Urinary Bladder and Urethra
URINARY BLADDER
The urinary bladder is a muscular reservoir of urine, lying in the anterior part of the pelvis. It is commonly involved in clinical conditions such as retention of urine, cystitis (inflammation of the urinary bladder), calculus, disorder of micturition, and cancer. Hence, its anatomy is of immense importance to clinicians.
LOCATION
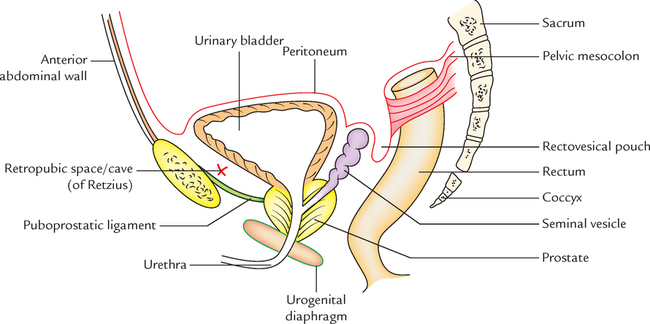
The urinary bladder is situated in the anterior part of the lesser pelvis immediately behind the pubic symphysis and in front of rectum in male and uterus in the female (Fig. 16.1). The location of the urinary bladder varies with the amount of urine it contains and with age.
When the bladder is empty it lies entirely within the lesser pelvis but when it becomes distended with urine, it expands upward and forward into the abdominal cavity.
In children, the bladder is an abdominopelvic organ even when it is empty because the pelvic cavity is small and the neck of bladder lies at the level of the upper border of pubic symphysis. It begins to enter the enlarging pelvis at the age of six years but does not become a pelvic organ entirely until after puberty.
Capacity
Normally in adult male the capacity varies from 120 to 320 ml. The mean capacity is about 220 ml.
1. An amount of urine beyond 220 ml causes a desire to micturate but the bladder is usually emptied at about 250–300 ml.
2. The filling of urine up to 500 ml may be tolerated but beyond this, it causes pain due to tension of its wall. On collection of urine about 800 ml, the micturition is beyond one’s voluntary control.
EXTERNAL FEATURES AND RELATIONS (Figs 16.2 and 16.3)
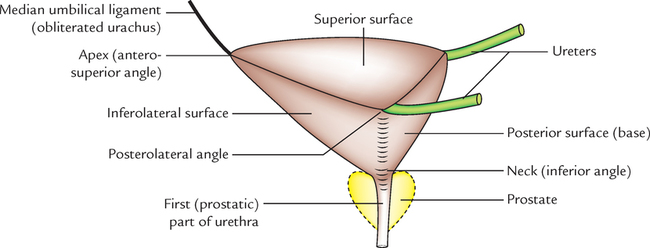
An empty and contracted bladder as seen in a cadaver is tetrahedral in shape and presents the following external features:

BASE (POSTERIOR SURFACE/FUNDUS)
• The urinary bladder is triangular in shape and directed posteroinferiorly toward the rectum.
• Its superolateral angles are joined by the ureters while its inferior angle gives rise to the urethra.
In the male, its relations are (Fig. 16.4):

1. Upper part is separated from rectum by the rectovesical pouch containing coils of the small intestine.
2. Lower part is separated from rectum by the terminal parts of vasa deferentia and seminal vesicles.
3. The triangular area between the vasa deferentia is separated from the rectum by rectovesical fascia (of Denonvilliers).
In the female, it is separated from the cervix of uterus and by the vesicouterine pouch.
SUPERIOR SURFACE
It is triangular in shape and bounded on each side by the lateral borders which extend from ureteric orifices posterolaterally to the apex anteriorly and posteriorly by the posterior border which joins the ureteric orifices.
In the male, it is completely covered by the peritoneum which separates it from:
Along its lateral borders, the peritoneum is reflected on to the pelvic walls.
In the female, it is covered by the peritoneum except for a small area near the posterior border, which is related to the supravaginal part of the uterine cervix. Here the peritoneum is reflected on to the uterine isthmus forming vesicouterine pouch.
INFEROLATERAL SURFACES
Each inferolateral surface slopes downward, forward, and medially to meet its fellow of the opposite anteriorly in the midline.
These surfaces are separated from each other, anteriorly by the anterior border, and from the superior surface by the lateral borders.
The inferolateral surfaces are devoid of peritoneum and in both male and female are related:
• In front to (Fig. 16.5)

