Infratemporal Fossa, Temporomandibular Joint, and Pterygo-palatine Fossa
INFRATEMPORAL FOSSA
The infratemporal fossa is the space beneath the base of the skull, between the side wall of the pharynx and ramus of the mandible. It communicates with the temporal fossa through a gap deep to the zygomatic arch. It is also referred to as the parapharyngeal space or lateral pharyngeal space.
BOUNDARIES
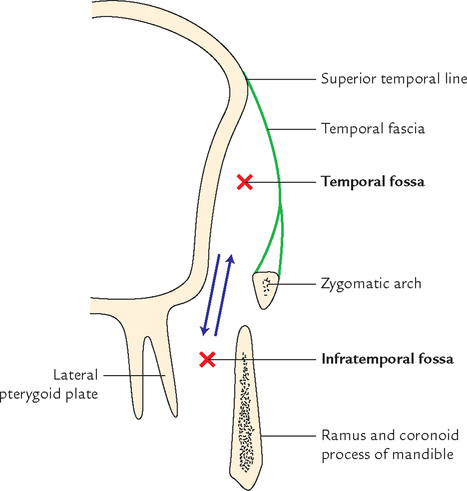
The boundaries of infratemporal fossa (Fig. 10.1) are:

| Roof: | Formed by the infratemporal surface of the greater wing of the sphenoid. It is pierced by foramen spinosum and foramen ovale. |
| Medial wall: | Formed by lateral surface of the lateral pterygoid plate of the sphenoid. It is separated from the anterior wall by pterygomaxillary fissure. |
| Lateral wall: | Formed by the ramus of the mandible. |
| Anterior wall: | Formed by the infratemporal surface of the maxilla. It is separated from roof by inferior orbital fissure. |
| Floor: | Open and extends up to the level of the base of the mandible. |
| Posterior wall: | Formed by styloid process of the temporal bone. |
COMMUNICATIONS (Figs 10.2 and 10.3)
The infratemporal fossa communicates:

(a) above with the temporal fossa through a gap, deep to zygomatic arch; and middle cranial fossa through foramen ovale and foramen spinosum,
(b) below it is continuous with the tissue spaces of the neck lateral to the pharynx,
(c) with the pterygopalatine fossa through pterygomaxillary fissure, and
All communications are presented in Flowchart 10.1.

N.B. The infratemporal fossa can be best visualized as a hollow cube without floor (Fig. 10.3).
MUSCLES
Lateral Pterygoid (Fig. 10.4)
It is a short, thick conical muscle with its apex pointing backwards. It passes backwards and slightly laterally from the roof and medial wall of the fossa to the neck of the mandible.

1. Lateral pterygoids of two sides depress the mandible (opens the mouth) by pulling forward the condylar processes of the mandible and the articular discs of the temporomandibular joints.
2. Lateral and medial pterygoid muscles of two sides acting together protrude the mandible.
3. Lateral and medial pterygoid muscles of the two sides contract alternately to produce side-to-side movements of the lower jaw as in chewing.
Relations (Fig. 10.5)
The lateral pterygoid is regarded as the key muscle of the infratemporal region because its relations provide a fair idea about the layout of structures in this region. Its relations are:

4. Superficial head of medial pterygoid.
5. Maxillary artery and its temporal and masseteric branches.
Structures emerging at the upper border:
Medial Pterygoid (Fig. 10.6)
The medial pterygoid is a thick quadrilateral muscle and consists of two heads: superficial and deep.

1. The small superficial head (a small slip of muscle) arises from maxillary tuberosity and lateral surface of the pyramidal process of palatine bone.
2. The large deep head (forming the bulk of muscle) arises from medial surface of the lateral pterygoid plate and grooved surface of the pyramidal process of palatine bone.
The fibres run downwards, backwards, and laterally to be inserted by a strong tendinous lamina into a roughened area on the posteroinferior part of the medial surface and angle of ramus of mandible as high as the mandibular foramen and as forwards as the mylohyoid groove (![]() Fig. 9.11).
Fig. 9.11).
Superficial (Fig. 10.7):

1. Medial pterygoids of two sides elevate the mandible to help in closing of mouth.
2. Acting with lateral pterygoids, the medial pterygoids protrude the mandible.
3. When medial and lateral pterygoids of one side act together, the corresponding side of the mandible is rotated forwards and to the opposite side.
4. Lateral and medial pterygoids of two sides when contract alternately produce side-to-side movements, which are used to grind the food.
BLOOD VESSELS
MAXILLARY ARTERY (Figs 10.7 and 10.8)
The maxillary artery is the larger terminal branch of the external carotid artery.

