Synopsis of conservative dentistry
V Gopikrishna
“I keep six honest servingmen (they taught me all I knew); their names are What and Why and When and How and Where and Who...”
— Rudyard Kipling
Definition of conservative dentistry (operative dentistry)
According to Sturdevant, operative dentistry is the art and science of the diagnosis, treatment, and prognosis of defects of teeth that do not require full coverage restorations for correction. It involves the restoration of proper tooth form, function, and aesthetics, while maintaining the physiologic integrity of the teeth in harmonious relationship with the adjacent hard and soft tissues. This field of dentistry is also referred to as conservative dentistry.
Patients seek dental treatment for symptoms, such as pain, sensitivity, trauma, decay, bleeding gums, discolouration of teeth, and for aesthetic corrections. The management of most of these problems is under the purview of this branch of dentistry. Hence, operative dentistry/conservative dentistry forms the core of any dental practice.
Operative dentistry/conservative dentistry deals with:
Indications for conservative dentistry
Structure of teeth and supporting tissues
A tooth has a crown portion seen clinically in the oral cavity and a root portion embedded in a bony socket surrounded by the periodontium (Fig. 1.1).

Enamel
• It is the hardest substance of human body.
• It is a highly mineralized structure containing 95−98% inorganic matter, predominantly hydroxyapatite (Fig. 1.2).
• It is translucent in nature (Fig. 1.3).
• Enamel provides the external shape to the tooth and protects the underlying dentin and pulp.
• Enamel thickness varies from one set of tooth to another and is thicker at the incisal or occlusal areas and becomes progressively thinner, till it terminates at the cementoenamel junction (Fig. 1.4).


Dentin
• Dentin forms the largest portion of the tooth structure and is covered by enamel in the crown portion and cementum in the root portion (Fig. 1.5).
• Dentin is around 3.0−3.5 mm in thickness in the coronal aspect of the tooth.
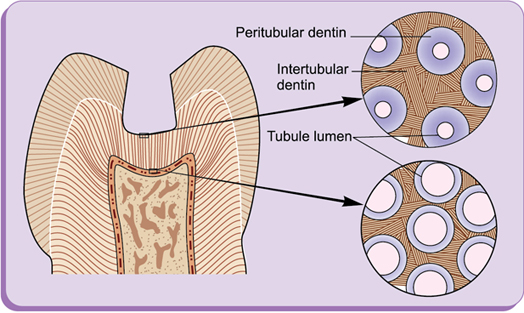
• Dentin consists of dentinal tubules which are lined by peritubular dentin and surrounded by intertubular dentin (Fig. 1.6).
• Dentinal tubules are present more in number towards the pulp and reduce in both number and diameter, as they approach the dentinoenamel junction (DEJ) (Fig. 1.7).


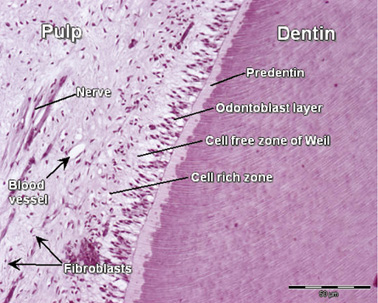
Pulp
Pulp is the vital soft connective tissue of the tooth consisting of collagen fibres, vital cells, blood vessels, and nerves. The pulp has four distinct zones (Fig. 1.8):
The pulp serves the following functions:
Periodontium
It is the connective tissue structure that attaches the teeth to the maxilla and mandible (Figs 1.9 and 1.10). It consists of:


Table 1.1
| Permanent dentition | Deciduous dentition |
| FIRST DIGIT | FIRST DIGIT |
| 1 → Maxillary right quadrant | 5 → Maxillary right quadrant |
| 2 → Maxillary left quadrant | 6 → Maxillary left quadrant |
| 3 → Mandibular left quadrant | 7 → Mandibular left quadrant |
| 4 → Mandibular right quadrant | 8 → Mandibular right quadrant |
| SECOND DIGIT | SECOND DIGIT |
| 1 → Central incisor | 1 → Central incisor |
| 2 → Lateral incisor | 2 → Lateral incisor |
| 3 → Canine | 3 → Canine |
| 4 → First premolar | 4 → First molar |
| 5 → Second premolar | 5 → Second molar |
| 6 → First molar | |
| 7 → Second molar | |
| 8 → Third molar |
Cementum
• Cementum is the hard tissue covering the radicular portion of the tooth (Fig. 1.11).
• It is more thicker near the apex and less near the neck of the tooth.
• Structurally, it consists of:
○ Acellular cementum → Presents in coronal half of the root and devoid of cells.
○ Cellular cementum → Predominately presents in apical half of the root and contains cementoblasts.
• Functions include protection of the radicular dentin and pulp, while attaching the tooth to the alveolar bone.

