Cardiovascular System
Introduction
Enumerate the functions of cardiovascular system
1. Distribution of metabolites and oxygen to all the body cells.
2. Collection of waste products and CO2 from different body cells and carry them to excretory organs.
3. Thermoregulation—Carrying of heat from active metabolic sites (where heat is generated) to body surface where it is dissipated. Blood flow through skin varies to enhance or decrease the heat loss to the environment.
Heart which is a muscle pump provides the driving force causing flow of blood for the system whereas arteries are the distributing channels. Veins act as reservoirs and also collect and return the blood back to the heart.
Between arteries and veins, there are capillaries which actually supply blood to tissue cells. They act as exchange vessels because they are thin walled.
Name various chambers of the heart
Heart is divided into left and right heart. Each half is further divided into two parts-atrium and ventricle. Thus, there are four chambers of the heart: left and right auricles (atria) and left and right ventricles. Right side of the heart collects the deoxygenated blood from tissues and pumps it to the lungs for oxygenation, whereas left heart collects the oxygenated blood from lungs and pumps the oxygenated blood to different tissues. Thus, heart actually has two pumps-right and left.
How are the different chambers of the heart separated?
Left chambers of the heart are separated from the right chambers by a continuous partition. The atrial portion of this partition is known as interatrial septum while ventricular part is known as interventricular septum.
The right atrioventricular opening is guarded by a tricuspid valve so named because it has three cusps, viz. anterior, posterior and medial. Left atrioventricular opening is guarded by a bicuspid valve (mitral) which has two cusps, viz. anterior and posterior.
What are semilunar valves?
From left ventricle arises the aorta which carries blood to the tissues and from right ventricle arises the pulmonary artery (trunk) which carries deoxygenated blood to the lungs. The openings between aorta, pulmonary artery and respective ventricles are guarded by semilunar valves, having three cusps.
What is the function of valves in the heart?
Valves allow unidirectional flow of blood. Atrioventricular valves open towards the ventricles and close towards the atria. They allow blood to flow from atria to ventricles but when ventricles contract, they are closed and thus prevent back flow of blood from ventricles to atria.
Semilunar valves open away from ventricles and close towards the ventricles. These valves open when ventricles contract allowing the blood to flow from ventricles to aorta and pulmonary trunk. They close when ventricles relax thus preventing back flow of blood from aorta or pulmonary trunk into the ventricles.
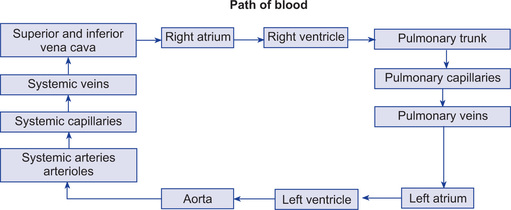
Describe the course of systemic circulation
Systemic or greater circulation is responsible for pumping oxygenated blood to different tissues and collecting deoxygenated blood from tissues back to the heart. In this circulation, blood is pumped by the left ventricle to all the tissues (except the lungs) and is returned back to the right atrium. Vessels carrying blood away from heart are termed arteries and those carrying blood from tissues to heart are called veins.
In systemic circuit, blood leaves left ventricle via a single large artery, the aorta. The systemic arteries branch from aorta dividing into progressively smaller branches. The smallest arteries form arterioles which branch into very small, thin walled capillaries only lined by single layer of endothelial cells. Through these, exchange of materials between blood, tissues and cells occurs. Capillaries unite to form thicker vessels called venules (arterioles, capillaries, and venules are collectively known as microcirculation).
Venules in systemic circulation unite to form larger vessels called veins. The veins from various peripheral organs unite to form two large veins: inferior vena cava which collects blood from lower portions of the body and superior vena cava collecting blood from the upper half of the body. Through these two veins, blood returns to the right atrium.
Describe the course of pulmonary circulation
Pulmonary circulation is responsible for pumping the deoxygenated blood to the lungs and collecting oxygenated blood from lungs back to the heart as follows:
Blood leaves the right ventricle via a single large artery, the pulmonary trunk which divides into two pulmonary arteries, one supplying each lung. In the lungs, the arteries continue to branch ultimately forming capillaries that unite into the venules and veins. The blood leaves the lungs via pulmonary veins which empty into the left atrium.
Cardiac muscle
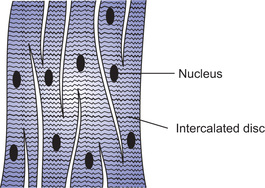
Describe in short the structure of cardiac muscle
Cardiac muscle (myocardium) consists of the separate cardiac muscle cells (striated) that are electrically connected to one another by tight junctions. These connections are low resistance pathways and are called intercalated disc. Though there is no anatomical connection between different cardiac muscle fibres from functional point of view, action potential passes from one cardiac muscle cell to the other through gap junctions and cardiac muscle acts as a syncytium of many cardiac muscle cells, i.e. excitation of one cardiac cell causes the action potential to spread to all the other cells. Heart is composed of two separate syncytium—the atrial syncytium (walls of two atria) and ventricular syncytium (walls of two ventricles). Action potential is conducted from atrial syncytium to ventricular syncytium by way of specialized conducting system. Normally there is one functional electrical connection between atria and the ventricles. This is AV node and its extension ‘bundle of His’. Because atria and ventricles are two separate syncytium, atria contract a short time ahead of ventricular contraction (Fig. 13.1).
Initiation and conduction of cardiac impulse
What is autorhythmicity?
Cardiac fibres especially, specialized conducting system have the property of self-excitation because of which they can cause initiation of rhythmic impulses which in turn can cause automatic rhythmic contractions. This property is called autorhythmicity. Sinus node normally initiates the rhythmic impulse and controls the rate of beating of the heart. Thus it is called pacemaker of the heart.
Describe the specialized excitatory conductive system of the heart
There is a specialized excitatory system which generates rhythmic impulses to cause rhythmic contraction of the heart and special conductive system which conducts these impulses throughout the heart.
Excitatory and conductive system (Fig. 13.2)
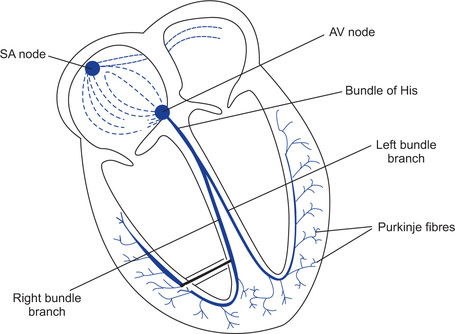
1. SA node (sinoatrial node). It is located near the junction of superior vena cava and the right atrium. It acts as a pacemaker because the rate of impulse generation is highest.
2. Interatrial tract (Bachmans bundle). It is a band of specialized muscle fibres that run from sinoatrial node to left atrium. It causes simultaneous depolarization of both the atria, since the velocity of conduction of impulse in this tract is faster than rest of the atrial muscles.
3. Internodal tracts. Three pairs of specialized cells connect sinoatrial node to atrioventricular node. They are anterior, middle and posterior. Through them impulses from sinoatrial node reach atrioventricular node to initiate ventricular contraction. These are specialized conducting fibres mixed in the atrial muscle.
4. AV node (atrioventricular node). It is located just beneath the endocardium on the right side of the interatrial septum, near the tricuspid valve. Normally it is the only path through which ventricles are activated.
5. Bundle of His. It is the continuation of AV node and is located beneath the endocardium on the right side of the interventricular septum. It divides into two branches known as right and left bundle branches. These proceed on each side of the interven-tricular septum to their respective ventricles.
6. Purkinje fibres. These fibres arise from both the bundle branches and branch out extensively just beneath the endocardium of both the ventricles.
Why does sinus node act as a pacemaker of the heart?
Other parts of the conductive system are also capable of generating their rhythm but still SA node acts as a pacemaker because rate of impulse generation by SA node is highest.
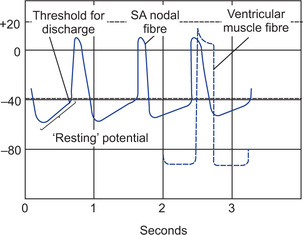
Explain the mechanism responsible for sinus nodal rhythmicity
Sinoatrial nodal fibres have a resting membrane potential which is not steady. It manifests a slow depolarization. This is because of leakage of the resting membrane for sodium. This causes slow diffusion of sodium ions into the SA nodal fibres under-resting condition. The potential therefore, slowly rises from −55 mV due to entry of sodium ions. When potential rises to a threshold level, i.e. −40 mV, the slow voltage-gated sodium-calcium channels open and action potential is initiated. Entry of sodium and calcium through the opened channels causes a rapid depolarization (i.e. action potential). Then at the end of depolarization, potassium channels open and Na+-Ca++ channels close. This causes potassium ions to diffuse out of the fibres resulting into rapid repolarization to −55 to −60 mV. Again because of leakage of membrane to sodium ions, there is slow diffusion of sodium ions causing slow depolarization. When potential reaches a threshold (−40 mV), another action potential is initiated because of opening of slow voltage-gated sodium-calcium channels. Thus, there is initiation of impulses (action potentials) at regular intervals of time (autorhythmicity) (Fig. 13.3).
Describe the impulse conduction from SA node to Purkinje system
Action potential is initiated in the SA nodal fibres. Ends of SA nodal fibres are fused with surrounding atrial muscle fibres. Therefore, action potential originated in SA node travels outward in these fibres. This way impulse spreads over the atria. Conduction is more rapid in several small bundles of atrial fibres called interatrial tract or band. Conduction through these fibres causes simultaneous depolarization of both the atria. The rate of conduction in these fibres is 1 m/s.
There are three pairs of internodal tracts (anterior, middle, posterior) through which impulse passes from SA node to AV node fibres.
Impulse reaches AV node within 0.03 sec after its origin in SA node. At AV node, there is a delay of 0.09 second and further delay in ‘bundle of His, for 0.04 second (total delay is 0.13 second) (Fig. 13.4).

Fig. 13.4 Transmission of the cardiac impulse through the heart showing the time of appearance (in fraction of a second) of the impulse in different parts of the heart.
Causes of AV nodal delay
• Fibres connecting internodal tract and AV node are called transitional fibres. These are very small fibres conducting the impulse at a very slow rate, i.e. 0.02 to 0.05 m/s.
• Velocity of impulse conduction in AV nodal fibres is also slow, i.e. 0.05 m/s.
• Resting membrane potentials of transitional fibres and AV nodal fibres are much less negative than rest of the cardiac muscle fibres.
• There are very few gap junctions connecting successive fibres in the pathway.
Bundle of His conducts impulse from AV node to its left and right branches. Except in certain abnormal states, fibres of AV bundle conduct the impulse from atria to ventricle and not in the reverse direction. This allows forward conduction of impulse. Atrial muscle is separated from ventricular muscle by a continuous fibrous barrier which acts as a barrier to passage of impulse through any other route from atria to ventricles except through AV bundle.
AV bundle passes downward in ventricular septum for 5 to 15 mm and then divides into left and right bundle branches. Through these branches, impulse passes to two ventricles. Branches divide into Purkinje fibres which become continuous with cardiac muscle fibres.
The time taken for impulse to travel from bundle branches to Purkinje fibres is 0.03 second. Through Purkinje fibres, impulse is spread rapidly to ventricular muscle fibres. The velocity of transmission of impulse in ventricular muscle fibres is 0.3 to 0.5 m/s. It first spreads over the endocardial surface and then the cardiac muscle fibres which are arranged in double spirals. Therefore, impulse does not necessarily travel outwards (towards the surface) but it angulates towards the surface along the directions of spirals. Therefore, transmission from endocardial surface to epicardial surface takes about 0.03 second. Thus total time for transmission in normal heart from initial bundle branches to ventricles is 0.06 second.
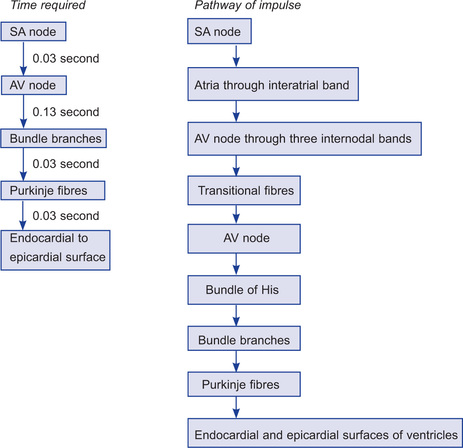
Total time required for conduction from SA node to endocardial surface is 0.22 second.
What is the importance of AV nodal delay?
Atria and ventricles are excited at different times and also contract at different times because of AV nodal delay.
What is the resting membrane potential of normal cardiac muscle?
Resting membrane potential of normal cardiac muscle is −85 to −95 mV.
Describe the action potential of the cardiac muscle
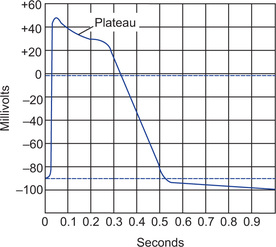
Record of action potential in the ventricular muscle shows that there is an initial spike, i.e. rising of resting membrane potential from −85 to −90 mV to a slightly positive value (up to +20 mV). The positive portion is called overshoot potential. After initial spike, membrane remains depolarized for 0.2 second in atrial and 0.3 second in ventricular muscle fibres. This sustained depolarization is seen as plateau. After plateau there is abrupt repolarization (Fig. 13.5).
What is the cause of plateau recorded in cardiac muscle action potential?
1. Initial spike of action potential of cardiac muscle is due to opening of fast voltage-gated sodium channels causing diffusion of sodium ions into the fibres. Plateau is due to opening of slow voltage-gated calcium sodium channels through which calcium and sodium ions continue to diffuse into the fibre. This causes prolonged phase of depolarization, i.e. plateau.
2. At the onset of action potential, permeability of membrane for potassium decreases about fivefold. This greatly decreases potassium outflux during action potential plateau and thereby prevents repolarization. When slow calcium-sodium channels close at the end of 0.2 to 0.3 second, then membrane permeability for potassium rapidly increases causing rapid outflux of potassium. This results into returning of membrane potential to resting level (repolarization).
What is the velocity of conduction of impulse in the cardiac muscle?
Velocity of conduction of impulse (action potential) in both atrial and ventricular muscle fibres is about 0.3 to 0.5 m/s.
How much is the refractory period of cardiac muscle?
Absolute refractory period of atrial muscle is 0.15 s and relative refractory period is 0.03 second. Ventricles have absolute refractory period much longer 0.25 to 0.30 second and relative refractory period for additional 0.05 second.
Explain phenomenon of excitation-contraction coupling in the cardiac muscle
Sarcoplasmic reticulum in the cardiac muscle is less well developed than in skeletal muscle. It is present as a network of tubules surrounding the myofibrils. It has dilated terminals (cisternae) which are located next to the external cell membrane and T tubules. Sarcoplasmic reticulum and cisternae contain high concentration of ionic calcium.
T tubules are continuations of cell membrane and they conduct action potential to the interior of the cell. They invaginate to the interior of the cell at the ‘Z’ line of sarcomere. Therefore, there is only one T tubule present per sarcomere.
When action potential passes over the cardiac muscle membrane, it passes to the interior of the muscle cells through T tubules.
Action potential acts on the membranes of longitudinal sarcoplasmic tubules to cause instantaneous release of calcium. Calcium ions diffuse into the myofibrils and catalyze chemical reactions that promote sliding of actin and myosin filaments which in turn produce muscle contraction. In addition, in cardiac muscle (as against that in skeletal muscle) extra calcium ions diffuse into the sarcoplasm from ‘T’ tubules without which contraction strength would be considerably reduced.
‘T’ tubules of cardiac muscle contain mucopolysaccharides which are negatively charged and bind an abundant store of calcium ions. ‘T’ tubules open directly to the exterior and therefore calcium ions in them directly come from extracellular fluid. These calcium ions diffuse into the sarcoplasm when action potential propagates along the ‘T’ tubules. Because of this, strength of cardiac muscle contraction depends to a great extent on calcium concentration in extracellular fluid. Whereas skeletal muscle contraction is hardly affected by calcium concentration in ECF.
Applied Aspect
What are the causes of shift of pacemaker?
Causes of shift of pacemaker from SA node to other sites are:
What is Stokes-Adams syndrome?
