Thoracic Wall and Mechanism of Respiration
The thoracic wall is formed posteriorly by the thoracic part of the vertebral column, anteriorly by the sternum and costal cartilages, and laterally by the ribs and the intercostal spaces. The floor of thorax is formed by the diaphragm and its roof is formed by suprapleural membranes. The diseases of thoracic viscera are the leading cause of death all over the world. Therefore, surface landmarks of the thorax are extremely important to the physicians in providing reference locations for performing inspection (visual observation), palpation (feeling with firm pressure), percussion (detecting densities through tapping), and auscultation (listening sounds with the stethoscope).
SURFACE LANDMARKS
BONY LANDMARKS
The bony landmarks of the thoracic wall are as follows (Fig. 16.1):

1. Suprasternal notch (jugular notch): It is felt just above the superior border of the manubrium sterni between the proximal medial ends of the two clavicles. It lies at the level of lower border of the body of T2 vertebra. The trachea can be palpated in this notch.
2. Sternal angle (angle of Louis): It is felt as a transverse ridge about 5 cm below the suprasternal notch. It marks the angle made between the manubrium and the body of the sternum (the angle between the long axis of manubrium and body of sternum is 163° posteriorly and 17° anteriorly). It lies at the level of intervertebral disc between the T4 and T5 vertebrae. The 2nd rib articulates on the either side with the sternum at this level. Hence it used as surface landmark for counting the ribs (for details see ![]() Page 198).
Page 198).
3. Xiphisternal joint: It can be felt at the apex infrasternal/subcostal angle formed by the meeting of anterior end of subcostal margins. The xiphisternal joint lies at the level of the upper border of the body of T9 vertebra.
4. Costal margin: It forms the lower boundary of the thorax on each side and is formed by the cartilages of the 7th, 8th, 9th, and 10th ribs and the free ends of 11th and 12th ribs. The lowest point of costal margin is formed by the 10th rib and lies at the level of L3 vertebra.
5. Subcostal angle: It is situated at the inferior end of the sternum between the sternal attachments of the 7th costal cartilage.
6. Thoracic vertebral spines: The first prominent spine felt at the lower end of nuchal furrow (midline furrow on the back of neck) is the spine of C7 vertebra (vertebra prominens). All the thoracic spines are counted below this level. For reference, the 3rd thoracic spine lies at the level of root of spine of scapula and 7th thoracic spine lies at the level of inferior angle of the scapula.
SOFT TISSUE LANDMARKS
1. Nipple: In males, the nipple is usually located in the 4th intercostal space about 4 in (10 cm) from the midsternal line. In females, its position varies considerably.
2. Apex beat of the heart: It is lowermost and outermost thrust of cardiac pulsation, which is felt in the left 5th intercostal space 3.5 in (9 cm) from the midsternal line or just medial to the midclavicular line.
LINES OF ORIENTATION (Fig. 16.1)
The following imaginary lines are often used to describe surface locations on the anterior and posterior chest wall.
1. Midsternal line: It runs vertically downwards in the median plane on the anterior aspect of the sternum.
2. Midclavicular line: It runs vertically downwards from the midpoint of the clavicle to the midinguinal point. It crosses the tip of the 9th costal cartilage.
3. Anterior axillary line: It runs vertically downwards from the anterior axillary fold.
4. Midaxillary line: It runs vertically downwards from the point in the axilla located between the anterior and posterior axillary folds.
5. Posterior axillary line: It runs vertically downwards from the posterior axillary fold.
6. Scapular line: It runs vertically downwards on the posterior aspect of the chest passing through the inferior angle of the scapula with arms at the sides of the body.
COVERINGS OF THE THORACIC WALL
The thoracic wall is covered from superficial to deep by:
Skin: The skin covering thoracic wall is thin on its anterior aspect and thick on its back aspect. The distribution of hair is variable and depends on the age, sex, and race.
Cutaneous nerves: The cutaneous innervation on the front of thorax is provided by cutaneous branches of anterior primary rami of thoracic spinal nerves (T2–T6) in sequence from above downwards by the T2 at the level of 2nd rib to the T6 at the level of xiphoid process. The skin above the level of 2nd rib is supplied by the anterior primary ramus of C4 via supraclavicular nerves.
• The anterior rami of C5–T1 innervate the skin of the upper limb.
• The cutaneous innervation on the back of thorax (on either side of midline for about 5 cm) is provided by posterior rami of thoracic spinal nerves.
Superficial fascia: The superficial fascia is more dense on the posterior aspect of the chest to sustain the pressure of the body when lying in the supine position. The superficial fascia on the front of the chest contains breast (mammary gland), which is rudimentary in males and well-developed in adult females. The breast is described in detail in ![]() Chapter 3.
Chapter 3.