• Behind to (Fig. 16.6)
N.B. Retropubic space (cave of Retzius): It is a perivesical space bounded anteriorly by the posterior aspect of pubic symphysis, and adjoining posterior wall of rectus sheath; posteriorly by inferolateral surfaces of the urinary bladder, superiorly by reflection of peritoneum from the superior surface of urinary bladder to the posterior aspect of the anterior abdominal wall up to the umbilicus, and inferiorly by puboprostatic/pubovesical ligaments (Fig. 16.1).
The relations of the urinary bladder are summarized in Table 16.1.

SUPPORTS OF THE URINARY BLADDER (FIXATION OF THE URINARY BLADDER)
The urinary bladder is anchored firmly at its neck, where it is fixed by its continuity with the prostate and urethra. The fixation of the bladder is also helped by the different ligaments of the urinary bladder.
LIGAMENTS (Fig. 16.7)
The ligaments of the bladder are of two types—true and false.

True Ligaments
These are formed by the condensation of pelvic fascia around the neck and the base of the bladder and have a supportive function for the bladder.
1. Lateral ligaments (two in number, right and left): They extend from the side (inferolateral surface) of the bladder to the tendinous arch of pelvic fascia.
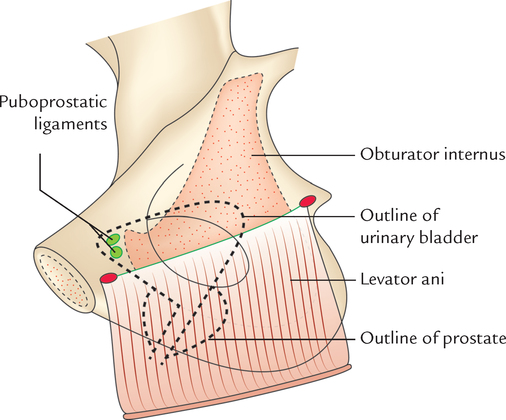
2. Puboprostatic ligaments (four in number, two on each side—lateral and medial): They fix the neck of bladder.
(a) Lateral puboprostatic ligament extends downward and medially from the anterior end of the tendinous arch of pelvic fascia to blend with the upper part of the prostatic sheath.
(b) Medial puboprostatic ligament extends downward and backward from the back of the pubic bone near the pubic symphysis to the prostatic sheath and forms the floor of retropubic space (of Retzius).
Fascial bands similar to puboprostatic ligaments in the female are termed pubovesical ligaments. They end around the neck of the urinary bladder.
3. Median umbilical ligament is the fibrous remnant of the urachus. It extends from the apex of the bladder to the umbilicus. It maintains the bladder in position anteriorly and superiorly.
4. Posterior ligament (two in number, right and left): They extend as a sheet of loose areolar tissue from the side of the base of the bladder to the lateral pelvic wall. They enclose the vesical venous plexus.
False Ligaments
These are peritoneal folds and do not have supportive function as performed by true ligaments. They are seven in number.
• Anteriorly there are three folds:
Median umbilical fold, the fold of peritoneum over the median umbilical ligament.
Two medial umbilical folds, the folds of peritoneum over the obliterated umbilical arteries.
• Laterally a pair of false lateral ligaments is formed by the reflection of the peritoneum from the bladder to the side wall of the pelvis and forms the floor of paravesical fossae.
• Posteriorly a pair of false posterior ligaments is formed. These are the sacrogenital folds which are the folds of peritoneum extending from the side of the bladder, posteriorly, on either side of the rectum, to the anterior aspect of the third sacral vertebra.
MICROSCOPIC STRUCTURE
The bladder wall from within outward is composed of:
Muscular coat:
It constitutes the detrusor muscle which consists of three layers of smooth muscle fibres.
There is profuse intermingling of the muscle fibres of these layers and they cannot be separated into three clearly defined layers.
Since the muscle fibres of the bladder wall are mainly concerned with the evacuation of the bladder they are collectively called the “detrusor muscle.”
INTERIOR OF THE BLADDER (Fig. 16.8)

