Orbit and Eyeball
ORBIT
The orbits are a pair of pyramidal-shaped bony cavities, located one on either side of the root of the nose and provides sockets for rotatory movements of the eyeballs. Each orbit is a four-sided pyramid with apex directed behind at the optic canal and base forward, represented by the orbital margin. The medial walls of two orbits are parallel to each other but the lateral walls are set at right angle to each other (Fig. 19.1).
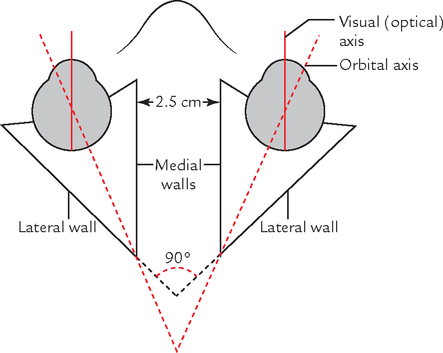
The long axis of each orbit (orbital axis) passes backwards and medially.
BOUNDARIES
The boundaries of the orbit (Fig. 19.2) are as follows:
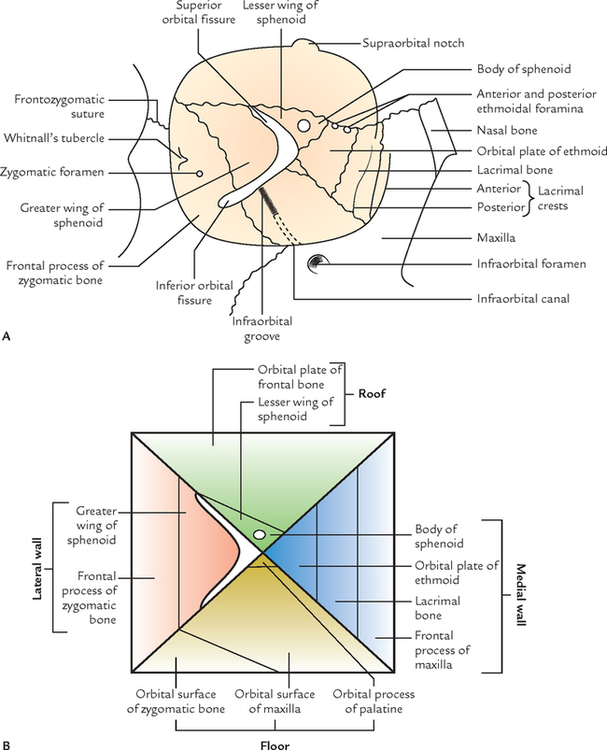
Medial wall (thinnest): Formed by four bones; from before backwards these are as follows:
Lateral wall (strongest): Formed by two bones, viz.
1. Orbital surface of the body of maxilla.
Roof: Formed by two bones, viz.
Presenting Features in Four Boundary Walls of Orbit (Fig. 19.3)
Medial wall: Presents two features, viz.

1. Lacrimal fossa is bounded in front by the anterior lacrimal crest of maxilla and behind by the posterior lacrimal crest of the lacrimal bone. The lacrimal fossa communicates with the nasal cavity through nasolacrimal canal. The lacrimal fossa and nasolacrimal canal lodge lacrimal sac and nasolacrimal duct, respectively.
2. Anterior and posterior ethmoidal foramina, lie at the junction between medial wall and the roof of the orbit.
Lateral wall: Presents two features, viz.
1. Zygomatic foramen. Sometimes there are two small foramina, for zygomaticofacial and zygomaticotemporal nerves.
2. Whitnall’s tubercle, a small bony tubercle just behind the lateral orbital margin and slightly below the frontozygomatic suture.
Floor: Presents two features, viz.
1. Infraorbital groove and canal.
2. Small rough impression in anteromedial angle for origin of inferior oblique muscle.
Roof: Presents three features, viz.
1. Fossa for lacrimal gland in the anterolateral part.
Apex: Lies at the posterior end of the orbit and is formed by sphenoid. More precisely it is formed by the centre of the bony bridge between optic canal and superior orbital fissure.
Base: Open and quadrangular, its boundaries form the orbital margins.
Orbital Margins
The orbital margins are formed as follows:
1. Supraorbital margin is formed by the frontal bone and presents a notch—supraorbital notch or foramen at the junction of its lateral two-third and medial one-third.
2. Infraorbital margin is formed by the zygomatic bone laterally and maxilla medially; it is continuous with anterior lacrimal crest medially.
3. Medial orbital margin is ill-defined. It is formed by the frontal bone above and lacrimal crest of the frontal process of maxilla below.
4. Lateral orbital margin is formed by zygomatic process of the frontal bone above and frontal process of the zygomatic bone below.
The margins of the orbit are readily palpable in vivo.
N.B. The orbital margins provide a fair bony protection to the eye except at the lateral margin. For this reason protective eye guards are designed to compensate for it, in squash and handball players and still permitting good peripheral vision.
RELATIONS
The relations of orbit are as follows:
Above: Anterior cranial fossa and frontal air sinus (usually).
Lateral: Temporal fossa in front and middle cranial fossa behind.
ORBITAL FASCIA OR PERIORBITA
It is the periosteum of the bony orbit, which lines the bony boundaries of the orbit and forms a funnel-shaped fascial sheath that encloses the orbital contents (Fig. 19.5). It is loosely attached to the bones, hence can be easily stripped off especially from roof and medial wall of the orbit.

