Skeleton
Learning objectives
After studying this chapter, the student should be able to:
• enumerate the types of skeleton and list the bones in each type
• list the functions of the bone
• enumerate the different type of cells of bone
• classify the bones according to their shape and give an example of each
• describe the sesamoid bones and list their characteristic features
• outline the parts of a growing long bone and discuss its arterial supply
• describe intramembranous ossification
• describe intracartilaginous ossification
• compare and contrast the structure of compact and spongy bones
• classify different types of cartilages and give an example of each
• describe the growth of the bone
• discuss remodeling of bone and its clinical significance
• correctly solve the review questions given at the end of the chapter
Introduction
The skeleton of the body is composed of bones and cartilages. Both bones and cartilages are made up of specialized connective tissue called skeletal (sclerous) tissue, which can bear weight without bending and has considerable tensile strength. The skeletal tissue consists of same components (e.g. cells, matrix) as that of general connective tissue, but physically differs from it as its matrix is solidified.
The functions of skeletal system are as follows:
Types of the skeleton
For the convenience of study, the skeleton is divided into two types (Fig. 6.1):
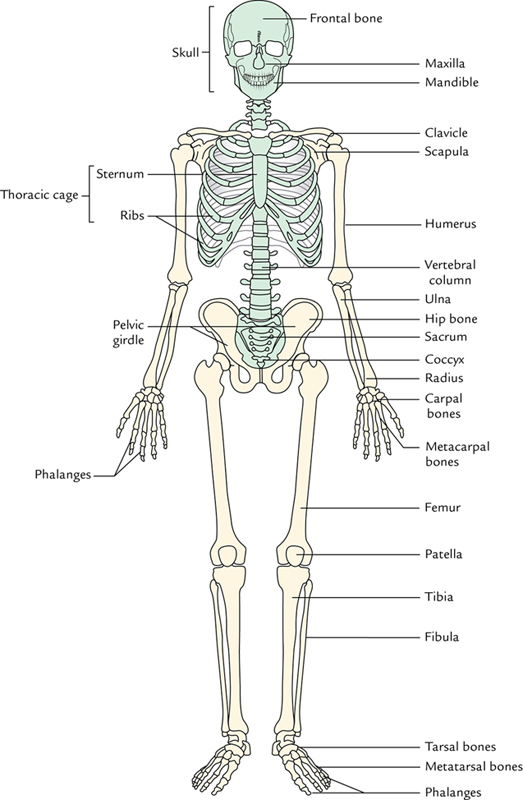
Axial skeleton
The axial skeleton consists of bones and cartilages that lie close to the central axis of the body. It includes skull, auditory ossicles, hyoid bone, vertebral column, and rib cage:
1. Skull: It consists of two sets of bones—the cranial bones that form the cranium or brain case and the facial bones.
2. Auditory ossicles: These are the three small bones present in each middle ear cavity.
3. Hyoid bone: It is located above the larynx and below the lower jaw.
4. Vertebral column (back bone): This consists of 33 vertebrae, 7 cervical, 12 thoracic, 5 lumbar, 5 sacral and 4 coccygeal; however, sacral vertebrae fuse to form sacrum and coccygeal vertebrae fuse to form coccyx, thus vertebral column consists of 26 individual or movable bones (vertebrae).
5. Rib cage: It forms the bony and cartilaginous framework of the thorax. The bone forming the rib cage includes 12 pairs of ribs with associated costal cartilages and sternum (breast bone).
Appendicular skeleton
The appendicular skeleton is bilaterally symmetrical and comprises the bones of the upper and lower extremities (or limbs) and bony girdles which anchor these extremities with the axial skeleton. Thus, it includes bones of pectoral girdle, upper limb, pelvic girdle and lower limb (Fig. 6.1).
1. Pectoral girdle: It consists of paired scapulae and clavicles. It is not a complete girdle as it is attached only anteriorly.
2. Bones of upper limb: Each upper limb contains the humerus within the arm (brachium); the radius and ulna within the forearm (antebrachium); the carpal bones, the metacarpal bones and the phalanges within the hand.
3. Pelvic girdle: It consists of two hip bones. It is a complete girdle as it is united anteriorly with symphysis pubis and posteriorly with the sacrum of vertebral column.
4. Bones of lower limb: Each lower limb contains the femur within the thigh; the tibia and fibula within the leg; the tarsal bones, the metatarsal bones and the phalanges within the foot.
The bones forming axial and appendicular skeleton are listed in Table 6.1 and shown in Figure 6.1.
Table 6.1
Number of bones present in axial and appendicular skeleton
| Number of bones | |
| Axial skeleton | |
| Skull | |
| Cranial bones | 8 |
| Facial bones | 14 |
| Hyoid | 1 |
| Ear ossicles (3 in each ear) | 6 |
| Vertebral bones | 26 |
| Rib cage | |
| Sternum | 1 |
| Ribs | 24 |
| Total | 80 |
| Appendicular skeleton | |
| Pectoral (shoulder) girdles | |
| Clavicle | 2 |
| Scapula | 2 |
| Upper limbs | |
| Humerus | 2 |
| Ulna | 2 |
| Radius | 2 |
| Carpals | 16 |
| Metacarpals | 10 |
| Phalanges | 28 |
| Pelvic (hip) girdle | |
| Hip bone | 2 |
| Lower limbs | |
| Femur | 2 |
| Fibula | 2 |
| Tibia | 2 |
| Patella | 2 |
| Tarsals | 14 |
| Metatarsals | 10 |
| Phalanges | 28 |
| Total | 126 |
| Total bones of axial skeleton | 80 |
| Total bones of appendicular skeleton | 126 |
| Total bones of the body | 206 |
Bones
The bones are the hard structures, which form the rigid framework of the body.
Structurally, bone is a highly vascular mineralized connective tissue consisting of cells and dense intercellular organic matrix impregnated with inorganic salts. The organic material mainly consists of collagen fibers and forms one-third of the bone. It provides resilience to the bone. The inorganic material mainly consists of calcium phosphate and traces of other salts. It provides hardness and rigidity to the bone and makes it radiopaque in x-ray films.
The bone is not an inert material as often thought of by some students but it is a living structure. It is supplied by blood vessels, lymph vessels and nerves. It has the power of regeneration and repair. In fact, bones have greater regenerative power than any other tissues of the body, except blood.
The bones are subject to diseases like any other tissue of the body.
Functions of bones
The following are the functions of bones:
1. Form rigid framework of the body to give it a shape and support.
2. Provide surface for attachment of muscles, tendons, ligaments, etc.
3. Serve as levers for muscles to bring about a movement.
4. Protect certain viscera, e.g. brain, spinal cord, heart, lungs, liver, bladder, etc.
5. Contain marrow which is factory of blood cells, e.g. white blood cells, red blood cells and platelets.
6. Storehouse of calcium and phosphorus, about 95% of the phosphorus within the body is deposited in the bones and the teeth.
7. Some bones around the nose contain large cavities filled with air (paranasal air sinuses which affect the timber of the voice).
Microscopic structure of bones
The bone is a specialized connective tissue and consists of the following three components:
The ground substance and fibers together form the intercellular substance or matrix which gets mineralized.
Cells:
The bone cells are of three types: osteoblasts, osteocytes and osteoclasts.
Osteoblasts
1. The osteoblasts are derived from pluripotent osteoprogenitor cells located in mesenchyme, periosteum and endosteum.
2. They secrete osteoid, which is unmineralized matrix, consisting of proteoglycans, glycoproteins and type I collagen fibers.
(a) For mineralization to occur, the osteoblasts secrete osteocalcin and alkaline phosphatase which release calcium and phosphate radicals from substances containing them.
(b) In addition, osteoblasts release matrix vesicles (membrane bound vesicles), which concentrate calcium and phosphate, and are the most important factors necessary for mineralization to occur.
Osteocytes
1. The osteocytes are derived from osteoblasts. Once an osteoblast becomes surrounded by matrix, it becomes an osteocyte.
2. The osteocytes are flattened cells with numerous cytoplasmic processes. They are located in spaces within matrix called lacunae and canaliculi, respectively. The cytoplasmic processes of neighboring cells communicate by gap junctions.
3. The osteocytes unlike osteoblasts do not undergo mitosis.
4. The canaliculi radiate from each lacuna and permit diffusion of nutritive material (Fig. 6.2). Thus, cells remain alive in calcified matrix and maintain the bone by their balanced osteogenic and osteoclastic activity. They secrete alkaline phosphatase to maintain calcification. When bone cells die, the matrix is decalcified.

