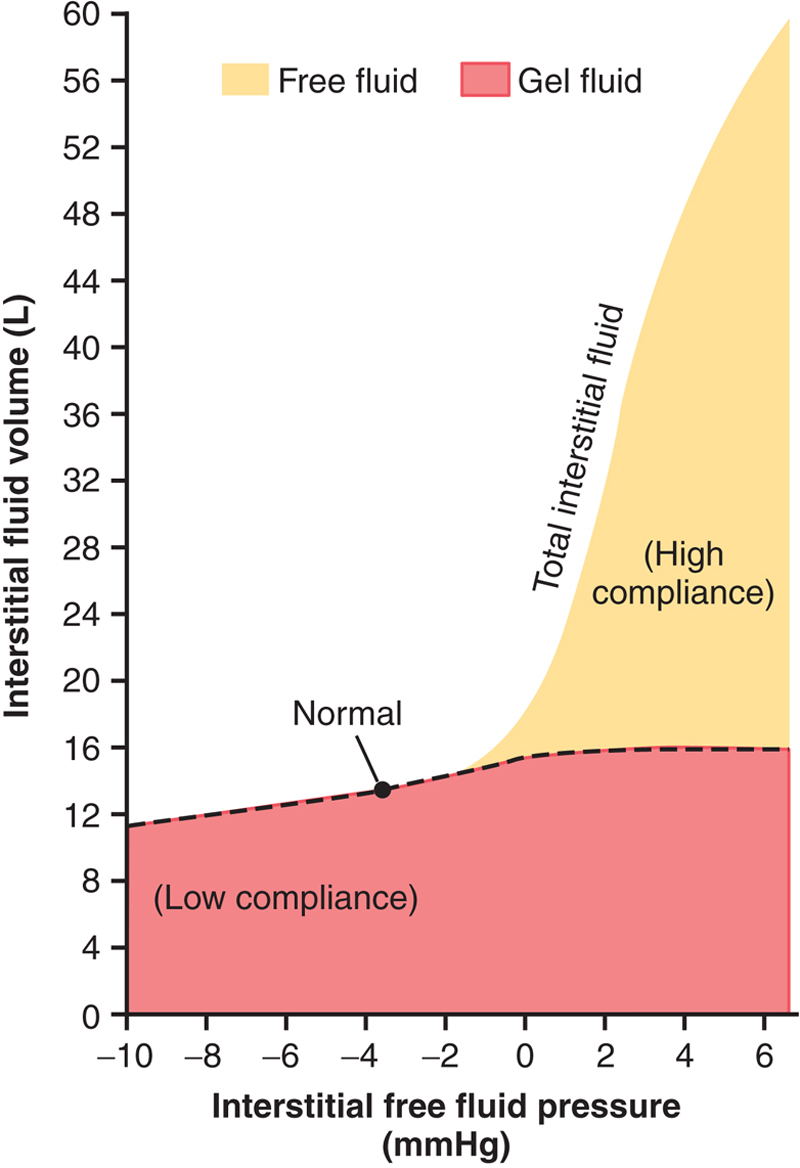
Figure 6-3 Relation between interstitial fluid hydrostatic pressure and interstitial fluid volumes, including total volume, free fluid volume, and gel fluid volume, for loose tissues such as skin. Note that significant amounts of free fluid occur only when the interstitial fluid pressure becomes positive. Modified from Guyton, A.C., Granger, H.J., Taylor, A.E., 1971. Interstitial fluid pressure. Physiol. Rev. 51, 527.
How does the low compliance of the tissues in the negative pressure range act as a safety factor against edema? To answer this question, recall the determinants of capillary filtration discussed previously. When interstitial fluid hydrostatic pressure increases, this increased pressure tends to oppose further capillary filtration. Therefore, as long as the interstitial fluid hydrostatic pressure is in the negative pressure range, small increases in interstitial fluid volume cause relatively large increases in interstitial fluid hydrostatic pressure, opposing further filtration of fluid into the tissues.
Because the normal interstitial fluid hydrostatic pressure is −3 mmHg, the interstitial fluid hydrostatic pressure must increase by about 3 mmHg before large amounts of fluid will begin to accumulate in the tissues. Therefore, the safety factor against edema is a change of interstitial fluid pressure of about 3 mmHg.
Once interstitial fluid pressure rises above 0 mmHg, the compliance of the tissues increases markedly, allowing large amounts of fluid to accumulate in the tissues with relatively small additional increases in interstitial fluid hydrostatic pressure. Thus, in the positive tissue pressure range, this safety factor against edema is lost because of the large increase in compliance of the tissues.