It arises behind the neck of the mandible, runs horizontally forward up to the lower border of lower head of lateral pterygoid. Now it turns upwards and forwards, crosses the lower head of lateral pterygoid superficially (sometimes deep). After emerging between the two heads of lateral pterygoid it enters the pterygopalatine fossa by passing through pterygomaxillary fissure. Here it ends by giving its terminal branches.
The maxillary artery has a wide territory of distribution. It supplies:
(b) muscles of temporal and infratemporal fossae,
(c) nose and paranasal sinuses,
(d) palate and roof of pharynx,
N.B. The maxillary artery enters the infratemporal fossa by passing forwards, between the neck of mandible and the sphenomandibular ligament.
Parts and Relations
The maxillary artery is divided into three parts by the lower head of lateral pterygoid muscle. The parts are:
1. First part (mandibular part): From beginning (origin) to lower border of lateral pterygoid. It lies between the neck of the mandible laterally and sphenomandibular ligament medially. The auriculotemporal nerve lies above this part.
2. Second part (pterygoid part): From lower border to the upper border of the lower head of lateral pterygoid (i.e., second part lies on or deep to lower head of lateral pterygoid).
3. Third part (pterygopalatine part): From upper border of the lower head of lateral pterygoid to pterygopalatine fossa. In pterygopalatine fossa it lies in front of the pterygopalatine ganglion.
• Most of the branches from the first and second parts of maxillary artery accompany the branches of the mandibular nerve.
• Branches from the third part of the maxillary artery accompany the branches of maxillary nerve and pterygopalatine ganglion.
• Branches from the second part of the maxillary artery are muscular only and supply muscles of mastication.
• All the branches (1st and 3rd part) of the maxillary artery pass through bony foramina and fissures except branches from its second part.
Branches of the Maxillary Artery (Fig. 10.8)
I Branches from the First Part (Five Branches)
1. Deep auricular artery—passes upwards and backwards to enter the external acoustic meatus by piercing its floor and supplies:
2. Anterior tympanic artery—enters the tympanic cavity by passing through petrotympanic fissure and it supplies the inner surface of the tympanic membrane.
3. Middle meningeal artery—is the largest meningeal branch. It supplies meninges as well as the skull bone.
Clinically it is the most important branch of the maxillary artery.
The middle meningeal artery arises from the first part of the maxillary artery. It ascends upwards deep to the lateral pterygoid, behind the mandibular nerve. Passing between the two roots of the auriculotemporal nerve, to enter the cranial cavity through foramen spinosum in company with meningeal branch of mandibular nerve (nervus spinosus).
As it emerges in the cranial cavity, it courses laterally on the floor of the middle cranial fossa and turns upwards and forwards on the greater wing of the sphenoid, where it divides into frontal and parietal branches:
(a) Frontal (anterior) branch, courses up towards the pterion and then curves backwards to ascend towards the vertex, lying over the precentral gyrus of the cerebral hemisphere. In the region of pterion the artery frequently lies in a bony tunnel in the parietal bone for a centimeter or more.
(b) Parietal (posterior) branches arch backwards on the squamous part of the temporal bone, cross the lower border of the parietal bone in front of its mastoid angle; here it divides into branches, which spread out as far as lambda. It lies along the superior temporal gyrus.
Distribution: The middle meningeal artery and its branches lie outside the dura and deep to the inner surface of the skull. Both of these are supplied by the artery.
N.B. The middle meningeal artery and its branches are accompanied by corresponding veins, which lie between the artery and the bone.
4. Accessory middle meningeal artery—runs upwards and enters the cranial cavity through foramen ovale.
It supplies meninges and structures in the infratemporal fossa.
5. Inferior alveolar/dental artery—runs downwards between the sphenomandibular ligament and the ramus of the mandible, enters the mandibular foramen, runs through the mandibular canal, supplies molar and premolar teeth and adjoining gum. It then divides into mental and incisive branches.
The incisive branch supplies the canine and incisor teeth. The mental artery emerges through the mental foramen to supply the skin of the chin. Before entering the mandibular foramen the inferior alveolar artery gives off two branches, namely,
II Branches from the Second Part (Four Branches)
1. Deep temporal arteries (usually two in number)—ascend up on the lateral aspect of the skull deep to the temporalis muscle, which they supply.
2. Pterygoid branches—supply the medial and lateral pterygoid muscles.
3. Masseteric artery—passes laterally through the mandibular notch and supplies the masseter muscle from its deep surface.
