Intrapartum
Phases of Parturition
• Parturition, the bringing forth of young, encompasses all physiological processes involved in birthing: the prelude to (phase 0), the preparation for (phase 1), the process of (phase 2), and the recovery from (phase 3) childbirth.
| Phase 0 | Phase 1 Activation | Phase 2 Stimulation | Phase 3 Involution |
| Prelude to parturition | Preparation for labor | Processes of labor | Parturient recovery |

Myometrial Changes
• The uterine smooth muscle must undergo a series of changes during phase 1 to prepare for labor. During phase 1, there is a striking increase in myometrial oxytocin receptors. There are increased numbers and surface areas of myometrial cell gap junction proteins such as connexin-43. Together these changes result in increased uterine irritability and responsiveness to uterotonins.
Phase 2 of Parturition: The Process of Labor
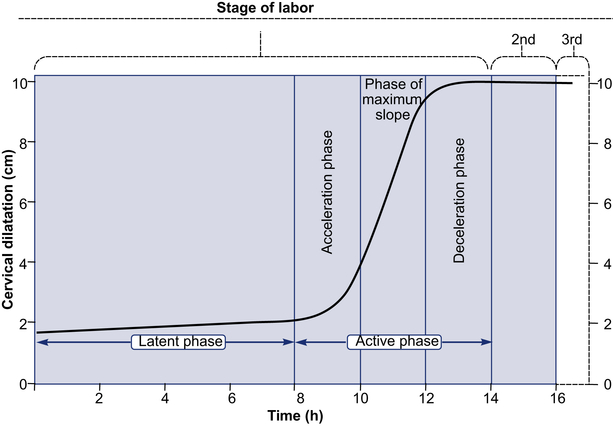
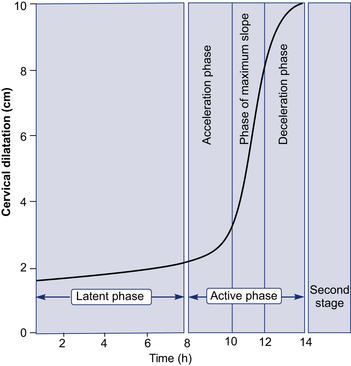
Phase 2 is synonymous with active labor, that is, the uterine contractions that bring about progressive cervical dilatation and delivery.
• The first stage is divided into a relatively flat latent phase and a rapidly progressive active phase. In the active phase, there are three identifiable component parts: an acceleration phase, a linear phase of maximum slope, and a deceleration phase.

Parts of Fetal Skull
| Part | Location |
| Bregma | Anterior fontanelle |
| Brow | Between bregma and root of nose |
| Face | Between root of nose and supraorbital ridges and junction of the floor of the mouth with neck |
| Occiput | Bony prominence behind lambda |
| Vertex | Diamond prominence behind anterior and posterior fontanelles and parietal eminences |

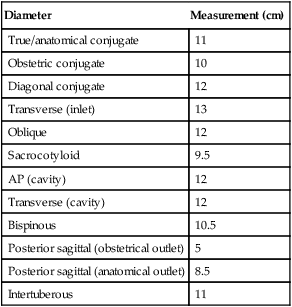
Important Diameters of Pelvis
| Diameter | Measurement (cm) |
| True/anatomical conjugate | 11 |
| Obstetric conjugate | 10 |
| Diagonal conjugate | 12 |
| Transverse (inlet) | 13 |
| Oblique | 12 |
| Sacrocotyloid | 9.5 |
| AP (cavity) | 12 |
| Transverse (cavity) | 12 |
| Bispinous | 10.5 |
| Posterior sagittal (obstetrical outlet) | 5 |
| Posterior sagittal (anatomical outlet) | 8.5 |
| Intertuberous | 11 |
Stages of Labor
| Stage | Definition |
| First | From the onset of true labor to full dilation of cervix |
| Second | From full dilation of cervix to birth of the baby |
| Third | From birth of the baby to delivery of the placenta |
| Fourth | 1 h observation period following delivery of the placenta |
Physiological chills are seen in the fourth stage of labor.
The cardinal movements of labor are engagement, descent, flexion, internal rotation, extension, external rotation, and expulsion.
The mechanism by which the biparietal diameter, the greatest transverse diameter of the fetal head in occiput presentations, passes through the pelvic inlet is designated as engagement.
Descent
The movement is the first requisite for the birth of a newborn.
Descent is brought about by one or more of four forces:
1. Pressure of the amniotic fluid
2. Direct pressure of the fundus upon the breech with contractions
American College of Obstetricians and Gynecologists (ACOG) began using a classification of station that divides the pelvis above and below the spines into five parts. These divisions represent centimeters above and below the spines. Thus, as the presenting fetal part descends from the inlet toward the ischial spines, the designation is –5, –4, –3, –2, –1, and then 0 station (at the spine). Below the ischial spines, the presenting fetal part passes +1, +2, +3, +4, and +5 stations to delivery.
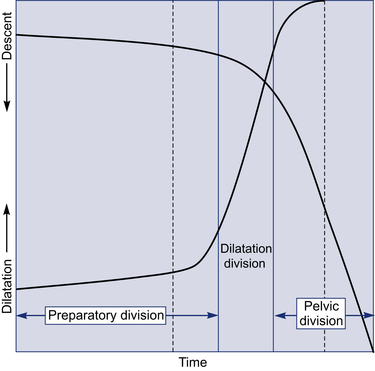
Labor course is divided functionally on the basis of dilatation and descent curves into:
1. Preparatory division, including latent and acceleration phases
2. Dilatational division, occupying the phase of maximum slope of dilatation
3. Pelvic division, encompassing both deceleration phase and second stage concurrent with the phase of maximum slope of descent
Although the differential diagnosis between false and true labor is difficult at times, it can usually be made on the basis of the contractions, as follows:
| True Labor | False Labor |
| Contractions occur at regular intervals | Contractions occur at irregular intervals |
| Intervals gradually shorten | Intervals remain long |
| Intensity gradually increases | Intensity remains unchanged |
| Discomfort is in the back and abdomen | Discomfort is chiefly in the lower abdomen |
| Cervix dilates | Cervix does not dilate |
| Discomfort is not stopped by sedation | Discomfort usually is relieved by sedation |
Caldeyro-Barcia and Poseiro from Montevideo, Uruguay, were pioneers who have done much to elucidate the patterns of spontaneous uterine activity throughout pregnancy.
They also introduced the concept of Montevideo units to define uterine activity. By this definition, uterine performance is the product of the intensity (increased uterine pressure above baseline tone during contraction) in millimeters of mercury multiplied by contraction frequency per 10 min. For example, three contractions in 10 min, each of 50 mm Hg intensity, would equal 150 Montevideo units.
According to Caldeyro-Barcia and Poseiro, clinical labor usually commences when uterine activity reaches values between 80 and 120 Montevideo units. This translates into approximately three contractions of 40 mm Hg every 10 min.
Origin and Propagation of Contractions
The normal contractile wave of labor originates near the uterine end of one of the fallopian tubes; thus, these areas act as “pacemakers.” The right pacemaker usually predominates over the left and starts the great majority of contractile waves. Contractions spread from the pacemaker area throughout the uterus at 2 cm/s, depolarizing the whole organ within 15 s. This depolarization wave propagates downward toward the cervix. Intensity is greatest in the fundus.
Partogram
Composite graphical record of key data (maternal and fetal) during labor entered against time on a single sheet of paper. It provides an accurate record of the progress of labor and any delay or deviation from normal may be detected quickly and treated accordingly. It was first devised by Freidman in 1954.
