Myology
The muscles provide an important mechanical stimulus for bone formation. A number of clinical and animal studies suggest a relationship between the masticatory muscle function and skeletal adaptation in the craniofacial region. A number of appliances used in orthodontics displace the mandible forward or downward, causing stretching of the orofacial soft tissues. Optimal masticatory muscular force and balance during growth is necessary for normal maxillomandibular growth.
Types of muscle
There are generally three types of muscle in the human body.
Skeletal muscle
This is striated and voluntary. Skeletal muscle or ‘voluntary muscle’ is anchored by tendons to bone and is used to affect skeletal movement such as locomotion and in maintaining posture. Though this postural control is generally maintained as a subconscious reflex, the muscles responsible also react to conscious control, like non-postural muscles.
Smooth muscle
This is striated and involuntary. Smooth muscle or ‘involuntary muscle’ is found within the walls of organs and structures such as the esophagus, stomach, intestines, bronchi, uterus, urethra, bladder, blood vessels, and even the skin (in which it controls erection of body hair). Unlike skeletal muscle, smooth muscle is not under conscious control.
Cardiac muscle
This is non-striated and involuntary. Cardiac muscle is also an ‘involuntary muscle’ but is more akin in structure to skeletal muscle, and is found only in the heart.
Properties of muscle
To propel the skeleton, man has 639 muscles, composed of 6 billion muscle fibers. Each fiber has 1000 fibrils, which means that there are 6000 billion fibrils at work at one time or another (Fig. 10.1).

Certain basic laws govern muscle activity. Muscle has two physical properties that are important in its kinetic activity. These are: (1) elasticity and (2) contractility.
Elasticity
Normal relaxed muscle withstands only a certain amount of elongation (about six-tenths of its natural length) before rupturing. This is only an approximation and, of course, is dependent on the muscle involved, the type of stress, the individual resistance, age and possible pathological conditions that have produced fibrotic changes that would markedly limit extensibility of the muscle.1 Extensibility within certain limits is quite easily accomplished by an external force, but the muscle returns to its exact original shape after being stretched, illustrating the quality of elasticity.
The factors which determine the inert elasticity of the muscle are its length, the cross-section, the force being exerted and a certain constant coefficient, which is determined by the nature of the body.
Contractility
Contractility is the ability of a muscle to shorten its length under innervational impulse. Although the elasticity of the muscle influences contractility, this phenomenon is quite different.2 The complex biochemical changes that induce muscle contraction are not completely known. A simplified version of current evidence indicates that a muscle is first stimulated by an electric action potential, causing contraction. Energy for the muscle is provided, for the most part, by the breakdown of the high-energy bonds in adenosine triphosphate.
Fatigue in a muscle is produced when lactic acid, an energy breakdown byproduct, collects in the tissues, lowering the pH to a level at which the muscle can no longer function efficiently.3 How much muscle will shorten during contraction again depends on a number of factors (striated or smooth muscle, number of fibers, cross-section, frequency of discharge, muscle fiber length, etc.). Some muscles may contract as much as 50–75% of their natural length. The temporalis muscle, because of its relatively long fibers, has a greater contraction length than the masseter muscle.
Isometric and isotonic contractions
Isometric contraction occurs when a muscle is simply resisting an external force without any actual shortening. In an isotonic contraction, such as flexing the biceps, there is an actual shortening. The dentist must know that the greatest strength of contraction is elicited when the muscle approximates its resting length (Fig. 10.2). A muscle develops its maximum force when all its fibers are repeatedly stimulated to ‘fire’. This summation of contractions of the muscle fibers produces muscle tetany and develops four times that of the normal ‘single contraction’ strength in the muscle.