When there is AV block, atria continue to beat at the normal rhythm (i.e. of SA node) while new pacemaker develops in Purkinje system of ventricles with a rate of 15 to 40/min. But after a sudden block, Purkinje system does not begin its rhythm immediately. It takes about 15 to 30 seconds. During this time, ventricles fail to contract. Thus the person faints because of lack of blood flow to the brain. This delayed pick-up of heart beat is called Stokes-Adams syndrome. If period is too long, death may occur.
Nervous control of heart rhythm
Explain the role of autonomic nervous system in controlling heart rhythm
Heart is supplied by parasympathetic and sympathetic nerves. Parasympathetic supply passes through vagus nerve. Sympathetic supply comes from 1 to 5 thoracic segments of spinal cord. Preganglionic fibres relay in superior, middle and inferior cervical ganglia. Postganglionic nerves supply the heart. Vagi nerves mainly innervate sinus and AV nodes, to a lesser extent the muscle of two atria and even to a lesser extent the ventricular muscle. Sympathetic nerves are distributed to all parts of the heart, especially to ventricular muscles as well as to other areas.
Effect of parasympathetic stimulation
Parasympathetic stimulation causes release of acetylcholine at vagal nerve endings. It causes: (a) decrease in the heart rate by decreasing the rate of sinus rhythm, (b) decreased excitation of AV node, AV junctional fibres, atrial musculature, thus reducing the rate of transmission of impulse into ventricles. Strong stimulation may completely block the transmission and ventricles may stop beating for 4 to 10 seconds. If it happens, Purkinje system initiates the rhythm causing ventricular contraction at a rate of 15 to 40/min. This phenomenon is called vagal escape.
Mechanism of action. Acetylcholine released at the nerve endings increases the permeability of the fibre membrane for potassium ions. This causes rapid diffusion of potassium to the exterior of the fibre causing hyperpolarization, decreasing excitability of the tissue.
Effect of sympathetic stimulation
Sympathetic stimulation increases the rate of sinus rhythm, rate of conduction of impulse as well as increased excitability in all the portions of the heart. Force of contraction of atria and ventricles increases greatly.
Mechanism of action. Stimulation of sympathetic nerves causes release of norepine-phrine at the nerve endings. Probably this increases permeability of cardiac muscle fibre to sodium and calcium. In AV node increased sodium permeability makes it easier for action potential to excite the surrounding portion, decreasing rate of conduction time from atria to ventricles. Increased permeability for calcium increases the contractile strength of the heart.
What is vagal tone?
Right vagus nerve innervates the SA node and liberates acetylcholine from its endings. Normally, vagal activity hyperpolarizes SA node fibres by increasing permeability of SA nodal fibres for potassium. This hyperpolarization slows the firing rate of SA node from its automatic rate of 90 to 120 beats/min to the actual heart rate of about 72 beats/min. This normal vagal activity is called vagal tone.
Cardiac cycle
What is cardiac cycle?
The period of beginning of one heart beat to the beginning of the next is called cardiac cycle.
What is bradycardia?
Heart rate below 60 beats/min is termed bradycardia. It is commonly seen in well-trained athletes.
Name various cardiac cycle events
Cardiac cycle includes both electrical (ECG) and mechanical events. Electrical events precede and initiate the corresponding mechanical events.
Name different mechanical events occurring during cardiac cycle
Main events in cardiac cycle are: (a) atrial contraction (systole) and atrial relaxation (diastole), (b) ventricular contraction (systole), and (c) ventricular relaxation (diastole).
The total period of one cycle is 0.8 second.
Atrial systole is 0.1 second and atrial diastole is 0.7 second.
Ventricular systole is 0.3 second and ventricular diastole is 0.5 second.
Describe various events in the cardiac cycle
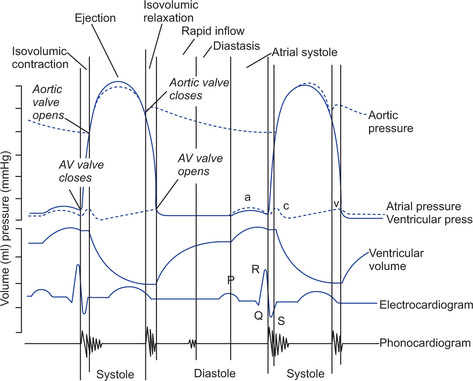
1. Atrial systole (contraction). During the period of ventricular relaxation, blood flows from atria to ventricles. About 75% of the blood flows to ventricles before atria contract. Both atria contract almost simultaneously and pump the remaining 25% of blood into the respective ventricles (therefore even if atria fail to function it is unlikely to be noticed unless a person exercises). The contraction of atria increases, the pressure inside the atria to 4 to 6 mmHg in the right atrium and about 7 to 8 mmHg in the left atrium. The pressure rise in right atrium is reflected into the veins and this wave is recorded as ‘a’ wave (recorded from jugular vein with the help of a transducer).
Then there is a period of atrial diastole for rest of the cardiac cycle (0.7 second) during which various ventricular events occur in sequence as follows:
2. Ventricular systole (contraction). At the termination of atrial contraction, the pressure of blood in the ventricles rises (normally less than 12 mmHg). Rising ventricular pressure now exceeds the atrial pressure.
This causes closure of AV valves which is a major component responsible for generating first heart sound. Then there are following phases of ventricular systole:
• Isovolumic or isometric contraction. At the beginning of this phase AV valves are closed but semilunar valves are not yet opened. Thus ventricular chambers are sealed from both atria and the arteries. The ventricle starts contracting but volume of blood inside both the ventricles remains the same hence this phase is called isovolumic phase of contraction. This phase lasts for about 0.05 second. During this phase ventricles contract as a closed chamber and pressure inside the ventricles rises rapidly to a high value. When pressure in the left ventricle is slightly above 80 mmHg and right ventricular pressure slightly above 8 mmHg, then the ventricular pressures push the semilunar valves open. This causes ejection of blood from ventricles to the respective arteries in next phases.
• Rapid ejection phase. As soon as the semilunar valves open, blood is rapidly ejected. About two-third of the stroke volume is ejected in this rapid ejection phase. The duration of this phase is about 0.11 second. Pressure inside the left ventricle rises to 120 mmHg during this phase. The end of rapid ejection phase occurs at about the peak of ventricular and atrial systolic pressure. The right ventricular ejection begins before that of left and continues even after left ventricular ejection is complete. As both the ventricles almost eject same volume of blood, the velocity of right ventricular ejection is less than that of the left ventricle.
• Reduced ejection phase. During later two-third of systole rate of ejection declines. During this phase of reduced ejection, rest one-third stroke volume is ejected. This phase lasts for about 0.14 second. During the period of slow ejection ventricular pressure falls to a value slightly lower than that in aorta but still blood continues to empty into aorta because blood flowing out has built up momentum. As this momentum decreases, kinetic energy of momentum is converted to pressure in the aorta. This causes aortic pressure to rise slightly above that of the ventricle.
3. Ventricular diastole or relaxation. It occurs in following phases:
• Protodiastole—At the end of ventricular systole, ventricles start relaxing allowing rapid fall in the intraventricular pressures. This is the period of protodiastole which lasts for 0.04 seconds. At the end of this phase, elevated pressures in distended arteries (aorta and pulmonary artery) immediately pushes the blood back towards the ventricles which snaps the aortic and pulmonary semilunar valves closed. This is the major component in generating second sound (closure of semilunar valves). It also causes dicrotic notch in the down slope of aortic pressure called incisura. Incisura indicates end of systole and the onset of diastole.
• Isovolumic or isometric relaxation—The ventricles continue to relax as closed chambers as semilunar valves are closed and AV valves are not yet open. This causes rapid fall of pressure inside the ventricles (from 80 mmHg to about 2 to 3 mmHg in the left ventricle). This phase lasts for 0.06 seconds. Because the ventricular volume remains constant, this phase is called isovolumic phase. When ventricular pressures fall below the atrial pressures the AV valves open.
• Rapid filling phase—During ventricular systole because AV valves are closed, large amount of blood accumulates in atria because veins continue to empty the blood into them and this causes increase in pressure inside atria. High atrial pressure causes the blood to flow rapidly into the ventricles. Then pressures in both the chambers fall as ventricular relaxation continues.
• Reduced filling phase or diastasis—After the rapid filling phase, pressures in atria and ventricles rise slowly as blood continues to return to the heart. This decreases the rate of blood flow from atria to ventricles causing slow filling of ventricles called diastasis.
During rapid filling and diastasis phase about 75% of blood passes from atria to ventricles. Then the next cycle begins with atrial contraction.
What is stroke volume?
Volume of blood that is ejected by each ventricle with each beat is stroke volume. It is 70 ml.
What is ventricular end diastolic volume?
Ventricular end diastolic volume is the volume of blood in the ventricle just prior to the onset of ventricular contraction. Normally left ventricular end diastolic volume is 110 to 120 ml. It is markedly reduced if the heart rate increases. When heart rate increases periods of systole and diastole become shorter. Decreased period of diastole decreases the filling of ventricle and therefore the end-diastolic volume.
What is ventricular end systolic volume?
Volume of blood remaining in the ventricle at the end of ejection is called end systolic volume. It is normally 40 to 50 ml.
What is ejection fraction?
The fraction of end-diastolic volume that is ejected is called the ejection fraction. Normally it is about 60%.
Describe the pressure changes in atria during cardiac cycle
Atrial pressure curves show three major pressure elevations which are called ‘a’, ‘c’ and ‘v’ waves.
1. The ‘a’ wave is caused by atrial contraction. Ordinarily, right atrial pressure rises about 4 to 6 mmHg and left atrial pressure rises about 7 to 8 mmHg during this atrial contraction. Wave appears during atrial systole.
2. The ‘c’ wave occurs when the ventricles begin to contract. It is partly caused by slight back flow of blood into atria at the onset of ventricular contraction but mainly caused due to bulging of AV valves towards the atria because of increasing pressure in the ventricles. This wave therefore appears in the phase of isovolumic contraction of the ventricles.
3. The ‘v’ wave occurs towards the end of ventricular contraction. It results from slow build up of pressure in atria due to collection of blood from veins while AV valves are closed during ventricular contraction. This wave occurs therefore during isometric relaxation phase of ventricle. After this phase AV valves open, allowing rapid flow of blood into the ventricles causing ‘v’ wave to disappear (Fig. 13.6).
Describe the pressure changes in the left ventricle during cardiac cycle
Before atrial systole, the pressure inside the left ventricle is almost zero. When left atrium contracts and forces blood into the left ventricle pressure rises to about 7 mmHg.
At the end of atrial systole, AV valve closes and semilunar valve is not yet open. Ventricle contracts as a closed chamber (isometric contraction) and therefore pressure inside the ventricle rapidly rises from 7 to 80 mmHg.
At the end of isometric contraction, semilunar valve opens and ventricle starts contracting isotonically. This causes pressure to rise to a peak level of 120 mmHg during rapid ejection phase. Then there is reduced ejection phase in which because of decreased volume of blood in the ventricle pressure decreases slightly to 100 mmHg. Then semilunar valve (aortic valve) is closed and ventricular diastole starts.
During isovolumic relaxation phase, ventricle relaxes as a closed chamber and therefore there is a great pressure fall in the left ventricle from 100 mmHg to about 2 to 3 mmHg. Then AV valve opens and ventricular filling begins.
During rapid filling and diastasis though the ventricle is getting filled and volume of blood is increasing because of relaxation of ventricle, pressure in the ventricle drops to almost zero (Fig. 13.6).
Describe the volume changes in the ventricles
During ventricular diastole, filling of ventricles increases the volume of blood in ventricle, to about 110 to 120 ml which is called end diastolic volume. During ventricular contraction, blood flows rapidly out in phase of rapid ejection and comparatively slowly in slow ejection phase leading to fall in volume to 40 to 50 ml (70 ml blood is pumped out). Thus end systolic blood volume is 40 to 50 ml (Fig. 13.6).
What is the function of papillary muscles?
Papillary muscles are attached to the veins of AV valves by the chordae tendineae. Papillary muscles contract when ventricular walls contract and pull veins of the valves towards the ventricle to prevent the excessive bulging of valves towards the atria during ventricular contraction.
Describe aortic pressure changes during cardiac cycle
Pressure in the aorta varies between 80 to 120 mmHg during cardiac cycle. During the period of rapid ventricular ejection, the pressure in the aorta is slightly less than that of the ventricle. The peak aortic pressure is arterial systolic pressure and occurs at the end of rapid ejection. It is 120 mmHg. Then pressure slightly falls during reduced ejection phase. At the end of reduced ejection phase aortic pressure becomes slightly more than that in the ventricles. This causes closure of semilunar valves, but also causes backward flow of blood. After the aortic valve has closed, pressure in the aorta falls slowly throughout the diastole because blood stored in distended elastic arteries continues to flow to the periphery. Before the ventricles contract again, aortic pressure falls to 80 mmHg (diastolic pressure). The incisura during the down slope of the aortic pressure indicates the end of ventricular systole (Fig. 13.6).
Describe pressure changes in the pulmonary artery during cardiac cycle
Pressure curve in the pulmonary artery is similar to that of aorta but pressures are low (about one-sixth of that in aorta). Pulmonary artery systolic pressure averages 15 to 18 mmHg and its pressure during diastole is 8 to 10 mmHg.
What is work output of heart?
Work output of the heart can be expressed as stroke work output or minute work output. Stroke work output of the heart is the amount of energy that the heart converts to work during each heart beat. Minute work output is the total amount of energy that is converted to work in a period of one minute.
How does heart muscle derive energy for work?
The energy for work of the heart is derived from oxidative metabolism mainly of fatty acids and to a lesser extent of other nutrients. Therefore, rate of O2 consumption by the heart is excellent measure of the chemical energy liberated while heart performs the work.
How much is mechanical efficiency of the heart muscle?
Ratio of work output to total chemical energy expenditures (amount of energy converted to work) is called efficiency of heart. Maximum efficiency of normal heart is 20 to 25%. In heart failure, it may reduce to 5 to 10%.
Describe regulation of heart pumping
Pumping of heart is regulated by two mechanisms: intrinsic cardiac regulation, and control by autonomic nervous system.
1. Intrinsic regulation. Heart adapts to changes in blood volume it receives. Rate of blood flowing into the heart through veins each minute is known as venous return. Greater the venous return, greater is the pumping ability to pump excess incoming blood into the arteries. This intrinsic ability to adapt to changing volume is called “Frank-Starling” mechanism of heart. This is because the force of contraction of heart is proportional to initial length of muscle fibre (Frank-Starling law). When there is increased venous return, there is stretch on the cardiac muscle wall which increases the initial length of muscle fibres which in turn increases the force of contraction. Stretch of muscle also increases the heart rate.
2. Control by autonomic nervous system.
(a) Sympathetic stimulation increases the heart rate and also the force of contraction of heart. Thus volume of blood pumped by heart increases. Also the ejection pressure increases. Sympathetic stimulation can increase cardiac output as much as two to threefold.
Inhibition of sympathetic system has opposite effects. Under normal conditions, there is a continuous slow rate of discharge through sympathetic fibres to the heart which maintains pumping 30% above that with no sympathetic stimulation. Therefore, when sympathetic activity is inhibited, both heart rate and force of ventricular contraction decrease.
(b) Parasympathetic (vagal) stimulation decreases the heart rate and force of contraction. The effect on the force is not much because vagal fibres are mainly distributed to the atria and not much to the ventricles. Decrease in strength of heart is only 20 to 30%. Very strong stimulation of vagi can actually stop the heart beat for few seconds but then heart escapes (vagal escape) action of vagus and starts beating but at a lower rate (20 to 30 beats/min).
What are the effects of ions on heart function?
Effect of potassium ions
• Excess potassium concentration in extracellular fluid causes heart to become extremely dilated.
• There is blockage of conduction of impulses from atria to ventricle through AV bundle. This is partially caused due to decreased resting membrane potential in cardiac muscles. As membrane potential decreases intensity of action potential also decreases.
What is the effect of temperature on heart?
Increase in temperature causes increased permeability of heart resulting into acceleration of self-excitation process. Contractile strength of heart is often enhanced temporarily with moderate increase in temperature. But prolonged elevation of temperature exhausts the metabolic system and causes weakness.