Components
2. Time: It is recorded at an interval of one hour. For spontaneous labor zero time is the time of admission in the labor ward while for induced labor, it is the time of induction.
3. Fetal heart rate: Recorded every thirty minutes.
4. Liquor color and membrane status: ‘I’ = intact membranes, ‘C’ = clear and ‘M’ = meconium stained liquor.
5. Cervical dilatation and descent of head.
6. Uterine contractions: Intensity and duration.
7. IV fluids and any drugs given.
9. Blood pressure: At an interval of 2 hours.
10. Pulse rate: Every 30 minutes.
Advantages
• Provides all important information on single sheet of paper.
• Predicts any deviation from normal progress of labor.
• Improvement in maternal and perinatal morbidity and mortality.
The concept of `alert line’ and `action line’ was introduced by Philpott and Castle in 1972. The action line can be placed at 2–4 hours interval, to the right and parallel to alert line. In partograms recommended by ‘WHO’ the distance between the alert and action lines is 4 hours.
Guidelines for Intrapartum Fetal Heart Rate Surveillance
| Surveillance | Low-Risk Pregnancies | High-Risk Pregnancies |
| Acceptable methods | ||
| Intermittent auscultation | Yes | Yes |
| Continuous electronic monitoring (internal or external) | Yes | Yes |
| Evaluation intervals | ||
| First-stage labor (active) | 30 min | 15 min |
| Second-stage labor | 15 min | 5 min |
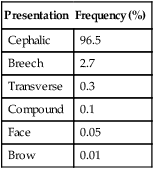
Frequency of various presentations
| Presentation | Frequency (%) |
| Cephalic | 96.5 |
| Breech | 2.7 |
| Transverse | 0.3 |
| Compound | 0.1 |
| Face | 0.05 |
| Brow | 0.01 |
Ritgen Maneuver
When the head distends the vulva and perineum enough to open the vaginal introitus to a diameter of 5 cm or more, a towel-draped, gloved hand may be used to exert forward pressure on the chin of the fetus through the perineum just in front of coccyx. Concurrently, the other hand exerts pressure superiorly against the occiput. This maneuver allows controlled delivery of the head.
Methods of Placental Separation
Schultz Mechanism
By far the most common mechanism of placental expulsion.
Delivery of the placenta with the fetal side presenting. Results when separation begins centrally with corresponding formation of a central retroplacental clot, which weights the placenta so the central portion descends first.
This then inverts the placenta and amniotic sac and causes the membranes to peel-off the remainder of the decidua and trail behind the placenta. Bleeding associated with Schultz mechanism is not visible until the placenta and membranes are delivered, since the inverted membranes hold and catch the blood.
Duncan Mechanism
Delivery of the placenta with the maternal side presenting. Results when separation first takes place at the margin or periphery of the placenta. The placenta descends sideways and the amniotic sac, therefore, is not inverted but trails behind the placenta for delivery. Blood escapes between the membranes and uterine wall and is visible externally.
Memory aid for remembering Schultz vs Duncan: Based on the appearance of the two different sides of the placenta. Fetal side is shiny and glistening because it is covered by membranes, therefore ‘shiny Schultz’. Maternal side is rough and red-looking, thus ‘dirty Duncan.’

Methods of Vaginal Delivery
There are three general methods of breech delivery through the vagina:
• Spontaneous breech delivery: The infant is expelled entirely spontaneously without any traction or manipulation other than support of the infant.
• Assisted breech delivery: The infant is delivered spontaneously as far as the umbilicus, but the remainder of the body is extracted or delivered with operator traction and assisted maneuvers, with or without maternal expulsive efforts. This is considered as the best method of vaginal breech delivery.
• Total breech extraction: The entire body of the infant is extracted by the obstetrician. This method is done only in cases of fetal distress.
The incidence of cord prolapse with frank breech presentation is about 0.5%. In contrast, the incidence of cord prolapse with complete breech presentation is 5%, and it is 15% with footling breeches.
Gynecoid and anthropoid pelves are favorable, but android and platypelloid pelvis are unfavorable for vaginal breech delivery.
Various maneuvers for breech delivery:
1. Kristellar: suprapubic pressure
2. Pinnard’s: arrested lower limbs (put the fingers in popliteal fossa, flex the knee and grasp the foot)
3. Prague’s: dorsoposterior breech
4. Lovset’s: nuchal arm. The diagnosis is made by noting the winging of the scapula.
Maneuvers for delivering after-coming head of breech:
1. Mauriceau-Smellie-Veit: malar flexion and shoulder traction
2. Burns-Marshall: baby held by ankle and trunk is swung in upward and forward direction
3. Wigard-Martin: malar flexion and supra-pubic pressure
4. Pipers forceps: Piper’s forceps is the best method to deliver the after-coming head of breech because:
Indications for Cesarean Section in Breech Presentation
3. Twins with first baby in breech
5. Preterm breech (risk of intraventricular hemorrhage increases with vaginal delivery)
In perhaps 5% of term breech presentations, the fetal head may be in extreme hyperextension. This presentation is referred to as the stargazer fetus or the flying fetus. With such hyperextension, vaginal delivery may result in injury to the cervical spinal cord. In general, marked hyperextension after labor has begun is considered an indication for cesarean delivery.
Preterm infants undergoing cesarean delivery have a better prognosis.
Occasionally, especially with small preterm fetuses, the incompletely dilated cervix will not allow vaginal delivery of the after-coming head. In such cases, Dührssen incisions are usually necessary (cut the cervix at 10 and 2 o’clock positions).
External Cephalic Version
The ACOG recommends that efforts should be made to reduce breech presentation by external cephalic version (ECV) whenever possible.
The success rate for external cephalic version ranges from 35% to 85%, with an average of about 60%.
ECV should be performed at 36 weeks of gestation for the following reasons:
1. If version results in fetal distress and need for immediate LSCS, iatrogenic prematurity is avoided.
2. The likelihood of spontaneous version is low.
3. An additional consideration in timing the version is that, although earlier attempts are more likely to be successful, they also are more likely to be associated with spontaneous reversion to breech.
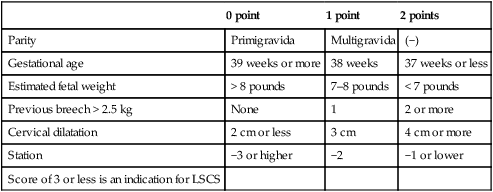
Breech Score of Zatuchni and Andros
| 0 point | 1 point | 2 points | |
| Parity | Primigravida | Multigravida | (−) |
| Gestational age | 39 weeks or more | 38 weeks | 37 weeks or less |
| Estimated fetal weight | > 8 pounds | 7–8 pounds | < 7 pounds |
| Previous breech > 2.5 kg | None | 1 | 2 or more |
| Cervical dilatation | 2 cm or less | 3 cm | 4 cm or more |
| Station | −3 or higher | −2 | −1 or lower |
| Score of 3 or less is an indication for LSCS |
Face
The commonest face position is LMA (left mentoanterior).
Etiology
| Maternal | Fetal |
| Multiparity with lax abdomen | Congenital anomalies (15%) |
| CPD | Anencephaly |
| Flat pelvis (platypelloid) | Congenital goiter |
| Dolichocephaly |
Delivery in mentoanterior occurs by flexion instead of extension of the head. In mentoposterior face, vaginal delivery is not possible and will always require LSCS.