Deep fascia: The deep fascia is thin and ill-defined (except in pectoral region) to allow free movement of the thoracic wall during breathing.
Muscles: The thoracic wall is liberally covered by the following extrinsic muscles:
2. Muscles of abdomen: Rectus abdominis and external oblique covers the lower part of the front of thoracic wall.
• The thoracic wall is more or less completely covered by extrinsic muscles except in the anterior and posterior median lines.
• On the back, the thoracic wall is thinly covered by musculature in the region of triangle of auscultation (see ![]() Page 62).
Page 62).
INTRINSIC MUSCLES (Figs 16.2–16.4)
The intrinsic muscles of the thoracic wall are arranged in three layers from superficial to deep. These are as follows (16.2A):
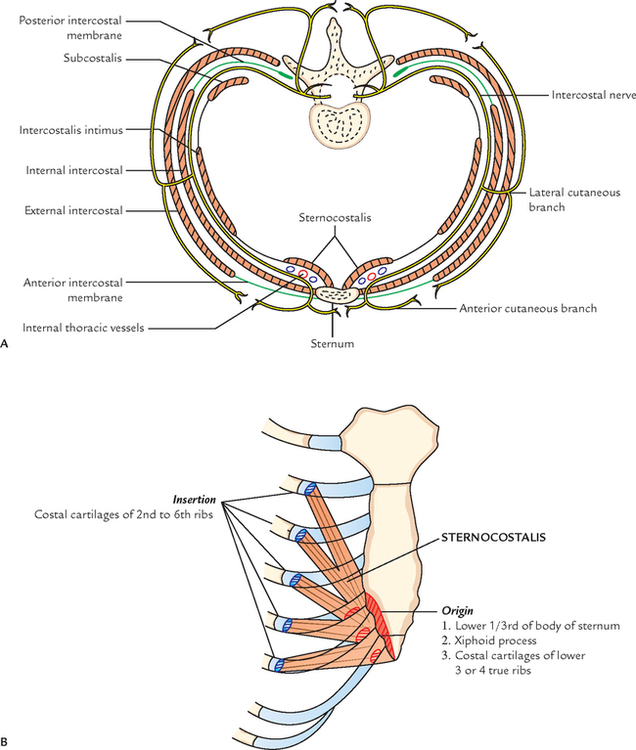

1. External intercostal muscle (superficial layer).
The muscle layer is lined by the endothoracic fascia, which in turn is lined by the parietal pleura.
These three layers of muscles are comparable to the three layers of muscles in the abdominal wall.
The intercostal nerve and vessels form neurovascular bundle lie between the intermediate and deep layer (neurovascular plane).
N.B. In addition to the above-mentioned three intrinsic muscles there is another set of muscles called levatores costarum.
External Intercostal Muscle (11 Pairs)
Extent: Each muscle extends in the intercostal space from tubercle of the rib behind to the costochondral junction in front, where it is replaced by anterior intercostal membrane.
Origin and insertion: It arises from the lower border of the rib above and inserted into the outer lip of the upper border of rib below.
Direction of fibres: The fibres of the external intercostal muscle are directed downwards, forwards, and medially (in the posterior part however, the fibres are directed downwards and laterally).
Nerve supply: By intercostal nerve of the same space.
Actions: The external intercostal muscles elevate the ribs during inspiration.
Internal Intercostal Muscle (11 Pairs)
Extent: Each muscle extends in the intercostal space from the lateral border of sternum in front to the angle of rib behind, where it is replaced by the posterior intercostal membrane.
Origin and insertion: It arises from the floor of the costal groove of the upper rib and inserts into the inner lip of the upper border of the rib below.
Direction of fibres: Its fibres are directed upwards, forwards, and medially (i.e., at right angle to those of external intercostal muscle).
Nerve supply: By intercostal nerve of the same space.
Actions: The internal intercostal muscles elevate the ribs during expiration.
Transversus Thoracis Muscle
The transversus thoracis muscle is divided into the following three parts:
Intercostalis intimus (11 pairs)
Extent: It occupies the middle two-fourth of the intercostal space.
Origin and insertion: It arises from the inner surface of the rib above and inserts on to the inner surface of the rib below.
Direction of fibres: It is same as those of internal intercostal muscles.
Nerve supply: By intercostal nerve of the same space.
Actions: The intercostal intimi muscles elevate the ribs during expiration.
Subcostalis (total number variable)
The subcostalis muscle lies in the same plane as the intercostalis intimus in the posterior part of the intercostal space. It intervenes between the intercostal nerve and vessels, and pleura.
Origin and insertion: It arises from the inner surface of rib near the angle and inserts on the inner surface of the 2nd or 3rd rib below.
Direction of fibres: It is same as that of the internal intercostal muscle.