Osteoclasts
1. The osteoclasts are derived from the fusion of uncommitted cells of red bone marrow that are related to a type of white blood cell called monocyte similar to the formation of giant cells by the fusion of macrophages.
2. They are large cells with multiple nuclei.
3. They help in resorption of the bone and play an important role in bone remodeling.
4. They reside in shallow depressions of the bone called Howship’s lacunae.
Ground substance:
It consists of the following components:
1. Proteoglycans containing a side chain of glycosaminoglycans (GAGs), specifically chondroitin sulfate and keratan sulfate.
2. Glycoproteins, such as osteonectin and osteocalcin (a calcium binding protein).
3. A mineral component that includes hydroxyapatite (calcium phosphate crystals), citrate ions and bicarbonate ions. Mineral component mainly consists of hydroxyapatite crystals of calcium phosphate (Ca10[PO4]6[OH]2), and contributes to the hardness/rigidity of bone.
4. Water (tissue fluid), which contributes to a low degree of bone hydration (7%).
Fibers:
They are type I collagen fibers and provide tensile strength to the bone.
Classification of bones
The bones are usually classified in three ways:
(b) According to the structure (structural classification)
(c) According to the development (developmental classification)
A. Classification according to the shape
Depending on the size, shape, etc., the bones are classified into the following types (Fig. 6.3):