Heart sounds
Give an account of the heart sounds
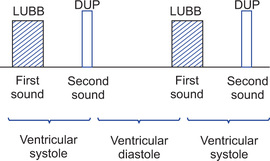
Closure of the valves of the heart is associated with audible sounds. Normally the heart sounds are heard with a stethoscope which are described as first and second heart sounds. Occasionally third heart sound which is very weak is heard. But fourth heart is not heard by stethoscope because it has very low frequency. It can only be recorded in phonocardiogram (Fig. 13.7).
Heart sounds are not directly heard over the valves themselves but they are better heard over four auscultatory areas.
• Mitral area. This area lies over the apex beat (normally in the fifth left intercostal space three and half inches lateral to the midsternal line).
• Tricuspid area. This lies at the lower end of sternum.
• Aortic area. This area lies in the right second intercostal space near the lateral border of the sternum.
• Pulmonary area. This area lies in the left second intercostal space near the lateral border of the sternum.
Both the heart sounds, first and second are heard in all four auscultatory areas, but at mitral and tricuspid areas first heart sound is better heard because sound caused by A-V valves are transmitted to the chest wall through the respective ventricles. Second heart sound is better heard over the aortic and pulmonary areas because sounds caused by closure of semilunar valves are transmitted to the aorta and pulmonary artery.
1. First heart sound. This sound is produced due to closure of A-V valves. Slapping together of valve leaflets sets up vibrations causing vibrations of the adjacent blood, walls of the heart and major vessels around the heart. Contraction of ventricles causes valves to bulge against atria until chordae tendineae abruptly stop the back bulging. The elastic tautness of the valves (tricuspid and mitral valves) then cause back surging blood to bounce forward again into each respective ventricle. This sets blood, ventricular walls and valves into vibration. It causes vibrating turbulence in the blood. Vibrations travel to surrounding tissues and to the chest wall where sound can be heard with the help of the stethoscope. It is like a word LUBB. It is better heard over mitral and tricuspid areas. The duration of the first sound is 0.14 second, and is low pitched.
Significance:
• It indicates the onset of clinical systole of the ventricles.
• The duration and intensity of the first sound indicates the condition of myocardium. If myocardium is weak, first heart sound is short and low pitched. It is prominent when there is hypertrophy of myocardium.
• Normal first sound also indicates that A-V valves are properly closing (there is no incompetence).
2. Second heart sound. The second heart sound is due to closure of semilunar valves. It is of higher frequency than the first sound because of (i) tautness of the semilunar valves in comparison with A-V valves, and (ii) greater elastic co-efficient of the arteries (which provide the principal vibrating chambers) in comparison with the much looser ventricular chambers (which are vibrating chambers for the first heart sound).
Thus second heart sound is of higher frequency (high pitched), sharp and of short duration (0.11 sec). It is like a word DUP. The intensity of the sound depends on blood pressure. Sometimes two valves aortic and pulmonary do not close simultaneously during inspiration. This causes splitting of second sound during inspiration.
Significance:
• It indicates end of systole and beginning of diastole of the ventricles.
• Clear second sound indicates that the semilunar valves are closing properly, i.e. there is no incompetence.
• Interval between first and second sound is shorter and it indicates clinical systole. The interval between second heart sound and the next first heart sound is longer and it indicates clinical diastole of the heart.
3. Third heart sound. Occasionally a very weak rumbling third heart sound is heard at the middle third of the diastole. It does not appear until middle third of diastole because in early part of the diastole the heart is not filled with blood sufficiently to create even small amount of elastic tension in the ventricles. The frequency of this sound is low and sometimes so low that it cannot be heard, yet it can be recorded in the phonocardiogram. Its duration is 0.04 second. It can be identified by its relation with the second sound and it coincides with descending limb of ‘v’ wave of jugular venous pulse.
4. Fourth heart sound. It is also called atrial sound and is caused by in-rushing of blood into the ventricle when atria contract which initiates vibrations similar to those of the third heart sound. It has a very low frequency, i.e. below 20 cycles/second. Therefore, it can never be heard with the help of stethoscope but it can only be recorded by phonocardiogram. It coincides with ‘a’ wave of jugular venous pulse.
What is phonocardiogram?
A specially designed microphone to detect low frequency. It is applied to the precor-dium. Heart sounds are amplified and recorded by a high speed recording apparatus (oscillograph). The recording is called a phonocardiogram. Machine is also connected with a mirror arrangement which reflects a beam of light on a moving photographic plate. Sounds thus can be graphically recorded.
Electrocardiogram
What is an electrocardiogram?
Record of the electrical changes during the cardiac cycle is known as electrocardiogram.
Describe the method of recording ECG
Action potentials generated in the muscle cells of heart can be recorded by placing recording electrodes on the surface of the skin.
The electrodes are connected to the machine (electrocardiograph). The tracings are usually made at a standard recording speed of 25 mm/sec and amplification (1 mV = 1 cm deflection). These tracings are made over the standard ECG paper. This paper is divided into small squares. Each small square on horizontal axis represents 0.04 sec and on vertical axis represents 0.1 mV.
Most modern electrocardiograph has a direct pen writing recorder that writes electrocardiogram with a pen directly on a moving sheet of paper. Pen is often a thin tube connected at one end to a ink well; and its recording end is connected to a electromagnet system capable of moving the pen back and forth at high speed. As the paper moves forward, the pen records the electrocardiogram. In other recorder instead of ink pen, special paper is used. The paper turns black on exposure to heat. The stylus (recording pen) is made hot by electrical current flowing through its tip. Another type of paper turns black when electric current flows from the tip of the stylus.
What is a lead?
Lead is the connection between two points on the body surface and the electrocardiograph. Hence a lead consists of:
What are bipolar leads?
Bipolar leads mean the ECG is recorded from two specific electrodes placed on the body.
Describe bipolar limb leads
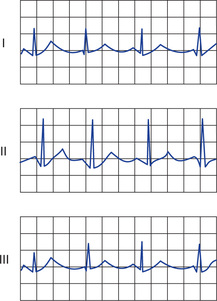
Three leads are formed by measuring the potential differences between any two of the limb electrodes. The leads are selected by a switch on standard ECG machine.
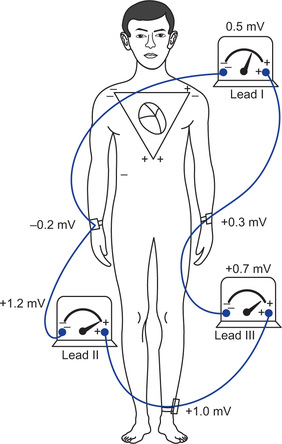
Lead I. For recording ECG in lead I, negative terminal of the electrocardiograph is connected to the right arm and positive terminal to the left arm. When right arm is negative with respect to left arm, the positive wave is recorded.
Lead II. For recording ECG in lead II, negative terminal of the electrocardiograph is connected to the right arm and positive terminal to the left leg. When right arm is negative with respect to left leg, the positive wave is recorded by electrocardiogram.
Lead III. For recording ECG in lead III, negative terminal of the electrocardiograph is connected to the left arm and the positive terminal to the left leg. If left arm is negative with respect to left leg, ECG records the positive wave.
What is Einthoven's triangle?
Einthoven's triangle is the diagrammatic way of illustrating that the two arms and left leg form apices of triangle surrounding the heart. It is the equilateral triangle with the right and left shoulders and left leg as the three apices. The right leg serves as a ground connector. All four electrodes must be attached to the extremities.
What is Einthoven's law?
Einthoven's law states that if electrical potentials of any two of the bipolar limb electro-cardiographic leads are known at any given instant, the third one can be determined mathematically by simply summing the first two (but positive and negative signs of different leads must be observed while making the summation) (Fig. 13.8).
What are unipolar leads? Describe unipolar chest leads
If the three limb leads are connected to a common terminal through electrical resistance the combined voltage from the three leads will be zero, theoretically. This common terminal can be attached to the negative pole of a galvanometer (indifferent electrode) and a fourth or exploring electrode can be attached to the positive pole. The galvanometer can still only read the potential difference between two points but because the common electrode is at zero volts, other electrode (exploring) will provide the actual or absolute voltage at the body surface. This arrangement of connections is termed a unipolar lead. They are used to record, from standardized sites on precordium. There are six such precordial leads called ‘V’ leads.
The placement of exploring electrode in leads V1 to V6 is as follows:
Lead V1 in the fourth intercostal space, just to the right of the sternum.
Lead V2 in the fourth intercostal space just to the left of the sternum.
Lead V4 in the midclavicular line in the fifth left intercostal space.
Lead V3 halfway between V2 and V4.
Lead V5 in the anterior axillary line at the same level as V4.
Lead V6 in the midaxillary line at the same level as V4 and V5.
Describe augmented unipolar leads
There are three unipolar augmented leads: aVR, aVL and aVF. Any of the three limb electrodes can be used to record cardiac potential in comparison to the common terminal, e.g. voltage recorded in RA (right arm) can be determined by the equation.
RA − (RA + LA + LL) the resulting voltage is small because the potential difference is reduced by the RA potential in common terminal, i.e. (RA + LA + LL).
Disconnecting the RA lead from the common terminal increases the potential difference by 50% and results in augmented limb lead aVR.
aVR is the potential difference between RA and (LA + LL).
In this type of recording two of the limbs are connected through electrical resistances to the negative terminal of the electrocardiograph while the third limb is connected to positive terminal.
Name different waves and intervals in normal ECG
1. P wave. It is due to atrial depolarization. It is normally positive (upright) in the standard limb leads and inverted in aVR.
2. P-R interval. It is measured from the onset of P wave to the onset of QRS complex. Actually it is PQ interval but Q wave is frequently absent and therefore it is called P-R interval. It is a measure of the AV conduction time and includes the delay through AV node. Its duration normally varies from 0.12 to 0.2 seconds depending upon heart rate.
3. QRS complex. It is caused by ventricular depolarization. Its duration is normally less than 0.08 second. It is a measure of intraventricular conduction time.
4. Q-T interval. It is measured from beginning of ‘Q’ wave to the end of ‘T’ wave. Normally it is 0.35 second. Ventricular contraction usually lasts almost during this interval.
5. T wave. It is caused by ventricular repolarization and is normally in the same direction as the QRS complex, since ventricular repolarization follows the path that is opposite to depolarization.
6. RR interval. It is the time interval during successive QRS complexes. If it is 1 second, heart rate is 60 beats/min. Normally it is 0.83 second and therefore heart rate is 60/0.83 = 72 beats/min (Fig. 13.9).
What is P-R interval? When is it prolonged?
Interval from onset of P to the onset of QRS is called P-R interval. It measures conduction time from SA node to the ventricles. Normally it is 0.13 to 0.16 second. If it exceeds 0.2 second, it indicates impaired conduction through AV node. First degree block is produced when PR interval is between 0.2 to 0.3 second. Second degree block is produced when the PR interval is increased to 0.25 to 0.45 second.
What is the effect of complete atrioventricular block?
When there is complete atrioventricular block, impulses from atria cannot pass to the ventricles. Ventricles start beating at their own rhythm called idioventricular rhythm. ECG shows that there is complete dissociation between P waves and QRS complexes.
How much is normal QRS interval? When is it prolonged?
Normal QRS interval is 0.08 second. It should not exceed 0.1 second. It is measured from onset of ‘Q’ to the cessation of ‘S’ wave. It measures total ventricular depolarization time. If it is prolonged it indicates bundle branch block.
What is P-P interval?
P-P interval is the interval between two successive P waves. Equal P-P intervals indicate rhythmic depolarization of the atria.
What are the abnormalities in ‘T’ wave?
‘T’ wave is the repolarization wave of the ventricles. It is normally positive because apex of heart repolarizes earlier than the base of the heart. In old age it is flattened. Exercise increases its amplitude in healthy hearts. It is inverted when there is ischaemia (sometimes T wave is inverted in lead III without any apparent reason). Abnormalities of ‘T’ wave in shape, size, duration, direction in leads I and II are of diagnostic importance. These changes indicate myocardial damage associated with cardiac hypoxia (ischae-mia). When there is ischaemia of the cardiac muscle, ischaemic portion of the heart takes a longer time for depolarization.
What is Q-T interval? What does it indicate?
Q-T interval is measured from the onset of ‘Q’ wave to the end of ‘T’ wave. It is normally 0.36 second and it indicates total systolic time of ventricles.
What is T-P interval? What is its significance?
T-P interval is measured from the end of T wave to the beginning of P wave. It measures the diastolic period of the heart. Variable T-P intervals indicate atrioventricular dissociation.
Name the conditions which cause abnormal voltages of QRS complex
Voltage of QRS is measured from peak of R wave to the bottom of S wave. It varies between 0.5 and 2 mV (lead III recording lowest and lead II recording the highest voltage). When sum of voltages of QRS complex in three standard leads is greater than 4 mV, it is considered that the patient has a high voltage ECG.
The cause of this high voltage in most of the cases is increased muscular mass of the heart (hypertrophy).
There may be decreased voltage of ECG due to cardiac myopathies, pericardial effusion (due to short circuiting of electrical potentials generated by heart into pericardial fluid), pulmonary emphysema (due to decreased conduction of electric current through emphysematous lungs). Lungs thus prevent flow of electric current from heart to the surface electrodes.
When is prolonged and bizarre pattern QRS complex obtained?
When there is hypertrophy of the ventricle or ventricles, ventricle takes a longer time for depolarization and therefore QRS complex lasts for a longer time. It can also be prolonged if there is a block in either the bundle branches, or in Purkinje fibres. Bizarre QRS pattern is obtained when
What is ‘J’ point? What is its significance?
The exact point at which the wave of depolarization just completes its passage through the heart (occurs at the end of QRS complex), all parts of the ventricles are depolarized so that no current is flowing around the heart (even the current of injury disappears). Therefore, the potential of ECG at this instant is exactly zero voltage. This point is known as ‘J’ point. A horizontal line is drawn through all ‘J’ points is the zero potential line in ECG from which all potentials caused by current of injury must be measured. The potential of current of injury in each lead is the difference of the level of T-P segment of ECG and zero potential time. Potential of current of injury above the zero line is positive (lead I) and potential of current of injury below the zero line is negative (lead III).
What is ST segment shift?
Portion of ECG between end of QRS complex and the beginning of T wave is called ST segment. J point lies at the very beginning of this segment. Whenever there is current of injury, ST segment and T-P segment are not at the same potential level in the record. Actually T-P segment shifts away from zero potential and not the ST segment that is shifted away from the zero axis. Still mostly TP segment of ECG is considered as reference potential level rather than ‘J’ point. Therefore, when a current of injury is evident in ECG it is called ST segment shift.
What is mean electrical axis?
During most of the cycle of ventricular depolarization, the direction of electrical potential (negative to positive) is from the base of ventricles toward the apex. This preponderant direction of the potential during depolarization is called mean electrical axis of the ventricles or the mean QRS vector. The mean electrical axis of normal ventricles is 59 degrees but it can swing to left about 20 degrees or to the right about 100 degrees.
What is right axis deviation? When does it occur? How is it diagnosed?
When mean axis is deviated to right, i.e. MEA of about 170°, it is called right axis deviated. It is caused by right ventricular hypertrophy or right bundle branch block. This can be diagnosed by observing QRS complex in leads I and III. When there is right axis deviation, S wave is prominent in lead I and R wave is prominent in lead III (S1 R3 pattern).
What is left axis deviation? When does it occur? How is it diagnosed?
When mean electrical axis is deviated to left, it is called left axis deviation, i.e. mean axis is about −15°. This is associated with obesity, left ventricular hypertrophy or left bundle branch block. This can be diagnosed by observing QRS complex in leads I and III. When there is left axis deviation, R wave is prominent in lead I and S wave is prominent in lead III (R1 S3 pattern).
What is sinus rhythm?
Sinus rhythm is present when SA node is the pacemaker. It is assumed if each P wave is followed by a normal QRS complex. P-R and, Q-T intervals are normal and P-R interval is regular.
What is sinus arrhythmia?
In sinus arrhythmia, there is a sinus rhythm except that RR interval (cardiac rate) varies with respiration. Heart rate normally increases during inspiration and decreases during expiration.
What is AV nodal rhythm?
When AV node becomes the pacemaker, the rhythm recorded is AV nodal rhythm, i.e. there is ectopic pacing from AV node. It is also called junctional rhythm. It is characterized by inverted ‘P’ wave and normal QRS complex. The rate is slower than sinus.