Dentition
Humans have two sets of teeth: Primary dentition and permanent dentition.
Primary dentition consists of 10 maxillary and 10 mandibular teeth. They are exfoliated and replaced by the permanent dentition, which consists of 16 maxillary and 16 mandibular teeth.
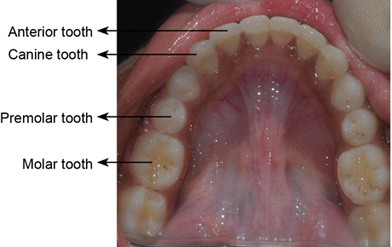
Human teeth are divided into classes on the basis of form and function. Primary dentition has three classes: incisors, canines, and molars. Permanent dentition includes a fourth class, the premolars.
Primary teeth
Permanent teeth
• The second set of teeth to erupt consists of a total of 32 teeth.
• They are also referred to as succedaneous teeth, as they succeed or replace the deciduous teeth.
• Maxilla and mandible each has (Fig. 1.12)
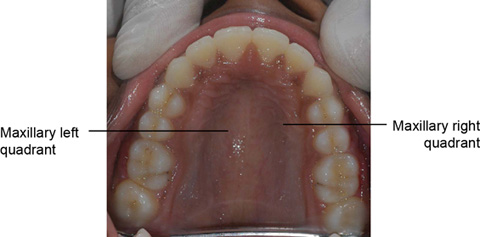
Dental arches and quadrants
• The human mouth has two dental arches, namely
• Upper/maxilla or lower/mandible has two quadrants—right and left (Fig. 1.13).
Classes of teeth
Incisors
Canines
Premolars
Molars
Anatomical landmarks
Anatomic crown: The portion of the tooth that extends from the cementoenamel junction or cervical line to the occlusal surface or incisal edge (Fig. 1.14a).

Clinical crown: The portion of the tooth that is visible in the oral cavity (Fig. 1.14a).
Cusp: A cusp is an elevation on the crown portion of a tooth making up a divisional part of the occlusal surface.
Ridge: A ridge is any linear elevation on the surface of a tooth and is named according to its location (e.g. buccal ridge, marginal ridge).
Marginal ridges (mesial and distal): These are stress-bearing ridges that border the mesial and distal margins of the occlusal surfaces of posterior teeth as well as the mesial and distal margins of the lingual surfaces of anterior teeth.
Triangular ridges: These are ridges that descend from the tips of the cusps of posterior teeth toward the central part of the occlusal surfaces.
Transverse ridge: It is a ridge formed by the union of a buccal and lingual triangular ridge.
Oblique ridge: It is a ridge that crosses obliquely the occlusal surfaces of maxillary molars and is formed by the union of the traingular ridge of the distobuccal cusp and distal cusp ridge of the mesiolingual cusp.
Fossa: It is an irregular depression or concave area in the enamel surface of a tooth.
Fissure: A developmental linear cleft is usually found at the base of a groove. It is commonly the result of the lack of fusion of the enamel of adjoining dental cusps or lobes (Fig. 1.14b).
Developmental groove: It is a shallow groove or line between the primary parts of a crown or root.
Pit: It is a small pinpoint depression in enamel, usually located in a groove and often at the junction of two or more fissures (Fig. 1.14b).
Tooth surfaces are named according to the anatomical structures it is closest to.
Mesial: Surface toward the midline of the arch.
Distal: Surface away from the midline.
Facial: Surfaces that are in the direction of the cheek or lips.
Lingual: Surface nearer to the tongue (in case of lower teeth).
Palatal: Surface nearer to the palate (upper teeth).
Occlusal: Biting or chewing surface, which contact opposing teeth in occlusion (in posterior teeth).
Incisal: Biting surface of anterior teeth.
Cervical/gingival: Surface nearer to the neck of the tooth or gingival margin.
Proximal: A surface that faces an adjacent tooth.
Interproximal contact: The surface that forms the contact between two adjacent teeth.
Contacts and contours
Knowledge about contacts and contours of various teeth is mandatory for understanding:
• The predisposal factors of proximal caries, like faulty interrelationships.
• Significance of marginal ridges, embrasures, for re-establishing form and function of the restored teeth.
• Periodontal aspect and health of the tooth to be restored.
Ideal contact and contour
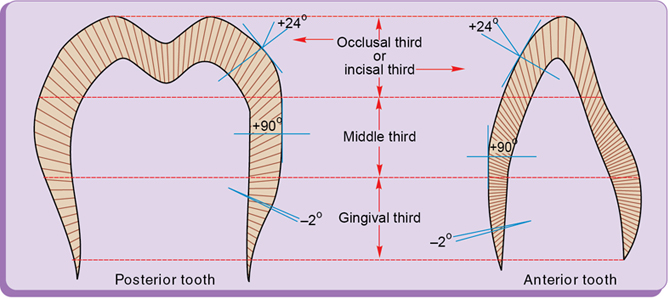
Height of contour
• The area of greatest circumference on the facial and lingual surfaces of the tooth is called height of contour (Fig. 1.15).
• It protects the gingival tissue by preventing food impaction.
• In the posterior teeth, the height of contour is located in the gingival third of the facial surface and in the middle one-third of the lingual surface.