In a recent study in which a gnathodynamometer was used on open- and closed bite cases, just the opposite results were observed.4 Open bite cases averaged 97 lb (431.47 Newtons) of force, while closed-bite cases averaged 118 lb (524.9 Newtons) (females only 96–104 lb or 427–462.6 Newtons).
Principle of electromyogram
The best way to visualize the innervation of a muscle is by the use of an electromyogram. Einthoven discovered in 1918 that a muscle during contraction gives off an idiomuscular current. This is referred to as an action current. Apparently, only the contraction of the muscle produces this electrical phenomenon. The current generated is so small that it must be amplified many thousands of times to be recorded. By means of the electromyogram, one can get a relatively accurate picture of muscular activity under diverse functional conditions (Fig. 10.3).

Two types of electrodes are used. They are surface electrode and needle electrode. Surface electrodes record from a larger population of muscle fibers than do needle electrodes.
Jaw reflex types
Myotatic reflex
It is the tonic contraction of the muscles in response to a stretching force, due to stimulation of muscle proprioceptors. It is also called Liddell-Sherrington reflex, muscular reflex, and stretch reflex.
Clasp knife reflex
This phenomenon is produced by stretching an extensor muscle against a background of increased extensor muscle tone. The result is a relaxation of the muscle being stretched, i.e. the muscle now lengthens easily after initial resistance. Clasp knife reflex is also called autogenic inhibition or inverse myotatic reflex.
Jaw-closing reflex
Jaw-closing reflex is the most basic reflex in the facial and oropharyngeal area. Jaw-closing reflex is sometimes referred to as jaw jerk reflex.
Jaw-opening reflex
This reflex is the first reflex movement to make its appearance in the orofacial region of human beings at about 8.5 weeks of intrauterine life. This is sometimes known as the linguomandibular reflex, since it also occurs with brief application of a noxious stimulus to the tongue.
Buccinator mechanism
Although bone is the hardest tissue in the body, it is one of the most responsive to change when there is an alteration in the environmental balance. The major factor in this environmental balance is the musculature. Muscles are a potent force, whether they are in active function or at rest. A resting muscle still is performing a function—that of maintaining posture and a relationship of contiguous parts.5, 6
Aberrations of muscle function can and do produce marked malocclusions. The restrictive, guiding role of the buccinator mechanism (Fig. 10.4) must be recognized and emphasized. Starting with the decussating fibers of the orbicularis oris muscle, joining right and left fibers in the lips (Fig. 10.5), the buccinator mechanism runs laterally and posteriorly around the corner of the mouth, joining other fibers of the buccinator muscle that insert into the pterygomandibular raphe just behind the dentition. At this point, it intermingles with fibers of the superior constrictor muscle and continues posteriorly and medially to anchor at the origin of the superior constrictor muscles, the pharyngeal tubercle of the occipital bone. There are 13 muscle attachments to the mandible alone, with elasticity, contractility and tonus making the analogy of the rubber bands acting on the bone system not too far-fetched.


Opposing the buccinator mechanism is a very powerful muscle—the tongue. The teeth and supporting structures are constantly under the influence of the contiguous musculature. The integrity of the dental arches and the relations of the teeth to each other within each arch and with opposing members are the result of the morphogenetic pattern, as modified by the stabilizing and active functional forces of the muscles (Figs. 10.6 and 10.7).


Tongue
The tongue begins its manifold activities even before birth, when it functions in the swallowing of amniotic fluid. It is relatively one of the best developed structures in the human body at birth. Not only is the tongue advanced in function because of its important role in nursing, but it is also relatively larger than contiguous structures and thus assumes a posture interposed between the gum pads, rather than completely contained within them, as might be expected7 (Fig. 10.8).