What is atrial tachycardia?
Atrial tachycardia is the one which occurs when an atrial site (outside the SA node) becomes the dominant pacemaker.
What is a premature beat?
Premature beat (premature contraction or ectopic beat) is a contraction of the heart prior to the time that normal contraction would have been expected.
What is premature atrial beat?
When the ectopic focus of the premature beat is located in atrium, atrial premature beat or atrial beat is recorded. The ‘P’ wave of this beat occurs too soon in the heart cycle. P-R interval is shortened indicating that ectopic origin of the beat is near the AV node.
An interval between premature contraction and next succeeding contraction is slightly prolonged which is called compensatory pause. The reason for this is that the premature contraction originated in the atrium some distance from the sinus node and the impulse had to travel through a considerable amount of atrial muscle before it discharged the sinus node. Therefore, the sinus node discharged very late in premature cycle, and this made the succeeding heart beat also late in appearing. Premature atrial contractions may occur frequently in healthy persons.
What is pulse deficit?
During premature contraction, heart contracts ahead of time. The ventricles are sometimes not filled with blood normally and stroke volume output during the contraction is therefore decreased or sometimes even absent. Therefore, during such a contraction, pulse wave passing to periphery may be so weak that it is not felt at the radial artery. Thus a deficit in the number of pulses felt in the radial pulse in relation to number of contractions in the heart is called pulse deficit.
What is premature ventricular contraction?
When the ectopic focus of the premature beat is located in the Purkinje system or myocardium of the ventricle, ventricular ectopic beat is recorded. Here the QRS complex is usually considerably prolonged and it has a high voltage. T wave has got potential opposite to that of QRS complex.
What is paroxysmal tachycardia?
When there is increase in heart rate in paroxysms, it is called paroxysmal tachycardia. Paroxysms usually begin suddenly and last for few seconds. It is called atrial paroxysmal tachycardia or ventricular paroxysmal tachycardia depending upon the site of irritable focus.
What is atrial flutter?
When atrial rates are between 220 to 350/min, it is called atrial flutter. During atrial flutter AV node is unable to transmit all of the atrial impulses and therefore the ventricular rate is half, one-third or one-fourth of the atrial rate.
What is atrial fibrillation?
A totally irregular, rapid atrial rate in which there is contraction of only small portions of atrial musculature at any one time is called atrial fibrillation. ECG shows small irregular oscillations called F waves due to depolarization of small units of atrial musculature. There are no recognizable P waves. QRS and T waves are normal but RR interval is irregular.
What is ventricular fibrillation?
Rapid, irregular ineffective contractions of small segments of ventricular myocardium is termed ventricular fibrillation. In this, peripheral pulse is absent because cardiac output is zero. Condition can be distinguished from cardiac standstill only on ECG. ECG shows undulating waves of varying frequency and amplitude.
Haemodynamics
What is the function of arteries?
Arteries are the vessels which carry blood from heart to the periphery. They transport blood under high pressure to the tissues. For this reason, they have strong vascular walls. Blood flows rapidly in the arteries.
What are arterioles? What is their function?
Arterioles are small branches of arterial system. They act as control valves through which blood is released into the capillaries. They have strong muscular wall capable of contracting and completely closing and dilating, thereby controlling the blood flowing to the capillaries.
What is the function of capillaries?
Capillaries are thin-walled vessels. Their function is to exchange fluid, nutrients, electrolytes, hormones and other substances between the blood and the interstitial fluid.
What is the function of veins?
Veins are the vessels which carry the blood towards the heart. They are thin-walled and act as major reservoirs of blood. The walls are muscular and therefore veins can contract or expand and reserve small or large volume of blood depending on the needs of the body.
Explain the proportion of blood present in different parts of circulation
About 84% of the entire blood volume of the body is in the systemic circulation (64% in veins, 13% in arteries, 7% in systemic arterioles and capillaries). Heart contains 7% of blood volume and pulmonary vessels contain 9% of blood volume.
What is the relationship between velocity of blood flow and cross-sectional area of the vessels?
Cross-sectional area of veins is about four times larger than that of arteries. Therefore, there is large storage of blood in venous system as compared to in the arterial system, because velocity of blood flow is inversely proportional to the cross-sectional area.
Which vessels have largest cross-sectional area?
Capillaries have largest cross-sectional area, i.e. 2500 cm2.
Describe how does pressure change in various portions of circulation
The pressure in aorta is highest because blood is pumped by heart continuously in aorta. As blood flows to systemic circulation, pressure falls progressively to approximately zero by the time it reaches the right atrium.
Pressure in aorta varies between 120 and 80 mmHg during systole and diastole of the heart respectively. Average pressure in aorta is about 100 mmHg.
In systemic capillaries pressure drops to 35 mmHg at the arterial ends and about 10 mmHg at the venous end with average functional pressure equal to 17 mmHg.
In pulmonary circulation pressure is much less. In pulmonary artery systolic pressure is 25 mmHg and diastolic pressure is of 8 mmHg. The average pulmonary capillary pressure is about 7 mmHg.
Explain the relationship between pressure, flow and resistance
Flow of blood through any vessel is determined by two factors:
Name the methods of measuring blood flow
Blood flow is expressed in ml/s or l/min. It is measured by:
What is streamline or laminar flow?
When each layer of blood remains the same distance from the wall while flowing through a long smooth vessel, it is called streamline or laminar flow. When the flow is streamline, blood flows at a steady rate.
What is turbulent flow?
When blood flows crosswise in the vessel as well as along the vessel usually forming whorls in the blood called eddy currents, the flow is said to be turbulent. When eddy currents are present blood flows with much greater resistance than when the flow is streamline because of increased friction of flow caused by eddy currents.
Explain factors causing tendency for turbulent flow
The tendency for turbulent flow is directly proportional to the velocity of blood flow, diameter of blood vessel and is inversely proportional to viscosity of the blood divided by its density.
Reynolds’ number is a measure of tendency to turbulence to occur. It is calculated as follows:
When Reynolds’ number rises above 200 to 400, turbulent flow will occur. When it is about 2000, turbulence will occur even in straight smooth vessel. In large arteries even normally Reynolds’ number rises to 200 to 2000. Therefore, there is always some turbulent flow.
What is the unit for resistance?
Unit for expressing resistance is the peripheral resistance unit (PRU). If pressure difference between two points in a vessel is 1 mmHg and the blood flow is 1 ml/sec, the resistance is said to be 1 PRU.
Occasionally resistance is expressed in CGS units as dyne sec/cm5 and is calculated by following formula:

How much is the total peripheral resistance normally?
At rest, rate of blood flow through circulatory system is 100 ml/s and the pressure difference from systemic arteries to systemic veins is 100 mmHg. Therefore, total peripheral resistance is 100/100, i.e. 1 PRU. It can increase to 4 PRU when vessels are strongly constricted. It can fall to low as 0.2 PRU when vessels become greatly dilated.
In pulmonary circulation, the net pressure difference (pulmonary arterial and left atrial pressure) is 14 mmHg whereas rate of blood flow is 100 ml/s. Therefore, total pulmonary resistance at rest is 0.14 PRU.
What is conductance of flow in a vessel?
Conductance is a blood flow through a vessel for a given pressure difference expressed as ml/s/mmHg. It is the reciprocal of resistance.

It changes directly with the diameter of vessel. The relationship is as follows:

Conductance thus increases in proportion to fourth power of the diameter.
What is Poiseuille's law?
Poiseuille's law is the formula which is useful in calculating the rate of blood flow in a vessel. According to it
Thus from the formula it is clear that the diameter of the vessel plays the greatest role in determining the rate of blood flow. This makes it possible for the arterioles, responding with small changes in diameter to nervous or local signals either to turn off completely the blood flow to the tissues or to cause a vast increase in blood flow.
Name major factors affecting resistance to blood flow
According to Poiseuille's law, 
Where r = radius of vessel, η = viscosity of blood, and l = length of the vessel.
How does viscosity of blood affect the blood flow?
According to Poiseuille's law, greater the viscosity, lesser is the blood flow. Viscosity in turn depends upon the haematocrit, i.e. percentage of cells. Greater the haematocrit, greater is the viscosity. Blood flow in very minute tubes exhibits far less viscosity effect because in these tubes red cells instead of moving randomly line up and move through the vessel thus eliminating viscous resistance.
What is the effect of pressure on vascular resistance and tissue blood flow?
Increase in arterial pressure greatly increases the blood flow because of two factors:
What is the importance of vascular distensibility?
All the vessels are distensible. Distensible nature of the arteries allows them to accommodate the pulsatile output of the heart and to average out the pressure pulsation. This provides almost smooth, continuous blood flow through the tissues.
Veins are most distensible vessels, therefore they act as blood reservoirs and store large quantities of blood which can be called into use whenever required.
In pulmonary circulation, veins are similar to those of systemic veins. Pulmonary arteries normally operate under low pressure and have distensibilities about one-half those of veins.
What is the unit of vascular distensibility?
Vascular distensibility is expressed as the fractional increase in volume for each mmHg rise in pressure.

What is vascular compliance?
Vascular compliance is the total quantity of blood that can be stored in a given portion of circulation for each mmHg pressure rise

Compliance of vein is about 24 times that of corresponding artery because it is 8 times as distensible and has a volume 3 times as great. Therefore, compliance is equal to distensibility × volume.
What is the relationship between volume and pressure in arterial system and venous system? What is the effect of sympathetic stimulation?
With mean arterial pressure of 100 mmHg, arterial system (larger and smaller arteries, arterioles) have 750 ml of blood which reduces to 500 ml when pressure falls to zero.
Normally, venous system contains 2500 ml of blood and tremendous changes in the volume are required to change the pressure. Sympathetic stimulation increases the smooth muscle tone of the vessels. This in turn increases the pressure. This causes large volume of blood to shift into the heart.
What is stress relaxation?
When extra volume of blood is suddenly injected into a vessel, at first there will be a large pressure increase but because of stretching of the wall, smooth muscle fibres of the vessel will relax and this will allow pressure to return back towards the normal. This phenomenon is known as stress relaxation.
Pulse
What is pulse?
It is the wave of expansion that passes along the arterial tree from aorta to the peripheral arteries during systole of the heart.
Normally which artery do you choose for feeling the pulse? Why?
Pulse is felt at the radial artery because the artery is superficial and it lies on the bone. On examination of pulse, one notes rate, rhythm, volume, tension, equality of both sides, etc.
What is pulsus paradoxus?
Pulsus paradoxus is the condition in which pulse becomes very strong (high volume) during inspiration and very weak (low volume) during expiration. Thus pulse becomes very strong and very weak alternately in relation to that of respiratory cycle. Normally also pulse volume increases during inspiration and decreases during expiration. But this change is so small that it is hardly noticed. When the change becomes very prominent, pulse is described as pulsus paradoxus. This type of pulse is noticed during deep breathing, cardiac tamponade (compression of heart from outside due to fluid in pericardial sac, constructive pericarditis, etc.). Under such conditions during inspiration there is increased (greater than normal) negative pressure in the thorax, venous return is increased, this in turn increases the stroke volume and pulse becomes stronger. Exactly opposite changes occur during expiration leading to reduced volume of pulse (weak pulse).
Venous system
What is central venous pressure?
Pressure in the right atrium is known as central venous pressure because all the systemic veins open into the right atrium.
Name the factors determining right atrial pressure
Right atrial pressure depends on balance between ability of atrium to pump the blood into the ventricle and the tendency for blood to flow from the peripheral vessels into right atrium. If right atrium is pumping strongly, the right atrial pressure tends to decrease. Weakness of the atrial wall tends to increase the right atrial pressure. Increase in flow of blood into the right atrium through veins (venous return) increases the right atrial pressure and vice versa.
How much is normal right atrial pressure? When does it rise or fall?
Normal right atrial pressure is zero mmHg (i.e. equal to atmospheric pressure). The pressure in the right atrium can rise as high as 20 to 30 mmHg in following abnormal conditions:
Right atrial pressure can decrease to as low as −3 to −5 mmHg due to the following reasons:
How much is the pressure in the large veins?
Large veins do not offer any resistance when they are distended. But at the entry of thorax most of the large veins are compressed at many points by the surrounding tissues. This impedes the blood flow. Therefore, large veins do offer considerable resistance to blood flow and thus pressure in the peripheral veins is greater than that of the right atrial pressure. It is 4 to 7 mmHg. Venous pressure rises in heart failure.
What is hydrostatic pressure? How much is it in vascular system?
Pressure at the surface of water is equal to the atmospheric pressure, i.e. zero mmHg but the pressure rises by 1 mmHg for each 13.6 mm distance below the surface. This pressure results due to weight of water and therefore is called hydrostatic pressure.
Hydrostatic pressure in vascular system
When a person is standing absolutely still
• Hydrostatic pressure in veins between heart and feet is +90 mmHg. Venous pressure at other levels of the body varies between 0 to 90 mmHg.
• Neck veins completely collapse due to atmospheric pressure on the outside of the neck. Therefore, pressure inside them almost remains zero.
• Veins in the skull are in non-collapsible chamber and thus they do not collapse. Therefore, negative hydrostatic pressure (−10 mmHg) exits in dural sinuses of head.
How does hydrostatic factor affect the arterial pressure?
Hydrostatic factor also affects the peripheral pressures in the arteries, e.g. standing person has arterial pressure of 190 mmHg in the feet. Therefore, arterial pressure is stated as pressure at the hydrostatic level of heart.
What is the function of valves in the veins?
The venous pressure in feet is always +90 mmHg in a standing position because of hydrostatic pressure effect. Movement of legs and muscle contractions (muscle pump) squeeze the blood out of veins. The valves are arranged in the veins so that direction of blood can only be towards the heart. This lowers the pressure in the veins. Therefore, in walking adult, venous pressure remains less than 25 mmHg.
What are varicose veins?
The valves in the venous system become incompetent (when there is overstretching of veins by excess venous pressure as in pregnancy). Stretching of the veins increases their cross-sectional area and valves of the veins no longer remain functional because of which there is failure of muscle pump leading to further increase in size of the veins and destroys the function of valves entirely. Thus large, bulbous protrusions of the veins called varicose veins develop.
How is venous pressure assessed?
Clinically venous pressure is assessed by observing the degree of distension of neck veins. When right atrial pressure is increased up to 10 mmHg, the lower neck veins begin to protrude in sitting position (in normal person in this position neck veins are never distended).
Venous pressure can be measured directly by inserting needle into the vein and connecting it to a pressure recorder. Right atrial pressure can be measured by inserting a catheter through the veins into the right atrium.
What is the function of veins?
Sixty per cent of the circulating blood is present in the venous system. So it serves as a blood reservoir. Especially extensive and compliant areas which act as specific blood reservoirs are liver sinuses, large abdominal veins, venous plexus beneath the skin and spleen.
Capillary system
What is the structure of capillary system?
Capillaries are thin-walled vessels which lie between arterioles and venules and supply blood to the tissues. Blood from arterioles passes into metarterioles → capillaries → venules → returns to the general circulation.
Arterioles are highly muscular and can change their diameter. The metarterioles (the terminal arterioles) do not have continuous muscle coat but at the point from where true capillaries originate smooth muscle fibres encircle the metarteriole forming precapillary sphincter. This sphincter can open or close the entrance to the capillaries. Total surface area of tissue capillaries is 500 to 700 sqm.
Capillary is lined by unicellular layer of endothelial cells which is surrounded by basement membrane on the outside. The diameter of capillary is 4 to 9 u. barely large enough for the passage of red blood cells, other blood cells squeeze through it. Thin slit lying between two endothelial cells of the capillary wall is called intercellular cleft. Each of this cleft is interrupted periodically by short ridges of protein attachments that hold the endothelial cells together but each ridge in turn is broken after a short distance, so that in between them fluid can percolate through the cleft. Cleft usually has a uniform spacing with a width of approximately 6 to 7 nm. These are termed ‘slit pores’. In some tissues, pores in the capillaries have special characteristics, e.g. (a) In the brain, junctions between capillary endothelial cells are tight junctions allowing only small molecules to pass into the brain tissue and therefore act as blood-brain barrier. (b) In the liver, clefts or pores are very wide so that even plasma proteins can pass from the blood into the liver tissues. (c) In kidney, number of small oval windows called fenestrae penetrate directly through the middle of endothelial cells in addition to clefts.