At the optic canal and superior orbital fissure, it becomes continuous with the periosteum lining the interior of the skull (endocranium). At the infraorbital fissure and orbital margins, it becomes continuous with the periosteum covering the external surface of the skull (periosteum).
CONTENTS
Contents of the orbit includes the following structures (Fig. 19.4):

All these structures lie within the orbital periosteum that lines the bony walls of the orbit.
N.B. Infraorbital nerve and vessels and zygomatic nerve lie outside the orbital periosteum, hence not included in the contents of the orbit.
EXTRAOCULAR MUSCLES
The extraocular muscles are classified into two groups: voluntary and involuntary.
VOLUNTARY MUSCLES
There are seven voluntary muscles in the orbit. Of these, six muscles move the eyeball and one muscle moves the upper eyelid.
The muscles moving the eyeball are four recti and two oblique muscles. The one which moves the upper eyelid is called levator palpebrae superioris (Fig. 19.6):

INVOLUNTARY MUSCLES
There are three involuntary/smooth muscles, viz. superior tarsal or Muller’s muscle, inferior tarsal and orbitalis.
The voluntary muscles are described in detail because of their functional significance in the following text:
Origin:
All the recti arise from the corresponding margins of the common tendinous ring. The lateral rectus arises by two heads.
The common tendinous ring encloses the optic canal and middle part of the superior orbital fissure. It is attached medially to apex of the orbit and laterally to a small tubercle (tubercle of Zinn) on the lower border of superior orbital fissure.
Insertion:
All the recti are inserted into sclera little posterior to the limbus (corneoscleral junction) in front of the equator of the eyeball. Average distance from limbus is:
The origin and insertion of recti muscles are shown in Figure 19.6.
The oblique muscles of the orbit are superior and inferior. Their origin and insertion (Fig. 19.6) are as follows:
Origin: from body of sphenoid superomedial to the optic canal.
Insertion: into sclera behind the equator in posterior superior quadrant of the eyeball, between the superior rectus and lateral rectus. The tendon of superior oblique passes through a fibrocartilaginous pulley attached to the trochlear notch in the anterolateral part of the roof of the orbit.
Origin: from rough impression in the anteromedial angle of the floor of orbit, lateral to the lacrimal groove.
Insertion: into sclera behind the equator in the postero-superior quadrant of the eyeball a little below and posterior to the insertion of superior oblique.
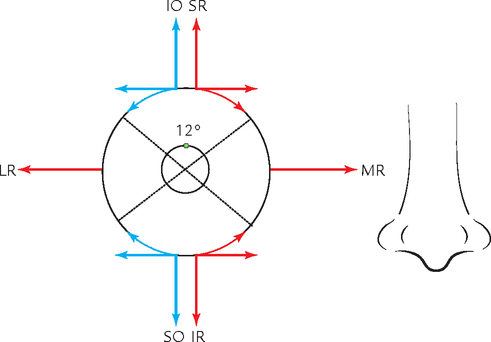
Nerve supply (Fig. 19.7): all the extraocular muscles that move the eyeball are supplied by the oculomotor nerve (CN3) except lateral rectus and superior oblique, which are supplied by the abducent nerve (CN6) and trochlear nerve, respectively [mnemonic: LR6, SO4, i.e., LR (lateral rectus) by 6 CN and SO (superior oblique) by 4 CN].

ACTIONS OF MUSCLES ON THE EYEBALL
The two eyes face forwards and their long axes (visual optic axes) lie in sagittal plane, parallel with each other and with medial walls of the orbits (Fig. 19.1). The lateral walls of orbits slope backwards and medially making a right (90°) angle with each other. The ocular muscles and optic nerve come from the apex of the orbit near the back of the medial wall and pass forwards and laterally to be attached to the eyeball. The actions of superior and inferior recti are, therefore, not straight, despite their name. The superior and inferior oblique muscles, therefore, have to act in concert with two recti in order to produce direct upward and downward movements of the eyeball.
Axis of Movements of the Eyeball
• Elevation and depression: around the transverse axis passing through the equator.
• Adduction and abduction: around the vertical axis passing through the equator.
• Rotation (torsion): around the anteroposterior axis extending from anterior pole to posterior pole of the eyeball.
When 12 o’clock position of the cornea rotates medially, it is called intorsion and when it rotates laterally, it called extorsion.
Actions of Individual Muscles
The actions of individual muscles are easily deduced from Starling’s diagram (Fig. 19.8).
Associated Movements of the Eyeball
1. Conjugate movements: when both the eyes move in the same direction with visual axes being parallel.
2. Disconjugate movements: when the axes of both eyes converge or diverge.
Levator palpebrae superioris (LPS) muscle
Origin: from undersurface of the lesser wing of sphenoid at the apex of the orbit, above the common tendinous ring by a narrow tendon.
Insertion (![]() Fig. 3.22): the muscle broadens as it passes forwards from its origin and divides into three lamellae:
Fig. 3.22): the muscle broadens as it passes forwards from its origin and divides into three lamellae:
1. Upper lamella consisting of skeletal muscle penetrates the orbital septum passes through the fibres of orbicularis oculi to be inserted into the skin of upper eyelid.
2. Intermediate lamella consisting of smooth muscle (superior tarsal muscle) is inserted on to the upper border of the superior tarsal plate.
3. Lower lamella consisting of connective tissue is inserted on to the superior fornix of the conjunctiva.
FASCIA BULBI OR FASCIAL SHEATH OF THE EYEBALL
The fascia bulbi (Tenon’s capsule) is a loose membranous sheath that envelops the eyeball and extends from optic nerve to the sclerocorneal junction. It is separated from the sclera by the episcleral space. The Tenon’s capsule forms a socket for the eyeball to facilitate free ocular movements. It separates the eyeball from orbital fat (Fig. 19.9).