Brow
1. Brow is the rarest presentation.
2. Brow is commonly unstable and converts into either vertex or face.
3. Supraorbital ridges and anterior fontanelle can be palpated on P/v examination.
4. There is no mechanism of labor in persistent brow presentation. Delivery is by LSCS.
5. It is associated with contracted pelvis or fetal macrosomia.
Transverse Lie
1. The dorsoanterior position is most common (60%).
2. In dorsoposterior, the chance of fetal extension is common with increased risk of arm prolapse and cord prolapse.
Etiology
There is no mechanism of labor in transverse lie. Delivery is by LSCS.
If the fetus is small (usually <800 g) and the pelvis is large, spontaneous delivery is possible in transverse lie. The fetus is compressed with the head forced against the abdomen. A portion of the thoracic wall below the shoulder thus becomes the most dependent part, appearing at the vulva. The head and thorax then pass through the pelvic cavity at the same time, and the fetus, which is doubled upon itself, is expelled—this is referred to as conduplicato corpora.

Common Clinical Findings in Women with Ineffective Labor
• Inadequate cervical dilatation or fetal descent
• Protracted labor—slow progress
• Inadequate expulsive effort—ineffective “pushing”
Recommendation of the ACOG is that the cervix should be dilated to 4 cm or more before a diagnosis of dystocia is made.
Types of Uterine Dysfunction
It is possible to define two types of uterine dysfunction. In the more common hypotonic uterine dysfunction, there is no basal hypertonus and uterine contractions have a normal gradient pattern (synchronous), but the slight rise in pressure during a contraction is insufficient to dilate the cervix. In the other, hypertonic uterine dysfunction or incoordinate uterine dysfunction, either the basal tone is elevated appreciably or the pressure gradient is distorted. Gradient distortion may result from contraction of the mid-segment of the uterus with more force than the fundus or from complete asynchronism of the impulses originating in each cornu, or from a combination of these two.
ACOG has suggested that, before the diagnosis of arrest during first-stage labor is made, both of these criteria should be met:
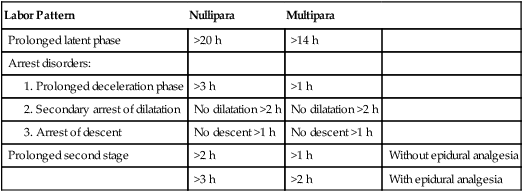
Abnormal Labor Patterns, Diagnostic Criteria
| Labor Pattern | Nullipara | Multipara | |
| Prolonged latent phase | >20 h | >14 h | |
| Arrest disorders: | |||
| >3 h | >1 h | ||
| No dilatation >2 h | No dilatation >2 h | ||
| No descent >1 h | No descent >1 h | ||
| Prolonged second stage | >2 h | >1 h | Without epidural analgesia |
| >3 h | >2 h | With epidural analgesia |
Shoulder Dystocia
A head-to-body delivery time exceeding 60 sec is used to define shoulder dystocia.
• Risk factors include D, O, P, E.
• Postpartum hemorrhage, usually from uterine atony, but also from vaginal and cervical lacerations, is the major maternal risk, following shoulder dystocia.
• Shoulder dystocia may be associated with significant fetal morbidity and even mortality.
• Transient Erb or Duchenne brachial plexus palsies are the most common injury, followed by clavicular fractures and humeral fractures.
As per ACOG guidelines, planned cesarean delivery is to be considered for the nondiabetic woman carrying a fetus with an estimated fetal weight exceeding 5000 g or the diabetic woman whose fetus is estimated to weigh more than 4500 g to avoid the risk of shoulder dystocia.
Management of Shoulder Dystocia
1. Extend the episiotomy, remove the lithotomy position. Never give fundal pressure. Moderate suprapubic pressure can be applied by an assistant while downward traction is applied to the fetal head.
Check if it is a unilateral shoulder dystocia (posterior shoulder is in hollow of sacrum, anterior is above pelvic brim) or a bilateral shoulder dystocia (both shoulders above pelvic brim).
If it is bilateral shoulder dystocia, directly proceed to perform LSCS after doing the Zavanelli maneuver (cephalic replacement into the pelvis and then cesarean delivery).
The rest of the maneuvers can be tried for unilateral shoulder dystocia, and if they fail, then proceed for Zavanelli maneuver (cephalic replacement into the pelvis) and LSCS.
2. The McRoberts maneuver: The maneuver consists of removing the legs from the stirrups and sharply flexing them up onto the abdomen. This procedure causes straightening of the sacrum relative to the lumbar vertebrae, rotation of the symphysis pubis toward the maternal head, and a decrease in the angle of pelvic inclination.
3. Woods reported that, by progressively rotating the posterior shoulder 180° in a corkscrew fashion, the impacted anterior shoulder could be released. This is frequently referred to as the Woods corkscrew maneuver.
4. Delivery of the posterior shoulder.
6. Cleidotomy consists of cutting the clavicle with scissors or other sharp instruments and is usually used for a dead fetus. Symphysiotomy has also been applied successfully.
7. Hibbard maneuver is not used, as it is associated with fetal orthopedic and neurological damage.
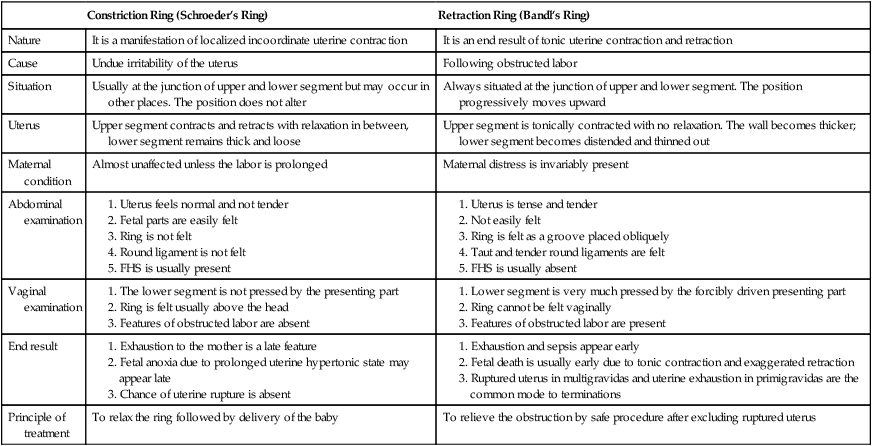
Difference Between Constriction and Retraction Rings
| Constriction Ring (Schroeder’s Ring) | Retraction Ring (Bandl’s Ring) | |
| Nature | It is a manifestation of localized incoordinate uterine contraction | It is an end result of tonic uterine contraction and retraction |
| Cause | Undue irritability of the uterus | Following obstructed labor |
| Situation | Usually at the junction of upper and lower segment but may occur in other places. The position does not alter | Always situated at the junction of upper and lower segment. The position progressively moves upward |
| Uterus | Upper segment contracts and retracts with relaxation in between, lower segment remains thick and loose | Upper segment is tonically contracted with no relaxation. The wall becomes thicker; lower segment becomes distended and thinned out |
| Maternal condition | Almost unaffected unless the labor is prolonged | Maternal distress is invariably present |
| Abdominal examination | ||
| Vaginal examination | ||
| End result | ||
| Principle of treatment | To relax the ring followed by delivery of the baby | To relieve the obstruction by safe procedure after excluding ruptured uterus |
Bishop Scoring System used for Assessment of Inducibility
| Factor | |||||
| Score | Dilatation (cm) | Effacement (%) | Station | Cervical Consistency | Cervical Position |
| 0 | Closed | 0–30 | −3 | Firm | Posterior |
| 1 | 1–2 | 40–50 | −2 | Medium | Mid-position |
| 2 | 3–4 | 60–70 | −1 | Soft | Anterior |
| 3 | ≥5 | >80 | +1 to +2 | – | – |
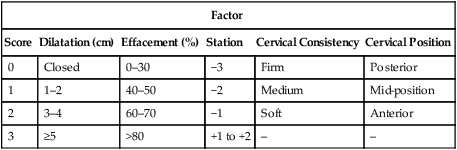
A score of 9 conveys a high likelihood for a successful induction. Score of 4 or less identifies unfavorable cervix and needs for cervical ripening.