Sternocostalis (Fig. 16.2B)
The sternocostalis muscle one on either side is situated on the inner aspect of front of the chest wall (behind the sternum and costal cartilages) occupying the anterior part of the upper intercostal spaces, except the first space. The sternocostalis muscle intervenes between the anterior end of the intercostal nerves and the pleura.
Origin: It arises from (a) lower one-third of the posterior surface of the body of sternum, (b) posterior surface of the xiphoid process of the sternum, and (c) posterior surface of the costal cartilages of lower three or four ribs.
Insertion: The fibres diverge upwards and laterally as slips to be inserted into the lower border and inner surfaces of the costal cartilages of 2nd–6th ribs.
Nerve supply: By intercostal nerves.
Action: It draws down the costal cartilages in which it is inserted.
Levatores Costarum (12 Pairs)
These are a series of 12 small muscles placed on either side of the back of thorax, just lateral to the vertebral column.
Origin: It arises from the tip of transverse process from 7th to 11th thoracic vertebrae.
Insertion: Each muscle passes obliquely downwards and laterally to be inserted on to the upper edge and outer surface of the rib immediately below in the interval between the tubercle and angle.
Actions
1. Elevate and rotate the neck of rib in a forward direction.
2. Are rotators and lateral flexors of the vertebral column?
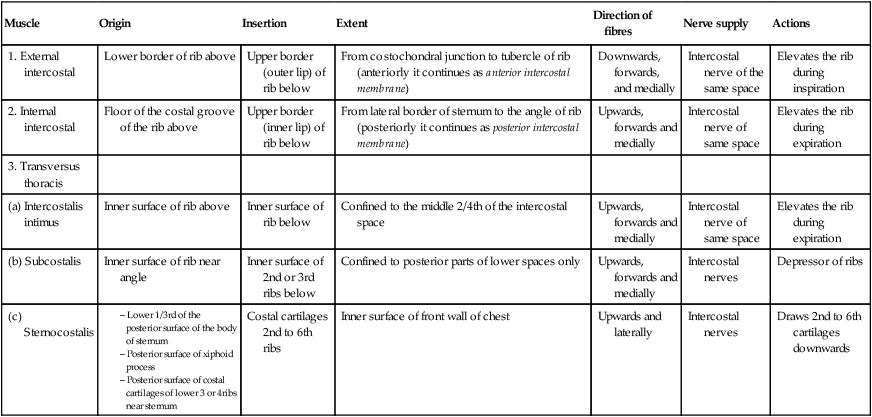
The origin insertion, extent, direction of fibres, nerve supply, and actions are given in Table 16.1.
Table 16.1
Intrinsic muscles of the thoracic wall
| Muscle | Origin | Insertion | Extent | Direction of fibres | Nerve supply | Actions |
| 1. External intercostal | Lower border of rib above | Upper border (outer lip) of rib below | From costochondral junction to tubercle of rib (anteriorly it continues as anterior intercostal membrane) | Downwards, forwards, and medially | Intercostal nerve of the same space | Elevates the rib during inspiration |
| 2. Internal intercostal | Floor of the costal groove of the rib above | Upper border (inner lip) of rib below | From lateral border of sternum to the angle of rib (posteriorly it continues as posterior intercostal membrane) | Upwards, forwards and medially | Intercostal nerve of same space | Elevates the rib during expiration |
| 3. Transversus thoracis | ||||||
| (a) Intercostalis intimus | Inner surface of rib above | Inner surface of rib below | Confined to the middle 2/4th of the intercostal space | Upwards, forwards and medially | Intercostal nerve of same space | Elevates the rib during expiration |
| (b) Subcostalis | Inner surface of rib near angle | Inner surface of 2nd or 3rd ribs below | Confined to posterior parts of lower spaces only | Upwards, forwards and medially | Intercostal nerves | Depressor of ribs |
| (c) Sternocostalis | Costal cartilages 2nd to 6th ribs | Inner surface of front wall of chest | Upwards and laterally | Intercostal nerves | Draws 2nd to 6th cartilages downwards |
INTERCOSTAL SPACES
The spaces between the two adjacent ribs (and their costal cartilages) are known as intercostal spaces. Thus there are 11 intercostal spaces on either side.
The 3rd–6th spaces are typical intercostal spaces because the blood and nerve supply of 3rd–6th intercostal spaces is confined only to thorax.