Proximal contact area
Proximal contact area denotes the area of proximal height of contour of the mesial or distal surface of a tooth that touches (contacts) its adjacent tooth in the same arch.
Initially, after tooth eruption, there is only one point of contact known as proximal contact point, but due to wear during physiological tooth movement, the proximal contact point becomes proximal contact area.
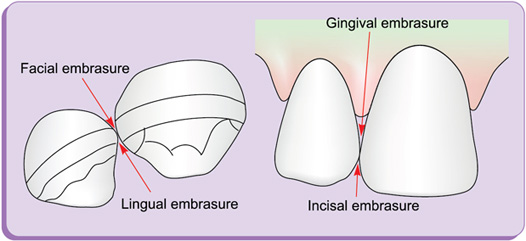
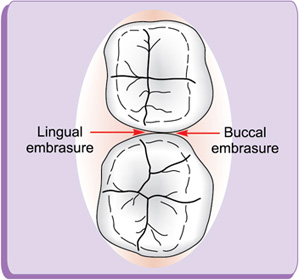
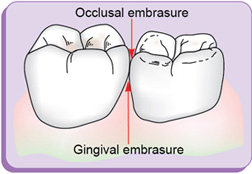
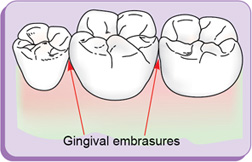
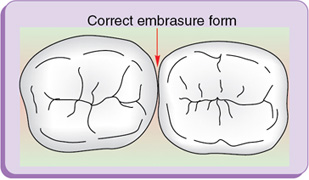
Embrasures (spillways) (fig. 1.16)
Embrasures are V-shaped spaces that originate at the proximal contact area between the adjacent teeth forming spillway spaces. They are named for the direction toward which they radiate. These embrasures are:
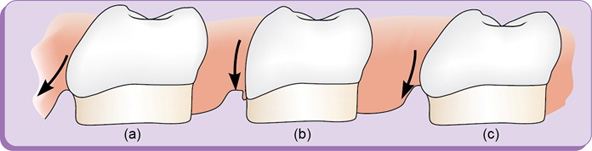
Normal contour and contact area of the teeth act in deflecting the food only to the extent that the passing food stimulates (by gentle massage) the underlying gingiva (Fig. 1.20).
Under and overcontouring during the restorative treatment has to be avoided as:
Clinical Note
Undercontouring of restorations (fig. 1.21)
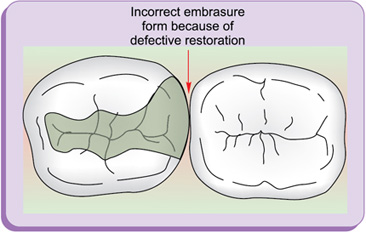
Overcontouring of restorations (fig. 1.22)

Figure 1.23 depicts importance of proper contour.
Occlusion
Occlusion is the relationship of cusps or masticating surfaces of maxillary and mandibular teeth.
Intercuspal position: The position of maximum intercuspation of the teeth.
Occlusal harmony: The absence of occlusal interferences, which allows mandibular movement in all excursions (with the teeth together), and does not result in discomfort, strain, or harm to the teeth or the masticatory apparatus (Fig. 1.24 a, b).