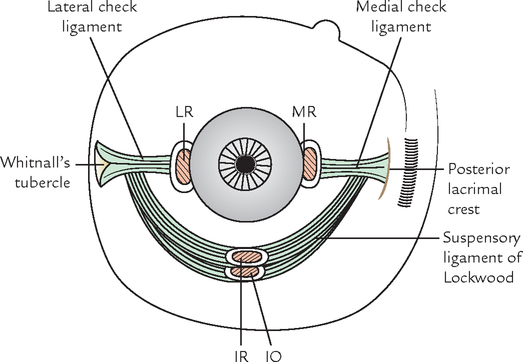
SUSPENSORY AND CHECK LIGAMENTS OF THE EYE
The fascia bulbi provides a tubular sleeve around each muscle that pierces it. From the fascial sleeve of lateral rectus, a triangular expansion (lateral check ligament) extends laterally for attachment to the lateral wall of the orbit on Whitnall’s tubercle. Similarly, a triangular expansion from sleeve of medial rectus (medial check ligament) extends medially for attachment to the medial wall of the orbit on posterior lacrimal crest of the lacrimal bone.
The fascial sleeve of inferior rectus thickens on its underside and blends with the sleeve of inferior oblique as well as with the medial and lateral check ligaments forming a hammock-like support for the eyeball. It is called as suspensory ligament of the eye (or suspensory ligament of Lockwood). It is expanded in the centre and narrows at its extremities. At the posterior pole of the eyeball the fascia bulbi becomes continuous with sheath of the optic nerve (Fig. 19.10).
NERVES OF THE ORBIT
Optic Nerve
It has been described in detail in ![]() Chapter 22. Therefore only brief account is presented here.
Chapter 22. Therefore only brief account is presented here.
This nerve of sight is 4 cm long. It is made up of about 1 million myelinated nerve fibres. The optic nerve emerges from the eyeball, 3 or 4 mm nasal to the posterior pole of the eyeball. It runs backwards and medially, passes through the optic canal to enter the cranial cavity where it joins the optic chiasma. The entire nerve is enclosed in three meningeal sheaths derived from the meninges of the brain. The subarachnoid space around the brain, therefore, extends around the nerve up to the eyeball.
Oculomotor Nerve (Fig. 19.11)
The two divisions of oculomotor nerve enter the orbit through superior orbital fissure within the common tendinous ring. Here the nasociliary nerve lies between the two divisions.
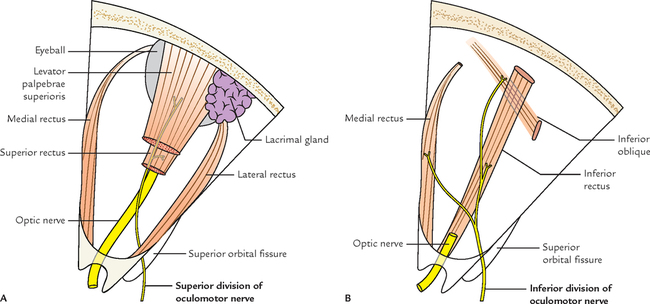
The smaller superior division runs forwards above the optic nerve and supplies the superior rectus, then pierces it to supply the levator palpebrae superioris.
The larger inferior division passes below the optic nerve and divides into three branches to supply medial rectus, inferior rectus, and inferior oblique.
The nerve to inferior oblique gives off the parasympathetic motor root to the ciliary ganglion.
Trochlear Nerve (Fig. 19.12)
The trochlear nerve enters the orbit through the superior orbital fissure superolateral to the common tendinous ring and curves medially above the levator palpebrae superioris to reach deep to the posterior part of superior oblique, which it supplies.

Abducent Nerve (Fig. 19.13)
The abducent nerve enters the orbit through superior orbital fissure within the common tendinous ring lateral to two divisions of the oculomotor nerve and nasociliary nerve, turns laterally away from optic nerve to enter the posterior part of lateral rectus.

Ophthalmic Nerve (Fig. 19.14)
The ophthalmic nerve is the first and the smallest of the three divisions of trigeminal nerve. It is purely sensory.