1. In an empty bladder, the greater part of mucosa shows irregular folds (rugae) because it is loosely attached to the subjacent muscular layer.
2. Over a small triangular area, immediately above and behind the internal orifice of the urethra (trigone of the bladder), the mucous membrane is firmly bound to the muscular coat and therefore is smooth. The limits of trigone are defined superiorly by the openings of the ureters and inferiorly by the urethra.
The trigone of urinary bladder presents the following features:
1. Anteroinferior angle, formed by the internal orifice of the urethra.
2. Two posterosuperior angles, formed by openings of the ureters.
3. Uvula vesicae, a slight elevation in the mucous membrane immediately above and behind the internal urethral orifice. It is produced by the median lobe of prostate.
4. Interureteric ridge/crest (bar of Mercier) forms the superior boundary of trigone and connects the two ureteric orifices. It is produced by the continuation into the bladder wall of the inner longitudinal coats of the ureters.
The lateral ends of this ridge extend beyond the openings of the ureter as ureteric folds (produced by the ureters as they run obliquely through the bladder wall).
N.B. The interureteric ridge (bar of Mercier) serves as a guide to locate the orifices of the ureter during cystoscopy.
5. Two uretero-urethral ridges (Bell’s bars) extend from the ureteric orifice to the urethral orifice. They are produced by longitudinal fibres of the ureter which extends behind the ureteric orifice down on each side of trigone toward the middle lobe of the prostate.
ARTERIAL SUPPLY
NERVE SUPPLY (Fig. 16.9)
Motor Innervation
It is provided by the parasympathetic, sympathetic, and somatic fibres.
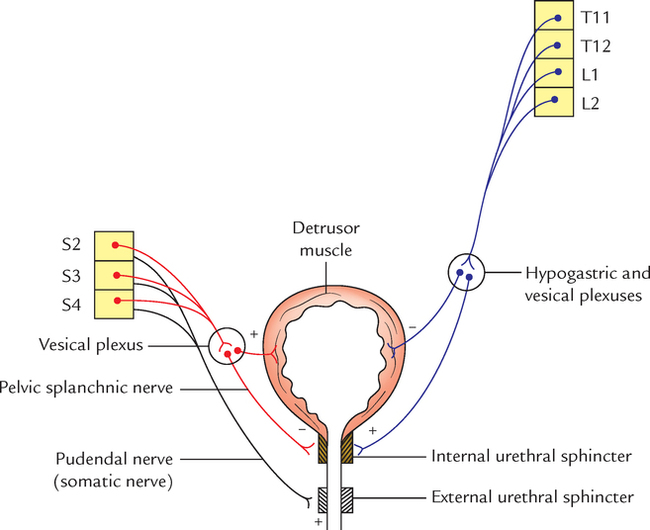
1. Parasympathetic fibres (nervi erigentes) are derived from S2, S3, S4 (spinal micturition centre) segments of the spinal cord. They are motor to the detrusor muscle and inhibitory to the sphincter vesicae (internal urethral sphincter).
2. Sympathetic fibres are derived from T11, T12 thoracic and L1, L2 lumbar segments of the spinal cord.
They are inhibitory to the detrusor and motor to the sphincter vesicae.
3. Somatic fibres (pudendal nerve) are derived from S2, S3, S4 spinal segments. They are motor to the external urethral sphincter.
N.B. The sympathetic innervation is responsible for the filling of the bladder and parasympathetic innervation for the emptying of the bladder. The somatic innervation is responsible for voluntary control of micturition.
Sensory Innervation
The majority of sensory fibres run along the parasympathetic fibres (pelvic splanchnic nerves/nervi erigentes; S2, S3, S4). Some fibres also run with the sympathetic fibres. The division of sympathetic fibres (presacral neurectomy does not alleviate bladder pain because pain fibres are carried by both sympathetic and parasympathetic fibres.
N.B. Two kinds of fibres are recognized:
1. Fibres concerned with pain.
2. Fibres concerned with conscious awareness of filling of the bladder.
Clinically, this accounts for the fact that awareness of the bladder being filled and desire to micturate remain normal after bilateral anterolateral cordotomy for the relief of pain.
DEVELOPMENT
The urinary bladder develops from the following sources:
1. Whole of bladder except its apex develops from vesicourethral canal (upper part of urogenital sinus).
2. Apex of the bladder is derived from the proximal part of the allantoic diverticulum.
3. Mucous membrane of trigonum vesicae is derived from the mesoderm of the incorporated lower ends of the mesonephric ducts.
4. Mucous membrane in the rest of the bladder is derived from the endoderm of the vesicourethral part of the cloaca.
5. Muscle and serous coat of the bladder are derived from the splanchnic layer of the lateral plate mesoderm.
• Congenital anomalies are defective obliteration of urachus (Fig. 16.10).