Nomenclature and tooth numbering system
Nomenclature is the scientific way of naming things. It helps in better understanding and communication (Fig. 1.25).

The following are the commonly used tooth notation systems employed by dentists to communicate and record data related to a particular tooth:
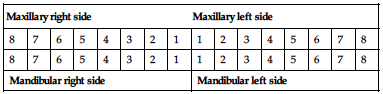
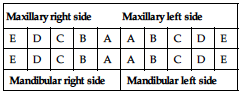
I. Zsigmondy—palmer notation system (fig. 1.26)
• Permanent teeth are denoted by numbers 1−8 with central incisor indicated as 1 and progresses on to the third molar which is designated as 8.
• Also called as angular or grid system.
• Deciduous teeth are denoted by upper case English alphabets A to E with A representing central incisor and E representing second molar.

Advantages
Simple to use
Disadvantages
Permanent teeth
| Maxillary right side | Maxillary left side | ||||||||||||||
| 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
| 8 | 7 | 6 | 5 | 4 | 3 | 2 | 1 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
| Mandibular right side | Mandibular left side | ||||||||||||||
Deciduous teeth
| Maxillary right side | Maxillary left side | ||||||||
| E | D | C | B | A | A | B | C | D | E |
| E | D | C | B | A | A | B | C | D | E |
| Mandibular right side | Mandibular left side | ||||||||
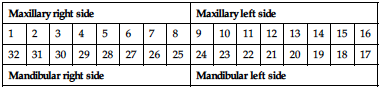
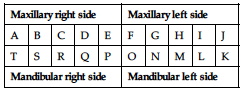
II. Universal notation system or american dental association (ADA) system (fig. 1.27)
• It is also known as Universal system.
• Numbering begins from maxillary right posterior most tooth, which is designated as 1 and proceeds to maxillary left posterior most tooth, which is designated as 16, then to mandibular left posterior tooth, which is designated as 17 and then proceeds to the mandibular right posterior most tooth, which is designated as 32.

Permanent teeth
| Maxillary right side | Maxillary left side | ||||||||||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 |
| 32 | 31 | 30 | 29 | 28 | 27 | 26 | 25 | 24 | 23 | 22 | 21 | 20 | 19 | 18 | 17 |
| Mandibular right side | Mandibular left side | ||||||||||||||
Deciduous teeth
| Maxillary right side | Maxillary left side | ||||||||
| A | B | C | D | E | F | G | H | I | J |
| T | S | R | Q | P | O | N | M | L | K |
| Mandibular right side | Mandibular left side | ||||||||
Advantage
Disadvantage
III. Federation dentaire international (FDI) system (fig. 1.28)
• Referred as two-digit system, where the two digits are used to identify an individual tooth.
• First digit represents the quadrant (1−4: permanent dentition) (5−8: deciduous dentition)

Advantages
Disadvantages
Permanent teeth
| Maxillary right side | Maxillary left side | ||||||||||||||
| 18 | 17 | 16 | 15 | 14 | 13 | 12 | 11 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 |
| 48 | 47 | 46 | 45 | 44 | 43 | 42 | 41 | 31 | 32 | 33 | 34 | 35 | 36 | 37 | 38 |
| Mandibular right side | Mandibular left side | ||||||||||||||
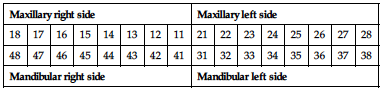
Deciduous teeth
| Maxillary right side | Maxillary left side | ||||||||
| 55 | 54 | 53 | 52 | 51 | 61 | 62 | 63 | 64 | 65 |
| 85 | 84 | 83 | 82 | 81 | 71 | 72 | 73 | 74 | 75 |
| Mandibular right side | Mandibular left side | ||||||||
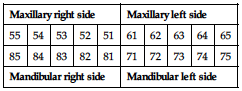
Figure 1.29 depicts both ADA universal and FDI nomenclature systems.

Causes of loss of tooth structure
The various causes of loss of tooth structure (Fig. 1.30) are provided in Box 1.1.