Long bones are those in which length exceeds the breadth and thickness. The long bones are of two types: typical and miniature/short.
(a) Typical long bones. They have the following features:
1. Consists of three parts: one elongated tubular shaft (diaphysis) and two expanded ends (epiphyses).
2. Contain medullar cavity filled with bone marrow.
(b) Miniature/short long bones: These are much shorter in length as compared to typical long bones with epiphysis present at one end only.
The examples of miniature long bones are metacarpals, metatarsals and phalanges. All the metacarpals and metatarsals have epiphysis at their distal end except first metacarpal and first metatarsal which have epiphysis at their proximal end.
Short bones are small in size and usually cuboidal in shape, presenting six surfaces. These bones are found in wrist (carpal bones) and foot (tarsal bones).
Flat bones are flat and shallow plate-like bones. They form boundaries of certain body cavities, e.g. cranium, thoracic cavity. The examples of flat bones include: (a) bones forming cranial vault (frontal, parietal, occipital, etc.), and (b) bones forming thoracic cage (scapulae, ribs, sternum, etc.).
Irregular bones are highly irregular in shape, viz. hip bone, vertebrae, bones forming base of the skull.
Pneumatic bones are a variety of irregular bones which contain air-filled cavity or cavities within them. These bones are mainly located around the nasal cavity, viz. maxilla, frontal, sphenoid and ethmoid bones. The air-filled cavities in these bones are called paranasal air sinuses.
The paranasal air sinuses not only make the skull light but also add resonance to the voice. They also act as air conditioning chambers for the inspired air.
Sesamoid bones (Arab. sesame = seed) are seed-like bony nodules which develop in certain muscle tendons where they rub against convex bony surfaces during the movements of the joint. The rubbing surface of the sesamoid bone is covered with an articular cartilage.
Sites of sesamoid bones
1. Patella in the tendon of quadriceps femoris in front of the knee joint.
2. Fabella in the lateral head of gastrocnemius behind the knee joint.
3. Two sesamoid bones below the head of the first metatarsal bone in the tendon of flexor hallucis brevis.
4. One sesamoid bone in the tendon of peroneus longus where it binds around the cuboid bone.
5. Pisiform in the tendon of the flexor carpi ulnaris.
6. One sesamoid bone on the ulnar side of the head of 1st metacarpal bone in the tendon of adductor pollicis.
7. Sometimes a sesamoid bone is found on the radial side of head of 1st metacarpal in the tendon of flexor pollicis brevis.
Functions of sesamoid bones
Characteristics of sesamoid bones
Accessory bones
These are bones that are not generally present in the body. If present they do not cause any harm, sometimes clinicians confuse it with a fractured bone. Accessory bones may be formed due to:
1. Appearance of extra ossification centers in skull sutures, viz. sutural or wormian bones.
2. Nonfusion of an epiphysis. The examples are:
(a) Os trigonium: the posterior tubercle of the talus that fails to fuse with the rest of the bone.
(b) Os vesalianum: the styloid process of the 5th metatarsal that fails to fuse with the rest of the bone.
(c) Patella cubiti: occasionally, the center of ossification for the olecranon process of ulna fails to fuse to the proximal end of the shaft.
B. Structural classification
Macroscopically (i.e. as seen on naked eye examination of a section of a long/flat bone), the architecture of bone may be compact (dense) or cancellous (spongy).
Most bones of the body have a basic structure of an outer region of compact bone and inner region of spongy (cancellous) bone. For example:
1. In long bones, the shaft consists of compact bone forming a cylinder that surrounds a central cavity called medullary cavity. The ends of long bones consist of cancellous bone surrounded by a thin layer of compact bone.
2. In flat bones of the skull, the cancellous bone is sandwiched between the plates of compact bone. The spongy part is called diploe and outer and inner plates of compact bone are called inner and outer tables.
Compact (dense) bone
The texture of compact bone is dense, ivory-like with no visible spaces on naked eye examination. The compact bone consists of (a) lamellae of collagenous sheets, and (b) haversian systems or osteons (Fig. 6.4).

Lamellae
The compact bone consists of three types of bony lamellae:
Haversian system (osteon)
Each haversian system consists of a haversian canal (or central canal), surrounded by concentric lamellae of bone.
Haversian canal runs parallel to the long axis of the bone and contains blood vessels, nerves and loose connective tissue.
The concentric lamellae, 4–20 in number, form rings around haversian canal. The osteocytes are located between the lamellar rings in lacunae.
The lacunae communicate with one another in between and across the lamellae, and with the central canal by numerous radiating canaliculi.
Haversian canals are lined by endosteum and communicate with each other, with the medullary cavity and with the surface of bone by numerous Volkmann’s canals. The Volkmann’s canals run perpendicular to the long axis of the bone.
The blood vessels from the periosteum or endosteum enter the bone through Volkmann’s canals.
The haversian canals receive blood vessels from Volkmann’s canals.
The osteocytes receive nutrients and eliminate waste products through the canal system.
Cancellous (spongy) bone
The cancellous bone is a meshwork of bony spicules. It consists of interconnecting rods and plates of bone called trabeculae, enclosing large spaces filled with red bone marrow. The trabeculae:
(a) consist of superimposed lamellae and do not form haversian system because they get nutrition from the blood vessels of tissues around them;
The differences between the compact and spongy bone are given in Table 6.2.
Table 6.2
Difference between compact and spongy bone
| Compact bone | Spongy bone | |
| Density | Dense like an ivory | Porous like a sponge |
| Haversian systems | Present | Absent |
| Arrangement of bony lamellae | Regular | Irregular |
| Location in bone | Outer region | Inner region |
| Bone marrow | Absent | Present |
| Amount in the body by weight | 75% | 25% |
Wolff’s Law (Trajectory theory of Wolff, 1892): According to this law, the bone formation (osteogenesis) is directly proportional to stress and strain. The tensile force favors bone formation, whereas compressive force favors bone resorption. This theory, however, no longer holds good because now it is noticed that both tensile and compressive forces can stimulate bone formation in appropriate conditions.
The architecture of cancellous bone is often interpreted in terms of Wolff’s law. Thus, the arrangement of bony lamellae is governed by the lines of maximal stress (Fig. 6.5):
1. Pressure lamellae are arranged parallel to the line of weight transmission.
2. Tension lamellae are arranged at right angles to the pressure lamellae.