III Branches from the Third Part (Six Branches)
1. Posterior superior alveolar artery arises from maxillary artery just before it enters the pterygomaxillary fissure. It divides into two or three branches, which enter the foramina on the posterior surface of the body of maxilla, runs into alveolar canals and supply the molar and premolar teeth and mucus membrane of maxillary air sinus.
2. Infraorbital artery also arises from maxillary artery just before it reaches the pterygopalatine fossa. The artery passes successively through inferior orbital fissure, infraorbital groove, and infraorbital canal, and appears on the face through the infraorbital foramen. It gives the following branches:
(a) Branches to orbital contents.
(b) Middle superior alveolar artery to premolar teeth.
(c) Anterior superior alveolar artery, which descends through canaliculus sinuosus in the anterior wall of the maxillary sinus. It supplies the maxillary air sinus, and canine and incisor teeth of the upper jaw. In the face, It gives off branches to supply the lacrimal sac, medial angle of the eye, side of nose, and upper lip.
3. Greater palatine artery passes downwards in the greater palatine canal and appears in the oral cavity at the posterolateral corner of the hard palate through the greater palatine foramen. Now it runs forwards in the groove along the alveolar arch to the incisive fossa where it enters the lateral incisive canal to enter the nasal cavity. It supplies the roof of the mouth and adjoining gum, while in the greater palatine canal the artery gives off lesser palatine arteries that emerge through foramina of the same name and supply the soft palate and tonsil.
4. Pharyngeal artery passes backwards through the palatovaginal canal and supplies the mucus membrane of the nasopharynx, auditory tube, and the sphenoidal air sinus.
5. Artery of pterygoid canal runs backwards in the pterygoid canal and supplies the pharynx, auditory tube, and the tympanic cavity.
6. Sphenopalatine artery is considered as the continuation of the maxillary artery. It is the most important branch of the third part of the maxillary artery. It enters the nasal cavity in the posterior part of the superior meatus through sphenopalatine foramen. Here it divides into:
The posterior lateral nasal branches supply the lateral wall of the nose and sphenoidal and ethmoidal air sinuses, the posterior septal branches cross the undersurface of the body of the sphenoid, and then pass forwards and downwards along the nasal septum. One of the branches of this group is long, runs in a groove on the vomer towards the incisive canal and anastomoses with the terminal branch of the greater palatine artery.
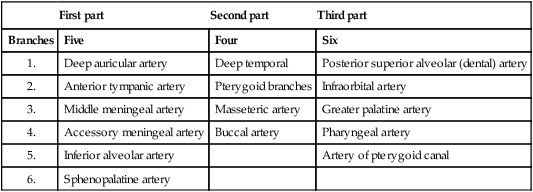
The branches of maxillary artery are summarized in Table 10.1.
Table 10.1
Branches of the maxillary artery
| First part | Second part | Third part | |
| Branches | Five | Four | Six |
| 1. | Deep auricular artery | Deep temporal | Posterior superior alveolar (dental) artery |
| 2. | Anterior tympanic artery | Pterygoid branches | Infraorbital artery |
| 3. | Middle meningeal artery | Masseteric artery | Greater palatine artery |
| 4. | Accessory meningeal artery | Buccal artery | Pharyngeal artery |
| 5. | Inferior alveolar artery | Artery of pterygoid canal | |
| 6. | Sphenopalatine artery |
MAXILLARY VEIN AND PTERYGOID VENOUS PLEXUS
Maxillary Vein
It is a short venous trunk, which accompanies the first part of the maxillary artery. It is formed by the confluence of veins from the pterygoid venous plexus and passes backwards between the sphenomandibular ligament and the neck of the mandible. Within the parotid gland it unites with the superficial temporal vein to form the retromandibular vein.
Pterygoid Venous Plexus
It is a network of very small veins that lie around and within the lateral pterygoid muscle.
The pterygoid venous plexus communicates:
(a) with inferior ophthalmic vein via inferior orbital fissure,
(b) with cavernous sinus by emissary veins via foramen ovale or foramen of Vesalius, and
The plexus is drained by maxillary vein which is formed at the lower border of the lateral pterygoid muscle.
N.B. The pterygoid venous plexus is sometimes referred to as a peripheral heart for during yawning when the mouth is widely open due to contraction of lateral pterygoid muscle, the stagnant venous blood is pumped up into the cavernous sinus and maxillary vein. Possibly this is the reason why people yawn in the morning when they get up from sleep.
NEURAL STRUCTURES
The infratemporal fossa contains the mandibular nerve and its branches, chorda tympani nerve, and otic ganglion.
MANDIBULAR NERVE (Fig. 10.9)
The mandibular nerve is the largest of the three divisions of the trigeminal nerve. It is a mixed nerve, consisting of both sensory and motor fibres. It is a nerve of the first pharyngeal arch, hence supplies all the structures derived from this arch, e.g., muscles of mastication.