Local application of prostaglandin E2 (dinoprostone) is commonly used for cervical ripening.
ACOG has approved use of 25 μg vaginal misoprostol for cervical ripening. A vaginal dose of 50 μg is associated with tachysystole/meconium passage aspiration.
Operative Vaginal Delivery (Forceps and Vacuum)
ACOG Classification of Forceps and Vacuum Delivery According to Station and Rotation
| Procedure | Criteria |
| Outlet | |
| Low | Leading point of fetal skull is at station ≥ +2, and not on pelvic floor |
| Rotation is 45° or less (left or right occiput anterior to occiput anterior, or left or right OP to OP) | |
| Rotation is greater than 45° | |
| Mid-pelvic | Station above +2 cm, but head is engaged |
| High | Not included in classification |
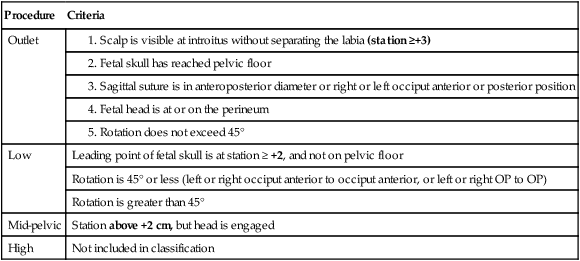
In modern day obstetrics, forceps is not applied if station is above +2 (station should be at least +2 before applying forceps).
Prerequisites for Forceps Application
There are at least six prerequisites for successful application of forceps:
• The fetus must present as a vertex or by the face with the chin anterior. The position of the fetal head must be precisely known.
• The cervix must be completely dilated.
• The membranes must be ruptured.
• There should be no suspected cephalic-pelvic disproportion.
With the application of forceps, the head of the fetus is perfectly grasped only when the long axis of blades corresponds to occipitomental diameter.
Generally, the indications and prerequisites for the use of the vacuum extractor for delivery are the same as for forceps delivery.
Differences between forceps and vacuum
| Forceps | Vacuum |
| Traction force = +18 kg for primi, +13 kg for multi | Negative pressure = 0.8 kg/cm2 (600 mm Hg) |
| Cervix should be fully dilated | Minimum 7 cm dilation |
| Less fetal but more maternal complications | More fetal but less maternal complications |
| Preferred in fetal distress | Less preferred (as vacuum takes time to build up) |
| Rotation forceps not applied nowadays | Vacuum causes rotation and extraction |
| Can be applied on face presentation and after-coming head of breech | Cannot be applied on face presentation and after coming head of breech |
| Can be applied on preterm fetus | Contraindicated on preterm fetus (increased risk of intraventricular hemorrhage) |
| Can be applied in cases of fetal coagulopathy and if recent scalp blood sampling has been done | Contraindicated in cases of fetal coagulopathy and if recent scalp blood sampling has been done |
| Can be applied in cases of IUFD | Should not be applied as chignon formation will not occur in IUFD |
When using rigid cups, it is recommended that the vacuum be created gradually by increasing the suction by 0.2 kg/cm2 every 2 min until a negative pressure of 0.8 kg/cm2 (600 mm Hg) is reached. With soft cups, negative pressure can be increased to 0.8 kg/cm2 within 1 min.
Comparisons: Forceps Versus Vacuum
• There are significantly more third- and fourth-degree lacerations, in the forceps-delivered group.
• Conversely, the incidence of shoulder dystocia and cephalohematomas are more in the vacuum group.
• Investigators have found decreased maternal trauma by vacuum compared with forceps.
• Although retinal hemorrhage occasionally is seen with vacuum usage, it has no apparent long-term effects. Johanson and Menon analyzed 10 randomized trials and confirmed that vacuum extraction was associated with less maternal but more fetal trauma, for example, cephalohematoma and retinal hemorrhage.
Definitions
| Term | Definition |
| Prophylactic forceps | Forceps delivery only to shorten the second stage (e.g., heart disease patients) |
| Trial forceps | It is a tentative attempt of forceps delivery in case of suspected mild CPD with a preamble declaration of abandoning it in favor of cesarean section if moderate traction fails to overcome the resistance. It is to be performed in the operation theater |
| Failed forceps | When a deliberate attempt in vaginal delivery with forceps has resulted in significant fetal or maternal trauma |
Cesarean Section
Most often the incision is made in the lower uterine segment transversely, as described by Kerr. Occasionally, a low-segment vertical incision, as described by Krönig, may be used. The classical incision is a vertical incision into the body of the uterus above the lower uterine segment and reaching the uterine fundus. This incision is seldom used today.
Indications
| Absolute | Relative |
| Central placenta previa | CPD |
| Adherent placenta | Previous LSCS |
| Severe degree of contracted pelvis | Dystocia |
| Previous two LSCS | Abruption |
| Classical CS | IUGR |
| Fetal distress | BOH |
| Transverse/oblique lie | Elderly primi/grand multipara |
| Advanced carcinoma cervix | MSAF |
| Preeclampsia/severe eclampsia |
Establishment of Fetal Maturity Prior to Elective Repeat Cesarean Delivery
Fetal maturity may be assumed if one of the following criteria is met:
1. Fetal heart sounds have been documented for 20 weeks by nonelectronic fetoscope or for 30 weeks by Doppler ultrasound.
2. It has been 36 weeks since a positive serum or urine chorionic gonadotropin pregnancy test was performed by a reliable laboratory.
3. An ultrasound measurement of crown-rump length, obtained at 6–11 weeks, supports current gestational age of 39 weeks or more.
4. Clinical history and physical and ultrasound examination performed at 12–20 weeks support current gestational age of 39 weeks or more.
Merits and Demerits of Lower Segment Operation over Classical
| Lower Segment | Classical | |
| Techniques | Operative field less bloody because of less vascularity | More bloody because of increased vascularity |
| The wall is thin, and as such apposition is perfect lie | The wall is thick, and coaptation of the margins is not perfect | |
| Postoperative | Hemorrhage and shock—less | More |
| Peritonitis is less even in infected uterus because of perfect peritonization and, if occurs, localized to pelvis | Chance of peritonitis is more in presence of uterine sepsis | |
| Peritoneal adhesions and intestinal obstruction are less Convalescence is better Mortality is much lower |
More because of imperfect peritonization Relatively poor Mortality is high |
|
| Wound healing | The scar is better healed because: Perfect apposition of the thin margins |
The scar is weak because: Imperfect apposition because of thick margins |
| Chance of blood collecting in the wound is less | Chance of blood collection in the wound is more, which hinders union | |
| The wound remains quiescent during healing process | The wound is in a state of tension and due to contraction and relaxation of the upper segment. As a result, the knots may slip or the sutures may become lax | |
| Chance of gutter formation is unlikely as placental implantation is usually fundal | Chance of gutter formation on the inner aspect is likely because of (a) inclusion of the deciduas or (b) inadequate coaptation of the friable inner part when the placenta is anteriorly situated | |
| During future pregnancy | Scar rupture is less (mainly in labor): 0.2–1.5% | More risk of rupture (mainly in third trimester): 4–9% |
• Trial of scar is different from trial of labor.
• A patient of previous LSCS attempting a vaginal delivery is called a trial of scar (as the previous scar is put to trial).