Microscopically, bones are of two types:
This classification is based on the manner in which the different components of the matrix are arranged.
Woven bone:
The collagen fascicles and bone crystals within a woven bone are arranged randomly forming a network resembling the warp and weft of a woven fabric and hence the name ‘woven bone’. The examples of woven bone are young fetal bones (most immature bone), callus at fracture repair sites.
Lamellar bone:
In lamellar bone, the mineralized matrix is arranged in thin layers (lamellae). The lamellae are arranged in two different patterns:
1. In number of concentric cylindrical units (haversian system), e.g. compact bone.
2. In number of branching and anastomosing curved plates, e.g. spongy bone.
C. Developmental classification
According to the process of bone development (ossification), the bones are of the following three types:
1. Membranous bones (membrane bones), developed by membranous ossification.
2. Cartilaginous bones (cartilage bones), developed by endochondral ossification.
3. Membrano-cartilaginous bones, developed by both membranous and endochondral ossification.
For details see development of bones on page 77.
The examples of bones according to their development are enumerated in Table 6.3.
Table 6.3
Examples of bones according to their development
| Types of bones | Examples |
| Membranous | Bones of cranial vault
Facial bones |
| Cartilaginous | Bones of limbs
Bones of base of skull Bones of vertebral column (vertebrae) Bones of thoracic cage (ribs, sternum) |
| Membrano-cartilaginous | Mandible
Clavicle Occipital bone Temporal bone Sphenoid bone |
Gross structure of a typical long bone
A typical long bone consists of three parts: a shaft (or body) and two ends (Fig. 6.6).
1. The shaft is an elongated part between the two expanded ends. It is made of an outer thick shell of compact bone (cortex) enclosing a cavity called medullary cavity, thus providing maximum strength with minimal material and weight.
The medullary cavity is filled with yellow bone marrow (remember that at birth it is filled with red bone marrow and is involved in active hemopoiesis).
2. The ends are knobby (expanded) and largely made up of cancellous bone covered by a thin shell of a compact bone. The ends of long bone are covered by an articular hyaline cartilage and take part in the formation of joints.

Periosteum and endosteum
The outer surfaces of all the bones are covered by a thick fibrous membrane called periosteum, whereas their inner surfaces are lined by a thin fibrous membrane called endosteum. Both periosteum and endosteum contain osteoprogenitor cells, osteoblasts and osteoclasts which are essential for formation, remodeling and repair of bone.
The periosteum (Figs 6.4 and 6.6) is a thick fibrous membrane covering the entire surface of bone except at the areas covered by an articular cartilage. At the articular margin, the periosteum is continuous with the joint capsule.
It is made up of two layers:
The periosteum is united to the underlying bone by extrinsic collagen fibers, the Sharpey’s fibers. These are coarse collagenous fibers from inner layer which extends inward to penetrate the bone matrix (outer cortical bone tissue) like spikes of a shoe, thus bolting the periosteum to the bone.
Functions of periosteum
1. Protects and maintains the shape of the bone.
2. Nourishes the outer part of the underlying cortex by abundant periosteal arteries.
3. Provides attachment to ligaments, tendons, muscles and intermuscular septa.
The endosteum is cellular membrane that lines the medullary cavity of the shaft. The osteoblasts and osteoprogenitor cells within the endosteum play an important role in bone remodeling and repair.
Nutrient foramen is usually present near the middle of shaft for the entry of nutrient artery.
Bone marrow
The bone marrow is a soft, loose, vascular tissue consisting of delicate network of reticular fibers and various types of cells. It is the main site of hemopoiesis.
It is present in the medullary cavity of the long bones and in the cavities of the spongy bone.
Types of bone marrow
Two types of bone marrow are described according to their appearance on gross examination.
Red bone marrow:
It is vascular and appears red in color due to the presence of red blood cells. It consists of network of fine reticular fibers containing blood forming cells, showing all stages of development: immature (nucleated) and mature (non-nucleated) red blood cells, myeloblasts, myelocytes, granulocytes, megakaryocytes, etc. At birth it is present in all the bones at all sites, and is an important site of hemopoiesis, but as the age advances the marrow in the medullary cavity of long bones is gradually replaced by yellow marrow. Hence in the adults, the red marrow is found in the cancellous bone. The sites (Fig. 6.7) are as follows:

Yellow bone marrow:
It mainly consists of adipose tissue. However, few hemopoietic elements may be found in it. Under certain conditions, such as severe bleeding or hypoxia, yellow bone marrow converts back into red bone marrow.
Parts of growing (young) long bone
A typical long bone develops from a preformed model of hyaline cartilage in three parts: two ends and an intervening shaft. The two ends are formed by secondary centers of ossification and the shaft is formed by primary center of ossification. Before the ossification is complete, the following parts can be defined in the young long bone (Fig. 6.8):

Epiphyses:
These are ends of long bones which ossify from secondary centers.
Types of epiphyses
The epiphyses are of the following four types (Fig. 6.9):
1. Pressure epiphysis: It is covered by an articular cartilage and takes part in the transmission of body weight, e.g. head of femur, humerus, lower end of radius, etc.
(a) It is produced by a pull of the muscle or muscles, e.g. greater and lesser trochanters of femur, greater and lesser tubercles of humerus, etc.
(b) It is always nonarticular and provides attachment to the muscle or muscles.
3. Atavistic epiphysis: It is an independent bone in lower mammals, which in man gets fused to the nearest bone to receive nutrition from the host bone. It grows like a parasite, e.g. coracoid process of scapula, posterior tubercle of talus which is also known as os trigonum.
4. Aberrant epiphysis: It is an epiphysis which appears at unusual end of a short long bone, e.g. epiphysis at the head of first metacarpal. Remember, normally epiphysis appears at the base of the first metacarpal bone.