Course and Relations
The mandibular nerve is the largest of three divisions of trigeminal nerve. It begins in the middle cranial fossa as two roots: a larger sensory root and a smaller motor root. The large sensory root arises from lateral convex part of the trigeminal ganglion and immediately leaves the cranial cavity by passing through foramen ovale to enter the infratemporal fossa. The small motor root arises from the pons, lies deep to the trigeminal ganglion and the sensory root. It also passes through foramen ovale to join the sensory root just below the foramen ovale in the infratemporal fossa, thus forming the main trunk. The mandibular nerve trunk is short and after a short course divides into a small anterior and large posterior division.
Branches
From the Main Trunk
Two branches arise from the main trunk, a sensory branch (nervus spinosus) and a motor branch (nerve to medial pterygoid):
1. Nervus spinosus (meningeal branch): It takes a recurrent course to enter the cranial cavity through foramen spinosum with middle meningeal artery and supplies the dura mater of the middle cranial fossa.
2. Nerve to medial pterygoid: It arises from the medial aspect of the main trunk, close to the otic ganglion traverses through the ganglion and supplies the medial pterygoid from its deep aspect. In addition to medial pterygoid it also supplies tensor palati and tensor tympani muscles.
From the Anterior Division
The anterior division is mainly motor and gives branches to all muscles of mastication except medial pterygoid, which is supplied by nerve to medial pterygoid from the main trunk. The branches from the anterior divisions are as follows:
1. Masseteric nerve: It emerges at the upper border of the lateral pterygoid, just in front of the temporomandibular joint, passes laterally through the mandibular notch, along with masseteric artery to supply the masseter from its deeper aspect. It also supplies the temporomandibular joint.
2. Deep temporal nerves: These are usually two in number, anterior and posterior. The anterior and posterior temporal nerves emerge at the upper border of the lateral pterygoid and ascend up in the temporal fossa to supply the temporalis muscle from its deep aspect.
3. Nerve to lateral pterygoid: It runs with the buccal nerve and enters the deep surfaces of both the heads of lateral pterygoid muscle, which it supplies.
4. Buccal nerve: It contains all the sensory fibres of the anterior division. It emerges between the two heads of the lateral pterygoid and courses downwards and forwards onto the buccinator muscle, giving branches to the skin of the cheek. It then pierces the buccinator muscle and supplies the mucus membrane of the cheek and gum of the lower jaw opposite the molars and second premolar teeth.
N.B. All the branches of anterior division of the mandibular nerve are motor except buccal nerve which is sensory.
From the Posterior Division
The posterior division is mainly sensory. It gives the following three branches:
1. Auriculotemporal nerve: This nerve arises by two roots, which after encircling the middle meningeal artery unite to form the single trunk. It runs backwards between the neck of the mandible and the sphenomandibular ligament. Behind the neck of the mandible, it turns upwards and ascends over the root of zygoma to enter the temple behind the superficial temporal vessels.
(a) Its auricular branches supply skin of the tragus, upper part of the pinna, external auditory meatus and tympanic membrane. The lower parts of these regions are supplied by great auricular nerve and auricular branch of the vagus nerve.