• Urachal fistula: The urachus is the abdominal part of allantois extending from the apex of the bladder to the umbilicus. It normally obliterates and forms the median umbilical ligament but rarely remains patent resulting in the urachal fistula, which may lead to discharge of the urine through umbilicus. Clinically it presents as discharge of urine from the umbilicus.
• Sometimes the intermediate part of the urachus fails to obliterate and forms the urachal cyst.
• If distal part of urachus fails to fibrose, it leads to formation of urachal sinus.
URETHRA
The urethra is a tubular passage, which transmits urine and seminal fluid in males and only urine in females. The study of urethra is important clinically to perform procedures of catheterization and cystoscopy. The urethral rupture is also common.
MALE URETHRA (Fig. 16.11)
The male urethra is about 18–20 cm long.
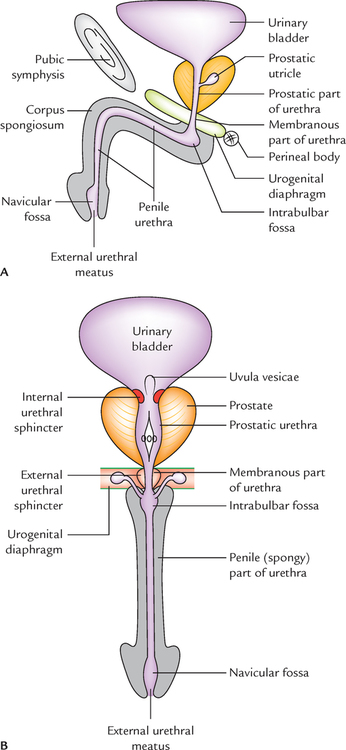
It extends from the internal urethral orifice at the neck of the urinary bladder to the external urethral orifice (EUO) at the tip of the glans penis.
In flaccid state of the penis, the long axis of the urethra presents two curvatures and is therefore S-shaped. In erect state of the penis, the distal curvature disappears and as a result it becomes ‘J-shaped’.
PARTS
According to its location, the urethra is divided into the following three parts:
1. Prostatic part (passes through the prostate).
2. Membranous part (passes through the urogenital diaphragm).
3. Spongy or penile part (passes through the corpus spongiosum of penis).
Prostatic Part of the Urethra (3 cm Long)
As its name implies it traverses through the anterior part of the prostate. It is the widest and most dilatable part of the male urethra. It is fusiform in the coronal section. The inner aspect of its posterior wall presents the following features (Fig. 16.12):