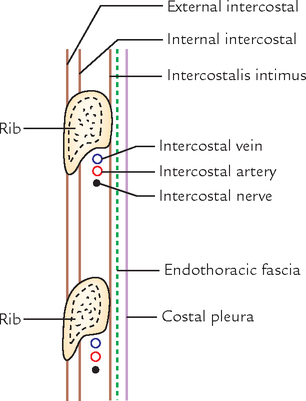
CONTENTS OF A TYPICAL INTERCOSTAL SPACE
Each space contains the following structures (Fig. 16.4):
N.B. Plane of neurovascular bundle in the intercostal space: The neurovascular bundle consisting of intercostal nerve and vessels lies between the internal intercostal and innermost intercostal muscles, i.e., between the intermediate and deepest layers of muscles.
They are arranged in the following order from above downwards:
INTERCOSTAL MUSCLES
Intercostal muscles are a group of muscles that are present in the intercostal space and help form and move the chest wall.
The following muscles constitute intercostal muscles:
N.B. Strictly speaking, the intercostalis intimi is not present in the intercostal space as it lies on the deeper aspects of the ribs.
Nerve supply: By intercostal nerves.
Actions
The actions of intercostal muscles are as follows:
1. They act as strong supports for the rib preventing their separation.
2. They act as elevators of the ribs during respiration. External intercostal muscles act during inspiration, while others act during expiration.
The intercostal muscles are described in detail on Page 213–214.
INTERCOSTAL NERVES
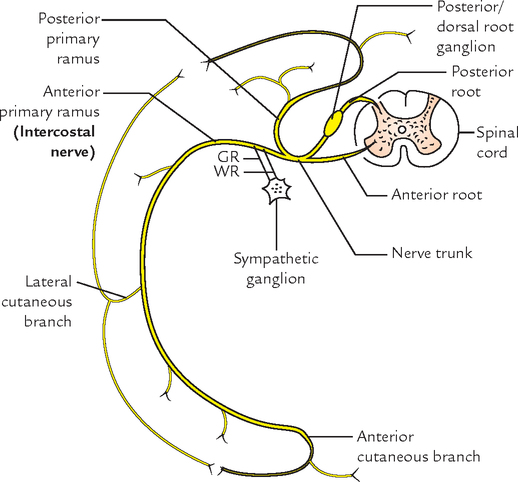
The 12 pairs of thoracic spinal nerves supply the thoracic wall. As soon as they leave, the intervertebral foramina they divide into anterior and posterior rami (Fig. 16.5).
The anterior primary rami of upper 11 thoracic spinal nerves (T1–T11) are called intercostal nerves as they course through the intercostal spaces. The anterior primary ramus of the 12th thoracic spinal nerve runs in the abdominal wall below the 12th rib, hence it is called subcostal nerve.
N.B. Unique features: The intercostal nerves are anterior primary rami of thoracic spinal nerves. They are segmental in character unlike the anterior primary rami from other regions of spinal cord which form nerve plexuses viz. cervical, brachial, lumbar and sacral.
Classification
The intercostal nerves are classified into the following two groups:
1. Typical intercostal nerves (3rd, 4th, 5th, and 6th).
2. Atypical intercostal nerves (1st, 2nd, 7th, 8th, 9th, 10th, and 11th).
The typical intercostal nerves are those which remain confined to their own intercostal spaces.
The atypical spinal nerves extend beyond the thoracic wall and partly or entirely supply the other regions.
TYPICAL INTERCOSTAL NERVE
Course and Relations
The typical intercostal nerve after its origin turns laterally behind the sympathetic trunk, and then enters the intercostal space between the parietal pleura and posterior intercostal membrane. It then enters the costal groove of the corresponding rib to course laterally and forwards.
In costal groove it comes into relation with corresponding intercostal vessels and forms neurovascular bundle of the intercostal space.
In the intercostal space, vein, artery and nerve lie in that order from above downwards.
Near the sternal end of the intercostal space, the intercostal nerve crosses in front of the internal thoracic artery. Then it pierces internal intercostal muscle, anterior intercostal membrane, and pectoralis major muscle to terminate as anterior cutaneous nerve.
• In the posterior part of intercostal space, the intercostal nerve lies between the pleura and posterior intercostal membrane.
• In the remaining greater part of intercostal space, it lies between the internal intercostal and intercostalis intimus muscles.
Branches
1. Rami communicantes: Each nerve communicates with the corresponding thoracic ganglion by white and grey rami communicantes.
2. Muscular branches: These are small tender branches from the nerve, which supply intercostal muscles and serratus posterior and superior.
3. Collateral branch: It arises in the posterior part of the intercostal space near the angle of the rib and runs in the lower part of the space along the upper border of the rib below in the same neurovascular plane. It supplies intercostal muscles, parietal pleura, and periosteum of the rib.
4. Lateral cutaneous branch: It arises in the posterior part of the intercostal space near the angle of the rib and accompanies the main nerve for some distance, then pierces the muscles of the lateral thoracic wall along the midaxillary line. It divides into anterior and posterior branches to supply the skin on the lateral thoracic wall.