(b) Its articular branches supply the temporomandibular joint.
(c) Its superficial temporal branches supply the skin of the temple.
(d) It also supplies secretomotor fibres to the parotid gland.
2. Lingual nerve: It is the smaller terminal branch of posterior division of the mandibular nerve. It is sensory to the mucus membrane of anterior two-third of the tongue except vallate papillae.
Course and relations: It begins about 1 cm below the skull. It runs first between tensor palati and lateral pterygoid and then between lateral and medial pterygoids. About 2 cm below the skull it is joined by the chorda tympani nerve. After emerging at the lower border of the lateral pterygoid, it first run downwards and forwards between the ramus of the mandible and medial pterygoid, comes in direct contact with the mandible where the bone is thinned to form a shallow groove below and medial to the last molar tooth, just above the posterior end of the mylohyoid line. This groove separates the attachments of pterygomandibular raphe above and mylohyoid muscle below. It enters the mouth on the superior surface of the mylohyoid, and then it crosses the styloglossus to reach the lateral surface of the hyoglossus. Finally it lies on the surface of the genioglossus. Here it winds round the submandibular duct (first above, then lateral, then below and finally medial to the duct) and divides into its terminal branches.
(a) Provides sensory supply to floor of mouth, lingual surface of the gum and anterior two-third of the tongue;
(b) Carries preganglionic secretomotor fibres to submandibular and sublingual salivary glands.
3. Inferior alveolar nerve: It is the larger terminal branch of the posterior division of mandibular nerve. It is a mixed nerve. It receives all the motor fibres of the trigeminal nerve.
Course: It emerges below the lower head of the lateral pterygoid and passes vertically downwards and forward on the medial pterygoid. The nerve lies anterior to inferior alveolar vessels between the sphenomandibular ligament and the ramus of the mandible. Then enters the mandibular foramen in company with inferior alveolar artery, traverses the mandibular canal as far as mental foramen, where it terminates by dividing into mental and incisive branches.
(a) Nerve to mylohyoid arises from the inferior alveolar nerve before it enters the mandibular canal. It pierces the sphenomandibular ligament to reach the mylohyoid groove. It supplies mylohyoid and anterior belly of digastric muscle.
(b) Dental branches supply molar and premolar teeth.
(c) Mental nerve emerges out through mental foramen to supply skin of the chin and skin and mucus membrane of the lower lip.
The branches of the mandibular nerve are summarized in Table 10.2.
Table 10.2
Branches of the mandibular nerve
| From main trunk | From anterior division | From posterior division |
| Nervus spinosus (meningeal branch) | Masseteric nerve | Auriculotemporal nerve |
| Nerve to medial pterygoid | Deep temporal nerves | Lingual nerve |
| Nerve to lateral pterygoid | Inferior alveolar nerve | |
| Buccal nerve |
N.B. All the branches of posterior division of the mandibular nerve are sensory except nerve to mylohyoid, which is motor.
CHORDA TYMPANI NERVE
The chorda tympani nerve is the slender branch of facial nerve. It is so named because of its intimate relationship to the middle ear (tympanum).
Function Components (Fig. 10.10)