Increased Lymph Flow as a Safety Factor Against Edema
A major function of the lymphatic system is to return to the circulation the fluid and proteins filtered from the capillaries into the interstitium. Without this continuous return of the filtered proteins and fluid to the blood the plasma volume would be rapidly depleted, and interstitial edema would occur.
The lymphatics act as a safety factor against edema because lymph flow can increase 10- to 50-fold when fluid begins to accumulate in the tissues. This increased lymph flow allows the lymphatics to carry away large amounts of fluid and proteins in response to increased capillary filtration, preventing the interstitial pressure from rising into the positive pressure range. The safety factor caused by increased lymph flow has been calculated to be about 7 mmHg.
“Wash Down” of the Interstitial Fluid Protein as a Safety Factor Against Edema
As increased amounts of fluid are filtered into the interstitium the interstitial fluid pressure increases, causing increased lymph flow. In most tissues the protein concentration of the interstitium decreases as lymph flow is increased, because larger amounts of protein are carried away than can be filtered out of the capillaries; the reason for this phenomenon is that the capillaries are relatively impermeable to proteins, compared with the lymph vessels. Therefore, the proteins are “washed out” of the interstitial fluid as lymph flow increases.
Because the interstitial fluid colloid osmotic pressure caused by the proteins tends to draw fluid out of the capillaries, decreasing the interstitial fluid proteins lowers the net filtration force across the capillaries and tends to prevent further accumulation of fluid. The safety factor from this effect has been calculated to be about 7 mmHg.
Summary of Safety Factors that Prevent Edema
Putting together all the safety factors against edema, we find the following:
1. The safety factor caused by low tissue compliance in the negative pressure range is about 3 mmHg.
2. The safety factor caused by increased lymph flow is about 7 mmHg.
3. The safety factor caused by wash down of proteins from the interstitial spaces is about 7 mmHg.
Therefore, the total safety factor against edema is about 17 mmHg. This means that the capillary pressure in a peripheral tissue could theoretically rise by 17 mmHg, or approximately double the normal value, before marked edema would occur.
Fluids in the “Potential Spaces” of the Body
Some examples of “potential spaces” are the pleural cavity, pericardial cavity, peritoneal cavity, and synovial cavities, including both the joint cavities and the bursae. Virtually all these potential spaces have surfaces that almost touch each other, with only a thin layer of fluid in between, and the surfaces slide over each other. To facilitate the sliding, a viscous proteinaceous fluid lubricates the surfaces.
Fluid Is Exchanged Between the Capillaries and the Potential Spaces
The surface membrane of a potential space usually does not offer significant resistance to the passage of fluids, electrolytes, or even proteins, which all move back and forth between the space and the interstitial fluid in the surrounding tissue with relative ease. Therefore, each potential space is in reality a large tissue space. Consequently, fluid in the capillaries adjacent to the potential space diffuses not only into the interstitial fluid but also into the potential space.
Lymphatic Vessels Drain Protein from the Potential Spaces
Proteins collect in the potential spaces because of leakage out of the capillaries, similar to the collection of protein in the interstitial spaces throughout the body. The protein must be removed through lymphatics or other channels and returned to the circulation. Each potential space is either directly or indirectly connected with lymph vessels. In some cases, such as the pleural cavity and peritoneal cavity, large lymph vessels arise directly from the cavity itself.
Edema Fluid in the Potential Spaces Is Called “Effusion”
When edema occurs in the subcutaneous tissues adjacent to the potential space, edema fluid usually collects in the potential space as well and this fluid is called effusion. Thus, lymph blockage or any of the multiple abnormalities that can cause excessive capillary filtration can cause effusion in the same way that interstitial edema is caused. The abdominal cavity is especially prone to collect effusion fluid, and in this instance, the effusion is called ascites. In serious cases, 20 L or more of ascitic fluid can accumulate.
The other potential spaces, such as the pleural cavity, pericardial cavity, and joint spaces, can become seriously swollen when generalized edema is present. Also, injury or local infection in any one of the cavities often blocks the lymph drainage, causing isolated swelling in the cavity.
The dynamics of fluid exchange in the pleural cavity are mainly representative of all the other potential spaces as well. The normal fluid pressure in most or all of the potential spaces in the nonedematous state is negative in the same way that this pressure is negative (subatmospheric) in loose subcutaneous tissue. For instance, the interstitial fluid hydrostatic pressure is normally about −7 to −8 mmHg in the pleural cavity, −3 to −5 mmHg in the joint spaces, and −5 to −6 mmHg in the pericardial cavity.