It arises from medial part of the convex anterior border of the trigeminal ganglion. It pierces the dura mater of the trigeminal cave and enters into the lateral wall of the cavernous sinus where it lies below the trochlear nerve. It enters the orbit through superior orbital fissure by dividing into three branches: lacrimal, frontal, and nasociliary.
1. Lacrimal nerve (smallest branch) runs along the lateral wall of the orbit along with lacrimal artery and ends in the lacrimal gland (hence its name). It is joined by a communicating twig from the zygomaticotemporal branch of the maxillary nerve carrying postganglionic secretomotor fibres to the lacrimal gland. The lacrimal nerve supplies lacrimal gland and conjunctiva. Then it pierces orbital septum to supply the lateral part of the skin of upper eyelid.
2. Frontal nerve (largest branch) runs forwards between levator palpebrae superioris and periosteum lining the roof of the orbit. In the middle of orbit, it divides into large supraorbital and small supratrochlear nerves:
(a) Supraorbital nerve continues in the line of the frontal nerve to pass through supraorbital notch, where it turns upwards into the forehead and divides into medial and lateral branches, which supply the scalp as far back as the vertex.
(b) Supratrochlear nerve runs forwards medial to the supraorbital nerve. It passes above the trochlea for tendon of superior oblique muscle and then turns upwards along the superior orbital margin and supplies the skin of the lower part of the forehead.
3. Nasociliary nerve runs forwards and medially, crossing the optic nerve from above and from lateral to medial side behind the ophthalmic artery. On reaching the medial wall of the orbit, it ends by dividing into anterior ethmoidal and infratrochlear nerves.
It gives the following branches:
(a) Sensory root to the ciliary ganglion is given just before crossing the optic nerve.
(b) Long ciliary nerves, 2 or 3, arise from nasociliary nerve as it crosses the optic nerve. They pass forward, enter the eyeball, and supply sensory fibres to the ciliary body, iris, and cornea.
The long ciliary nerves also carry some postganglionic sympathetic fibres to the dilator pupillae.
(c) Posterior ethmoidal nerve enters the posterior ethmoidal foramen and supplies the ethmoidal and sphenoidal air sinuses.
(d) Anterior ethmoidal nerve enters the anterior ethmoidal foramen and then passes through anterior ethmoidal canal to reach the anterior cranial fossa. Now it runs forwards over the cribriform plate of ethmoid and enters the nasal cavity by passing through a nasal slit at the side of crista galli. In the nasal cavity, the nerve lies in the groove on the posterior surface of the nasal bone and gives internal nasal branches to the nasal septum and lateral wall of the nose. At the lower border of the nasal bone, the nerve leaves the nasal cavity and appears on the dorsum of nose as external nasal nerve.
(e) Infratrochlear nerve runs forwards on the medial wall of the orbit just below the trochlea and ends by supplying the skin of upper eyelid.
Ciliary Ganglion (Fig. 19.15)
It is a peripheral parasympathetic ganglion, connected with the nasociliary nerve. Although topographically it is connected to the nasociliary nerve from ophthalmic division of the trigeminal, but functionally it is connected to the oculomotor nerve.

Three roots enter its posterior end. These are as follows:
1. Motor (parasympathetic) root: It is derived from nerve to inferior oblique and consists of preganglionic parasympathetic fibres from Edinger–Westphal nucleus. These fibres relay in the ganglion. The postganglionic parasympathetic fibres arise from the cells of the ganglion and pass through short ciliary nerves to supply the ciliary muscle and sphincter pupillae.
2. Sensory root: It is derived from nasociliary nerve. It consists of sensory fibres (for pain, touch, and temperature) from eyeball, which pass through the ciliary ganglion without relay.
3. Sympathetic root: It is derived from sympathetic plexus around internal carotid artery. It consists of post-ganglionic sympathetic fibres from superior cervical sympathetic ganglion. The fibres pass through the ganglion without relay and further pass through short ciliary nerves to supply the dilator pupillae and blood vessels of the eyeball.
The branches of ciliary ganglion are short ciliary nerves (8–10). They contain fibres from all the three roots, run above and below the optic nerve towards the eyeball. On reaching the eyeball they pierce the sclera around the attachment of the optic nerve and pass forwards in the space between the sclera and choroid to reach the target organs.
Infraorbital and Zygomatic Nerves (Fig. 19.16)
They lie outside the periosteum of the orbit. They are described in detail in ![]() Chapter 10.
Chapter 10.

OPHTHALMIC ARTERY
It is branch of the internal carotid artery. It arises from internal carotid artery as it emerges from the roof of the cavernous sinus medial to anterior clinoid process close to the optic canal. The artery enters the orbit through optic canal inferolateral to the optic nerve, both lying in a common dural sheath (Fig. 19.17).