I. Dental caries
Definition
Dental caries is defined as a multifactorial, transmissible, and infectious oral disease caused primarily by the complex interaction of cariogenic oral flora (biofilm) with fermentable dietary carbohydrates on the tooth surface overtime.
• Dental caries is the most predominant cause of loss of tooth structure (Fig. 1.31).
• It is an irreversible microbial disease of the calcified tissues of the teeth characterized by demineralization of the inorganic portions and dissolution of the organic portion.
Factors causing dental caries (fig. 1.32)
Caries is a multifactorial disease and the most important factors are
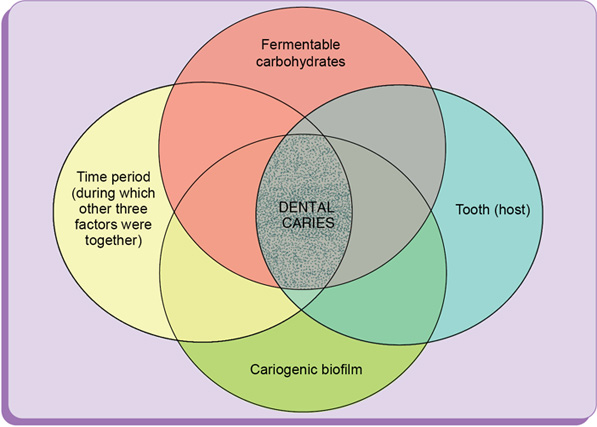
Pathophysiology of dental caries
Dental plaque or biofilm is a tenaceous film on the surface of teeth composed of bacteria, like Streptococcus sanguis and Streptococcus mutans. These bacteria present in plaque biofilm ferment a suitable dietary carbohydrate substrate to produce acid causing the plaque pH to fall. The critical pH for enamel and dentin is 5.5 and 6.2, respectively. Repeated fall in pH below the critical pH overtime may result in demineralization of a susceptible tooth structure. When the pH returns to neutral and when the concentration of Ca and P supersaturated minerals gets added back to partially demineralized enamel, remineralization starts. This demineralization–remineralization cycle is elaborated in Box 1.2. When the demineralization cycle overwhelms the ability of the host to remineralize, then dental caries manifests clinically.
The common terms used in this manual to define caries lesions is provided in Box 1.3.
Classification of dental caries (box 1.4)
I. According to location of caries
The characteristics of a caries lesion vary with the nature of the surface on which the lesion develops.
A. Primary caries
Primary caries is the original caries lesion of the tooth. Three morphologic types of primary caries are evident in clinical observation:
Lesions originating in enamel pits and fissures
Lesions originating on enamel smooth surfaces
Lesions originating on root surfaces.
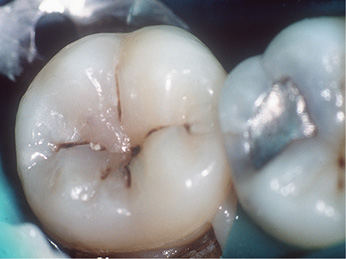
1. Pit-and-fissure caries
Pits and fissures are particularly susceptible surfaces for caries initiation (Fig. 1.33). The pits and fissures provide excellent mechanical shelter for organisms and harbour a community dominated by S. sanguis and other streptococci. The relative proportion of mutans streptococci (MS) most probably determines the cariogenic potential of the pit-and-fissure community.


2. Smooth surface caries
The proximal enamel surfaces immediately gingival to the contact area are the second most susceptible areas to caries.
Clinical Note
i. A rough surface (caused by caries, a poor-quality restoration or a structural defect) restricts adequate biofilm removal. This situation favours the occurrence of caries or periodontal disease at this site.
ii. Lesions starting on smooth enamel surfaces have a broad area of origin and a conical or pointed extension toward the DEJ (Fig. 1.34). A cross-section of the enamel portion of a smooth-surface lesion shows a V-shape, with a wide area of origin and the apex of the V directed towards the DEJ.

3. Root surface caries
The proximal, facial, or lingual root surface, particularly near the cementoenamel junction (CEJ), often is unaffected by the action of hygiene procedures, such as flossing, because it may have concave anatomic surface contours (fluting) and occasional roughness at the termination of the enamel. These conditions, when coupled with exposure to the oral environment (as a result of gingival recession), favour the formation of mature and cariogenic biofilm and proximal root surface caries (Fig. 1.35).