5. Anterior cutaneous branch: It is the terminal branch of the nerve, which emerges on the side of the sternum. It divides into medial and lateral branches and supplies the skin on the front of the thoracic wall.
ATYPICAL INTERCOSTAL NERVES
The atypical intercostal nerves are as follows:
1. First intercostal nerve: The greater part of this nerve joins the ventral ramus C8 spinal nerve to form lower trunk of the brachial plexus. The remaining part of the nerve is very small and it lacks both lateral and anterior cutaneous branches.
2. Second intercostal nerve: Its lateral cutaneous branch is called intercostobrachial nerve. It courses across the axilla and joins the medial cutaneous branch of the arm. The intercostobrachial nerve supplies the skin of the floor of the axilla and upper part of the medial side of the arm. In coronary arterial disease, the cardiac pain is referred along this nerve to the medial side of the arm.
3. Seventh to eleventh intercostal nerves: These nerves leave the corresponding intercostal spaces to enter into the abdominal wall; hence they are called thoraco-abdominal nerves. These nerves supply intercostal muscles of the corresponding intercostal spaces. In addition they supply:
• Root pain/girdle pain: Irritation of intercostal nerves caused by the diseases of thoracic vertebrae produces severe pain which is referred around the trunk along the cutaneous distribution of the affected nerve. It is termed root pain or girdle pain.
• Sites of eruption of cold abscess on the body wall: Pus from the tuberculous thoracic vertebra/vertebrae (Pott’s disease) tends to track along the neurovascular plane of the space and may point at three sites of emergence of cutaneous branches of the thoracic spinal nerve, viz. (a) just lateral to the sternum, (b) in the midaxillary line, and (c) lateral to the erector spinae muscle (Fig. 16.6).

• Herpes zoster: In herpes zoster (shingles) involving the thoracic spinal ganglia, the cutaneous vesicles appear in the dermatomal area of distribution of intercostal nerve. It is an extremely painful condition.
• Intercostal nerve block is given to produce local anesthesia in one or more intercostal spaces by injecting the anesthetic agent around the nerve trunk near its origin, i.e., just lateral to the vertebra.
• Thoracotomy: The conventional thoracotomy (posterolateral) is performed along the 6th rib. The neurovascular bundle is protected from injury by lifting the periosteum of the rib.
• Considering the position of neurovascular bundle in the intercostal space, it is safe to insert the needle, a little above the upper border of the rib below.
INTERCOSTAL ARTERIES
The thoracic wall has rich blood supply. It is provided by the posterior and anterior intercostal arteries.
Each intercostal space contains one posterior and two anterior intercostal arteries (upper and lower).
POSTERIOR INTERCOSTAL ARTERIES (Fig. 16.7)
There are 11 pairs of intercostal arteries, one in each space. They supply the greater part of the intercostal spaces.
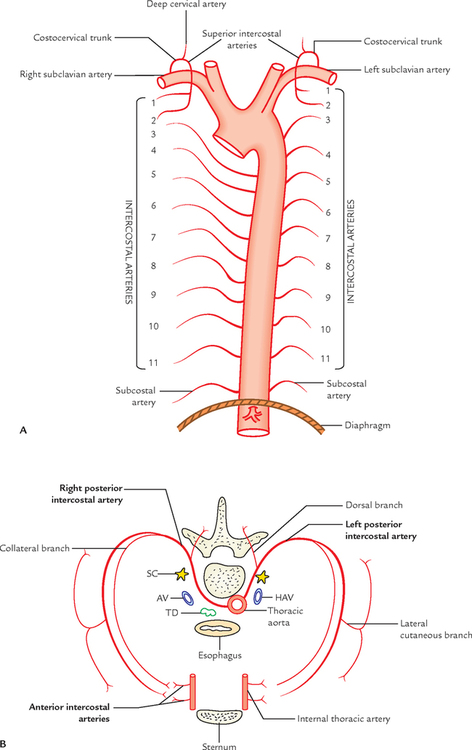
Origin
1. The 1st and 2nd posterior intercostal arteries are the branches of superior intercostal artery—a branch of the costocervical trunk.
2. The 3rd–11th posterior intercostal arteries arise directly from the descending thoracic aorta (Fig. 16.7A).
Course and Relations
In front of the vertebral column (Fig. 16.7B)
• The right posterior intercostal arteries are longer than the left because the descending aorta lies on the left side of the front of the vertebral column. They pass behind the esophagus, thoracic duct, azygos vein, and sympathetic chain but in front of the anterior aspect of vertebral body.
• The left posterior intercostal arteries are smaller and pass behind the hemiazygos vein and sympathetic chain, but in front of the side of the vertebral body
In the intercostal space, the posterior intercostal artery lies between the intercostal vein above and the intercostal nerve below. The neurovascular bundle in the intercostal space lies between the internal intercostal and intercostalis intimus muscles.