The artery pierces the dura mater, ascends over the lateral side of the optic nerve to cross it superiorly from lateral to medial side along with the nasociliary nerve. It then runs forwards along the medial wall of the orbit tortuously to allow the movements of the eyeball. Near the medial angle of the eye it terminates by dividing into two branches: supratrochlear and dorsal nasal.
The branches of the ophthalmic artery are as follows:
1. Central artery of the retina (first and most important) arises from ophthalmic artery (still in dural sheath) below the optic nerve, runs forwards in the dural sheath and pierces the optic nerve inferomedially about 1.25 cm behind the eyeball. The central artery reaches the optic disc through the central part of the nerve. It supplies the optic nerve and inner 6/7 layers of the retina.
2. Lacrimal artery arises from ophthalmic artery just before it crosses the optic nerve. It passes forwards along the upper border of lateral rectus and supplies the lacrimal gland, eyelids, and conjunctiva. The lacrimal artery gives off the following branches:
(a) Glandular branches to lacrimal gland.
(b) Two lateral palpebral arteries—one to each eyelid.
(c) Two zygomatic branches: zygomaticofacial and zygomaticotemporal.
(d) Recurrent meningeal branch runs backwards to enter the middle cranial fossa through the superior orbital fissure.
3. Posterior ciliary arteries consist of two sets: long and short, both of which pierce the sclera of the eyeball around the optic nerve and chiefly supply the choroid and sclera. Long ciliary arteries are usually two and short ciliary arteries are usually seven in number. (Remember that anterior ciliary arteries arise from muscular arteries.)
4. Supraorbital artery accompanies the supraorbital nerve. It passes through supraorbital notch to enter the scalp and divides into medial and lateral branches.
5. Posterior ethmoidal artery enters the posterior ethmoidal foramen in the medial wall of the orbit and supplies the ethmoidal air sinuses, nasal cavity, and dura mater.
6. Anterior ethmoidal artery enters the anterior ethmoid foramen in the medial wall of the orbit and supplies the ethmoidal air sinuses, medial and lateral wall of nasal cavity, and dura mater.
7. Dorsal (external) nasal artery supplies the lower part of the dorsum of nose.
8. Supratrochlear artery accompanies the supratrochlear nerve to supply the forehead.
9. Medial palpebral branches, one to each eyelid, anastomose with the corresponding lateral palpebral branches of the lacrimal artery.
N.B. Branches of ophthalmic artery accompany all the branches of nasociliary frontal and lacrimal nerves (derived from ophthalmic nerve), and within the orbit supply all the extraocular muscles, lacrimal gland, and the eyeball.
OPHTHALMIC VEINS
The ophthalmic veins drain the orbit and receive tributaries, which correspond to the branches of the ophthalmic artery (Fig. 19.18). The ophthalmic veins are as follows:

1. Superior ophthalmic vein: It is a large vein and accompanies the ophthalmic artery. It commences above the medial palpebral ligament and runs backwards above the optic nerve along with the ophthalmic artery, passes through the superior orbital fissure to drain into cavernous sinus.
It communicates anteriorly at its commencement with the supraorbital and angular veins.
2. Inferior ophthalmic vein: It runs below the optic nerve and ends either by joining the superior ophthalmic vein or drain directly into the cavernous sinus.
It communicates with pterygoid venous plexus by small veins passing through the inferior orbital fissure.
LACRIMAL GLAND
It is a tubulo-acinar type of exocrine gland, which secretes watery lacrimal fluid. It consists of two parts: orbital and palpebral. The orbital part is located in the lacrimal fossa on the anterolateral part of the roof of the orbit, while palpebral part is located in lateral part of the upper eyelid. Lacrimal gland has already been described in detail in ![]() Chapter 3.
Chapter 3.
EYEBALL (BULBUS OCULI)
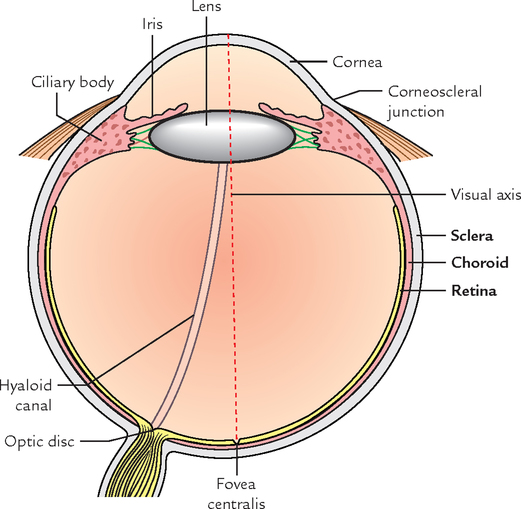
The eyeball (L. oculus; Gk. ophthalmos) or globe of the eye is an organ of sight and closely resembles a camera in its structure. It has light-sensitive retina and is provided with a lens system (cornea, lens, and refractive media) for focusing images and device for controlling the amount of light admitted (the iris diaphragm). Further, like a camera, its inside is black to prevent reflection of light (Fig. 19.19).
The eyeball is a highly durable structure for its wall enclosing the refractory media, is made up of three coats, and the fluid filled within it distributes hydraulic pressure uniformly to maintain its shape.
TUNICS OF THE EYEBALL
The eyeball consists of three concentric coats (Fig. 19.19), viz.
1. An outer fibrous coat consisting of sclera and cornea.
2. A middle vascular coat consisting of choroid, ciliary body, and iris.
OUTER FIBROUS COAT OF THE EYEBALL
Sclera
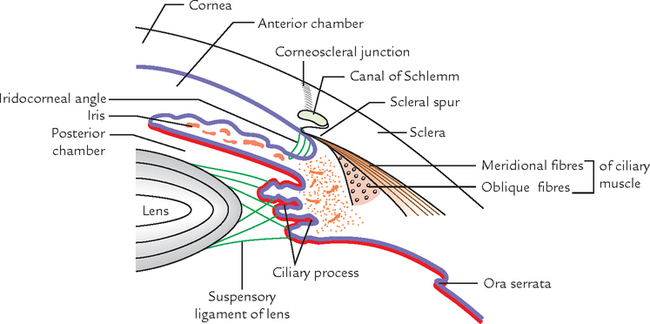
The sclera is the posterior five-sixth of the outer coat. It consists of dense fibrous tissue. It is opaque and a small portion of it is seen as the white of the eye in the palpebral fissure. The sclera is continuous anteriorly with the cornea. The junction between the sclera and cornea is termed corneoscleral junction. Just behind the corneoscleral junction, within the sclera is a circularly running canal called sinus venosus sclerae (canal of Schlemm). Posterior to the canal is a triangular projection—the scleral spur—which points forwards and inwards and provides attachment to the ciliary muscle (Fig. 19.20). It is thinnest at the equator and thickest at the back but weakest at the site of emergence of optic nerve.
Structure Piercing the Sclera
1. Optic nerve pierces the sclera, a little inferomedial to the posterior pole of the eyeball. The perforating fibres of nerve make the area sieve-like (hence called lamina cribrosa).
2. Posterior ciliary vessels and nerves around the optic nerve.
3. Anterior ciliary arteries pierce the sclera close to corneoscleral junction.
4. Four choroidal veins (also called venae vorticosae) pierce the sclera, just behind the equator.
Cornea
The cornea is the anterior one-sixth of the outer coat. It bulges forwards from the sclera at the corneoscleral junction called
limbus. It is transparent and more convex than sclera because it represents the segment of a smaller sphere. Its thickness is about 1 mm at the periphery and 0.5 mm at the centre.
Features
1. It is avascular and nourished by permeation of nutrients from loops of capillaries at the limbus, aqueous humour, and lacrimal fluid.
2. It not only permits the light to enter the eye but also reflects the entering light.
3. It is highly sensitive and supplied by the ophthalmic division of trigeminal nerve.
4. The nerves of cornea form the afferent limb of the corneal reflex (closure of the eyelids on stimulation of the cornea).
Structure
It consists of five layers, from outside inwards these are as follows (Fig. 19.21):