• Trial of labor is indicated in mild-to-moderate CPD (with no prior uterine scar) and if it fails then the patient is delivered by LSCS, whereas trial of scar is absolutely contraindicated in CPD.
• The absolute risk of uterine rupture attributable to a trial of scar resulting in death or injury to the fetus is about 1 per 1000.
Recommendations of the ACOG Useful for the Selection of Candidates for Vaginal Birth after Cesarean Delivery
1. No more than one prior low-transverse cesarean delivery
2. Clinically adequate pelvis (no CPD)
3. No other uterine scars or previous rupture
4. Physician immediately available throughout active labor who is capable of monitoring labor and performing emergency cesarean delivery
5. Availability of anesthesia and personnel for emergency cesarean delivery
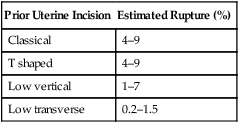
Estimated Risks for Uterine Rupture in Women with a Prior Cesarean Delivery
| Prior Uterine Incision | Estimated Rupture (%) |
| Classical | 4–9 |
| T shaped | 4–9 |
| Low vertical | 1–7 |
| Low transverse | 0.2–1.5 |
• In women with uterine malformations who have undergone cesarean delivery, the risks for uterine rupture in a subsequent pregnancy may be as high as with a classical incision.
• Women who have previously sustained a uterine rupture are at increased risk of recurrence. Those with a rupture confined to the lower segment have been reported to have a 6% recurrence risk in subsequent labor, whereas those whose prior rupture included the upper uterus have a 32% recurrence risk.
• The rate of uterine rupture is increased nearly fivefold in women with two previous cesarean deliveries compared with that in those only with one—3.7% versus 0.8%.
• Any previous vaginal delivery, either before or following a cesarean birth, significantly improves the prognosis for a subsequent successful vaginal birth after cesarean delivery (VBAC).
• The success rate for a trial of scar depends to some extent on the indication for the previous cesarean delivery. Generally, about 60–80% of trials after prior cesarean birth result in vaginal delivery, with success being maximum if previous cesarean section was because of breech presentation.
• Women attempting VBAC who had no previous vaginal deliveries, the relative risk of uterine rupture is more than doubled when the birth weight is at least 4000 g.
• As maternal weight increases, the rate of VBAC success decreases.
• Any attempt to induce cervical ripening or to induce or augment labor increases the risk of uterine rupture in women undergoing a trial of scar.
Use of oxytocin to induce or augment labor has been implicated in uterine ruptures in women attempting VBAC.
• The American Academy of Pediatrics and the ACOG have concluded that oxytocin may be used for both labor induction and augmentation with close patient monitoring, in women with a prior cesarean delivery undergoing a trial of scar.
• Several prostaglandin preparations commonly are employed for cervical ripening or labor induction. Recent evidence indicates that their use in women attempting VBAC substantively increases the risk of uterine rupture.
• The ACOG discourages the use of prostaglandin cervical ripening agents for the induction of labor in women with previous LSCS.
Rupture Uterus
Uterine rupture typically is classified as either complete (all layers of the uterine wall separated) or incomplete (uterine muscle separated but visceral peritoneum is intact). Incomplete rupture is also commonly referred to as uterine dehiscence.
The greatest risk factor for either complete or incomplete uterine rupture is prior cesarean delivery.
Following uterine rupture the most common electronic fetal monitoring finding tends to be sudden, severe heart rate decelerations that may evolve into late decelerations, bradycardia, and undetectable fetal heart action.
In some cases in which the fetal presenting part has entered the pelvis with labor, loss of station may be detected by pelvic examination. If the fetus is partly or totally extruded from the site of uterine rupture, abdominal palpation or vaginal examination may be helpful to identify the presenting part, which will have moved away from the pelvic inlet. A firm contracted uterus may at times be felt alongside the fetus.
With rupture and expulsion of the fetus into the peritoneal cavity, the chances for intact fetal survival are dismal, and reported mortality rates range from 50% to 75%.
Clinical Features of Ruptured Uterus
| Impending Scar Rupture (Scar Dehiscence) | Ruptured Uterus |
| Unexplained tachycardia | Weak thready fast pulse |
| Hypotension | Shock |
| Fetal tachycardia | Persistent fetal bradycardia/IUFD |
| Uterine scar tenderness | Hematuria |
| Bleeding pv | Bleeding pv |
| Hematuria | Recession of presenting part |
Change in fetal heart rate (tachycardia/loss of beat to beat variability/decelerations) is the earliest sign of impending scar dehiscence, followed by maternal tachycardia.
MULTIPLE CHOICE QUESTIONS
Answer: a (Uterine contraction in mm of Hg per 10 min)
• Montevideo units (MVUs) refer to the strength of contractions in mm of Hg multiplied by the frequency per 10 min as measured by intra-uterine pressure transducer.
• The uterine contractile force produced must exceed 200 MVUs/10 min for active labor to be considered adequate.
For example, three contractions in 10 min such that each reaches a peak of 60 mmHg above the baseline, then the strength of contraction is 60 × 3 = 180 MVUs.
Three significant advances in the treatment of uterine dysfunction have reduced the risk of perinatal morbidity (PNM) and mortality: (1) the avoidance of undue prolongation of labor, (2) the use of intravenous oxytocin in the treatment of some patterns of uterine dysfunction, and (3) the liberal use of cesarean section (rather than midforceps) to affect delivery when oxytocin fails.
Prolonged latent phase is not associated with increased risk of PNM or low Apgar scores and should be treated by therapeutic rest. Protraction disorders have a higher rate of PNM and low Apgar scores, but not if spontaneous labor follows the abnormality.
Arrest disorders are associated with significantly higher rates of PNM following either spontaneous or instrument-assisted delivery.
Cord clamping is a part of management of the second stage of labor and not third stage.
Delay in clamping for 2–3 min or till cessation of the cord pulsation facilitates transfer of 80–100 mL of blood from the compressed placenta to a baby, when placed below the level of uterus. This is beneficial to a mature baby but may be deleterious to preterm or a low-birthweight baby due to hypervolemia. But early clamping should be done in cases of Rh incompatibility (to prevent transfer from the mother to the baby) or babies born asphyxiated or born to a diabetic mother.

Hypertonic uterine dysfunction is characterized by a lack of coordination of uterine contractions, possibly caused by disorganization of the contraction gradient, which normally is greatest at the fundus and least at the cervix. This type of dysfunction usually appears during the latent phase of labor and is responsive to sedation, not oxytocin stimulation. The disorder is accompanied by a great deal of discomfort with little cervical dilation. After being sedated for a few hours, affected women usually awaken in active labor.
Sedation is also given to differentiate whether the patient is in prolonged latent phase or in false labor: Patients in false labor sleep and awake without contractions, but patients in latent phase show cervical changes after a period of sleep.
There are two varieties of breech presentation.
1. Complete (flexed breech): The normal attitude of full flexion is maintained. The thighs are flexed at the hips and the legs at the knees. The presenting part consists of the buttocks, external genitalia and the two feet. It is commonly present in multiparas.
2. Incomplete: This is due to varying degrees of extension of thighs or legs at the podalic pole. Three varieties are possible:
a. Breech with extended legs (Frank breech) (MC variety): In this condition, the things are flexed on the trunk and the legs are extended at the knee joints. The presenting part consists of the two buttocks and external genitalia only. It is commonly present in primigravidas. The increased prevalence in primigravidas is due to tight abdominal wall, good uterine tone and early engagement of breech.
b. Footling presentation: Both the thighs and legs are partially extended, bringing the legs to present at the brim.
c. Knee presentation: Thighs are extended but the knees are flexed, bringing knees down to present at the brim. The two latter varieties are not common.