B. Secondary (recurrent) caries
Secondary caries occurs at the junction of a restoration and the tooth and may progress under the restoration. It is often termed recurrent caries. This condition usually indicates that microleakage is present, along with other conditions conducive to caries development.
II. According to direction of caries
A. Backward caries
When the spread of caries along the DEJ exceeds the caries in the contiguous enamel, caries extends into this enamel from the junction and is termed backward caries (Fig. 1.36).

B. Forward caries
Forward caries is said to be present, wherever the caries in enamel is larger or at least the same size as that in dentin (Fig. 1.36).
III: According to extent of caries
A. Incipient caries/white spot lesion (reversible)
Incipient caries or white spot lesion (WSL) is the first evidence of caries activity in enamel. On smooth surface enamel, the lesion appears opaque white when air-dried and seems to disappear when wet (Fig. 1.37).

B. Cavitated caries (irreversible)
In cavitated caries, the enamel surface is broken (not intact) and usually the lesion has advanced into dentin. Usually, remineralization is not possible and treatment that includes tooth preparation and restoration is indicated (Fig. 1.38).

IV. According to rate (speed) of caries
A. Acute (rampant) caries
Acute caries, often termed rampant caries, refers to disease that rapidly damages the tooth. It is usually in the form of numerous soft, lighter-coloured lesions in a mouth and is infectious (Fig. 1.39A).

B. Chronic (slow) or arrested caries
Chronic caries is slow or it may be arrested after several active phases. The slow rate results from periods, when demineralized tooth structure is almost remineralized (the disease is episodic overtime, because of changes in the oral environment). The condition may be found in only a few locations in a mouth and the lesion is discoloured and fairly hard (Fig. 1.39B).

V. According to the histological depth of penetration
A. Enamel caries
i. Non-cavitated enamel caries or incipient caries (white spot lesion)
The earliest evidence of caries on the smooth enamel surface of a clean, dry tooth is seen as a white spot. White spots are chalky white, opaque areas (Fig. 1.40) that are revealed only when the tooth surface is desiccated and are termed non-cavitated enamel caries lesions or incipient caries or white spot lesions (WSL). These areas of enamel lose their translucency, because of the extensive subsurface porosity caused by demineralization. However, it has also been shown experimentally and clinically that non-cavitated caries of enamel can remineralize (Box 1.5).

BOX 1.5
Remineralization mechanism of a white spot lesion (WSL)
The supersaturation of saliva with calcium and phosphate ions serves as the driving force for the remineralization process
![]()
Non-cavitated enamel lesions retain most of the original crystalline framework of the enamel rods, and the etched crystallites serve as nucleating agents for remineralization
![]()
Calcium and phosphate ions from saliva can penetrate the enamel surface and precipitate on the highly reactive crystalline surfaces in the enamel lesion
![]()
The presence of trace amounts of fluoride ions during this remineralization process greatly enhances the precipitation of calcium and phosphate, resulting in the remineralized enamel becoming more resistant to subsequent caries attack, because of the incorporation of more acid-resistant fluorapatite
![]()
Remineralized (arrested) lesions can be observed clinically as intact, but discoloured, usually brown or black, spots. The change in colour is presumably caused by trapped organic debris and metallic ions within the enamel. These discoloured and remineralized arrested caries areas are intact and are more resistant to subsequent caries attack than the adjacent unaffected enamel. They should not be restored, unless they are aesthetically objectionable.
Location: These lesions usually are observed on the facial and lingual surfaces of teeth. They can also occur in the proximal surfaces, but are difficult to detect.
Remineralization mechanism
The remineralization mechanism of white spot lesion (WSL) is summarized in Box 1.5.
Clinical Note
i. Care must be exercised in distinguishing white spots of non-cavitated caries from developmental white spot hypocalcifications of enamel.
ii. Non-cavitated (white spot) caries partially or totally disappears visually when the enamel is hydrated (wet), whereas hypocalcified enamel is affected less by drying and wetting.
iii. Hypocalcified enamel does not represent a clinical problem, except for its aesthetically objectionable appearance.
iv. Injudicious use of an explorer tip can cause actual cavitation in a previously non-cavitated area, requiring in most cases, restorative intervention.
v. Role of explorer the recommended instrument for probing is CPITN probe having a 0.5 mm ball-ended tip. Probing should be done judiciously with tactile sensation to detect surface roughness, by gently stroking across the tooth surface (Fig. 1. 41).