Branches
1. Dorsal branch: It supplies the spinal cord, vertebra and muscles, and skin of the back.
2. Collateral branch: It arises near the angle of the rib and runs forwards along the upper border of the rib below and ends by anastomosing with the lower anterior intercostal artery.
3. Muscular branches: They supply intercostal, pectoral, and serratus anterior muscles.
4. Lateral cutaneous branch: It closely follows the lateral cutaneous branch of the intercostal nerve.
5. Mammary branches (external mammary arteries): They arise from posterior intercostals arteries of the 2nd, 3rd, and 4th intercostal spaces and supply the breast mammary gland.
6. Right bronchial artery: It arises from right 3rd posterior intercostal artery.
INTERCOSTAL VEINS
The number of intercostal vein corresponds to the number of intercostal arteries, i.e., each intercostal space contains two anterior intercostal veins and one posterior intercostal vein. Their tributaries correspond to the branches of the arteries.
POSTERIOR INTERCOSTAL VEINS
1. They are present in all the spaces.
2. Each space contains only one posterior intercostal vein.
3. Each vein accompanies the posterior intercostal artery.
4. Its tributaries correspond to the branches of posterior intercostal artery.
Termination (Fig. 16.8)
The mode of drainage (termination) of posterior intercostal veins differs on the right and left sides (Table 16.2).
Table 16.2
Mode of termination of right and left posterior intercostal veins
| Right posterior intercostal veins | Left posterior intercostal veins |
| 1st (highest) drains into the right brachiocephalic vein | 1st (highest) drains into left brachiocephalic vein |
| 2nd, 3rd, and 4th join to form right superior intercostal vein, which in turn drains into the azygos vein | 2nd, 3rd, and 4th join to form left superior intercostal vein, which in turn drains into left brachiocephalic vein |
| 5th–11th drain into the azygos vein | |
| Subcostal vein drains into the azygos vein | Subcostal vein drains into the hemiazygos vein |


INTERCOSTAL LYMPH VESSELS AND LYMPH NODES
LYMPH VESSELS
1. The lymph vessels from the anterior parts of the spaces drain into anterior intercostal/internal mammary lymph nodes. The efferent from these nodes unite with those of tracheobronchial and brachiocephalic nodes to form the bronchomediastinal trunk, which drains into subclavian trunk on the right side and thoracic duct on the left side.
2. The lymph vessels from the posterior parts of the spaces drain into posterior intercostal nodes. The efferent from the posterior intercostal nodes of lower four spaces unite to form a slender lymph trunk, which descends and drain into the cysterna chyli. The efferent from posterior intercostal nodes of upper spaces drain into right lymphatic duct on the right side and thoracic duct on the left side.
INTERNAL THORACIC ARTERY (Fig. 16.9)
There are two internal thoracic arteries, right and left, situated deep to anterior chest wall, one on either side of sternum.
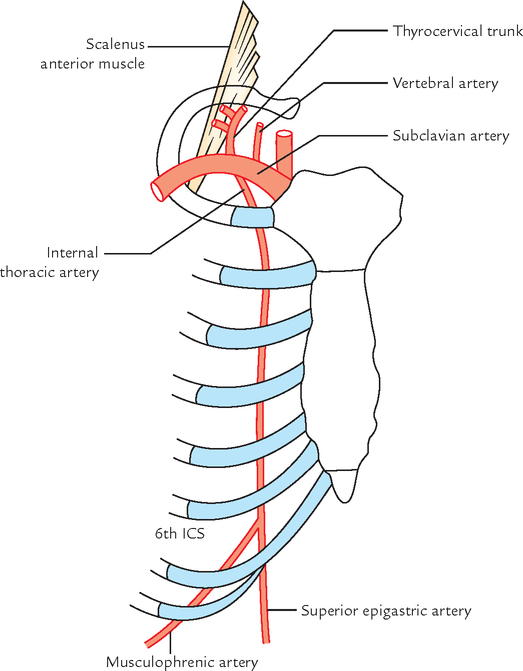
Course and Termination
The internal thoracic artery descends behind the medial end of the clavicle and upper six coastal cartilages, about 1 cm away from the lateral margin of the sternum. It ends in the 6th intercostal space by dividing into superior epigastric and musculophrenic arteries.
Relations
Anteriorly: From above downwards, it is related to:
• Above the 2nd costal cartilage, it is related to endothoracic fascia and pleura.
• Below the 2nd costal cartilage, it is related to sternocostalis muscle, which intervenes between the artery and the endothoracic fascia and pleura.