1. Williams, 22nd Ed., Pgs. 566–7.
6. A 25-year-old primigravida patient at 38 weeks complains of gross rupture of membranes and painful uterine contractions every 2–3 min. On digital examination, her cervix is 3 cm with fetal feet palpable through the cervix, and the fetal heart rate tracing is reactive. What is the best method to achieve delivery?
The patient described here has a fetus in the footling breech presentation. Because of the very high risk of cord prolapse, it is recommended that fetuses with footling breech presentations undergo delivery by cesarean section. External cephalic version is a procedure by which the presentation of the fetus is changed from breech to cephalic, by manipulating the fetus externally through the abdominal wall. It is not indicated in this patient because the membranes are ruptured and the risk of cord prolapse is great. In addition, this procedure generally requires that the uterus be soft and relaxed, which is not the case with this patient in labor. Internal podalic version is a procedure used in the delivery of a second twin. It involves turning the fetus by inserting a hand into the uterus, grabbing both feet, and delivering the fetus by breech extraction.
1. Williams, 22nd Ed., Pg. 571.
7. You are delivering an obese primigravida at 41 weeks. After 15 min of pushing, the baby’s head delivers spontaneously but then retracts back against the perineum. As you apply gently downward traction to the head, the baby’s anterior shoulder fails to deliver. All of the following are appropriate next steps in the management of this patient, except:
In this clinical scenario, a shoulder dystocia is encountered. A shoulder dystocia occurs when the fetal shoulders fail to spontaneously deliver secondary to impaction of the anterior shoulder against the pubic bone, after delivery of the head has occurred. Shoulder dystocia is an obstetric emergency, and one should always call for help when such a situation is encountered. A generous episiotomy should always be made to allow the obstetrician to have adequate room to perform a number of manipulations to try to relieve the dystocia. Such maneuvers include the following: suprapubic pressure, McRoberts maneuver (flexing maternal legs upon the abdomen and abduct them), Wood’s corkscrew maneuver (rotating the posterior shoulder), and delivery of the posterior shoulder.
There is no role for fundal pressure because this action further impacts the shoulder against the pubic bone and makes the situation worse. Never give fundal pressure in cases of shoulder dystocia.
1. Williams, 22nd Ed., Pgs. 514–5.
8. A 38-year-old G3P2L2 at 40 weeks gestational age presents with pain and regular uterine contractions every 4–5 min. On arrival, the patient is in a lot of pain and requesting relief immediately. You check her cervix and note that it is 5 cm dilated. What is the most appropriate method of pain control for this patient?
The most appropriate modality for pain control in this patient is administration of an epidural block. An epidural block provides relief from the pain of uterine contractions and delivery. It is accomplished by injecting a local anesthetic agent into the epidural space at the level of the lumbar intervertebral space. An indwelling catheter can be left in place to provide continuous infusion of an anesthetic agent throughout labor and delivery via a volumetric pump.
When delivery is imminent, as in the case of this patient, a rapidly acting agent can be administered through the epidural catheter to affect perineal anesthesia. In this patient, intramuscular narcotics such as morphine would not be preferred because these agents can cause respiratory depression in the newborn. A pudendal block involves local infiltration of the pudendal nerve, which provides anesthesia to the perineum for delivery but no pain relief for uterine contractions. A local block refers to infusing a local anesthetic to the area of an episiotomy.
1. Williams, 22nd Ed., Pg. 483.
9. A 30-year-old primigravida at 39 weeks has been completely dilated and has been pushing for 3 h. She had taken epidural analgesia. She is exhausted and has a temperature of 37.8°C. The fetal heart rate is 170/min with decreased variability. The patient’s membranes have been ruptured for over 24 h. The patient’s cervix is completely dilated and effaced, and the fetal head is visible at the introitus between pushes. The fetal bones are at the +3 station. What is the most appropriate next step in the management of this patient?
Indications for an operative vaginal delivery with a vacuum extractor or forceps occur in situations where the fetal head is engaged, the cervix is completely dilated, and there is a prolonged second stage, suspicion of potential fetal compromise, or need to shorten the second stage for maternal benefit. In this situation, all the indications for operative delivery apply. This patient has been pushing for 3 h, which is the definition for prolonged second stage of labor in a nulliparous patient with an epidural. In addition, potential maternal and fetal compromise exists, since the patient has the clinical picture of chorioamnionitis and the fetal heart rate is not reassuring. It is best to avoid cesarean section, since it would take more time to achieve and since the patient is infected. At full dilatation and a suitable station, forceps is faster than LSCS.
1. Williams, 22nd Ed., Pgs. 549–50.
10. A 24-year-old primigravida woman, at term, has been dilated to 9 cm for 3 h. The fetal vertex is in the right occiput posterior position, at +1 station. There have been mild late decelerations for the last 10 min. Twenty minutes ago the fetal scalp pH was 7.27; it is now 7.20. Next line of management is:
A woman who has been dilated 9 cm for 3 h is experiencing a secondary arrest in labor. The deteriorating fetal condition (as evidenced e.g., by late decelerations and falling scalp pH) dictates immediate delivery.
As per ACOG guidelines only, outlet or low forceps should be attempted.
A forceps rotation would be inappropriate because the cervix is not fully dilated and, besides, in modern day obstetrics LSCS is preferred over rotation forceps.
Forceps are constructed so that their cephalic curve is closely adapted to the sides of the fetal head. The biparietal diameter of the fetal head corresponds to the greatest distance between the appropriately applied blades. Consequently, the head of the fetus is perfectly grasped only when the long axis of the blades corresponds to the occipitomental diameter, with the major portion of the blade lying over the face, while the concave margins of the blades are directed toward either the sagittal suture (occipitoanterior position) or the face (occipitoposterior position).
The pelvic inlet usually is considered to be contracted if its shortest anteroposterior diameter is less than 10 cm or if the greatest transverse diameter is less than 12 cm. The anteroposterior diameter of the pelvic inlet is commonly approximated by manually measuring the diagonal conjugate, which is about 1.5 cm greater. Therefore, inlet contraction is usually defined as a diagonal conjugate of less than 11.5 cm.
In women with contracted pelves, face and shoulder presentations are encountered three times more frequently, and cord prolapse occurs 4–6 times more frequently.
The midpelvis is likely contracted when the sum of the interischial spinous and posterior sagittal diameters of the midpelvis (normal, 10.5 + 5 cm = 15.5 cm) falls to 13.5 cm or below.
There is reason to suspect midpelvic contraction whenever the interischial spinous diameter is less than 10 cm. When it measures less than 8 cm, the midpelvis is contracted.
This finding usually is defined as an interischial tuberous diameter of 8 cm or less.
Outlet contraction without concomitant midplane contraction is rare.
Müller and Hillis both described a clinical maneuver to predict dis-proportion.
In an occiput presentation, the fetal brow and the suboccipital region are grasped through the abdominal wall with the fingers and firm pressure is directed downward in the axis of the inlet. Fundal pressure by an assistant is usually helpful. The effect to the forces on the descent of the head can be evaluated by concomitant vaginal examination. If no disproportion exists, the head readily enters the pelvis, and vaginal delivery can be predicted. Inability to push the head into the pelvis, however, does not necessarily indicate that vaginal delivery is impossible. A clear demonstration of a flexed fetal head that overrides the symphysis pubis, however, is presumptive evidence of disproportion.
PGF2α causes strong tetanic contractions of the whole of uterus (like methergin), so it is never used for induction of labor as it will lead to fetal distress and IUFD. It is mainly used in prevention and treatment of atonic PPH.