1. Corneal epithelium: It consists of non-keratinized stratified squamous epithelium.
2. Anterior limiting membrane (or Bowman’s membrane): It is made up structureless homogeneous mass without any elastic fibres.
3. Substantia propria (corneal stroma): It is made up of about 200–250 lamellae of fine collagen fibres, which cross each other at right angles to form corneal spaces.
Flattened fibroblasts are located between the lamellae.
The transparency of cornea is due to precise lattice arrangement of its lamellae embedded in the ground substance.
4. Posterior limiting membrane/Descemet’s membrane: It is made up of structureless homogeneous mass containing elastic fibres.
5. Endothelium: It consists of a single layer of low cuboidal cells.
MIDDLE VASCULAR COAT OF THE EYEBALL
The middle coat is often called vascular coat because it contains most of the blood vessels of the eyeball. It is frequently known as uveal tract by the clinicians. This coat also contains a large number of melanin-containing cells. It consists of three parts; from behind forwards these are: choroid, ciliary body, and iris. These three parts together form uvea or uveal tract.
Choroid
The choroid is the posterior part of the vascular coat of the eyeball. It is brown, thin, and highly vascular membrane lining the inner surface of the sclera. Anteriorly, it is connected to the iris by the ciliary body and posteriorly, it is pierced by the optic nerve.
Arteries: They are derived from short ciliary arteries, which pierce the sclera around the optic nerve.
Veins: They are arranged in the form of whorls, which converge to form the 4 or 5 venae vorticosae, which pierce the sclera just behind the equator to open into the ophthalmic veins.
N.B. The inner surface of the choroid is firmly attached to the retina and nourishes the rods and cones of the retina by diffusion.
Structure
It consists of four layers (from outside inwards), viz.
1. Suprachoroid lamina (lamina fusca): It consists of loose network of elastic and collagen fibres and is traversed by long posterior ciliary vessels and nerves.
2. Vascular lamina: It consists of loose areolar tissue and pigment cells. It contains branches of short posterior ciliary arteries and veins, which converge in whorls to form 4 or 5 venae vorticosae, which pierce the sclera and drain into ophthalmic veins.
3. Capillary lamina (capillary layer of choroid): It consists of fine network of capillaries, which nourish photoreceptors of the retina (rods and cones) by diffusion.
4. Basal lamina (membrane of Bruch): It is a thin transparent membrane, which is firmly attached to the pigment cell layer of the retina.
The last three layers form the choroid proper, which is separated from sclera by suprachoroid lamina.
N.B. In some animals such as cat, tiger, lion, etc. the specialized cells of choroid form a reflecting media called tapetum, which produces greenish glare in the eyes of these animals in the night.
Ciliary Body
The ciliary body is the thickening in the vascular tunic. It is continuous with the choroid behind and the iris in front. It is situated posterior to the corneoscleral junction in front of the ora serrata of the retina.
The ciliary bodies suspend the lens via suspensory ligaments.
Parts of the Ciliary Body
The ciliary body is triangular in cross section, thick in front and thin behind. The ciliary body consists of (a) ciliary ring, (b) ciliary processes, and (c) ciliary muscle.
Ciliary ring is an outer fibrous ring, which is continuous with the choroid, viz.
Ciliary processes are a group of 60–90 folds on the inner aspect of the ciliary body. They are arranged radially between the ciliary ring and the iris. The grooves between the processes provide attachment to the fibres of suspensory ligament of the lens.
The ciliary processes are a complex of capillaries and cuboidal epithelium, which secretes aqueous humour. The ciliary processes may be compared with choroidal plexus of the brain ventricles involved in the secretion of CSF.
The ciliary muscle is a small unstriped (smooth) muscle mass consisting of mainly two types of fibres, viz.
Functions
Its main function is to focus the lens for near vision. The ciliary muscle as a whole acts as a sphincter, therefore, when its muscle fibres, both radial and circular contract, the choroid is pulled towards the lens reducing the tension on the suspensory ligaments. This allows the lens to assume a more spherical form because of its own elastic nature. Now lens can cause more refraction needed for accommodation.
Iris
The iris is a contractile diaphragm between the cornea and the lens. An opening in its centre is called the pupil. The iris is attached at its periphery to the middle of the anterior surface of the ciliary body. Peripheral to this attachment the ciliary body and narrow rim of sclera form the iridocorneal angle.
Structure
The iris consists of four layers; from before backwards, these are as follows:
1. An anterior mesothelial lining.
2. A connective tissue stroma containing pigment cells and blood vessels.
3. A layer of smooth muscle, which consists of two parts.
(a) Constrictor pupillae—an inner (near the margin of the pupil) part made of circular fibres.
(b) Dilator pupillae—a peripheral part made up of radial fibres.
Nerve supply: Constrictor pupillae is supplied by the parasympathetic fibres and dilator pupillae by the sympathetic fibres.
Actions: The constrictor and dilator pupillae constricts and dilates the pupil, respectively.
4. A posterior layer of pigment cells, which is continuous with the ciliary part of the retina.
INNER NERVOUS COAT OF THE EYEBALL (RETINA)
The retina is the innermost coat of the eyeball (Fig. 19.22). It consists of two layers, viz.