Blood flows into the capillaries intermittently, because of phenomenon of vasomo-tion, i.e. intermittent contraction of metarterioles and precapillary sphincters. This in turn is mainly controlled by concentration of oxygen in the tissues.
What is the function of capillary system?
Function of capillaries is to maintain average rate of blood flow through each tissue. Capillary bed maintains average capillary pressure and average rate of transfer of substances between blood of capillaries and the surrounding interstitial fluid.
Lipid soluble substances can directly diffuse through the cell membranes of the capillary. Water soluble substances cannot pass through lipid membranes of endothe-lial cells. Such substances pass through the pores.
What is interstitium? What is present in it?
Spaces between the cells are collectively known as interstitium. It contains fluid known as interstitial fluid and two major types of solid structures—collagen fibres and proteoglycan filaments. Collagen fibres are strong and therefore they provide most of the tensional strength to the tissue. Proteoglycan filaments form fine reticular filaments described as ‘brush pile’.
Proteoglycan filaments and fluid entrapped in them has a characteristic of gel and is called tissue gel. Rest of the fluid (which is in very small quantity) forms the free fluid. This amount is very slight (less than 1%). When the free fluid in the tissue space increases, oedema results. Free fluid and gel are continuously interchanging with each other.
State the factors determining fluid movement from blood to interstitial fluid and in opposite direction.
Following factors affect the fluid movement between blood in capillaries and the interstitial fluid:
1. Capillary pressure. This tends to force the fluid out through the capillary membrane. At the arterial end of capillary, pressure is 30 to 40 mmHg and at the venous end of capillary, pressure is 10 to 15 mmHg and in the middle, pressure is about 25 mmHg.
2. Interstitial fluid pressure. This tends to force fluid inward through the capillary membrane. It is about −3 to −5 mmHg.
3. Plasma colloid osmotic pressure. This tends to cause inward movement of fluid through the capillary membrane. It is about 28 mmHg.
4. The interstitial fluid colloid osmotic pressure. This tends to cause the fluid movement outward through the capillary membrane and it is about 8 mmHg.
Control of blood flow
What are the functions of tissue blood flow?
• Delivery of oxygen to the tissues.
• Delivery of other nutrients to the tissues.
• Removal of CO2 from the tissues.
• Removal of hydrogen ions from the tissues.
• Maintenance of proper concentration of other ions in the tissues.
• Transport of various hormones and other specific substances to the different tissues.
Blood flow to the various tissues is usually regulated at the minimal level that will supply its requirements, neither more, nor less.
Name the local mechanisms controlling blood flow
Local blood flow control occurs in two different phases:
1. Acute control occurs by rapid changes in local constriction of arterioles, metarterioles and precapillary sphincters. This occurs within seconds or minutes.
2. Long-term control causes slow change in the flow over a period of days, weeks or even months. This is due to increase or decrease in physical sizes and the number of blood vessels supplying the tissue.
Describe acute control of local blood flow
Local blood flow increases with increase in rate of tissue metabolism and vice versa. There are two basic theories for regulation of blood flow:
1. Vasodilator theory. Greater the rate of metabolism, lesser is the blood flow and lesser is the availability of oxygen and other nutrients to the tissues. This causes greater release of certain vasodilator substances from the tissues. These substances diffuse to precapillary sphincters, metarterioles and arterioles to cause their dilatation. Different vasodilator substances suggested are adenosine, CO2, lactic acid, adenosine phosphate compounds, histamine, potassium ions and hydrogen ions. Most of these substances are released in response to oxygen deficiency (especially adenosine and lactic acid). Adenosine plays important role in controlling coronary blood flow. But it is difficult to prove whether sufficient quantifies of any single vasodilator substance are formed in the tissues to cause measured increase in blood flow. Probably there is a combined effect of number of vasodilator substances.
2. O2 demand theory (nutrient demand theory). O2 is required to maintain vascular muscle contraction. In absence of adequate blood flow, there is inadequate supply of oxygen and other nutrients. This causes vasodilatation because of opening of precapil-lary sphincters and metarterioles.
Normally precapillary sphincters and metarterioles, open and close cyclically (vaso-motion). When there is a lack of oxygen, precapillary sphincters cannot contract properly. They open up and remain open for a long time. When O2 concentration is high, precapillary sphincters and metarterioles close and remain closed until tissue cells consume excess oxygen and oxygen concentration comes back to normal. Similarly, lack of glucose, also has the same effect as lack of O2 on smooth muscle of precapillary sphincters and metarterioles.
What is the reactive hyperaemia?
When blood supply to a tissue is blocked for a few seconds to several hours and then is unblocked, the flow through the tissue usually increases to about five times normal and increased flow continues for few seconds to few hours (depending on how long the flow was blocked). This phenomenon is known as reactive hyperaemia. This is due to metabolic control of local blood flow and explains close relationship between local blood flow regulation and delivery of nutrients to the tissues.
What is active hyperaemia?
When tissue becomes very active, such as during exercise, the rate of blood flow to the tissues increases. This is due to relative lack of nutrients and O2 leading to local vasodilatation. This is known as active hyperaemia.
What is the effect of arterial blood pressure on blood flow to the tissue?
Blood flow is maintained relatively normal despite of the arterial pressure variation between 70 to 175 mmHg. This is called autoregulation of blood flow. It is explained by two theories:
1. Metabolic theory. When arterial blood pressure increases, the excess flow provides too many nutrients to the tissues and it also flushes the vasodilator substances. These two effects cause blood vessels to constrict and flow returns to almost normal despite of the increased pressure.
2. Myogenic theory. It is observed that sudden stretch on the small blood vessels causes smooth muscles of blood vessel wall to contract. Therefore, when arterial blood pressure increases and stretches the vessel, it causes vascular contraction and reduces the blood flow nearly back to normal. Conversely at low blood pressures, the degree of stretch of the vessel is less, so that smooth muscle of the vessel relaxes and allows increased blood flow.
It is yet doubtful whether myogenic autoregulation is powerful mechanism.
Explain the long-term mechanism of blood flow regulation
Long-term mechanism gives far more complete regulation than the acute mechanism. In this mechanism, degree of vascularity of the tissues changes. There is reconstruction of tissue vasculature to meet the needs of the tissue, e.g. arterial pressure falls to 60 mmHg and remains at this level for a long time. The physical structural sizes of the vessels in the tissue increase and also the number of vessels increase.
Probable stimulus for increased or decreased vascularity in many instances is needed for tissue oxygen, e.g. increased vascularity occurs in tissues of many animals who live at high altitude.
Angiogenesis, i.e. growth of new blood vessels occurs mainly in response to ang-iogenic factors released from: (a) ischaemic tissues, (b) tissues that are growing rapidly, and (c) tissues having excessively high metabolic rate.
Many angiogenic factors are small peptides. Three of them are most important. They are endothelial cell growth factor (ECGF), fibroblast growth factor (FGF) and angiotensin. They are released either from the tumours or from other tissues that generally have inadequate blood supply. Deficiency of oxygen and other nutrients leads to formation of these factors. Essentially all the angiogenic factors promote new vessel growth in the same manner. They cause sprouting of new vessels from either venules or capillaries in following steps:
• Dissolution of basement membrane of the endothelial cells.
• Rapid reproduction of endothelial cells.
• Streaming out of new endothelial cells out of the vessel wall in extended cords towards the source of angiogenic factor.
• Continued division of the cells in the cord and their folding in tube.
• Connection of the tube with another tube budding from another donor vessel, forming capillary loop.
What is collateral circulation?
When either an artery or a vein is blocked, a new vascular channel usually develops around the blockage and allows at least partial resupply of blood to the affected tissue. The circulation through these new channels is called collateral circulation.
What is humoral regulation of circulation?
Humoral regulation of circulation is regulation by substances secreted into or absorbed into body fluids, e.g. hormones, ions, etc. Most important humoral factors affecting circulation are:
1 Vasoconstrictive agents
• Norepinephrine and epinephrine. Especially norepinephrine is a powerful vasoconstrictor. Epinephrine is less effective because it causes vasodilatation at certain places, e.g. coronary arteries. These hormones are released on sympathetic stimulation as in exercise.
• Angiotensin. It is also a powerful vasoconstrictor. It causes vasoconstriction of small arterioles and increases total peripheral resistance and the arterial blood pressure.
• Vasopressin or ADH. ADH is also a very powerful vasoconstrictor, but usually it is secreted in minute quantities and therefore mainly affects water reabsorption in renal tubules. But after a severe haemorrhage its concentration rises to a high level and then it has vasoconstrictive effect.
2 Vasodilator agents
• Bradykinin. It causes arteriolar dilatation and increased capillary permeability. It plays role in regulating blood flow in the skin and in salivary and gastrointestinal glands.
• Serotonin. It is present in high concentration in chromaffin tissue of intestine and other abdominal structures and in platelets. It has vasodilator or vasoconstrictor effect depending upon the condition or area of circulation. Its function in regulation of blood flow is almost unknown.
• Histamine. It is released by every tissue when it is damaged, inflamed or is subject to the allergic reaction. Mostly it is derived from the mast cells. It has a powerful vasodilator effect on arterioles.
What is the effect of different ions on the vessels?
1. Increase in calcium ion concentration causes vasoconstriction due to stimulating effect of calcium on smooth muscle.
2. Increase in potassium ion concentration causes vasodilatation as a result of inhibition of smooth muscle due to excess potassium.
3. Increase in magnesium ion concentration also causes vasodilatation as magnesium inhibits the smooth muscle.
4. Increase in sodium ion concentration causes mild arteriolar dilatation, due to increase in osmolality of blood. Anions, urates and citrate cause mild degree of vasodilatation.
5. Increase in hydrogen ion concentration also causes dilatation of arterioles.
Nervous control of blood flow
Describe sympathetic and parasympathetic nerve supply to heart and vessels
There is autonomic nerve supply to the heart and blood vessels, i.e. sympathetic and parasympathetic supply. The most important system which controls circulation is the sympathetic nervous system.
1. Sympathetic supply. All the blood vessels except capillaries, precapillary sphincters and metarterioles are innervated by sympathetic nerves.
Stimulation of sympathetic nerves to small arteries and arterioles causes vasocon-striction and therefore increased peripheral resistance, thus changing rate of blood flow to the tissues. There are very few vasodilator fibres supplying the vessels.
Stimulating sympathetic nerves to large vessels especially veins cause their constriction and therefore blood stored in them is translocated to the heart. This increases the venous return and therefore the cardiac output (plays a major role in regulation of cardiovascular function). Stimulation of sympathetic nerves to heart causes increase in the heart rate (positive chronotropic), increase in the force of contraction of the heart (positive inotropic), increased rate of conduction of impulse through the heart (positive dromotropic) and increased excitability (positive bathmotropic).
2. Parasympathetic supply. Parasympathetic fibres are carried to the heart through vagus nerve. The effect of parasympathetic stimulation is to decrease the heart rate, force of contraction, rate of conduction of impulse through the heart and decreased excitability (negative chronotropic, inotropic, dromotropic and bathmotropic effects). There is no parasympathetic supply to blood vessels.
Blood pressure
What is blood pressure?
Blood pressure is the lateral pressure exerted by flowing blood on the walls of the vessels. Systolic pressure is the maximum pressure during systole and diastolic pressure is the minimum pressure in the arteries during diastole.
How much is normal blood pressure?
Normal systolic pressure in adult is 120 ± 15 mmHg and diastolic pressure varies from 80 ± 10 mmHg.
What is mean arterial pressure?
Mean arterial pressure is the average of all the pressures measured millisecond by millisecond over a period of time. It is determined by adding 60% diastolic and 40% systolic pressure. It is about 100 mmHg.
When mean arterial pressure is chronically above 110 mmHg, person is labelled is hypertensive. Hypertension can be mild, moderate or severe.
Vasomotor centre
Describe the vasomotor centre
Vasomotor centre is situated bilaterally in the reticular substance of medulla and lower third of pons. It transmits impulses through the spinal cord and then through vasoconstrictor fibres to almost all the blood vessels. Following are certain important areas in the centre (Fig. 13.10):
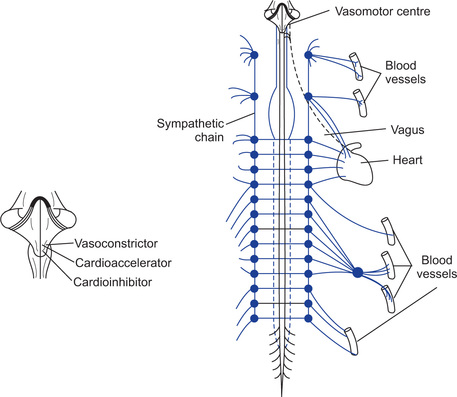
• Vasoconstrictor area. It is also called area C-1. It is located bilaterally in the anterolateral portions of upper medulla.
• Vasodilator area. It is called area A-1. It is located bilaterally in anterolateral portions of lower half of medulla.
• Sensory area. It is called area A-2. It is located bilaterally in the tractus solitarius, in the posterolateral portions of the medulla and lower pons. Neurons in this area receive signals from glossopharyngeal and vagus nerves.
What is vasomotor tone?
Vasoconstrictor area of vasomotor centre transmits signals continuously through the sympathetic vasoconstrictor fibres to the blood vessels. These impulses maintain partial state of contraction in the blood vessel which is called vasomotor tone.
How does vasomotor centre control heart activity?
Lateral portions of vasomotor centre transmit excitatory signals through the sympathetic nerves to the heart. The medial portion of the vasomotor centre which lies near the dorsal motor nucleus of vagus nerve transmits inhibitory impulses to the heart through the vagus nerve.
Thus vasomotor centre can either increase or decrease the heart activity.
Describe the role of higher centres in controlling the vasomotor centre
Higher centres control the vasomotor centre as follows:
1. Reticular substance of pons, mesencephalon and diencephalon. Lateral and superior portions of reticular substance cause excitation of the vasomotor centre. Medial and inferior portions of reticular substance cause inhibition of the vasomo-tor centre.
2. Hypothalamus. Posterolateral portions of hypothalamus cause excitation whereas the anterior part causes mild excitation or inhibition of vasomotor centre.
3. Cerebral cortex. Stimulation of motor cortex excites the vasomotor centre because of impulses transmitted to it via hypothalamus. Stimulation of anterior temporal lobe, orbital areas of frontal cortex, anterior part of cingulate gyrus, amygdala and septum can either excite or inhibit the vasomotor centre.
Explain the role of sympathetic vasodilator fibres
Vasodilator sympathetic fibres mainly supply the skeletal muscles. Anterior hypothala-mus mainly controls their activity. It plays role only during muscular exercise causing initial vasodilatation in the vessels of skeletal muscles to cause anticipatory rise in their blood flow.
What is vasovagal syncopy?
Fainting occurs when the person has intense emotional disturbances. This is due to intense stimulation of vasodilator fibres to skeletal muscle and at the same time transmission of strong inhibitory signals through the vagus nerve to the heart. There is fall in arterial pressure, decreased blood supply to the brain and person loses consciousness. This effect is known as vasovagal syncopy.
Explain the role of nervous system in controlling arterial pressure
Nervous system is capable of controlling the circulation to cause rapid increase in arterial pressure. This is done by arteriolar constriction, constriction of veins and direct stimulation of the heart. The pressure rises within few seconds. Conversely sudden inhibition of nervous system can cause fall in arterial pressure within 10 to 40 seconds. Thus nervous control of arterial pressure is most rapid.
Short-Term mechanisms regulating blood pressure
Enumerate various short-term mechanisms regulating blood arterial pressure
The various short-term mechanisms regulating blood pressure are:
Describe the anatomy of baroreceptors
Baroreceptors or pressoreceptors are the stretch receptors and are located in the walls of large systemic arteries. They are extremely abundant in two areas:
• Wall of internal carotid artery slightly above the carotid bifurcation is known as carotid sinus.
• Wall of aortic arch is known as aortic sinus. Baroreceptors are spray type nerve endings lying in the walls. They are stimulated when stretched.
Impulses from carotid sinus are carried by Hering's nerves to the glossopharyngeal nerve and then to tractus solitarius of medulla. Impulses from aortic sinus are carried through vagus nerve to the tractus solitarius (Fig. 13.11).