PGE1 and PGE2 cause cervical ripening, softening and uterine contractions and hence can be used for induction and augmentation of labor.
PGE2 is most commonly used at term for induction of labor. It is preferred over PGE1. It has got great collagenolytic properties and also sensitizes the myometrium to oxytocin.
PGE2 is available as gel or tablets.
ACOG has only recently approved use of 25 μg vaginal PGE1 (misoprostol) for cervical ripening. A 50 μg vaginal dose is associated with tachysystole/meconium passage aspiration/fetal distress.
Prostaglandins are more effective than oxytocin in cases of intra-uterine death or early gestational period with unfavorable cervix where oxytocin is less effective.
| Various Uses of Prostaglandins in Obstetrics | |
| Medical method of first trimester MTP (mifepristone followed by misoprostol) | Induction of labor (PGE2 and PGE1. PGE2 preferred as more safe) |
| Second trimester MTP (PGE1 and PGF2α, PGE1 preferred) | Acceleration of labor (PGE2 and PGE1. PGE2 preferred as more safe) |
| Management of atonic postpartum hemorrhage (PGF2α and PGE1) | Medical management of tubal ectopic pregnancy (PGF2α was used in the past as direct injection into the ectopic sac. Not used nowadays) |

Deflection of fetal head in relation to the pelvic inlet is called asynclitism.
When the sagittal suture lies anteriorly, the posterior parietal bone is the leading presenting part and is called posterior or Litzman asynclitism. It is more common in primigravidas due to good uterine and abdominal wall tone.
When the sagittal suture is more posterior and the anterior parietal bone is the leading presenting part, it is called anterior or Naegele’s asynclitism. It is more common in multiparous patients.
Cord prolapse is an obstetric emergency. After cord prolapse on exposure to external environment the whole cord goes into spasm, leading to severe decelerations in fetal heart rate and fetal distress. If the fetus is alive and mature enough for survival, immediate delivery should be done.
Risk factors for cord prolapse include:

(At full dilatation and a suitable station, forceps is faster than LSCS in delivering the baby).
Two main principles in management of obstructed labor are:
In patients of obstructed labor, the uterine contractions (power) are always adequate.
There is a problem with the passage or the passenger.
By increasing the power (by giving oxytocin) we are increasing the risk of rupture uterus.
It is like flogging a dead horse. Uterus is already contracting, and there is no point in increasing the contractions further in a case of obstructed labor.
The patient should be given IV fluids to correct the dehydration and ketoacidosis, which usually develops due to prolonged labor. Patient should be given antibiotics to prevent infection, and then steps should be taken to immediately relieve the obstruction either by instrumental deliver or by LSCS. LSCS may have to be done even if the baby is dead and if vaginal delivery is not possible, or else rupture uterus will occur.
NOTE: In cases of prolonged labor where there are hypotonic uterine contractions, oxytocin is justified.
Pain during first stage of labor is generated largely from the uterus.
Early in labor the pain of uterine contractions is transmitted predominantly through the T11 and T12 nerves.
Pain with vaginal delivery arises from stimuli from lower genital tract.
These are transmitted mainly through pudendal nerve (S 2,3,4)
Motor pathway to the uterus leave the spinal cord at the level of T7 and T8.
Complete analgesia from pain of labor and vaginal delivery necessitates a block from T10 to S5 dermatome
Methergin can be given by IM or IV route.
In routine management of third stage of labor IM methergin is given after placental delivery.
Active management of third stage of labor includes giving IV methergin at the time of delivery of anterior shoulder. The timing is very important because if given early it will give rise to shoulder dystocia.
The principle of active management is to induce strong uterine contractions, so that the placenta separates and immediately follows the delivery of baby. This decreases the time duration and blood loss during third stage of labor.
Absolute contraindications to the use of methergin are:
1. Chronic hypertension/preeclampsia/eclampsia
3. After the delivery of the first baby of the twins. (It can be given after 2nd baby delivery of twin.
Obviously the contraindications to the use of methergin are also the contraindications for active management of the 3rd stage of labor.
The only disadvantage of active management of third stage of labor is slightly increased incidence of retained placenta. This can happen because the placenta separates but the cervical os closes giving rise to trapped placenta.
NOTE: Rh negative pregnancy is a relative (not absolute) contraindication for use of methergin.
Caldwell and Moloy classification of pelvis
| Pelvis | Incidence (%) |
| Gynecoid | 50 |
| Anthropoid | 25 |
| Android | 20 |
| Platypelloid | 5 |

Android pelvis is a/w deep transverse arrest.
Anthropoid pelvis is a/w occipitoposterior position and face to pubis delivery.
Occipitoposterior (OP) is the most common malposition. Anthropoid and android variety of pelvis favor this position.
In cases of occipitoposterior position the best management is to wait and watch.
In around 80% cases there is a long anterior rotation through 3/8th of a circle and normal delivery like occipito anterior will take place.
Only if there are inadequate uterine activity then oxytocin augmentation is required.
Per say, OP is not an indication for LSCS.
If there is a short anterior rotation then a deep transverse arrest will happen and then LSCS is required.
Oblique posterior arrest and occipito sacral arrest are indications for LSCS.
The main risk of trial of scar (V.B.A.C) is scar dehiscence & rupture uterus.
Rupture of previous LSCS scar is the most common cause of rupture uterus.
Hematuria is seen with rupture uterus and also with impending rupture of scar.
Clinical features of impending scar rupture (scar dehiscence)
Unexplained tachycardia
Hypotension
Fetal tachycardia
Uterine scar tenderness
Bleeding PV
Hematuria
Methods for induction of labor include:
2. Prostaglandins (PGE1 and PGE2): Prostaglandins act on the cervix to enable ripening by a number of different mechanisms. They alter the extracellular ground substance of the cervix and PGE2 increases the activity of collagenase in the cervix. They cause an increase in elastase, glycosaminoglycan, dermatan sulfate, and hyaluronic acid levels in the cervix. A relaxation of cervical smooth muscle facilitates dilation. Finally, prostaglandins allow for an increase in intracellular calcium levels, causing contraction of myometrial muscles. Risks associated with the use of prostaglandins include uterine hyperstimulation and maternal side effects such as nausea, vomiting, diarrhea, and fever.
PGE2 is available in the form of gel and tablets. Misoprostol (PGE1) tablets can also be used vaginally.
3. Mifepristone: Mifepristone is an antiprogesterone agent. Progesterone inhibits contractions of the uterus, while mifepristone counteracts this action.
PGF2α is not available in tablet form. It ia available as intramuscular injection.
It has action similar to Methergin. It causes a strong titanic contraction of the entire uterus, and hence, it is used only for prevention and treatment of PPH.
1. Brow is the rarest presentation.
2. Brow is commonly unstable and converts into either vertex or face.
3. Supra-orbital ridges and anterior fontanelle can be palpated on P/V examination.
4. There is no mechanism of labor in persistent brow presentation. Delivery is by LSCS.
5. It is associated with contracted pelvis or fetal macrosomia.
Clinical features of impending scar rupture (scar dehiscence):
Hematuria in case of rupture is due to injury to bladder and in case of dehiscence is due to pelvic congestion.
Passage of meconium does not mean that there is fetal distress. It was an old concept that:
Passage of meconium = Fetal distress
But this does not hold true anymore. Baby can pass meconium even without distress (e.g., postdatism).
Patient has presented at term and is in labor since 10 hours. This could be either prolonged latent phase of labor or false labor. Best plan is to give sedation to the patient and wait and watch.
Patients in false labor sleep and awake without contractions. But patients in latent phase show cervical changes and will progress after period of sleep.
Amniotomy (ARM) should be done in active labor. There is no need of doing LSCS at present.