N.B. The internal mammary artery is accompanied by two venae comitantes, which unite at the level of 3rd costal cartilage to form the internal thoracic (mammary) vein, which runs upwards along the medial side of the artery to terminate into the brachiocephalic vein at the root of the neck.
Branches
1. Pericardiophrenic artery: It arises in the root of the neck above the 1st costal cartilage, and descends along with phrenic nerve to the diaphragm. It supplies pericardium and pleura.
2. Mediastinal branches: They are small inconstant twigs, which supply connective tissue, thymus, and front of the pericardium.
3. Anterior intercostal arteries: They are two for each of the upper six intercostal spaces.
4. Perforating branches: They accompany the anterior cutaneous branches of intercostal nerves. In females, the perforating branches of 2nd, 3rd, and 4th intercostal spaces are quite large and supply the breast.
5. Superior epigastric artery: It runs downwards behind the 7th costal cartilage between the sternal and 1st costal slips of diaphragm to enter the rectus sheath where it ends by anastomosing with the inferior epigastric artery. It supplies anterior body wall from clavicle to the umbilicus.
6. Musculophrenic artery: It runs downwards and laterally behind the 7th, 8th, and 9th costal cartilages, and gives two anterior intercostal arteries to each of the 7th, 8th, and 9th intercostal spaces. It pierces the diaphragm near the 9th costal cartilage, to reach under surface. It supplies diaphragm and muscles of the anterior abdominal wall.
MECHANISM OF RESPIRATION
The respiration consists of two alternate phases of (a) inspiration and (b) expiration, which are associated with alternate increase and decrease in the volume of thoracic cavity, respectively. During inspiration, the air is taken in (inhaled) and during expiration, the air is taken out (exhaled).
INSPIRATION
During inspiration the volume of thoracic cavity increases, which creates a negative intrathoracic pressure, consequently air is sucked into the lungs.
An increase in the capacity of thoracic cavity occurs vertically, anteroposteriorly, and transversely (i.e., side to side).
Vertical Diameter
Theoretically, the vertical diameter of the thoracic cavity can increase, if the roof of the thoracic cavity is raised or its floor lowered or both. The roof of thoracic cavity is formed by tough suprapleural membrane, which is fixed, hence cannot move up and down. However, the floor of thoracic cavity is formed by the freely movable diaphragm. Thus when the diaphragm contracts, its central tendon descends, and its domes are flattened. As a result, there is an increase in the vertical diameter of the thoracic cavity (Fig. 16.10).

Anteroposterior Diameter
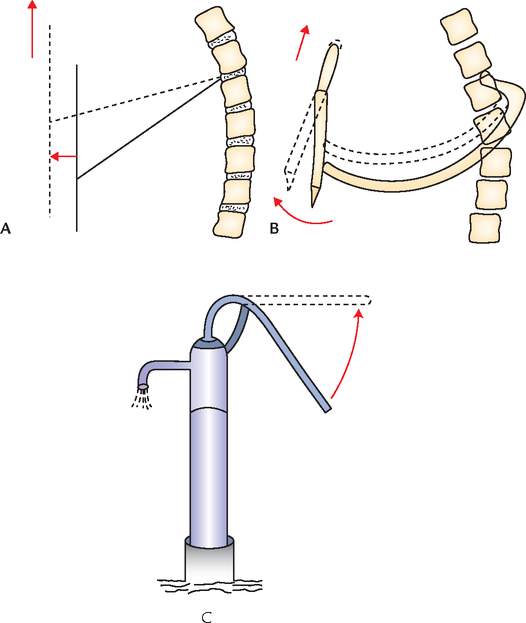
An increase in anteroposterior diameter of the thoracic cavity occurs when sternum moves forwards and upwards.
Each rib acts a lever, the fulcrum of which lies just lateral to the tubercle of the rib. Thus two arms of lever are greatly disproportional, e.g., posterior arm is very short and anterior arm is very long. Thus slight movement at the vertebral end of the rib is greatly magnified at the anterior end of the rib (Fig. 16.11).
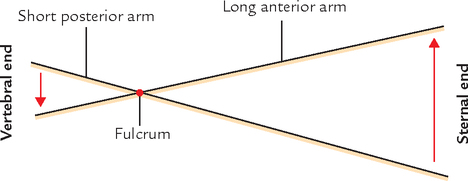
Since anterior ends of the ribs are at a lower level than their posterior ends, during elevation of the ribs, when their anterior ends move upwards and forwards, they carry with them the sternum. (This movement occurs mostly in vertebrosternal ribs.) Consequently, the anteroposterior diameter of the thoracic cavity is increased. This movement is termed pump-handle movement because sternum moves up and down like a handle of pump during respiration (Fig. 16.12).