Epiphyseal (growth) plate:
It is a plate of hyaline cartilage which intervenes between the epiphysis and diaphysis of a growing long bone. The proliferation of cells in the epiphyseal cartilage is responsible for growth in length of a long bone (for details see page 85). After the fusion of epiphysis with diaphysis, the bone can no longer grow in length. The epiphyseal plate/cartilage is nourished by both epiphyseal and metaphyseal arteries.
Metaphysis:
The end of diaphysis toward the epiphyseal cartilage is called metaphysis. It is the most actively growing area of a long bone. Before fusion of epiphysis, the metaphysis is profusely supplied by blood from nutrient, periosteal and juxta-epiphyseal arteries. These are end arteries and form hair-pin-like bends. Therefore, metaphysis is the common site of osteomyelitis in children for bacteria and emboli are easily trapped in the hair-pin bends leading to infarction. After the epiphyseal fusion the communications are established between the epiphyseal and metaphyseal arteries, as a result metaphysis contains no more end arteries. For this reason, osteomyelitis in this region is rare in adults.
Diaphysis:
It is the elongated part of bone between the metaphyses. It develops from primary ossification center.
Blood supply of bones
1. Blood Supply of a Long Bone: The long bone is supplied by the following four sets of arteries: nutrient artery, periosteal arteries, metaphyseal arteries and epiphyseal arteries (Fig. 6.10).
(a) Nutrient artery: It enters the middle of the shaft through a nutrient foramen, runs obliquely through the cortex and then divides into ascending and descending branches in the medullary cavity. Each branch then subdivides into a number of smaller parallel vessels which enter the metaphysis and form hair-pin loops. These loops anastomose with epiphyseal, metaphyseal (juxta epiphyseal) and periosteal arteries. Therefore, the metaphysis is the most vascular zone of the long bone.
The nutrient artery supplies the medullary cavity containing bone marrow and inner two-third of the outer shell of compact bone of diaphysis and metaphysis.

(b) Periosteal arteries: They are numerous and ramify beneath the periosteum. They enter the bone through Volkmann’s canals to supply the outer one-third of the cortex. The periosteal vessels are especially numerous beneath the muscular and ligamentous attachments.
(c) Metaphyseal (juxta-epiphyseal) arteries: They are derived from neighboring arteries and enter the metaphysis directly along the attachment of joint capsule.
(d) Epiphyseal arteries: They are derived from arterial anastomosis around the joint (circulus vasculosus). They enter the epiphysis either directly or after piercing the epiphyseal cartilage.
2. Blood Supply to Short Long Bones: To an extent it is similar to that of a long bone except that:
(a) The nutrient artery enters the middle of the shaft and immediately divides to form a plexus.
(b) The periosteal vessels supply the major part of the bone in adult and replace the nutrient vessels.
3. Blood Supply of a Vertebra: It is supplied by three sets of vessels:
(a) One or more large but short vessels enter the body from its posterior aspect through basivertebral foramen.
(b) A set of small vessels pierce the anterolateral surface of the body.
(c) A set of long vessels pierce the root of the transverse processes and supply the vertebral arch, and transverse and spinous processes.
4. Blood Supply of a Rib: It is supplied by two sets of vessels:
Fracture of bone
The fracture is a break in the continuity of the bone. It is the most common type of bone injury. Fracture mostly occurs due to trauma (traumatic fractures), however, they may occur spontaneously due to disease that weakens the bone (spontaneous or pathological fractures).
A fracture may be simple or compound.
1. Simple or closed fracture: the fractured bone is not exposed to the exterior through skin.
2. Compound fracture: the fractured bone is exposed to the exterior through an opening in the skin.
When a bone fractures, the treatment involves realigning the broken ends and then immobilizing them until the fracture is healed (repaired).
Repair of a fractured bone
It involves the following steps:
1. When bone is fractured, the blood collects and coagulates to form fracture hematoma in and around the fracture site.
2. Two or three days later, new blood capillaries and uncommitted cells from the surrounding tissue invade the hematoma.
3. After 1 week, some of the uncommitted cells differentiate into fibroblasts, which produce a fibrous network between fractured ends. The other cells differentiate into chondroblasts, which produce islets of fibrocartilage in the fibrous network forming a fibrocartilage callus (temporary callus).
4. The osteoprogenitor cells in the periosteum and endosteum around the fracture site proliferate and differentiate into the bone-forming cells, the osteoblasts, which invade the temporary callus and lay down the woven-bone (primary bone tissue or osteoid) which unites the extremities of the fractured bone. It is called bony callus.
5. The primary bone tissue of the callus is gradually replaced by a secondary bone (mature bone).
6. Remodeling takes place and restores the original bone structure.
Figure 6.11 depicts repair of a fractured bone.