1. Urethral crest, a median longitudinal ridge of the mucous membrane.
2. Colliculus seminalis (verumontanum), an elevation on the middle of the urethral crest. The prostatic utricle opens on its summit by a slit-like orifice. On either side of the orifice of the prostatic utricle opens the ejaculatory ducts.
3. Prostatic sinuses, vertical grooves one on each side of the urethral crest. Each sinus presents 15–20 openings of the prostatic glands.
N.B. Prostatic utricle: It is a mucous cul-de-sac (5.5 cm long) in the substance of the median lobe of the prostate. It develops from united caudal ends of the two Müllerian ducts; hence it corresponds to (i.e., homologous to) the uterus and vagina of the female. It is also termed vaginus masculinus.
Membranous Part of the Urethra (2 cm Long)
It traverses through the urogenital diaphragm and pierces the perineal membrane about 2.5 cm below and behind the pubic symphysis. It is surrounded by the sphincter urethrae muscle, which serves as the voluntary external sphincter of the bladder.
With the exception of external urethral orifice, it is the narrowest and least dilatable part of the urethra. Numerous mucous glands are often found in it. In cross section, its lumen is star-shaped.
Spongy Part of the Urethra (15 cm Long)
It traverses through the corpus spongiosum of the penis. It first passes upward and forward in the bulb of penis to lie below the pubic symphysis. Then it bends downward and forward, and traverses the corpus spongiosum in the free part of the penis and terminates as the external urethral orifice just below the tip of glans penis.
It presents two dilatations: (a) in the bulb of penis to form intrabulbar fossa (3 cm long) and (b) in the glans penis to form navicular fossa/terminal fossa (1.25 cm long).
In cross section, the shape of the spongy urethra differs in different parts, viz., trapezoid-shaped in the bulb, like a transverse slit in the body and like a vertical slit at the external urethral orifice.
• The small simple tubular mucous glands called urethral glands (Littre’s glands) open in the entire spongy part of the urethra except in the terminal fossa.
• The pit-like small mucous recesses, the urethral lacunae (of Morgagni) project from the entire spongy part of the urethra except in the terminal fossa. The lacunae receive the openings of urethral glands. One lacuna present in the roof of terminal fossa is called lacuna magna or sinus of Guerin.
The external urethral orifice is the narrowest part of the male urethra. It is in the form of a sagittal slit about 6 mm long.
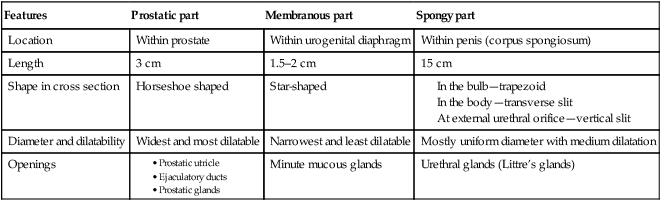
The features of different parts of the male urethra are summarized in Table 16.2 and shown in Figure 16.13.
Table 16.2
Different parts of the male urethra
| Features | Prostatic part | Membranous part | Spongy part |
| Location | Within prostate | Within urogenital diaphragm | Within penis (corpus spongiosum) |
| Length | 3 cm | 1.5–2 cm | 15 cm |
| Shape in cross section | Horseshoe shaped | Star-shaped | |
| Diameter and dilatability | Widest and most dilatable | Narrowest and least dilatable | Mostly uniform diameter with medium dilatation |
| Openings | Minute mucous glands | Urethral glands (Littre’s glands) |

N.B. The lumen of the male urethra is irregular, i.e., it has different shapes in different parts. This makes the urine projectile in nature and provides a spiral twist to the urinary flow. As a result, the early separation of droplets of urine does not occur which prevents the wetting of the clothes.
URETHRAL MUCOSA
The urethral mucosa presents regional variations as follows:
1. Prostatic urethra above the seminal colliculus is lined by transitional epithelium and below it by stratified columnar epithelium.
2. Membranous urethra is lined by stratified columnar epithelium.
3. Spongy urethra up to navicular fossa is lined by stratified columnar epithelium. The navicular fossa and external urethral orifice are lined by stratified squamous epithelium.
• Rupture of the urethra: The rupture of the urethra leads to extravasation of urine. The commonest site of rupture is bulb of the penis, just below the urogenital diaphragm following a fall astride a sharp object. The urethra is crushed against the edge of the pubic bones. The urine extravasates into the superficial perineal pouch and passes forward over the scrotum, penis, and anterior part of the anterior abdominal wall deep to membranous layer of the superficial fascia (superficial extravasation; Fig. 16.14A). If the urethra ruptures above urogenital diaphragm urine escapes above the deep perineal pouch and may pass upward around the prostate and bladder in the extraperitoneal space (deep extravasation; Fig. 16.14B).