Transverse Diameter
The middle of the shaft of the ribs lies at the lower level than the plane passing through its two ends (anterior and posterior; ![]() Fig. 15.3). This arrangement resembles a bucket handle. Therefore, during elevation of the ribs, the shafts of the ribs move outwards like the bucket handle—bucket handle movement. This causes increase in the transverse diameter of the thoracic cavity (Fig. 16.13). The axis of movement passes from the tubercle of this rib to the middle of the sternum.
Fig. 15.3). This arrangement resembles a bucket handle. Therefore, during elevation of the ribs, the shafts of the ribs move outwards like the bucket handle—bucket handle movement. This causes increase in the transverse diameter of the thoracic cavity (Fig. 16.13). The axis of movement passes from the tubercle of this rib to the middle of the sternum.
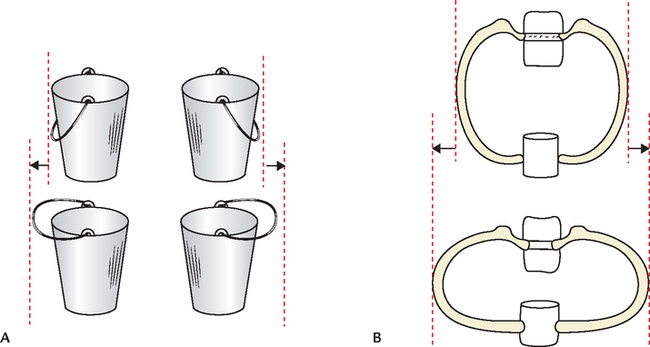
The bucket-handle movement is produced by vertebrochondral ribs.
The main factors responsible for increase in various diameters of the thoracic cavity are summarized in Table 16.3.
Table 16.3
Factors responsible for the increase in various diameters of the thoracic cavity during inspiration
| Diameter | Factors responsible for increase |
| Vertical | Descent (contraction) of the diaphragm |
| Anteroposterior | Pump-handle movement of the sternum (brought about by the elevation of vertebrosternal ribs |
| Transverse | Bucket-handle movement of the vertebrochondral ribs |
TYPES OF RESPIRATION (BREATHING)
The respiration is classified into the following three types:
In quiet respiration, the movements are normal as described above.
In deep respiration, movements described for quiet respiration are increased. The 1st rib is elevated by scalene and sternocleidomastoid muscles.
In forced respiration, all movements are exaggerated. The scapula is fixed and elevated by trapezius, levator scapulae, rhomboideus major, and rhomboideus minor muscles, so that pectoral muscles and serratus anterior can raise the ribs.
The muscles acting during different types of respiration (i.e., respiratory muscles) are enumerated in Table 16.4.
Table 16.4
Muscles acting during different types of respiration
| Type of respiration | Inspiration (elevation of ribs) | Expiration (depression of ribs) |
| Quiet respiration | ||
| Deep respiration | ||
| Forced respiration |

 Anterior primary rami of all the thoracic spinal nerves are intercostal nerves except Anterior primary rami of all the thoracic spinal nerves are intercostal nerves except |
Anterior primary ramus of T12 spinal nerve which is subcostal nerve |
| Main movement to increase the anteroposterior diameter of the thoracic cavity |
Pump-handle movement of sternum brought about by the elevation of vertebrosternal ribs (2nd-6th ribs) |
| Main movement to increase the transverse diameter of the thoracic cavity |
Bucket-handle movement of vertebrochondral ribs |
| Main factor responsible for increase of vertical diameter of the thoracic cavity |
Contraction of the diaphragm |
| Position of body in which diaphragm lies at the highest level |
Supine position |
| Position of body in which diaphragm lies at the lowest level |
Sitting position |
| Principal muscle of respiration |
Diaphragm |
| Muscle of weight lifting |
Diaphragm |


A 55-year-old patient came to the hospital with complaints of weakness, loss of weight, and pain on the back of chest. On examination, tenderness was noted on percussion, in the region of thoracic spine. Small bulges were also seen on the surface of the chest at three sites: (a) lateral to the sternum, (b) in the midaxillary line, and (c) lateral to the erector spinae muscle. The X-ray of thoracic spine revealed collapse of vertebral bodies of T5 and T6 vertebrae and a perispinal soft tissue shadow. He was diagnosed as a case of Pott’s disease.
2. What is the cause of perispinal soft tissue shadow?
3. Mention the anatomical basis of small bulges noted on the surface of the chest wall (vide supra).
1. Tuberculosis of spine (i.e., vertebrae).
3. The pus from the region of tubercular spine (cold abscess) tracks around the thoracic wall along the plane of neurovascular bundle and points on the surface of the chest at the sites of exit of cutaneous branches of the intercostal nerve, i.e., (a) lateral to the erect spinae muscle, (b) in the midaxillary line, and (c) just lateral to the sternum.