ii. Cavitated enamel caries
Cavitated enamel lesions can be initially detected as subtle breakdown of the enamel surface. These lesions are very sensitive to probing and can be easily enlarged by using sharp explorers and excessive probing force. More advanced cavitated enamel lesions are more obviously detected as enamel breakdown.
Zones of enamel caries
The four zones in a sectioned incipient lesion when examined in quinoline by transmitted light are:
B. Dentin caries
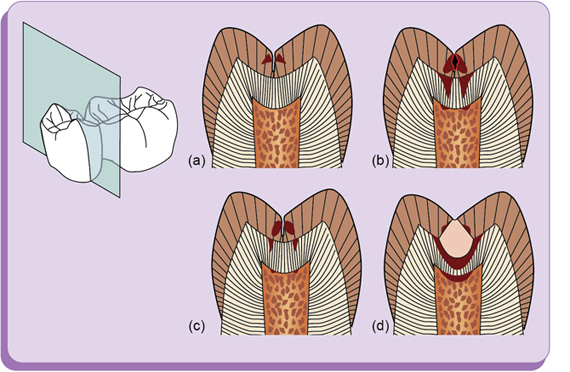
Progression of dental caries (Fig. 1.42)


Rate of progression: Caries advances more rapidly in dentin than in enamel because:
Dentin provides much less resistance to acid attack owing to less mineralized content.
Dentin possesses microscopic tubules that provide a pathway for the ingress of bacteria and egress of minerals
Shape of lesion: Dentin caries is V-shaped in cross-section with a wide base at the DEJ and the apex directed pulpally (Figs 1.43 and 1.44).

Dentinal reaction to caries
The three levels of dentinal reaction to caries that can be recognized are:
Reaction to a long-term, low-level acid demineralization associated with a slowly advancing lesion → Sclerotic dentin formation
Reaction to a moderate-intensity attack → Reparative dentin formation
Reaction to severe, rapidly advancing caries characterized by very high acid levels → Pulpal necrosis and periradicular progression of disease
I. Reaction to a long-term, low-level acid demineralization associated with a slowly advancing lesion: Sclerotic dentin formation
Dentin that has more mineral content than normal dentin is termed sclerotic dentin.
Sclerotic dentin formation occurs ahead of the demineralization front of a slowly advancing lesion and may be seen under an old restoration.
Sclerotic dentin is usually shiny and darker in colour, but feels hard to the explorer tip. By contrast, normal freshly cut dentin lacks a shiny, reflective surface and allows some penetration from a sharp explorer tip.
The apparent function of sclerotic dentin is to wall off a lesion by blocking (sealing) the tubules.
II. Reaction to a moderate-intensity attack: Reparative dentin formation
The second level of dentinal response is to moderate-intensity irritants, by forming reparative dentin (Box 1.6).
BOX 1.6
Mechanism of reparative dentin formation
Infected dentin contains a wide variety of pathogenic materials or irritants, including high acid levels, hydrolytic enzymes, bacteria, and bacterial cellular debris.
![]()
The pulp may be irritated sufficiently from high acid levels or bacterial enzyme production to cause the formation (from undifferentiated mesenchymal cells) of replacement odontoblasts (secondary odontoblasts)
![]()
These cells produce reparative dentin (reactionary dentin) on the affected portion of the pulp chamber wall
III: Reaction to severe, rapidly advancing caries characterized by very high acid levels: Pulpal necrosis and periradicular progression of disease
The third level of dentinal response is to severe irritation. Acute, rapidly advancing caries with high levels of acid production overpowers dentinal defences and results in infection, abscess, and death of the pulp (Box 1.7).
BOX 1.7
Mechanism of pulpal necrosis
Small, localized infections in the pulp produce an inflammatory response involving capillary dilation, local oedema, and stagnation of blood flow
![]()
As the pulp is contained in a sealed chamber, and its blood is supplied through narrow root canals, any stagnation of blood flow can result in local anoxia and necrosis
![]()
The local necrosis leads to more inflammation, oedema, and stagnation of blood flow in the immediately adjacent pulp tissue, which becomes necrotic in a cascading process that rapidly spreads to cause entire pulpal necrosis
Zones of dentin caries
Three different zones have been described in carious dentin (Fig. 1.45).