Methylergometrine (Methergin) can be used in the prevention and treatment of PPH. Absolute contraindications to the use of Methergin are:
1. Chronic hypertension/preeclampsia/eclampsia
3. After the delivery of the first baby of the twins. (It can be given after second baby delivery of twin.)
Hence, if the patient has a heart disease and develops PPH, Methergin is absolutely contraindicated. Obviously, the contraindications to the use of Methergin are also the contraindications for active management of the third stage of labor.
Two main principles in the management of obstructed labor are:
In patients of obstructed labor, the uterine contractions (power) are always adequate.
The patient should be given i.v. fluids to correct the dehydration and ketoacidosis, which usually develop due to prolonged labor. Patient should be given antibiotics to prevent infection and then steps should be taken to immediately relieve the obstruction by LSCS.
LSCS may have to be done (even if the baby is dead) if vaginal delivery is not possible, or else, rupture uterus will occur.
In modern-day obstetrics, destructive operations (decapitation, craniotomy, evisceration, etc) are never to be performed as they are more dangerous and can lead to complications like rupture uterus and bladder injury.
LSCS is much safer than destructive operations.
NOTE: So remember that if vaginal delivery is not possible, then LSCS has to be done. Destructive operations never to be marked as the answer.
Breech is the most common malpresentation.
The most difficult and dangerous part in vaginal breech delivery is the delivery of the after-coming head.
The breech and limbs being soft can easily deliver, but there is a danger of head getting entrapped, leading to perinatal morbidity and mortality.
Three types of vaginal breech deliveries are described, as follows:
• Spontaneous breech delivery: No traction or manipulation of the infant is used. This occurs predominantly in very preterm, often previable, deliveries.
• Assisted breech delivery: This is the most common type of vaginal breech delivery. The infant is allowed to spontaneously deliver up to the umbilicus, and then maneuvers are initiated to assist in the delivery of the remainder of the body, arms, and head.
• Total breech extraction: The fetal feet are grasped, and the entire fetus is extracted. Total breech extraction should be used only for a non-cephalic second twin or in cases of fetal distress; it should not be routinely used for a singleton fetus because the cervix may not be adequately dilated to allow passage of the fetal head.
Extension of head (stargazing fetus), hydrocephalus, and incomplete dilatation of cervix, all will create problems in delivery of the fetal head, leading to difficult second stage and head entrapment and morbidity and mortality.
Question of vaginal delivery does not occur in case of placenta previa.
Patients with placenta previa (placenta is in front of presenting part) are to be delivered by LSCS (whether it is vertex or breech). There would be profuse hemorrhage leading to maternal mortality if vaginal delivery is attempted in cases of placenta previa.
• In modern-day obstetrics forceps is not applied if station is above +2 (station should be at least +2 before applying forceps).
• Forceps can be applied in vertex and face presentation and also in cases of after-coming head of breech.
• Sagittal suture at 15° to anteroposterior diameter means that the rotation required is 15° (rotation should not exceed 45°).
| Procedure | Criteria |
| Outlet | |
| Low | |
| Midpelvic | Station above +2 cm but head is engaged |
| High | Not included in classification |

Active management of the third stage of labor is highly effective at preventing postpartum hemorrhage (PPH). In a systematic review of randomized controlled trials, active management of the third stage of labor was more effective than physiological management in preventing blood loss.
Active management of the third stage of labor (AMTSL) includes 3 steps:
1. Administration of auterotonic drug (oxytocin, 10 IU injection, is the drug of choice).
3. Uterine massage after delivery of placenta, followed by palpation of the uterus every 15 minutes for 2 hours to assess the continued need for massage.
Oxytocin (10 IU), administered intramuscularly, is the preferred medication and route for the prevention of PPH in low-risk vaginal deliveries. Care providers should administer this medication after delivery of the anterior shoulder. Intravenous infusion of oxytocin (20–40 IU in 1000 mL, 150 mL/h) is an acceptable alternative for AMTSL.
Ergometrine (Methergin) can be used for prevention of PPH but may be considered second choice to oxytocin owing to the greater risk of maternal adverse effects and of the need for manual removal of a retained placenta. Ergometrine 0.2 mg IM and misoprostol 600–800 mg given by the oral, sublingual, or rectal route may be offered as alternatives in vaginal deliveries when oxytocin is not available.
Timing of cord clamping (early or late) is controversial at present. There are no clear guidelines available at present. But as mentioned in earlier MCQ, cord clamping is a part of second stage of labor.
31. Mrs. AR, G3P1L1A1 is admitted in labor in a full-term pregnancy. On examination, she has uterine contractions 2/10 minutes, lasting 30–35 seconds, cervix is 4 cm dilated, membranes intact and 3/5ths of the head palpable per abdomen. On repeat examination 4 hours later, cervix is 5 cm dilated, station is unchanged, and the cervicograph remains to the right of the alert line. Which of the following statements is true?
Three-fifths of the head was palpable at the time of presentation. This indicates that the head is not engaged.
The head is said to be engaged when only 1/5th of the head is palpable per abdomen.
In active labor, rate of cervical dilation in a multigravida should be 1.5–2 cm/h.
In this multigravida patient, in 4-hour duration, cervix has dilated only 1 cm, and therefore, the cervicograph progress is obviously not satisfactory.
Some intervention is needed at present in terms of either oxytocin augmentation or doing an ARM and reassessment of the fetal position and pelvis (rule out CPD).

The alert line starts at 1 cm in ‘0’ hours and ends at 10 cm in 9 hours. The action line is drawn 2 hours to the right and parallel to the alert line.

In this patient, the cervicograph would have touched the action line if in 5 hours there was no change in cervical dilation, i.e., if the patient would have remained 4 cm dilated. If the cervicograph is on alert line, then it touches the action line if there is no dilation for 2 hours.
When the cervicograph touches the action line or crosses it, the pregnancy should be terminated by lower segment cesarean section (LSCS) immediately.
A patient of previous LSCS attempting a vaginal delivery is called a trial of scar (as the previous scar is put to trial).
Trial of scar is absolutely contraindicated in CPD/contracted pelvis.
In case of previous classical CS, the risk of rupture of uterus during trial is 4–9 %, hence trial of scar is absolutely contraindicated.
Recommendations useful for the selection of candidates for vaginal birth after cesarean delivery (ACOG Guidelines)
1. No more than one prior LSCS.
2. Clinically adequate pelvis (no CPD).
3. No other uterine scars or previous rupture.
4. Physician immediately available throughout active labor who is capable of monitoring labor and performing emergency cesarean.
5. Availability of anesthetist and operation theatre facilities.
The success rate for a trial of scar depends to some extent on the indication for the previous cesarean delivery. Generally, about 60–80% of trials after and to prior cesarean birth result in vaginal delivery; with success being maximum if previous cesarean section was because of breech presentation.
Comparisons: Forceps versus vacuum
There are significantly more third- and fourth-degree perineal lacerations, with forceps. Conversely, the incidence of cephalohematomas is more with the vacuum. Investigators have found decreased maternal trauma by vacuum compared with forceps.
Although retinal hemorrhage occasionally is seen with vacuum usage, it has no apparent long-term effects. Johanson and Menon analyzed 10 randomized trials and confirmed that vacuum extraction was associated with less maternal but more fetal trauma, for example, cephalohematoma and retinal hemorrhage.
The 2 major types of scalp injury associated with vacuum operations are the cephalohematomas and the relatively rare, but potentially life-threatening, subgaleal hemorrhages.
Vacuum extraction has a lower rate of maternal injury in comparison with forceps.
Vacuum requires less clinical expertise as compared to forceps.