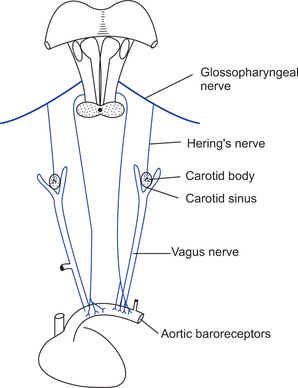
Explain the response of baroreceptors to changes in arterial pressure
Baroreceptors are stimulated on distension of the vessel wall. The carotid sinus represents the most distensible area of the arterial system. Carotid sinus baroreceptors are not stimulated at all when pressure is between 0 and 60 mmHg. They respond progressively more and more rapidly and reach maximum at 180 mmHg pressure.
Baroreceptors respond much more rapidly to changing pressures than to a stationary pressure. The normal operating range of baroreceptor varies from 60 to 180 mmHg. The normal arterial pressure is around 100 mmHg. A slight change in pressure causes strong autonomic reflexes to readjust the pressure.
Thus baroreceptor reflex mechanism functions most effectively in the pressure range where it is most needed.
Describe the baroreceptor reflex
When the blood pressure increases above the normal level, it causes baroreceptor reflex as follows:
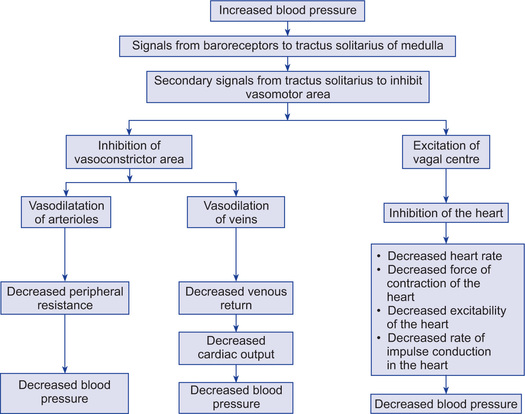
Thus blood pressure returns back to normal.
Exactly opposite sequence of events occur when blood pressure is lowered.
Explain buffer function of the baroreceptor reflex
Baroreceptor system opposes either increase or decrease in arterial pressure and therefore it is called pressure buffer system and the nerves from the baroreceptors are called buffer nerves. This is possible because the baroreceptor system operates within 60 to 180 mmHg pressure.
Baroreceptors therefore relatively maintain constant arterial pressure during various activities or changes in position, e.g. if the person who is lying down suddenly stands, this can cause arterial pressure in the head and upper part of the body to fall and marked reduction can cause unconsciousness. But this is not allowed to occur, because of falling pressure in the baroreceptors. When the person stands, he will elicit baroreceptor reflex resulting into sympathetic discharge minimizing the decrease in pressure in the head and upper part of the body.
Why baroreceptor system is ineffective in causing long-term regulation of blood pressure?
When there is increase in blood pressure, baroreceptors send impulses but later on rate becomes slower and slower (adaptation).
Describe the role of chemoreceptors in control of blood pressure
Carotid and aortic bodies contain chemoreceptors which are mainly stimulated by chemical stimuli such as oxygen lack, carbon dioxide excess and hydrogen ion excess. They are profusely supplied with blood and therefore when blood pressure falls below a critical level 80 mmHg chemoreceptors are stimulated because of diminished blood flow resulting into diminished O2 supply and building up of CO2 and H+ ions. They send impulse through Hering's nerves (from carotid bodies) and vagi nerves (from aortic bodies) to the vasomotor centre. This elevates arterial pressure. Thus reflex is responsible for bringing arterial pressure back to normal. But this reflex is not very powerful controller of arterial blood pressure. Still it is important as it is stimulated at low pressure and helps in preventing further fall in blood pressure.
Describe atrial reflex
Atria contain stretch receptors. These are also called low pressure receptors. They play role in minimizing the effect of decreased blood volume on arterial blood pressure. The reflex occurs as follows:
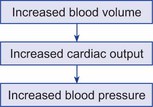
This pressure is brought to normal as follows:
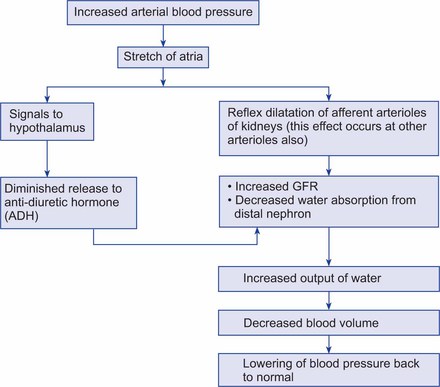
Increase in atrial pressure also causes an increase in the heart rate. This is partly due to direct effect of stretching the sinus node but is mostly due to Bainbridge reflex. Stimulation of stretch receptors in atria → afferent signals through vagus to medulla of brain → efferent signals are transmitted through vagus and sympathetic nerves to increase heart rate and probably also the strength of contraction of heart.
What is CNS ischaemic response?
When blood flow to the vasomotor centre in the brain stem is decreased enough to cause nutritional deficiency (i.e. cerebral ischaemia) the neurons in the vasomotor centre are strongly excited. This is due to accumulation of CO2, lactic acid locally near the vasomotor centre. Excitation of vasomotor centre causes strong sympathetic stimulation leading to vasoconstriction leading to increase in blood pressure. Peripheral vessels become totally occluded at certain areas, e.g. kidneys. This most powerful response that activates sympathetic vasoconstrictor system strongly is called CNS ischaemic response. It is initiated when blood pressure falls below 60 mmHg. This acts as an emergency arterial pressure control system. If rise of pressure does not relieve CNS ischae-mia, neuronal cells begin to suffer and within 3 to 10 minutes become totally inactive.
What is Cushing reaction?
When CSF pressure rises and becomes equal to arterial pressure, it compresses the arteries in the brain and cuts off the blood supply to the brain. This initiates the CNS ischaemic response. This causes rise in blood pressure. When blood pressure becomes greater than CSF pressure, blood flows through the vessels of brain and ischaemia is relieved. Blood pressure comes to equilibrium at a new level. This effect is called Cushing reaction. It protects the vital centres in the brain.
What is the role of skeletal nerves and muscles in controlling blood pressure?
Though mostly autonomic nervous system controls circulation, the skeletal nerves and muscles play role as follows:
1. Abdominal compression reflex. Whenever vasomotor centre is stimulated (e.g. baroreceptor reflex, chemoreceptor reflex) other reticular areas of brain stem are also stimulated. They send simultaneous impulses through skeletal nerves to skeletal muscles of the body especially abdominal muscles. Contraction of abdominal muscles compresses the abdominal venous reservoirs. This causes increased venous return to the heart and therefore increased cardiac output. This overall response is called abdominal compression reflex.
2. During exercise. During exercise the skeletal muscles contract and compress the blood vessels. This causes translocation of large quantities of blood from the peripheral vessels into the heart and lungs. This increases the cardiac output.
What is the role of nervous reflexes described above in maintaining the blood pressure?
Nervous reflexes cause rapid, powerful but short-term regulation of the arterial blood pressure. They gradually lose their ability with time because of adaptation of receptors.
What is stress relaxation and reverse stress relaxation?
When blood pressure is high, after some time smooth muscle of blood vessel relaxes leading to vasodilation and fall in blood pressure this is termed stress relaxation.
When blood volume and pressure is low the vessel constricts over a small volume and pressure inside rises, this is termed reverse stress relaxation.
Explain role of capillary fluid shift mechanism in regulation of blood pressure
When arterial blood pressure rises, the pressure at arterial end of capillaries becomes higher than normal. This causes greater fluid to be shifted from capillaries to interstitial fluid. This in turn reduces the total circulating blood volume and venous return and thus reduces the blood pressure.
When arterial blood pressure falls, pressure at arterial end of capillaries and therefore at venous end of capillaries is reduced.
This causes greater absorption of fluid from interstitial space into the capillary. This increases blood volume and therefore the blood pressure.
Long-Term mechanisms regulating blood pressure
What is the basis for long-term regulation of blood pressure?
When there is increase in extracellular fluid volume, it causes rise in blood volume and therefore rise in blood pressure. Rising pressure has a direct effect on kidneys to excrete excess of water (pressure diuresis) and also increase output of sodium (pressure natri-uresis). Pressure diuresis and pressure natriuresis bring blood volume back to normal and therefore returning blood pressure back to normal.
Thus pressure diuresis and natriuresis is the fundamental mechanism of long-term regulation of blood pressure. With evolution however multiple refinements have been added to make the fundamental system more exact in its control. Especially important refinement is renin-angiotensin mechanism.
What is the role of salt in renal body fluid mechanism for controlling blood pressure?
Accumulation of salt indirectly increases the extracellular fluid volume because of two reasons:
1. When there is excess salt in the body, there is increased osmolality of body fluids. This increased osmolality stimulates the thirst centre, making person drink large quantities of water to dilute the extracellular fluid. Thus there is increase in extracellular fluid volume.
2. Increased osmolality of body fluids also stimulates hypothalamic posterior pituitary gland system to secrete increased quantities of ADH (antidiuretic hormone). This causes increased reabsorption of fluid from the distal renal tubules. This causes increase in extracellular fluid volume.
What is renin? What is its role in long-term regulation of blood pressure?
Renin is a protein synthesized by juxtaglomerular cells of the kidneys. It is secreted in inactive form called prorenin and is stored in the juxtaglomerular cells. Renin is an enzyme. It acts on the substrate, i.e. plasma globulin or renin substrate or angiotensino-gen present in the blood to release angiotensin I. This angiotensin I is converted to angiotensin II by angiotensin converting enzyme present in small vessels mainly in the lungs. Angiotensin II has two principal effects by which it causes elevation of arterial pressure as follows:
• It is a powerful vasoconstrictor. Therefore, causes powerful vasoconstriction of arterioles and to a lesser extent also of veins. Constriction of arterioles increases the peripheral resistance and thus also increases the blood pressure. Mild constriction of veins increases the venous return. This in turn increases the cardiac output. Increased cardiac output increases the blood pressure.
• It directly acts on renal tubules and causes decreased excretion of salt and water. This causes increase in extracellular fluid volume and therefore the blood pressure.
• Angiotensin also increases salt and water retention by kidneys indirectly by stimulating release of aldosterone from the adrenal cortex.
Aldosterone in turn acts on distal renal tubules to cause increased absorption of salt and water.
What is one kidney Goldblatt's hypertension?
When one kidney is removed and a constrictor is placed on the renal artery of the remaining kidney, then within few minutes arterial pressure begins to rise and continues to rise for several days. The hypertension produced in this way is called one kidney Goldblatt's hypertension. The early rise in blood pressure is due to renin-angiotensin vasoconstrictor mechanism. The second rise is caused by fluid retention.
What is two kidney Goldblatt's hypertension?
Hypertension that develops when the artery to one kidney is constricted while artery to the other kidney is still normal, is called two kidney Goldblatt's hypertension.
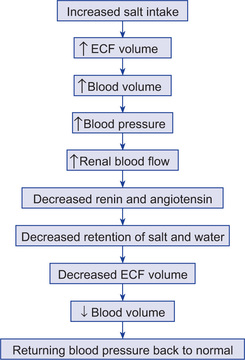
Hypertension
What is neurogenic hypertension?
Acute hypertension which is caused by strong stimulation of sympathetic nerves (due to excessive anxiety) is called neurogenic hypertension. Repeated acute episodes can lead to prolonged renal type of hypertension because of sympathetic neurotransmitter directly affecting renal arteries leading to their permanent damage.
What are the lethal effects of hypertension?
Hypertension if left untreated can cause following lethal effects:
What is the treatment of essential hypertension?
There are many antihypertensive drugs. The common drugs are:
• Which decrease the activity of sympathetic nervous system, e.g. beta blockers.
• Which decrease tubular absorption of salt and water, e.g. diuretics.
• Which block the action of renin-angiotensin, e.g. angiotensin converting enzyme inhibitors.
• Drugs paralyzing the smooth muscle of renal vasculature, e.g. calcium channel blockers.
Cardiac output
What is cardiac output? How much is it normally?
Cardiac output is the quantity of blood pumped into the aorta each minute by the heart. It is 5 litres in normal adult person.
What is cardiac index? How much is it normally?
Cardiac index is the cardiac output per square metre of body surface area. It is 3 litres in normal adult person weighing 70 kg.
What is stroke volume?
Stroke volume is the volume of blood pumped by each ventricle per heart beat.
What is venous return?
The quantity of blood flowing from the veins into the right atrium each minute is known as venous return.
What is Frank-Starling law of the heart?
Frank-Starling's law refers to the relationship between venous return (venous pressure) and cardiac output. An increase in venous return causes greater filling of ventricle during diastole resulting in a greater stretch on the cardiac muscle fibres. This produces a stronger contraction and a greater ejection of blood during systole. Stretch on the SA node also increases the rate of the heart. Stretched right atrium also initiates Bainbridge reflex (passing to vasomotor centre) causing increased heart rate. Thus an increased venous return produces increased cardiac output within physiological limits (Frank-Starling law). Therefore, venous return is the most important factor controlling cardiac output.
What is the effect of local blood flow regulation on cardiac output?
The venous return to the heart is the sum of all the local blood flows from individual segments of the peripheral circulation. Cardiac output regulation therefore is a sum of all the local blood flow regulations and is therefore determined by all the factors that control local blood flow throughout the body. Cardiac output varies reciprocally to the changes in total peripheral resistance, when arterial blood pressure is maintained normal, i.e.

How much amount of blood can normal heart pump without any excess nervous stimulation?
Normal heart can increase the cardiac output with increased venous return (Frank-Starling law) up to about two and half times its normal. Venous return is limiting factor. So normal heart without any excess nervous stimulation has the cardiac output up to 13 l/min.
What is hypoeffective heart? Enumerate the factors causing hypoeffective heart
When the pumping ability of the heart is below the normal, the heart is said to be hypoeffective heart.
What is hypereffective heart? Enumerate the factors that cause hyper-effective heart
When the pumping ability of the heart is greater than normal, the heart is said to be hypereffective heart (Fig. 13.12).
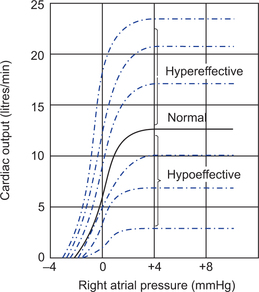
Factors causing hypereffective heart:
1. Nervous stimulation. When there is sympathetic stimulation of the heart, there is greatly increased heart rate and also increase in the strength of contraction of the heart. Because of these two effects, cardiac output may be increased up to 25 l/min.
2. Hypertrophy of the heart. Increase in mass and contractility of cardiac muscle is termed hypertrophy of the heart, e.g. heavy exercise.
When above two effects are combined, cardiac output becomes as much as 30 to 35 l/min.
What is the effect of sympathetic stimulation on cardiac output?
Sympathetic stimulation increases the cardiac output as follows:
Describe the methods for measuring cardiac output
Cardiac output can be measured by following methods:
1. With the help of flowmeter. In animals, aorta and pulmonary artery or a great vein entering the heart is cannulated and other end of cannula is connected to a flowmeter of any type to record the cardiac output. Electromagnetic or ultrasonic flowmeter can be placed on the aorta or pulmonary artery to measure the cardiac output.
2. Fick method of measuring output. O2 consumption per minute is determined— say it is 200 ml. O2 concentration of blood entering the heart on right side collected from right ventricle by cardiac catheterization. O2 concentration of blood leaving the left side of the heart (blood collected from any peripheral artery) are determined. From the above data one can find the amount of O2 carried by 1 litre of blood. Since total quantity of O2 consumed is known, cardiac output can be calculated as follows:
Concentration of O2 in arterial blood = 200 ml/L
Concentration of O2 in venous blood = 160 ml/L
Therefore, arteriovenous difference in O2 concentration is 40 ml. This means that one litre of blood picks up 40 ml of oxygen from the lungs. Therefore for picking up 200 ml of O2, 5 L of blood would be required. So 5 L is the cardiac output.