Winders8, 9 has shown that during mastication and deglutition, the tongue may exert two to three times as much force on the dentition as the lips and cheeks at any one time but the net effect is one of balance as tonal contraction, peripheral fiber recruitment of the buccal and labial muscles and atmospheric pressure team up to offset the momentarily greater functional force of the tongue.
The tongue has amazingly versatile functional possibilities by virtue of the fact that it is anchored at only one end. This very freedom permits the tongue to deform the dental arches when function is abnormal.
Equilibrium theory
The equilibrium theory of tooth position proposes that a stable dentition exists in a state of balance—where the net resting pressure of the tongue, lips, cheeks, and periodontium is zero. If this balance is disrupted, then the teeth will move until a new state of equilibrium is reached. Thus, the equilibrium position of a tooth is the position from which it will not be moved by natural environmental forces.10
Proffit identifies four major primary factors, the factors that directly influence dental equilibrium.11 They are listed in Box 10.1.
Teeth are positioned between the lips and cheeks on the outer aspect and tongue on the inner aspect. Recent studies analyzing the forces provided by the tongue and lips have shown that there is no balance of force between the tongue and lips. Tongue exerts more force than lips during swallowing and rest position (Fig. 10.9). The dental apparatus is well developed to resist short-acting forces that are generated during speaking, swallowing, and chewing. It is clearly evident that the minimum time to induce tooth movement is around 6 hours. It is not the magnitude of the force that is important but the duration of the force. Even light, sustained forces from the tongue, lips, and cheeks can induce tooth movement. Hence lips and tongue forces during mastication alone do not contribute to equilibrium. The most significant factor in dental equilibrium seems to be the resting pressures of the tongue and lips along with the forces generated by the periodontal ligament. If the restraining pressure from the tongue is removed, then the teeth will collapse lingually (Fig. 10.10) and in the same way, if forces from the tongue are not counteracted by the lips and cheek musculature, then the teeth will move outward.

The forces from occlusion, probably, play a role in the vertical positioning of the teeth. The vertical position of the tooth is influenced by the equilibrium between the forces that promote eruption and those that prevent or oppose eruption. Altered head, jaw, and tongue posture due to respiratory needs can alter the equilibrium. The periodontal attachment apparatus of the teeth acts as an efficient hydrodynamic damping system similar to the shock absorber. This kind of system is able to withstand the forces from occlusion. The force from occlusion is usually of shorter duration. Thus, the periodontal ligament serves as a sort of active stabilization in maintaining the position of the teeth.
Extrinsic forces, like orthodontic appliances and habits, produce the effects by altering the equilibrium. But in these conditions too, it is the duration of the force applied by the appliance or due to habits that is critical. Constant pressure habits of prolonged duration (minimum 6 hours) and prolonged force from orthodontic appliances alter the position of teeth.
Thus, the two major primary factors influencing equilibrium are the resting pressures of lips, cheeks, and tongue and forces produced due to the metabolic activity of the periodontal ligament.
Functional movements
The mandible is the only movable bone in the head and face, and it can only be moved in certain directions because of the limitations of morphology and of the structure of the temporomandibular articulation. The precarious balance that the head maintains on the vertebral column illustrates the constant demand for activity in holding the head erect (Fig. 10.11). The postural function must be effective enough to permit the muscle activity associated specifically with mastication, deglutition, respiration and speech. The functions are superimposed on the primary and postural function.