Development and growth of bones
Development
All the bones develop from a mesenchyme by a process called ossification.
Ossification
As stated above it is the process of bone formation.
Types of ossification
There are two types of ossifications:
In intramembrane ossification mesenchymal models of bones undergo ossification, while in intracartilaginous ossification, cartilaginous models of bones undergo ossification. The details are as under:
Intramembranous ossification:
It involves the following steps:
Step 1: Mesenchymal tissue condenses to form a membranous sheet model. Osteoprogenitor cells located in this sheet differentiate into osteoblasts. The sites where the osteoblasts first appear are called ossification centers.
Step 2: Osteoblasts secrete organic substance (ground substance and collagen fibers) in the intercellular spaces to form osteoid tissue or bone matrix.
Step 3: Under the influence of alkaline phosphatase secreted by osteoblasts, the osteoid tissue is mineralized with calcium salts to become bone. The osteoblast now becomes trapped in mineralized matrix and are called osteocytes.
The intramembranous ossification is shown in Figure 6.12. Bones formed by the intramembranous ossification include flat bones of skull, viz. frontal, parietal, occipital, clavicle, etc.

Intracartilaginous (endochondral) ossification:
The intracartilaginous ossification is more complicated, but clinically more important because all the long bones of limbs (and many others) are ossified by this process.
It involves the following steps (Fig. 6.13):

Step 1: The cartilage cells (chondroblasts) of cartilaginous model enlarge and matrix surrounding them is calcified under the influence of alkaline phosphatase secreted by cartilage cells.
Step 2: The cartilage cells die and disappear leaving behind empty spaces called primary areolae.
Step 3: The cells on the surface of periosteum differentiates into osteoblasts which enter at the site of ossification along with blood vessels (periosteal bud).
Step 4: The most of calcified matrix is absorbed forming large empty spaces called secondary areolae, leaving behind only thin bars of calcified matrix.
Step 5: The new bone (osteoid) is laid down on the surface of calcified bars of matrix.
Step 6: The mineralization of osteoid.
Ossification of a long bone
The following is a simplified account of intracartilaginous ossification of a long bone (Fig. 6.14).

Step 1: First the bone is laid down as a hyaline cartilaginous model surrounded by perichondrium.
Step 2: A primary centre of ossification then appears in the center of the shaft and this spreads toward the ends to form the diaphysis.
Step 3: At the same time, periosteum lays down a collar of bone (periosteal collar) around the circumference of the shaft.
Step 4: Later, one or more secondary centres of ossification develop at each end of the cartilaginous model and form the epiphysis.
Step 5: The epiphyseal cartilage separating epiphysis from diaphysis and articular cartilage at each end of bone remain cartilaginous.
Step 6: The epiphyseal plate of cartilage continues to produce new cartilage and thus enables the bone to grow in length. For this reason, epiphyseal plate of cartilage is also called growth plate. Once the growth in length is completed, the remaining epiphyseal cartilage ceases to proliferate and becomes ossified leaving only an epiphyseal scar called epiphyseal line.
Ossification centres
These are sites, where bone formation begins. The ossification centres are generally classified into two types: primary and secondary.
1. Primary centres of ossification, appear before birth (usually between the 7th to 12th week) with some exceptions (viz. primary centers of tarsal and carpal bones appear after birth except those of talus, calcaneum and cuboid).
2. Secondary centres of ossification, appear as a rule after birth (usually from the time of birth to 5 years of age).
A primary centre forms centres diaphysis, and the secondary centre form epiphyses. The fusion of epiphysis with the diaphysis starts at puberty and is usually complete by the age of 25 years, therefore after the age of 25 years, no more bone growth can take place.
In general, the appearance of secondary centres and fusion of epiphyses occur about 1 year earlier in females than in males.
Clinical correlation
• The visibility of centre of ossification in the distal end of femur in radiograph of newborn child found dead is of medicolegal importance because it indicates that the child was full term (Fig. 6.15). In x-ray of newborns, the shaft of long bone presents a white (radiopaque) shadow, whereas ends and joints cast black (radiolucent) shadow. This is because, at birth the shaft of cartilaginous model is ossified, i.e. bony, but ends are still unossified, i.e. cartilaginous.
• On the other hand in x-rays of growing children, the shaft and epiphyses cast white (radiopaque) shadow but the epiphyseal plate between the epiphysis and diaphysis cast a black (radiolucent) shadow.
• Achondroplasia (dwarfism): It is a congenital condition with the following clinical features:
1. Individual is abnormally short (dwarf).
This condition occurs due to defective endochondral ossification.

Growing end of the long bone
In most of the long bones the two epiphyses do not fuse simultaneously. The epiphysis at one end always fuses few years before than that at the other end.
The end at which fusion occurs later is called the growing end and this is also the end at which secondary center of ossification appears first.
The growing end is always located opposite to the direction of nutrient foramen.
The direction of nutrient foramen is easily remembered by a ‘dictum’ that says, ‘To the elbow I go and from knee I flee’.
In the milking cow position, the direction of nutrient foramina is always downward (Fig. 6.16).

Thus in upper limb, shoulder end of humerus and wrist ends of ulna and radius are growing ends, whereas in the lower limb, the knee ends of femur, tibia and fibula are growing ends.
Law of union of epiphyses (law of ossification)
According to this law, the epiphyseal centre (secondary centre of ossification) which appears first unites last and the epiphyseal centre which appears later unites first except in case of fibula where the epiphyseal centre for lower end appears first and also unites first. On the other hand, the epiphyseal centre for upper end appears late and also unites late (Fig. 6.17). Thus, fibula is the only long bone which violates the law of union of epiphyses.