3. Indicator dilution method. Small amount of indicator dye is injected in the large vein (5 mg of cardio green dye is injected). Dye passes from veins to right side of the heart, then to lungs and back to the left side of the heart and then to the arterial system. Concentration of the dye is recorded as it passes through the arterial system. None of the dye passes to arterial system for first 3 seconds after the injection, but later the arterial concentration of the dye increases and reaches maximum at the end of 6 to 7 seconds. Then the concentration of the dye falls rapidly but before reaching a zero point, some dye gets recirculated through the heart and concentration starts rising. To calculate mean concentration of dye in the artery, the down stroke of the graph is extrapolated to zero point (Fig. 13.13). Then area under entire curve is measured and the average concentration for the duration of time curve is determined. After this cardiac output is calculated as follows:
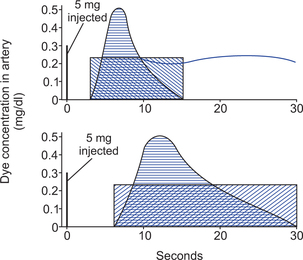
Fig. 13.13 Dilution method: Dye concentration curves used to calculate two separate cardiac output levels.

4. Thermal dilution method. Small quantity of cold saline is rapidly injected through a catheter inserted into a peripheral vein and advanced to the right atrium. The quantity of thermal indicator delivered to the blood is derived from the volume of injectate and its temperature is recorded by a fast response thermistor placed in the lumen of the catheter near the injection orifice. The resultant change in blood temperature is measured by a second thermistor bead mounted in the end of a cardiac catheter advanced from peripheral vein through right heart into the pulmonary artery. The shape and time course of the change in pulmonary artery blood temperature is almost similar to that of the dye concentration curve, following dye injection. Cardiac output is determined by the following formula:
Shock
What is circulatory shock?
Circulatory shock means generalized inadequacy of blood flow throughout the body to the extent that body tissues get damaged due to too little delivery of oxygen and nutrients.
Explain different types of shock and their causes
1. Shock caused by reduced cardiac output
(a) Cardiogenic shock, due to decreased pumping ability of the heart because of cardiac abnormalities, e.g. myocardial infarction, toxic states of heart, severe heart valve dysfunction, heart arrhythmias.
(b) Shock caused by decreased venous return:
• Hypovolumic shock. There is decrease in blood volume due to any cause, e.g. external or internal haemorrhage (injury, fracture), fluid loss (diarrhoea, vomiting, excess sweating, burns).
• Decrease in vascular tone, especially of venous reservoirs as in
– Neurogenic shock, caused by general or spinal anaesthesia, brain damage, emotional fainting.
– Anaphylactic shock, an allergic reaction which causes marked venous and arteriolar dilatation and increased capillary permeability due to release of histamine or histamine like substances.
– Obstructive shock, caused by obstructive blood flow, e.g. tension pneu-mothorax, pulmonary embolism, cardiac tumour, etc.
2. Shock occurring without decrease in cardiac output
(a) Excessive metabolism of the body due to which normal cardiac output is inadequate.
(b) Septic shock. Abnormal tissue perfusion patterns so that most of the cardiac output is passing through blood vessels besides those that are supplying the local tissues with nutrition. It occurs due to blood borne infection, e.g. peritonitis. Usually there is high fever, vasodilation, high cardiac output and sludging of blood in septic shock.
What are signs and symptoms of circulatory shock?
• Tachycardia and therefore reduced stroke volume.
• Reduction in velocity of blood flow producing stagnant hypoxia and cyanosis.
• Pale and cold skin due to vasoconstriction.
• Decreased urine output due to reduced renal blood flow and GFR.
• Blood flow to vital organs is affected. Reduced blood flow to brain causes fainting.
• Due to tachycardia there is increase in work of heart but its blood flow is reduced. This leads to excessive production and collection of lactic acid.
Name different stages of circulatory shock
Stages of shock
1. Non-progressive stage (compensated stages). Normal circulatory compensatory mechanisms eventually cause full recovery without help of outside therapy.
2. Progressive stage. Shock becomes steadily worse until death.
3. Irreversible stage. Shock progresses to such an extent that all forms of known therapy are inadequate to save person's life.
Explain different compensatory mechanisms occurring in hypovolumic shock
In hypovolumic shock there is reduction in blood volume most commonly due to haemorrhage. The degree of shock depends on the amount of blood loss. About 10% of total loss of blood has no effect either on blood pressure or cardiac output. If loss is more cardiac output is reduced and later on blood pressure decreases.
Circulatory system can recover if degree of loss is not greater than a certain critical amount. Crossing this critical amount causes death as shock itself causes more shock resulting into progressive shock.
If shock is not severe enough to cause its own progression, person recovers. Shock of this lesser degree is non-progressive shock. Circulatory system recovers due to various negative feedback control mechanisms set for maintaining cardiac output and blood pressure. They are termed compensatory mechanisms. These are:
Rapid compensatory mechanisms
1. Baroreceptor reflex. Fall in blood pressure causes lesser degree of stretching of barore-ceptors. Discharge from these receptors stimulates vasomotor centre and there is sympathetic stimulation leading to generalized vasoconstriction (sparing vessels of brain and heart). Vasoconstriction is most marked in skin, kidneys and viscera. This causes shifting of greater amount of blood in circulation. Constriction of veins on account of sympathetic stimulation also causes increased shifting of stored venous blood in circulation leading to increased venous return and cardiac output. In kidneys both afferent and afferent blood vessels constrict but afferent vessels constrict to a greater extent. This leads to reduction in GFR.
2. Chemoreceptor reflex. Haemorrhage causes loss of red cells leading to reduced O2 carrying capacity. The resultant anaemia and stagnant hypoxia as well as acidosis stimulates chemoreceptors which also excite vasomotor centre to cause same effects as those caused by baroreceptor reflex. Fall in blood pressure below 80 mmHg usually initiates chemoreceptor reflex.
3. CNS ischaemic response. When blood pressure falls below 50 mmHg this response is initiated. It causes more powerful sympathetic stimulation.
4. Reverse stress relaxation. This causes blood vessels to constrict down around the diminished blood volume so that available blood volume is adequately circulated.
5. Release of epinephrine and norepinephrine. Haemorrhage is a potent stimulator of secretion of these hormones from adrenal medulla. The increase in blood levels of these hormones contribute relatively little to generalized vasoconstriction. They cause stimulation of reticular formation making patient restless and apprehensive.
6. Increase in circulating angiotensin II level. Due to ischaemia there is a secretion of renin from the kidneys which increases level of angiotensin II in blood.
7. Thirst centre is stimulated which makes person drink more fluid which helps to restore extracellular fluid (ECF).
Increased angiotensin II causes vasoconstriction leading to rise in blood pressure. It also causes increased aldosterone secretion (after about 30 minutes) which in turn causes increased absorption of salt and water by kidneys which helps in restoring extracellular fluid volume. All these effects help in preventing progression of shock.
8. Release of excess vasopressin or ADH. Release of ADH causes retention of water by kidneys and helps in restoring ECF.
9. Capillary fluid shift mechanism. Drop in capillary pressure causes fluid from interstitial space to move into the capillaries along most of their course helping to maintain circulatory volume.
From different mechanisms described above reflexes provide immediate help within 30 seconds of haemorrhage. Angiotensin, vasopressin, reverse stress relaxation require 10 minutes to an hour for complete response. Readjustment of blood volume by increased absorption of water from intestine and increased absorption of salt and water from kidneys require 1 to 48 hours. Recovery takes place if shock does not become progressive.
Long-term compensatory mechanisms
1. Restoration of plasma volume and proteins. After a moderate haemorrhage plasma volume is restored to normal in 12 to 72 hours. There is rapid entry of preformed albumin from extravascular stores. After this initial influx albumin and rest of the plasma protein losses are restored by hepatic synthesis over a period of 3 to 4 days.
2. Restoration of red cell mass. There is excess release of erythropoietin which leads to increased rate of erythropoiesis within 10 days. Normal red cells mass is restored in 4 to 8 weeks.
What is progressive shock?
When shock becomes severe enough structures of circulatory system begin to deteriorate and various types of positive feedback mechanisms develop. These cause vicious cycle of progressively decreasing cardiac output. This is called progressive shock.
What is irreversible shock?
After shock has progressed to a certain stage, transfusion or any other therapy becomes incapable of saving the life of a person. This is irreversible shock.
What is the treatment of circulatory shock?
The treatment of shock is aimed at correcting the cause and helping physiological compensatory mechanisms.
Regulation of blood flow through skeletal muscle
How is the blood flow through the skeletal muscles regulated?
During the periods of rest, the rate of blood flow to skeletal muscles is 3 to 4 ml/100 g of muscle.
At this time only 20 to 25% of muscle capillaries have flowing blood. During exercise when there are rhythmic contractions of the muscles, all dormant capillaries open up, greatly increasing the surface area and the rate of blood flow to the skeletal muscles. There is rhythmic increase in blood flow between the contractions.
Strong tetanic contraction of the muscle causes compression of blood vessels and even total stoppage of blood supply. Increase in blood supply during activity (exercise) is due to local regulation and also due to nervous control.
Local regulation. Due to exercise, muscles use oxygen very rapidly. This in turn decreases local oxygen concentration leading to vasodilatation. Many vasodilator substances (e.g. adenosine ions, acetylcholine, lactic acid) are also released which cause vasodilatation.
Nervous control. Skeletal muscles are supplied by sympathetic vasoconstrictor fibres and sympathetic vasodilator fibres.
Sympathetic vasoconstrictor nerves. These nerves release noradrenaline on stimulation and cause vasoconstriction and reduced blood flow to muscles. In addition nore-pinephrine secreted by adrenal medulla also passes into circulating blood to cause vasoconstriction. Adrenaline secreted by adrenal medulla acts on beta receptors of the vessels and causes vasodilatation.
Sympathetic vasodilator fibres. In cat and other lower animals, there are sympathetic vasodilator fibres which secrete acetylcholine at their endings, which in turn causes vasodilatation. Such fibres are not yet been proved in human beings (but adrenaline acting on beta receptors of the vessels causes vasodilatation).
Heart rate
How much is normal heart rate and how is it regulated?
Normal heart rate varies between 72 and 80 beats/min.
Regulation of heart rate
Heart rate is adjusted according to the metabolic needs of the body, e.g. it increases during exercise and decreases during sleep so that optimum blood is supplied to the tissues.
Two factors mainly regulate the heart rate as follows:
1. Local mechanism. Any factor which affects SA node or junctional tissue affects the rhythmicity and also the heart rate.
2. Nervous mechanism. There is cardioinhibitory centre connected with vagus and cardioexcitatory centre connected with sympathetic nerves. Vagus exerts a tonic inhibitory control over the heart which is referred to as vagal tone. In addition vagus is reflexly stimulated through the sinoaortic mechanism. Stimulation of vagus causes decrease in the heart rate, whereas stimulation of sympathetic causes increase in the heart rate.
Cardiac centres, i.e. cardioinhibitory and cardioacceleratory centres are in reciprocal relation, i.e. stimulation of one depresses the other and vice versa. These cardiac centres are influenced either directly or reflexly.
1. Excitement quickens the heart rate and sudden shock lowers the heart rate. These changes are due to impulses coming to centres from the cerebral cortex and the hypothalamus.
2. Heart rate is also influenced reflexly by cardioinhibitory and cardiostimulatory reflexes and reflexes from other parts of the body.
• Sinoaortic reflex. When blood pressure rises, baroreceptors are stretched and sensory impulses from them increase the vagal tone, so that heart rate falls.
• Cardioacceleratory reflexes. Venous engorgement of the right atrium and the great veins reflexly increases the heart rate. This is known as Bainbridge reflex. Afferent impulses from engorged veins and right atrium pass via afferent nerves to cardiac centre to cause increase in the heart rate. This occurs during muscular exercise (due to increased venous return).
• Reflexes from other parts of the body.
– Hypoxia. Hypoxia stimulates the respiratory centre reflexly through the chemoreceptors. It also stimulates cardiac centre to cause increase in heart rate. Therefore, rapid pulse in heart failure, anaemia, haemorrhage, high altitude, CO poisoning is due to this mechanism.
– CO2 excess. It has a direct as well as reflex effect in causing stimulation of the heart rate.
– Body temperature. Increase in body temperature increases the heart rate by direct action on SA node as well as by stimulating cardioacceleratory centre.
– Increased intracranial pressure. It directly stimulates the vagus and lowers the rate.
– Adrenaline. It directly stimulates the heart rate but reflexly inhibits it (adrenaline increases the blood pressure and therefore by sinoaortic reflex mechanism reduces the heart rate).
– Thyroxine. Thyroxine increases the heart rate by stimulating metabolic rate of SA node, increasing BMR of the body and by stimulating the sympathetic.
– Exercise. It increases the heart rate by causing increased venous return, Bain-bridge reflex, sympathetic stimulation, CO2 excess, etc.
Circulation time
What is circulation time? How is it determined?
Circulation time
Time taken for particle in the blood to flow from one point in circulation to the other is known as circulation time. It measures average linear velocity of blood.
Methods of determination
Some substance is injected intravenously and time taken for arrival of that substance at the point of question is determined. The substances used are histamine, fluorescein, potassium ferrocyanide, calcium chloride, radioactive substances, etc.
• Method employed. Repeated estimation with same method should be done. Time is measured with the help of the stop watch. Each substance has a characteristic effect on arriving at a specific point, e.g. ether has smell, decholine causes bitter taste.
Factors affecting circulation time are:
Normal values of some circulation times:
• Arm to tongue. 5 ml of 2% decholine is injected into the cubital vein. As soon as drug reaches the tongue, patient feels a bitter taste. The total time taken from arm to tongue is 13 seconds.
• Arm to lungs. Found with the help of ether. It is 6 seconds.
• Arm to face. Found with histamine which causes flushing of face. Time is 24 seconds.
Cardiac failure
What is cardiac failure? What are its causes?
Failure of the heart to pump enough blood to satisfy the needs of the body is called cardiac failure. It may be manifested in two ways:
What are acute and chronic effects of moderate heart failure?
Acute effects
When there is sudden damage to the heart as in myocardial infarction, pumping ability of the heart is immediately depressed. This causes reduction in cardiac output to as low as 2 l/min. It also causes damming of blood in the veins resulting into increased systemic venous pressure so that right atrial pressure rises to 4 mmHg. This low cardiac output still sustains life but is associated with fainting.
When cardiac output becomes low, different circulatory reflexes are activated within 30 seconds, e.g. baroreceptor reflex, chemoreceptor reflex, CNS ischaemic response, reflexes originating in heart. Due to these reflexes, there is strong sympathetic stimulation within few seconds which causes direct effect on the heart. If musculature of the heart is diffusely damaged but still functional, it strengthens the musculature. Or if the part of the muscle has become non-functional, normal muscle is stimulated and compensates for non-functional muscle. Thus heart becomes a stronger pump. Sympathetic stimulation also causes increased tone in the blood vessels, especially the veins. This results into increased venous return. This, in turn, increases the pumping ability of the heart increasing cardiac output to about 4.2 l/min adequate to sustain life.
Chronic effects
After the few minutes of acute attack, a prolonged secondary state begins which causes:
(a) retention of fluid by the kidneys, and (b) progressive recovery of the heart.
• Retention of fluid by the kidneys. Decreased cardiac output decreases the urine output and therefore causes retention of fluid and increase in blood volume. When it is moderate, it helps in compensating the diminished pumping ability of the heart. It increases mean systemic filling pressure causing flow of blood towards the heart. Secondly it distends the veins, reduces the venous resistance and increases the flow of blood towards the heart.
If cardiac pumping ability is greatly reduced (less than 25 to 50% of normal) then blood flow to kidneys is greatly reduced and there is low urinary output. Also there is retention of excess fluid but it has no beneficial effect on circulation as heart is already pumping at its maximal ability. This leads to development of oedema which is detrimental.
• Progressive recovery of the heart. Heart gradually recovers because of new collateral blood supply and hypertrophy of undamaged musculature. This is achieved ordinarily within 5 to 7 weeks.
Thus there is compensation for the damage (compensated heart failure) and person has normal resting cardiac output but if he performs heavy exercise, pumping ability of the heart cannot be increased to a desired level and symptoms of acute failure may return, i.e. cardiac reserve is reduced in compensated heart failure.
What is the effect of severe heart damage?
If heart is severely damaged, sympathetic reflexes, fluid retention are not useful in causing weakened heart to pump a normal output. Therefore, cardiac output can never rise enough. Fluid continues to be retained and person develops more and more oedema progressively eventually leading to death. This is called decompensated heart failure. This is treated by: (i) strengthening the heart by giving cardiotonic drugs, and (ii) by administering diuretic drugs.