The space between the two layers contains a gummy substance that glues the two layers.
The retina is present between the choroid and the hyaloid membrane of the vitreous. The retina diminishes in thickness from behind forwards. Anteriorly, it presents an irregular edge called ora serrata.
Structure
1. The outer layer of the retina is insensitive to light and made up of pigmented cuboidal epithelium.
2. The inner sensory layer of the retina is sensitive to light and is made up of photoreceptors cells called rods and cones; as well as numerous relay neurons, viz. bipolar neurons and ganglion cells. The very thin non-cellular continuation of the retina in front of the ora serrata covers the ciliary body and iris. Thus the photosensitive part of the retina lines the inner surface of the eyeball posterior to the ciliary body. The nerve fibres arising from its ganglion cells covers inner surface and collect in the inferomedial region, where they pierce the outer two coats of eyeball and emerge as the optic nerve.
N.B. Histologically, the retina is composed of following 10 layers:
Development of the Retina (Fig. 19.23)
The retina develops from a hollow outgrowth the optic vesicle from diencephalon of primitive brain. The optic vesicle becomes invaginated to form the optic cup, consisting of two layers of cells. The outer layer differentiates to form the pigment cell layer and the inner layer differentiates to form the neural layer. The neural layer forms the remaining layers of the retina with photoreceptor cell (rods and cones) outermost, i.e., next to pigment cells. The ganglion cells are innermost. Therefore light has to pass through them to stimulate the rods and cones.

The two layers of optic cup remain separate during embryonic period but fuse later during early fetal period with potential space between the two. Therefore in retinal detachment, the plane of cleavage is between pigment cell layer and neural layer.
• Retinal detachment: In retinal detachment there is separation of two layers of the retina (i.e., pigment and neural layers).
• Appearance of the retina as seen through an ophthalmoscope: The posterior region of retina (fundus) can be examined by an ophthalmoscope, a procedure called fundoscopy (funduscopic examination). The following features are observed (Fig. 19.24):

– Macula lutea, a pale yellowish area near the posterior pole.
It is approximately 4 mm in diameter. A small pit (1.5 mm in diameter) in its center is called fovea centralis, which is the point where light is normally focused.
The fovea is the portion of retina with maximum concentration of cone receptors, hence the site of greatest visual acuity, i.e., the ability to see the fine images (keenest vision).
– Optic disc (1.5 mm in diameter), a white spot about 3 mm medial to the macula. The depressed area in the center is called physiological cup.
The nerve fibres from retina meet and pass through this region (optic disc) of the eyeball to form the optic nerve. The blood vessels of retina also pass through this spot.
Since there are no photoreceptor cells in the optic disc, it does not respond to the light. Therefore, the optic disc is also called blind spot.
– The central artery of the retina enters the eye through the center of the optic disc. It divides into superior and inferior branches. Each of them further divides into temporal and nasal branches. The retinal veins follow the arteries. The branches of the central artery of retina are seen radiating over the edges of the optic disc. They are smaller and paler than veins. At points where they cross veins, the vein wall can be seen through the artery.
The normal optic disc appears as a cup-shaped area paler than the surrounding area (fundus). The edges of the disc are sharp and well-defined.
The congestion of the optic disc from increased intracranial pressure is called papilledema in which the optic cup is obscured and the disc margin is blurred.
N.B. The fovea centralis is the thinnest part of retina and its size is comparable to optic disc.
ARTERIAL SUPPLY OF THE EYEBALL
The eyeball is supplied by the following arteries (Fig. 19.25):

In the region of ciliary body, a major arterial circle is formed by the anastomosis between long posterior ciliary artery and anterior ciliary artery. From major arterial circle the vessel passes centripetally and anastomoses close to the pupillary margin to form the minor arterial circle.
COMPARTMENTS OF THE EYEBALL
The interior of the eyeball is divided into two compartments by the lens: a small anterior compartment in front of the lens and a large posterior compartment behind the lens (Fig. 19.26):