• Catheterization of the male urethra: It is done in the patients who are unable to pass urine and their bladders are distended due to retention of urine leading to severe discomfort and pain in the hypogastric region. While passing the catheter one should remember the normal curvatures of the urethra. Further one should know that immediately above the external urethral meatus the urethra presents a large mucosal recess guarded by a mucosal fold, which may catch the tip of catheter. The catheter/iron bougie should therefore always be introduced into the urethra with its beak turned downward. Otherwise the forceful insertion of catheter may create a false passage in urethra or rupture it.
• Hypospadias: It is a congenital anomaly in which external urethral orifice is located on the inferior/ventral aspect of penis instead at the tip of the glans penis. It occurs due to failure of the fusion of urethral folds. Depending upon the location of external urethral orifice (EUO), the hypospadias are classified into 5 types (Fig. 16.15):

1. Glandular: If external urethral orifice opens on the under surface of the glans.
2. Balanic: If urethral orifice opens at the base of glans penis.
3. Penile: If urethral orifice opens on ventral aspect of the body of penis.
4. Penioscrotal: If urethral orifice opens at the junction of penis and scrotum.
5. Perineal: If urethral orifice opens as sagittal slit on ventral aspect of scrotum.
SPHINCTERS OF THE URETHRA
The urethra has two sphincters—internal and external.
Internal Sphincter
The internal sphincter surrounds the internal urethral orifice and is probably formed from the muscle of the bladder wall. It is involuntary in nature and often termed sphincter vesicae. It is supplied by the sympathetic fibres from lower thoracic and upper lumbar segments of the spinal cord (T11 to L2). It relaxes during urination but closes (i.e., contracts) during ejaculation (to prevent the retrograde entry of semen into the bladder).
External Sphincter (or Sphincter Urethrae)
The external sphincter surrounds the membranous part of the urethra and is derived from the sphincter urethrae muscle. It is voluntary in nature and is supplied by the pudendal nerve (S2, S3, S4).
The differences between the internal and external sphincters of the urethra are given in Table 16.3.

FEMALE URETHRA
The female urethra is about 4 cm long. It begins at the internal urethral orifice at the neck of bladder and passes downward and forward embedded in the anterior wall of the vagina through urogenital diaphragm. It pierces the perineal membrane, and opens in the vestibule of vagina in front of the vaginal orifice. In the vestibule of vagina, the urethral orifice is situated in front of the vaginal orifice and about 2.5 cm behind the glans of clitoris.
Glands and Lacunae around the Female Urethra
1. Urethral glands: These are small tubular glands and surround the entire urethra.
2. Paraurethral glands (of Skene): These are relatively large mucous glands and aggregated on each side of the upper part of the urethra. These glands are homologous to the male prostate.
3. Urethral lacunae: These are pit-like mucous recesses along the entire urethra.
 Most fixed part of the urinary bladder Most fixed part of the urinary bladder |
Neck of the urinary bladder |
| Most common tumor of the urinary bladder |
Transitional cell carcinoma (>90%) |
| Widest and most dilatable part of the male urethra |
Prostatic part |
| Narrowest and least dilatable part of the male urethra |
Membranous part |
| Narrowest part of the male urethra |
External urethral orifice (EUO) |
| Uterus and vagina in the male is represented by |
Prostatic utricle |
| Prostate gland in the females is represented by |
Paraurethral glands (of Skene) |


An inebriated 37-year-old man was involved in a verbal fight with a woman, using unparliamentary language. Seeing this, the woman’s husband came and gave the man a severe blow in the lower part of his anterior abdominal wall. Following the blow, the man doubled up with pain and collapsed on the road. Police was called and they took him to the emergency department of a nearby hospital. The man was in a state of shock and complained of pain in the lower abdomen. He did not pass urine since he received the blow. A diagnosis of ruptured urinary bladder was made.