Opening of mandible
Gravity and also the primary contraction of the lateral pterygoid muscles are largely responsible for the opening movement. Stabilizing and adjusting activities are seen in the suprahyoid and infrahyoid groups, in the geniohyoid, mylohyoid and digastric muscles. The stylohyoid muscle changes in length. The hyoid bone itself moves downward and backward with the opening movement of the mandible. The temporal, masseter and medial pterygoid muscles show a controlled relaxation as the mandible opens. This controlled relaxation serves to make the opening movement smooth.
During the opening movement of the mandible, the articular disk is brought forward by the lateral pterygoid muscle and intimately related capsular ligaments as the condyle rotates against the inferior surface of the disk and as the disk itself glides forward on the articular eminence.12, 13
Mandible closure
The closing movement of the mandible is also a closely coordinated activity of the closing and opening muscles. Considerably more power is elicited on mandibular closure due to the bilateral activity of the masseter and temporalis muscles, assisted by the smaller medial pterygoid muscles. The hyoid bone moves upward and forward during mandibular closure. The lateral pterygoid muscles, through their controlled relaxation, help affect a smooth and uninterrupted activity. If resistance is met during the closure, greater activity is generated in the lateral pterygoid, suprahyoid and infrahyoid muscles.14
Mandible protraction
To protrude the mandible, the lateral and medial pterygoid muscles contract in unison, in conjunction with controlled stabilizing relaxation of the opening muscles.
Mandible retrusion
The retruding action of the mandible is less definite and less efficient. Retrusion is accomplished largely by the contraction of the posterior fibers of the temporalis muscles, with some assistance from the geniohyoid, digastric and mylohyoid muscles. The hyoid bone also moves posteriorly, indicating some action of the infrahyoid muscle group. It should be remembered that the ligaments that make up the stabilizing elements of the temporomandibular joint tend to restrict any retruding action.
Lateral movement
Lateral movement is initiated by the combined activity of the lateral pterygoid muscle on one side with controlled relaxation on the other side, and by the contraction of the temporalis muscle on one side and controlled relaxation on the opposite side. In other words, if the mandible is being moved to the left to masticate a bolus of food, there is a contraction of the right lateral pterygoid muscle and a controlled relaxation of the right temporalis muscle. On the left side, there is a definite contraction of the left temporalis muscle and a controlled relaxation of the lateral pterygoid muscle on that side.
Bennett movement (fig. 10.12)
• Bodily side shift of the mandible towards the working side during lateral excursion is called Bennett movement.
• The working side condyle may either rotate, or rotate and move laterally, and also upwards or downwards.
• Bennett movement is necessary to permit rotation of the working condyle, because of the restraining influence of the temporomandibular ligament on the working side, the walls of the glenoid fossa.
• Stages of Bennett movement—immediate shift or progressive side shift.
• If the lateral component occurs early in the movement, it is termed as immediate or early side shift.
• A gradual lateral component is termed as progressive side shift.
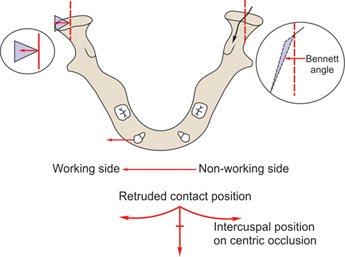
Bennett angle
• When the working side condyle shifts laterally, the non-working side condyle moves downwards, forwards and inwards.
• Angle formed between the forward and inward movements of the non-working condyle and a straight forward movement is known as Bennett angle (Fig. 10.12).
Positions of mandible
To better understand variations from the normal, let us first outline the basic positions of the mandible with respect to the maxilla and cranium. These basic positions are listed in Box 10.2. Because of the manifold demands on the muscles associated with mandibular movements, coordination is essential in both synergistic and antagonistic groups.
Postural resting position (postural vertical dimension)
The mandibular resting position is one of the earliest postural positions to be developed. The mandible is literally suspended from the cranial base by the cradling musculature (Fig. 10.11). The jaws are not clamped together, but they are separated by a rather constant distance, even before there are any teeth in the mouth (Fig. 10.13).