Origin, Course, and Relations (Fig. 10.11)
It arises from facial nerve in the facial canal about 6 mm above the stylomastoid foramen, within the posterior wall of the tympanic (middle ear) cavity. It enters the middle ear through the posterior canaliculus of chorda tympani in the posterior wall, runs across the lateral wall (tympanic membrane). Here it crosses medial aspect of handle of malleus and lateral aspect of long process of incus. At the anterior margin of tympanic membrane it enters anterior canaliculus in the anterior wall of the middle ear passes through canaliculus and emerges at the base of skull through medial end of petrotympanic fissure. It then goes medially, forwards and downwards, grooves the medial side of the spine of the sphenoid, running anteroinferiorly deep to lateral pterygoid to join the posterior aspect of the lingual nerve about 2 cm below the base of the skull.

OTIC GANGLION (Fig. 10.12)
It is a small parasympathetic ganglion connected to the mandibular division of trigeminal nerve and provides a relay station to the secretomotor fibres to the parotid gland. Topographically, it is intimately related to the mandibular nerve but functionally it is related to glossopharyngeal nerve.

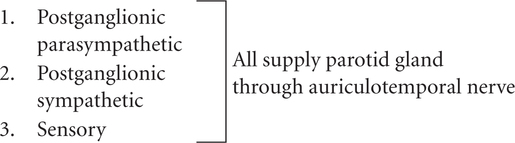
Roots or Connections
1. Parasympathetic motor (secretomotor): From lesser petrosal nerve.
Preganglionic parasympathetic fibres arise from inferior salivatory nucleus; pass successively through glossopharyngeal nerve, tympanic branch of glossopharyngeal nerve (Jacobson’s nerve), tympanic plexus, and lesser petrosal nerve to relay in the ganglion. Postganglionic parasympathetic fibres from ganglion cells pass through auriculo-temporal nerve to supply parotid gland.
2. Sympathetic: From sympathetic plexus around the middle meningeal artery.
Preganglionic sympathetic fibres arise from T1 and T2 spinal segments, enter the cervical sympathetic chain at the level of its inferior ganglion and then ascend to relay in the superior cervical sympathetic ganglion. The postganglionic fibres arise from this ganglion and form plexus around the middle meningeal artery. They then pass through the ganglion without relay to reach the parotid gland via auriculotemporal nerve. They are vasomotor in nature and responsible for thick salivary secretion.
3. Sensory: From auriculotemporal nerve.
4. Somatic motor: Nerve to medial pterygoid. It passes through ganglion to supply medial pterygoid, tensor palati, and tensor tympani muscles.
Branches
• In humans, the chorda tympani nerve is connected to the otic ganglion and nerve to pterygoid canal. These connections provide an alternative pathway of taste sensations from anterior two-third of the tongue.
• Clinical evidence suggests that in humans the parotid gland also receives secretomotor fibres through chorda tympani nerve.
TEMPOROMANDIBULAR JOINT
The temporomandibular joint (TMJ), one on each side of the head, is a joint between temporal bone and mandible that allows the movements of the mandible for speech and mastication.
The mandible is a single bone having two heads, which articulate on each side with temporal bone of cranium. The cranium, with which the mandible articulates, is also, mechanically a single component. The movement cannot take place at one temporomandibular joint without a concomitant movement occurring at the joint on the opposite side. Therefore, temporomandibular joints are the bilateral components of a single craniomandibular articulation/joint. The temporomandibular joints are often involved in various disease processes. Therefore medical students, particularly dental students need to understand the anatomy of TMJ, including movements and disorders associated with the joint.
Type: It is a synovial joint of condylar variety.
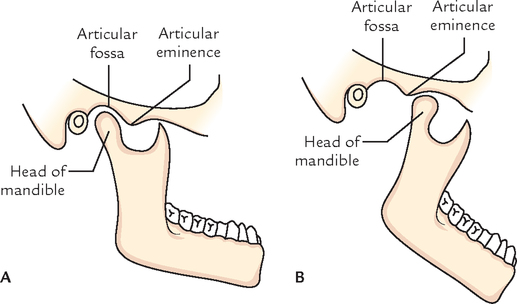
Articular Surface
The upper articular surface is formed by the (a) articular fossa, and (b) articular eminence of the temporal bone. This surface is concavo-convex from behind forwards (Fig. 10.13).

The lower articular surface is formed by the head (condyle) of the mandible. This surface is elliptical in shape.
The articular surfaces are covered by fibrocartilage and not by hyaline cartilage, hence temporomandibular joint is an atypical synovial joint (Fig. 10.13).
JOINT CAVITY (Fig. 10.14)
The cavity of temporomandibular joint is divided into upper menisco-temporal and lower menisco-mandibular compartments by an intra-articular disc of fibrocartilage.