Growth of a long bone
The growth of long bone after birth occurs by two methods:
Appositional growth:
The appositional growth refers to the addition, i.e. growth, at the periphery of the bones resulting in an increase in the diameter of the long bones.
In appositional growth, the osteoblasts on the surface of bones proliferate. The superficial osteoblasts produced from these divisions remain as such or divide again. The deep osteoblasts resulting from these divisions produce bone matrix, and when they are surrounded by matrix, they become osteocytes. Consequently, a new layer of bone is deposited on the surface of the bone.
In cancellous bone, appositional growth adds bone matrix to the outer surface of trabeculae.
Endochondral growth:
The endochondral growth is responsible for the increase in the length of long bones.
The endochondral growth occurs due to multiplication of the cells of the epiphyseal plate of cartilage.
The surface of epiphyseal plate facing toward epiphysis gives rise to new cartilage which pushes the epiphysis away from diaphysis.
The amount of new cartilage produced is equal to the amount of cartilage replaced by spongy bone toward the metaphyseal surface of the epiphyseal plate leading to increase in the length of diaphysis. The thickness of epiphyseal plate remains almost the same. The details are as under:
The epiphyseal plate is organized into four zones (Fig. 6.18); from superficial to deep these are:

The zone of resting cartilage is nearest to the epiphysis and contains randomly arranged chondrocytes which do not divide rapidly.
In the zone of proliferation, the chondrocytes proliferate and form longitudinal columns of young cartilage cells resembling stacks of plates or coins.
In the zone of hypertrophy, the chondrocytes mature and hypertrophy. They secrete alkaline phosphatase.
Thus, maturation gradient exists in each column of chondrocytes. The cells near the zone of resting cartilage are younger and actively proliferating, whereas cells progressively near the diaphysis are older and are undergoing hypertrophy.
The zone of calcification is very thin. It consists of matrix mineralized with calcium carbonate. When the hypertrophied chondrocytes die, the blood vessels from diaphysis grow into this area. The connective tissue surrounding the blood vessels contains osteoblasts from the endosteum. The osteoblasts line up on the surface of the calcified cartilage and deposit bone.
Remodeling of bone
The bone does not grow by multiplication of its cells or by increase in its intercellular material (i.e. interstitial growth), hence its shape cannot be maintained.
The bone grows by deposition of new bone by osteoblasts on its ends and on its surface in a random fashion. Therefore to maintain its shape, the unwanted bone is removed by osteoclasts. This process of bone removal is called remodeling.
Surface remodeling
As the bone grows in length, there occurs subperiosteal bone deposition in the shaft while subperiosteal bone resorption occurs in conical region toward the end. Thus diverging regions are straightened to become the part of the shaft (Fig. 6.19).

Internal remodeling
As the bone grows in diameter by deposition of new layers of bone deep to periosteum, the periosteal bone becomes thicker and thicker which is neither necessary nor desirable. Hence as the bone is laid down outside the shaft, it is removed from inside by osteoclasts. Consequently the shaft grows in diameter, and at the same time its wall does not become too thick.
The osteoclasts also remove trabeculae in the center of bone that were formed by endochondral ossification. This leads to the formation of marrow cavity.
Factors affecting growth of bones
(a) Vitamin A co-ordinates the activity of osteoblasts and osteoclasts. The deficiency of vitamin A slows down the activity of osteoclasts, consequently the size of spinal and cranial foramina is reduced, with eventual compression of nerve roots. On the other hand, the high concentration of Vitamin A causes rarefaction and resorption of bone.
(b) Vitamin C is essential for the synthesis of organic intercellular matrix (i.e. collagenous fibers and ground substance) by osteoblasts. The deficiency of vitamin A leads to defective development of growing ends of the bone. It also leads to rupture of capillaries producing painful subperiosteal hematoma.
(c) Vitamin D is essential for the absorption of calcium and phosphate from intestine. Deficiency of vitamin D leads to defective mineralization (calcification) of osteoid tissue. As a result children suffer from rickets (characterized by bowing of legs, knobby metaphyseal regions); and adults suffer from osteomalacia (i.e. softening of the bones).
2. Hormonal factors: The hormones play very important role in bone growth. The hormones which are essential for proper development and growth of bone include pituitary hormones, thyroid hormones, parathyroid hormones and sex hormones. Their defective secretion can cause number of skeletal defects.
3. Genetic factors: A clinical condition ‘chondrodystrophia foetalis’ occurs due to defective autosomal dominant inheritance. In this condition, endochondral ossification fails to occur properly.
4. Mechanical factors: Tensile force helps in bone formation whereas compressive forces favor bone resorption. In practice, orthopedic surgeons provide traction for quick healing of fractures.
Cartilage
The cartilage is a specialized connective tissue which provides rigidity along with elasticity. Hence it is found in those areas of the body, where both rigidity and elasticity are required. It consists of chondrocytes embedded in a gel-like matrix.
Phylogenetically, the cartilage tissue is older than bone tissue. Most of the bones in the intrauterine life are preformed in cartilage. The cartilages which are replaced by bones are called temporary cartilages and those that persist throughout life are called permanent cartilages.
Function of cartilage
The following are the functions of the cartilage:
1. Provides rigidity and support to soft tissues.
Structure
The cartilage has all common features of connective tissue, which include the following:
Cells:
Cells of the cartilage are of the following three types:
1. Chondrogenic cells: found in the perichondrium, where they undergo mitosis and differentiate into chondroblasts.
2. Chondroblasts: young cartilage cells occupying small spaces (lacunae) and may undergo mitosis.
3. Chondrocytes: mature cartilage cells which reside in lacunae. They form isogenous cell clusters surrounded by territorial matrix.
Fibers:
Cartilage has the following two types of fibers:
Ground substance:
It consists of:
1. Proteoglycans, specifically chondroitin sulphate and keratan sulphate.
2. Glycoproteins, viz. chondronectin and chondrocalcin (a calcium-binding protein).
3. Water (tissue fluid) contributes to 75% hydration of the ground substance (high degree of hydration).
Growth of cartilage
The cartilage grows by both appositional and interstitial methods.
1. Appositional growth: In this, layers of new cartilage are deposited at the surface beneath the perichondrium. The new cartilage is formed by chondroblasts derived from perichondrium. By appositional growth the cartilage increases in width.
2. Interstitial growth: It occurs due to increase in size and the number of existing cells and by an increase in the amount of intercellular matrix, due to proliferation of chondrocytes by mitosis in the center of cartilaginous model. By interstitial growth the cartilage increases in length.
Characteristic features of cartilage
The distinguishing features of cartilage are as follows:
1. It is avascular and receives its nutrition by diffusion through the ground substance from nearest capillaries. Here thin cartilage canals provide nutrition to the deepest core of cartilaginous mass.
3. It has no nerves, hence it is insensitive.
4. It is surrounded by perichondrium.
5. It grows by appositional as well as by interstitial methods of growth.
6. When cartilage calcifies, chondrocytes die because they are deprived of nutrition by diffusion.
Types of cartilage
The cartilages are classified into three types (Fig. 6.20):