Zone 1: Normal dentin
• The deepest area is normal dentin, which has tubules with odontoblastic processes that are smooth and no crystals are present in the lumens.
• The intertubular dentin has normal cross-banded collagen and normal dense apatite crystals.
• No bacteria are present in the tubules.
• Stimulation of dentin (e.g. by osmotic gradient [from applied sucrose or salt], a bur, a dragging instrument, or by desiccation from heat or air) produces a sharp pain.
Zone 2: Affected dentin
• Also called inner carious dentin, affected dentin is a zone of demineralization of intertubular dentin and of initial formation of fine crystals in the tubule lumen at the advancing front.
• Damage to the odontoblastic process is evident.
• Affected dentin is softer than normal dentin and shows loss of mineral from intertubular dentin and many large crystals in the lumen of the dentinal tubules.
• Stimulation of affected dentin produces pain.
• Although organic acids attack the mineral and organic contents of dentin, the collagen cross-linking remains intact in this zone.
• The intact collagen can serve as a template for remineralization of intertubular dentin and this region remains capable of self-repair, provided that the pulp remains vital.
• The affected dentin zone can also be subclassified into three subzones:
Zone 3: Infected dentin
• Also called outer carious dentin, this is the outermost carious layer, the layer that the clinician would encounter first when opening a lesion.
• The infected dentin is the zone of bacterial invasion and is marked by widening and distortion of the dentinal tubules, which are filled with bacteria.
• Little mineral is present, and the collagen in this zone is irreversibly denatured.
• The dentin in this zone does not self-repair.
• This zone cannot be remineralized, and its removal is essential to sound, successful restorative procedures and the prevention of spreading the infection.
Visual clinical examination using international caries detection and assessment system (ICDAS)
The ICDAS was developed to serve as a guide for standardized visual caries assessment that could be used for clinical practice, clinical research, education, and epidemiology. During the clinical examination, every accessible surface of each tooth must be inspected for localized changes in colour, texture, and translucency, as described in the ICDAS codes.
Preliminary preparation
This requires two minimum conditions for the examination to be properly conducted:
- Biofilm or plaque must be thoroughly removed from teeth prior to the examination.
- Teeth must be sufficiently air-dried, so that the changes can be seen properly.
The visual examination is then conducted in a dry, well-illuminated field. Through direct vision and reflecting light through the occlusal surface of the tooth, the occlusal surface is diagnosed as diseased, if chalkiness or apparent softening or cavitation of tooth structure forming the fissure or pit is seen or a brown-gray discolouration, radiating peripherally from the fissure or pit, is present.
ICDAS assessment
The ICDAS uses a two-stage process to record the status of the caries lesion. The first is a code for the restorative status of the tooth and the second is for the severity of the caries lesion. The status of the caries severity is determined visually on a scale 0−6:
1 = first visual change in enamel
2 = distinct visual change in enamel
3 = enamel breakdown, no dentin visible
4 = dentinal shadow (not cavitated into dentin)
This severity code is paired with a restorative/sealant code 0−8:
3 = sealant, full; tooth-coloured restoration
5 = stainless steel restoration
6 = ceramic, gold, or PFM (porcelain-fused-to-metal) crown or veneer
See Figure 1.46 for the ICDAS for examples of coding for restorative status and caries severity. The details of this system for detection and training to use the system with an online tutorial are available at www.icdas.org.

Non-carious destruction of tooth
I. Tooth wear
1. Attrition
• Loss of tooth structure on chewing surfaces (occlusal and incisal) is due to frictional forces between contacting surfaces (Fig. 1.47).






2. Abrasion
• Mechanical loss of tooth structure mainly on the buccal and lingual surfaces is due to an abrasive medium (Fig. 1.48).

3. Erosion
• Loss of tooth structure is due to chemical agent, like acidic drinks, by regurgitation of acid due to gastric acidity (Fig. 1.49).

4. Abfraction
• Abfraction is defined as loss of tooth structure or microfractures in the cervical areas of the teeth due to abnormal tooth flexure (Fig. 1.50).
• Emphasis is on prevention and monitoring of tooth wear in early stages.
• Restorations are necessary when the teeth become sensitive and in severe cases, crowns are needed.

II. Trauma
• Trauma caused by falls or injury leads to:
○ Fracture of the tooth involving enamel alone, enamel and dentin, or pulp exposure (Fig. 1.51).