What is left heart failure? When does it occur?
In large number of patients with acute failure, left sided failure predominates over right sided failure leading to unilateral left sided failure. Very rarely there is unilateral right sided failure. When there is predominant left heart failure, right heart pumps normal quantity of blood to the lungs but blood is not pumped out of lungs into the systemic circulation because of left sided failure. This causes increased volume of blood to be retained in the lungs, increased pulmonary capillary pressure (pulmonary vascular congestion) and pulmonary oedema.
What is high output cardiac failure? When does it occur?
When person's cardiac output is much higher than normal, and he has signs of heart failure (high right and left atrial pressures, oedema), it is called ‘high output failure’. This is due to over beating of heart with increased venous return and not due to decreased pumping ability of the heart.
This is caused due to circulatory abnormality that drastically decreases the total peripheral resistance.
What is low output cardiac failure?
In many cases of acute heart attacks, there is slow progressive cardiac deterioration and heart becomes incapable of pumping adequate blood flow to keep the body alive. All body tissues suffer and begin to deteriorate, ultimately leading to death, within few hours or few days. This type of circulatory shock is called cardiogenic shock or cardiac shock or power failure syndrome. Patient dies of cardiogenic shock before compensatory processes can return cardiac output to normal.
Coronary circulation
Describe the anatomy of coronary blood supply
The heart receives its nutrient supply through left and right coronary arteries. Only inner 75 to 100 μm of endocardial surface can obtain significant amounts of nutrients from the blood present in heart chambers.
Left coronary artery mainly supplies the anterior and lateral portions of the left ventricle. Right coronary artery mainly supplies most of the right ventricle as well as posterior part of the left ventricle in most of the persons. In about 20% of people, left artery predominates and in 30% both arteries provide nutrients equally. In 50% of people, right coronary artery predominates.
Most of the venous blood from the left ventricles is collected by way of coronary sinus (it is 75% of total coronary flow) and the venous blood from the right ventricle is collected through anterior cardiac veins directly into the right atrium. A small amount of blood is collected through Thebesian veins which directly open into all the chambers of the heart (Fig. 13.14).
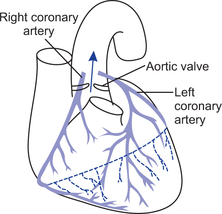
How much is the resting coronary blood flow?
Resting coronary blood is 225 ml/min or 0.7 or 0.8 ml/g of heart muscle, i.e. 4 to 5% of the total cardiac output.
Describe the phasic changes in coronary blood flow
During the phases of cardiac cycle there are changes in coronary blood flow. During systole, blood flow in the left ventricle falls to a low value. This is due to compression of intramuscular vessels during systole. During diastole, the blood through coronary capillaries rapidly rises, because there is relaxation of ventricular muscle and therefore there is no longer obstruction to the blood flow.
Blood passing through coronary capillaries of right ventricle also show similar phasic changes. They are far less because force of contraction of the right ventricle is much less (Fig. 13.15).
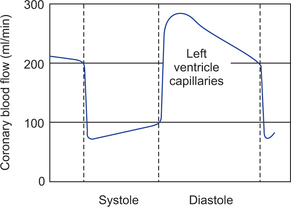
Describe the arrangement of coronary vessels in different layers of the heart
On the surface of the cardiac muscle there are large epicardial arteries. From them smaller intramuscular arteries penetrate the muscle. They give rise to nutrient arteries in their way to supply muscle. Immediately beneath the endocardium, there is a plexus of subendocardial arteries. During systole when the left ventricle contracts forcefully, blood flow through subendocardial plexus almost falls to zero. To compensate for this, subendocardial arterial plexus is more extensive than the nutrient arteries in the middle and outer layers of the heart. Therefore, during diastole, flow through the subendo-cardial arteries is considerably greater.
How is the coronary blood flow controlled?
Coronary blood flow is controlled as follows:
1. Local blood flow regulation. It is most important factor which regulates coronary blood flow. Under the resting state, 70% of O2 is removed by the heart muscles as the blood passes through arteries. Therefore, not much additional oxygen can be provided unless the blood flow increases. Increased oxygen consumption by the heart increases the blood flow proportionately. Yet exact mechanism by which this is done is not certain. Probably decreased oxygen consumption causes release of vasodilator substances such as adenosine (due to increased degradation of adenosine triphosphate) from the muscle cells. This adenosine causes vasodilatation and then reabsorbed back into the cardiac cells to be reused. Hydrogen ions, bradykinin, CO2, prostaglandins are the other suggested vasodilator substances.
According to other theory, O2 lack directly causes vasodilatation because muscles of the vessel wall itself get deficient oxygen. This causes muscle wall relaxation and vasodilatation.
2. Nervous control. Autonomic nerves control the blood flow directly as well as indirectly. Normally indirect effects are opposite to direct effect but play important role in control of blood flow.
• Direct effect. Distribution of parasympathetic nerve fibres (through vagus) to coronary system is so less that parasympathetic stimulation has very slight direct effect, causing dilatation of coronary arteries.
Sympathetic nerve fibres extensively innervate the coronary vessels. The transmitters released at their endings are epinephrine and norepinephrine. Norepinephrine acts on alpha receptors and causes vasoconstriction. Epicardial vessels have preponderance of alpha receptors. Epinephrine acts on beta receptors of coronary vessels causing vasodilatation. Intramuscular arteries have preponderance of beta receptors. But overall effect is vasoconstriction of the coronary vessels. Metabolic local factors are more important in controlling blood flow, therefore they over-ride the effect of nervous stimulation.
• Indirect effect. Sympathetic stimulation releases norepinephrine and epinephrine which increase the heart rate, force of contraction of heart and rate of metabolism of heart. Increased metabolism of heart causes relative lack of O2 supply and sets off the local blood flow regularity mechanisms for dilating the coronary vessels thus increasing the blood flow in proportion to metabolic needs of heart muscle.
Parasympathetic stimulation releases acetylcholine which causes decrease in heart rate and force of contraction of heart. These effects decrease O2 consumption of heart and indirectly cause constriction of coronary arteries and decrease in blood flow.
What does cardiac muscle use for its metabolism normally?
Under the resting condition, cardiac muscle uses mainly fatty acids for its energy, rather than carbohydrate. But under anaerobic or ischaemic conditions, glucose is utilized through anaerobic glycolysis.
How is coronary blood flow measured?
The most common method used for measuring coronary blood flow is nitrous oxide method. This is based on Fick principle. It gives almost accurate value.
Procedure
Person inhales a mixture of 15% nitrous oxide and air for 10 minutes. The amount of nitrous oxide taken in per minute is determined.
During inhalation of the gas several blood samples are taken from an artery and through a catheter introduced into the mouth of coronary sinus (collection of mixed venous blood) at intervals. The nitrous oxide content of each of the blood sample is determined. Arteriovenous difference in nitrous oxide is calculated. Then coronary blood flow is determined by following formula:

Enumerate the factors affecting coronary blood flow
Factors affecting coronary blood flow are:
1. Mean aortic pressure. This is the force for driving blood into the coronary arteries. Rise in mean aortic pressure increases the blood flow and vice versa. But if pressure remains high for a long time, because of increased work load on the heart, heart will go into congestive cardiac failure.
2. Cardiac output. Greater the cardiac output, greater is the coronary blood flow.
3. Metabolic factors. Increased metabolism of the heart increases O2 consumption leading to relative hypoxia. This hypoxia causes dilatation of vessels and increase in blood flow (blood flow also increases due to release of adenosine).
4. Effect of ions. K+ ions in low concentration causes dilatation of coronary vessels whereas high K+ ion concentration causes constriction of the coronary vessels.
5. Nervous stimulation. Already explained.
6. Hormones. Thyroid hormone increases coronary blood flow because of increase in metabolism.
Adrenaline and noradrenaline cause increase in blood flow as already explained.
7. Exercise. During exercise, coronary blood flow increases because of sympathetic stimulation.
What is ischaemic heart disease?
Ischaemic heart disease is the disease resulting from insufficient coronary blood flow. The most common cause of decreased coronary blood flow is atherosclerosis. Coronary vessel occlusion may occur due to thrombus formation of the atherosclerotic plaque, embolus coming from other areas or coronary vessel spasm due to irritation of smooth muscle.
Describe the collateral circulation in the heart
In the heart there is almost no communication existing among larger coronary arteries, but many anastomoses do exist among the smaller arteries (20 to 250 u.m diameter). They open up within few seconds after the sudden occlusion of larger artery. The blood flowing through them is only one-half that needed to keep cardiac muscle alive. But collateral blood flow begins to increase and become double by the end of second or third day and reaches to normal by one month. When atherosclerosis causes constriction of coronary arteries slowly over a period of many years, collateral vessels develop at the same time and therefore patient never experiences acute episode of cardiac dysfunction.
What is myocardial infarction?
Immediately after an acute coronary occlusion, the area of muscle that has either zero flow or very little flow that cannot sustain the cardiac muscle function, is said to be infarcted. The overall process is known as myocardial infarction.
Subendocardial muscle normally has difficulty in obtaining adequate blood flow as blood vessels are intensely compressed during systole of the heart. Subendocardial muscle frequently becomes infarcted without any evidence of infarction in the outer portions.
What are the causes of death following acute coronary occlusion?
There are four major causes of death following acute myocardial infarction as follows:
1. Cardiac shock. The heart becomes incapable of contracting with sufficient force to pump enough blood in the arterial tree. This is called coronary shock or cardiac shock or low cardiac output failure.
2. Damming of blood in venous system. When heart is not properly pumping the blood forward, it causes damming of blood in blood vessels of lungs or in the systemic circulation. This increases right and left atrial pressures, increased capillary pressure. The cause of death is acute pulmonary oedema.
3. Rupture of infarcted area. Few days after the infarction, dead cardiac muscle begins to degenerate, becomes thin and ruptures leading to loss of blood in pericardial cavity (cardiac tamponade), compression of heart from outside, blood cannot return to right atrium. This leads to sudden decreased cardiac output and death.
4. Ventricular fibrillation. In this condition coordinated, effective contraction of ventricles is lost. At any given instant many small portions of ventricular muscle will be contracting, at the same time, equally as many other portions are relaxing. Thus there is never a coordinate contraction of the entire ventricular muscle at once. This leads to failure of a ventricle as a pump leading to negligible amount of stroke volume. It is a very serious condition because if ventricular fibrillation begins within 4 to 5 seconds there is a lack of blood flow to the brain. Unless ventricular fibrillation is treated instantly it is almost invariably fatal. Main factors which can initiate ventricular fibrillation are sudden electric shock or ischaemia of the heart.
What is angina pectoris?
Development of cardiac pain whenever the load on the heart becomes too great in relation to coronary blood flow is called angina pectoris. Therefore, patient gets pain on exertion. Pain is hot, pressing and constricting type. It is treated by giving vasodilator drugs. Most commonly used vasodilators are nitroglycerin and other nitrate drugs.
What is the surgical treatment for coronary disease?
Following surgical procedures are done for treating coronary disease:
1. Aortic coronary bypass. Small vein grafts are anastomosed from the aorta to the side of the more peripheral coronary vessels. Each graft supplies a peripheral coronary artery beyond a block. The vein that is usually used is a long saphenous vein.
2. Coronary angioplasty. This is done to open partially blocked coronary vessel (before they become totally occluded) by passing small balloon-tipped catheter under radiographic guidance into the coronary system.
Cerebral circulation
Describe anatomy of cerebral circulation
Blood enters the cranium through two internal carotid and two vertebral arteries. Two vertebral arteries combine to form a basilar artery which in turn divides into two posterior cerebral arteries.
Each internal carotid artery divides into middle and anterior cerebral arteries. These six arteries (anterior, middle and posterior cerebral arteries on two sides) intercommunicate with the help of their branches forming circle of Willis. These three vessels supply different parts of brain.
Brain has a very rich blood supply. Grey matter has a greater supply than the white matter. Cerebral arteries are not end arteries. They freely anastomose especially at the circle of Willis. Because of this, blood flows adequately to different parts of brain, especially during the time of emergency. Venous blood drains into large cerebral sinuses (superior sagittal, inferior sagittal, cavernous). All sinuses ultimately form two transverse sinuses which become continuous with the two internal jugular veins.
How is cerebral blood flow measured?
Cerebral blood flow is measured by nitrous oxide method based on Fick principle.
Procedure
Person inhales 15% nitrous oxide. Blood samples are collected from any peripheral artery and from the jugular vein at frequent intervals, while the subject is inhaling the mixture of nitrous oxide and air. Nitrous oxide content of each sample is determined. Cerebral blood flow per minute is determined from the arteriovenous difference of nitrous oxide and the partition co-efficient for N2O between the blood and the brain.
What is average blood flow to the brain?
Under-resting state, 54 ml of blood is supplied per 100 g of brain tissue per minute or 770 ml/min. Total O2 consumption by brain is 50 ml/min.
How is cerebral circulation regulated?
Cerebral blood flow is autoregulated. Various factors help in this autoregulation as follows:
• Arterial CO2 tension. Increase in CO2 tension in the arterial blood increases the blood flow by causing dilatation of arterioles (Fig. 13.16).
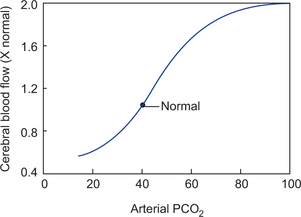
• Hypoxia. Decreased O2 supply to the brain also causes vasodilatation. This is due to lack of O2 supply to smooth muscle of the vessel (causing smooth muscle to relax and cause vasodilatation). Lack of O2 also causes release of certain vasodilator substances which cause direct effect on the vessel wall causing vasodilatation. The most important of it is adenine.
Cerebral blood flow depends upon the difference between mean arterial pressure and internal jugular pressure because the difference between these two pressures is the driving force for cerebral circulation. Greater the driving force, greater is the blood flow. Cerebral blood flow is maintained therefore by maintaining general blood pressure through sinoaortic mechanism.
Cerebral blood flow is inversely related to cerebrovascular resistance which in turn depends on:
Pulmonary circulation
What is the minute blood flow in pulmonary circulation?
The right ventricular output flows to pulmonary circulation. It is about 5 l/min.
What is the systolic and diastolic pressure in pulmonary circulation?
Pulmonary circulation is a low pressure circulation. Pressure in the pulmonary artery during systole is about 25 mmHg and during diastole it is about 10 mmHg. Pulmonary capillary pressure is about 8 mmHg.
What are the functions of pulmonary circulation?
2. Pulmonary blood vessels act as filters. They trap emboli which pass through pulmonary circulation.
3. Pulmonary circulation maintains nutrition to the lung tissue.
4. Left ventricular output is dependent on return of blood from pulmonary circulation to the left atrium.
5. Conversion of angiotensin I to angiotensin II by angiotensin converting enzyme.
What are the peculiarities of pulmonary circulation?
1. At the arterial end of capillaries, fluid filters out in tissues through the capillary endothelium. But from pulmonary capillaries no fluid passes into the tissues. This is because in pulmonary capillary blood colloidal osmotic pressure (25 mmHg) is much higher than the hydrostatic pressure of blood in capillaries.
2. Pulmonary capillaries filter emboli and prevent them reaching and blocking the blood vessels of important organs such as heart and brain.
3. Pulmonary vascular bed is a low resistance circuit. Vessels are short and distensible and therefore can accommodate large quantity of blood.
4. Local action of CO2 and low O2 on pulmonary vascular bed is opposite to that at systemic vessels. Excess CO2 and low O2 causes vasoconstriction.
Model Questions
Long Questions
1. Describe how normal arterial blood pressure is maintained.
2. Describe the normal electrocardiogram. How is it recorded? What is the physiological significance of its reflections?
3. Describe the pressure and volume changes occurring in the left ventricle during the cardiac cycle.
4. Describe the sequence of events in a cardiac cycle.
5. Define cardiac output. What are the factors affecting it? Describe any one method for its measurement in man.
6. Describe in detail the production and propagation of cardiac impulse.
7. Describe the regulation of heart rate.
8. Describe the physiology of coronary circulation.
9. What is shock? Explain different causes, symptoms, signs and treatment of shock.