Hyaline cartilage (Gk. hyalos = transparent stone):
It appears bluish-white and transparent because it contains very fine collagen fibers having same refractive index as that of ground substance.
It is the most widely distributed cartilage in the body (see Table 6.5). All the long bones in the body are preformed in hyaline cartilage.
Elastic cartilage:
It is made up of numerous chondrocytes embedded in matrix containing rich network of yellow elastic fibers. The sites of distribution of elastic cartilage include pinna of the ear, epiglottis.
Fibrocartilage:
It appears white and opaque due to abundance of collagen fibers in it. The collagen fibers are arranged in bundles. The chondrocytes are few, small and scattered singly or arranged in rows. It is formed at sites subjected to great pressure like intervertebral disc.
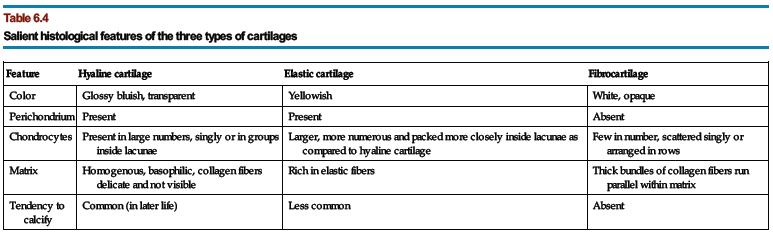
The key histological features of three types of cartilages (Fig. 6.16) are presented in Table 6.4.
Table 6.4
Salient histological features of the three types of cartilages
| Feature | Hyaline cartilage | Elastic cartilage | Fibrocartilage |
| Color | Glossy bluish, transparent | Yellowish | White, opaque |
| Perichondrium | Present | Present | Absent |
| Chondrocytes | Present in large numbers, singly or in groups inside lacunae | Larger, more numerous and packed more closely inside lacunae as compared to hyaline cartilage | Few in number, scattered singly or arranged in rows |
| Matrix | Homogenous, basophilic, collagen fibers delicate and not visible | Rich in elastic fibers | Thick bundles of collagen fibers run parallel within matrix |
| Tendency to calcify | Common (in later life) | Less common | Absent |
The distribution of the three types of cartilages in the body is enumerated in Table 6.5.
Table 6.5
Sites of hyaline, elastic and fibrocartilages
| Hyaline cartilage | Elastic cartilage | Fibrocartilage |
| Articular cartilages of most of the joints | Pinna of external ear | Intervertebral discs |
| Thyroid cartilage | Epiglottis | Interpubic disc |
| Cricoid cartilage | Corniculate cartilage | Menisci of knee joint |
| Lower part of arytenoids cartilage | Cuneiform cartilage | Articular discs of temporo-mandibular, sterno-clavicular and inferior radio-ulnar joints |
| Tracheal rings | Apex of arytenoid cartilage | Articular cartilages of temporo-mandibular, sterno-clavicular and acromio-clavicular joints |
| Costal cartilages | Auditory tubes | Glenoid labrum, acetabular labrum, etc. |
| Bronchial cartilage | External auditory meatus | |
| Nasal cartilages |
| 206 | |
| Femur | |
| Stapes | |
| Femur | |
| Malleus | |
| Fibula | |
| Hip bone | |
| Patella | |
| Metaphysis | |
| Metaphysis | |
| Clavicle in children and adults, radius in people over 50 years of age | |
| Nutrient artery of tibia | |
| Metaphysis | |
| Clavicle which lies horizontally | |
| Sesamoid bones and ear ossicles | |
| Inferior nasal concha | |
| Hyoid bone | |
| Manubrium sternum in adults and iliac crest in children | |
| Clavicle | |
| Achondroplasia (dwarfism) | |
| Cleidocranial dysostosis | |
| Lambdoid suture of skull | |
| Fibula | |
| Hyaline cartilage | |
| Fibrocartilage | |
| Cartilage of ear auricle | |
| Thyroid cartilage of larynx |