1. Anterior compartment: It is divided into two chambers: a smaller anterior chamber and a larger posterior chamber.
The anterior chamber lies between the iris and cornea and posterior chamber between iris and lens. The two compartments communicate with each other through pupil.
The two chambers are filled with an aqueous humour, which helps in maintaining the intraocular pressure. The aqueous humour is rich in ascorbic acid, glucose, and amino acids. It nourishes the cornea and the lens which are otherwise avascular.
Circulation of aqueous humour: The aqueous humour is secreted in the posterior chamber by the ciliary processes. From here it passes into the anterior chamber through the pupil. Here it passes through the spaces in the iridocorneal angle, located between the fibres of ligamentum pectinatum and then enter into the canal of Schlemm, from where it is drained by the anterior ciliary veins.
2. Posterior compartment: It is behind the lens and much larger than the anterior compartment (comprising four-fifth of the eyeball). It is surrounded almost completely by the retina and is filled with colorless, transparent jelly-like substance called vitreous humour/vitreous body. The vitreous humour is enclosed in a delicate hyaloid membrane. Anteriorly, the hyaloid membrane forms a depression the hyaloid fossa in which rests the lens. The vitreous humour helps in maintaining intraocular pressure and therefore the shape of the eyeball. Further, it holds the lens and the retina in place. The hyaloid canal extends from optic disc to the lens. The canal marks the site of the hyaloid artery in the fetus. The hyaloid artery is a continuation of central artery of the retina which disappears 6 weeks before birth.
LENS
The lens is an unusual biological structure. It is a transparent, biconvex body, 1 cm in diameter and 4 mm thick, placed between the anterior and posterior compartments of the eyeball.
Structure
The lens is enclosed in a transparent elastic capsule. Anteriorly deep to capsule lies capsular epithelium. In the center, the epithelium is made up of a single layer of cuboidal cells. The cells at periphery prolongate to give rise to lens fibres. These fibres get arranged concentrically and form the lens substance. The center (nucleus) of the lens consists of oldest fibres. Here the lens fibres lose their nuclei and organelles. As a result, a special set of proteins called crystallines lie in the center. The center of the lens is, therefore, hard. The periphery of the lens (cortex) is soft because it is made up of more recently formed fibres.
FUNCTIONS OF THE EYE
The main function of the eye is focusing of light waves and stimulation of photoreceptors of the retina. This requires five basic processes, viz.
1. Transmission of light waves through transparent media of the eyeball.
2. Refraction (bending) of light waves through different refractive media of different densities.
3. Accommodation of the lens to focus the light waves.
4. Regulation of amount of light entering the eye through pupil by iris diaphragm.
The stimulation of photoreceptors of retina generates action potentials that are relayed through the optic pathways to the visual cortex of the brain, where image is formed. The visual impairment may result if any one or more of these processes fail to function properly.
REFRACTIVE MEDIA OF THE EYE
All these media together form the refractive apparatus of the eye.
N.B. Most of the refraction by eye takes place at the anterior surface of the cornea (not in the lens as generally thought).
 Most important content of the orbit Most important content of the orbit |
Eyeball |
| All structures within the orbit lie inside the orbital periosteum except |
Infraorbital nerve and vessels and zygomatic nerve, which lie outside the orbital periosteum |
| White of the eye |
Sclera |
| Uvea (or uveal tract) |
Consists of choroid, ciliary body, and iris |
| Weakest site of sclera |
Lamina cribrosa |
| Site of keenest vision in retina |
Fovea centralis |
| Blind spot of the retina |
Optic disc |
| Maximum refraction by the eye takes place at |
Anterior surface of the cornea |
| Most successful homotransplant (i.e., between the individuals of the same species) |
Corneal transplant |
| Most important branch of ophthalmic artery |
Central artery of the retina |
| All the extraocular muscles are supplied by the oculomotor nerve except |
Lateral rectus (supplied by the abducent nerve) and superior oblique (supplied by the trochlear nerve) |
| Canal of Schlemm |
Circular vascular channel within sclera just behind the corneoscleral junction |
| Refractive apparatus of the eye |
Consists of cornea, aqueous humour, lens, and vitreous humour |
| Tenon’s capsule |
Thin membranous sheath enclosing the eyeball |
| Most common of all eye operations |
Cataract extraction |


A 66-year-old person visited his family physician and complained of headache and blurring of vision. He referred him to an ophthalmologist, who on ophthalmoscopic examination found papilledema (edema of optic discs) and congestion of retinal veins. CT scan of his head revealed a large intracranial tumor in the region of the posterior cranial fossa.
1. The optic disc is a white spot (or plate area) about 3 mm medial to the posterior pole of eye—seen on ophthalmoscopic examination. The nerve fibres from retina leave the eyeball at this site to become the optic nerve. This area is devoid of photoreceptor cells. The central artery of retina enters and tributaries of central vein of retina leave the eyeball through the centre of the optic disc. The region of optic disc does not respond to light due to absence of photoreceptor cells (rods and cones), hence it is also called the blind spot.
2. The optic nerve and retina develop from optic stalk and optic cup, respectively. The optic stalk and optic cup are derived from diencephalon as hollow outgrowth. The optic nerve being derived from brain is surrounded by three meninges.
3. The optic nerve is surrounded by three meninges of the brain, up to its entry in the eyeball, and the subarachnoid space filled with CSF is continuous with subarachnoid space around the brain. As a result, rise in intracranial pressure (and hence CSF pressure) due to intracranial tumor, the central vein of retina traversing the subarachnoid space around optic nerve is compressed. This leads to venous congestion and edema of the optic disc called papilledema.