Definition. Physiologic rest position or postural rest position is defined as the position of the mandible when the muscles of mastication are in a minimum tonus of contraction.
It is the position where the antagonist and agonist concerned with the mandibular opening are in a state of equilibrium.
Factors affecting rest position. Body and head position, sleep, psychic factor, age, pain, proprioception from the dentition and muscles, occlusal changes, TMJ disease, muscle disease and spasm.
Freeway space. It is the measured distance between the occlusal surfaces of the maxillary and mandibular dental arches. The distance between the rest intermaxillary dimension and full occlusion indicates the amount of clearance between the teeth in the dental arches. This constitutes the interocclusal space or freeway space.
Centric relation
Centric relation refers to the position of the mandibular condyle in the articular fossa. Centric relation may be defined as the unstrained, neutral position of the mandible in which the anterosuperior surfaces of the mandibular condyles are in contact with the concavities of the articular disks as they approximate the posteroinferior third of their respective articular eminentia. This means that the mandible is deviating neither to the right nor to the left and is neither protruded nor retruded.
Initial contact
When the patient takes the mandible from rest position to occlusion, the position at which first tooth contact occurs is called initial contact position, the movement that occurs in the temporomandibular joint is entirely rotation in the lower joint space. Initial contact and centric occlusion should coincide.
Premature contacts are, unfortunately, quite frequent. They can and do initiate deflections in the mandibular path of closure. In situations, like premature contact, anterior crossbite and pseudo class III malocclusion, from initial contact mandible slides to new occlusal contact position.
Centric occlusion (occlusal vertical dimension)
Centric occlusion in orthodontics also implies a state of balance. With maximal contact of the inclined planes of the opposing teeth, there must be bilaterally symmetrical activity, a balanced and unstrained relationship of temporomandibular structures. Centric occlusion is defined as the mandibular position in which there is maximum intercuspation of the teeth.
Centric occlusion is a static position and can be easily reproduced by having the patient bring the teeth together, if there is no malocclusion or malfunction present (Fig. 10.14A). Premature contacts, loss of teeth, over eruption of teeth, overextension of artificial restorations, and malpositions of individual teeth—all these mitigate against the establishment of a centric occlusion.
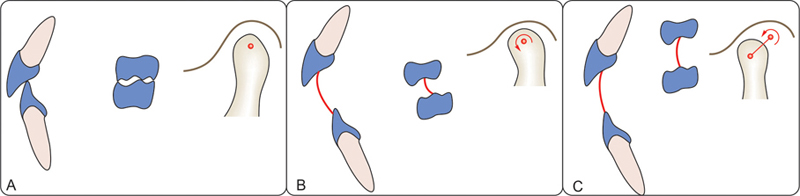
Most retruded position (terminal hinge position)
Mandible can hinge about a horizontal axis called the retruded axis or terminal hinge axis (RP). This is the most retruded position of mandible (Fig. 10.14B).
Maximum opening of mouth
As the mandible continues to open beyond the retruded axis, the condyle translates forwards and downwards to a position of maximum opening (Fig. 10.14C).
Most protruded position
The most protruded position in the mandible is more variable from individual to individual than the retruded position. Within the same individual, however, it is reproducible.
Posterior tooth relationship during lateral excursions
During lateral excursions of the mandible, three types of posterior tooth relationship can occur:
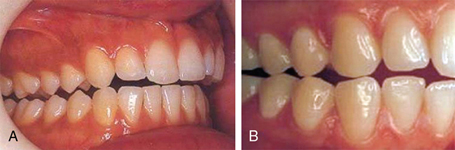
1. Canine protected occlusion. Lateral movements of the mandible are guided by the working side canines, with disclusion of all the other teeth on both working and non-working sides. There is contact in lateral movement only between canines on the working side (Fig. 10.15A). On the non-working side, there is no tooth contact. The canine tooth is considered to be the ideal tooth to guide the mandible during lateral excursion due to certain reasons (Box 10.3).
2. Group function occlusion. If there is contact on the working side between two or more teeth, the working side guidance is referred to as group function. There is no tooth contact on the non-working side (Fig. 10.15B).
3. Balanced occlusion. During lateral movement, posterior teeth on both the working and non-working sides are in contact. Early researchers in the field of occlusion were of the opinion that this type of balanced occlusion is the best for normal occlusion. Present concept has dismissed this view, and it is being used only in the denture construction.
Habitual resting position
It needs to be recognized in orthodontics, that the habitual resting position may not be the same as the true physiologic postural position.
There are certain types of malocclusions that prevent the patient from achieving a physiologic resting position. In a severe Class II, division 2 malocclusion with the maxillary incisors markedly inclined to the lingual, there is a tendency to force the condyles posteriorly and superiorly in the articular fossae (Fig. 10.16).

Electromyographic studies seem to show greater activity in the muscles associated with mandibular posture than would be normal for an unstrained position at rest. In many cases, the removal of the abnormal guiding force of the lingually inclined maxillary incisors allows the mandible to come forward, and a demonstrable reduction in electrical activity at this new resting position can be seen.
Habitual occlusal relation (occlusal vertical dimension)
In a normal occlusion, the centric occlusion and habitual occlusion should be the same. In malocclusion, there is asynchronous activity of the closing muscles in habitual and working bite occlusions.