The upper compartment permits gliding movements, whereas lower compartment permits gliding as well as rotational movements.
Articular Disc
The articular disc is an oval plate of fibrocartilage. Though termed fibrocartilage, it consists mainly of collagen fibres with few cartilage cells. It is congruent with both the articular surfaces. Thus its upper surface is concavo-convex (from before backwards) and its inferior surface is concave. The concavo-convex superior surface fits against the articular eminence and the concavity of the articular fossa. The lower concave surface fits with convex head of the mandible.
The periphery of the disc is attached firmly to the fibrous capsule.
The disc has a thick margin, the peripheral annulus and a central depression on its inferior surface. In sagittal section, the disc appears to possess a thin intermediate zone and thickened anterior and posterior bands (Fig. 10.14). The anterior band extends anteriorly through the capsule to be continuous with the tendon of lateral pterygoid. The posterior band splits into two laminae: upper and lower. The upper lamina composed of fibroelastic tissue is attached to the squamotympanic fissure. The lower lamina composed of fibrous non-elastic tissue is attached to the back of the condyle. The bilaminar region contains a venous plexus. The central part of the disc is avascular.
The elastic fibres in the posterior part of the disc bring back the disc in the articular fossa when the open mouth is closed.
N.B. Parts of articular disc (Fig. 10.14): In sagittal section, the articular disc of TMJ presents five different parts, from before backwards these are: (a) anterior extension, (b) anterior thick band, (c) intermediate zone, (d) posterior thick band, and (e) posterior bilaminar zone.
LIGAMENTS
The ligaments are the fibrous capsule, temporomandibular, sphenomandibular, and stylomandibular ligaments. The latter two are accessory ligaments (Fig. 10.15A and B).
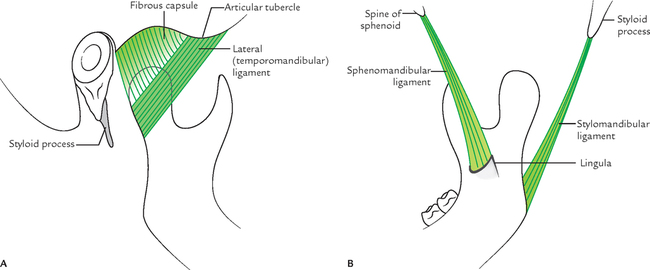
1. Fibrous capsule: It is a fibrous sac to enclose the joint cavity. It is attached above to the articular tubercle, the circumference of articular fossa, and the squamotympanic fissure; and below to the neck of mandible.
The capsule is loose above the intra-articular disc and tight below it.
The synovial membrane lines the inner aspect of the fibrous capsule and the neck of the mandible.
2. Lateral (temporomandibular) ligament: It is a true ligament and formed as a result of thickening on the lateral aspect of the capsular ligament. Its fibres are directed downwards and backwards. It is attached above to the articular tubercle on the root of zygoma and below to the posterolateral aspect of the neck of the mandible. The lateral ligament strengthens the lateral aspect of the capsule.
3. Sphenomandibular ligament: It is attached above to the spine of the sphenoid and below to the lingula and lower margin of the mandibular foramen of the mandible. It lies on a deeper plane away from the joint capsule. The sphenomandibular ligament represents the unossified intermediate part of the sheath of the Meckel’s cartilage of the first pharyngeal arch. It becomes accentuated and taut when the mandible is protruded.
Relations of sphenomandibular ligament (Fig. 10.16A and B) are as under:

Laterally, it is related to: (a) lateral pterygoid muscle, (b) auriculo-temporal nerve, (c) maxillary artery, and (d) inferior alveolar nerve and vessels.
Medially, it is related to: (a) medial pterygoid, (b) chorda tympani nerve and (c) wall of the pharynx.
N.B. Near its lower end the sphenomandibular ligament is pierced by mylohyoid nerve and vessels.
4. Stylomandibular ligament: It is attached above to the lateral surface of the styloid process and below to the angle and adjoining posterior border of the ramus of the mandible.
The stylomandibular ligament is formed due to thickening of the investing layer of deep cervical fascia, which separates the parotid and submandibular glands.
This ligament also becomes taut when the mandible is protruded.
N.B. The accessory ligaments of temporomandibular joints control range of motion (ROM) of TMJs and with mandible form a ’swing’ (Fig. 10.17).

STABILITY
The joint is much more stable when the mouth is closed (i.e., when the teeth are in occlusion) than when the mouth is open. In occlusion, the teeth themselves stabilize the mandible on maxilla and no strain is thrown on the joints when an upward blow is received on the mandible. Further in the occluded position, the forward movement of condyle is discouraged by the articular eminence and by the contraction of the posterior fibres of the temporalis muscle, while the backward movement of the condyle is prevented by the lateral ligament and the contraction of the lateral pterygoid muscle.
MOVEMENTS OF THE MANDIBLE
When the TMJ of two sides are in position of rest a small free space exists between the upper and lower teeth but lips are in contact. The various movements of mandible occur in this position.
The lower jaw can be depressed, elevated, protruded retracted and moved from side-to-side, by movements at temporomandibular joints.
All of the above mentioned movements of lower jaw involve two basic movements, which occur at TMJ, of course with the help of muscles:
The upper menisco-temporal compartment of TMJ permits gliding movements, during protraction (protrusion), retraction, and chewing.
The lower menisco-temporal compartment permits rotation around two axes (a) a transverse axis, during depression and elevation and (b) a vertical axis during side-to-side/chewing movements.
With these two types of movements, gliding and rotation, and with right and left TMJs working together, most of the movements of the lower jaw can be accomplished perfectly as desired. These include opening and closing the jaws and shifting the lower jaw to one side (Fig. 10.18).
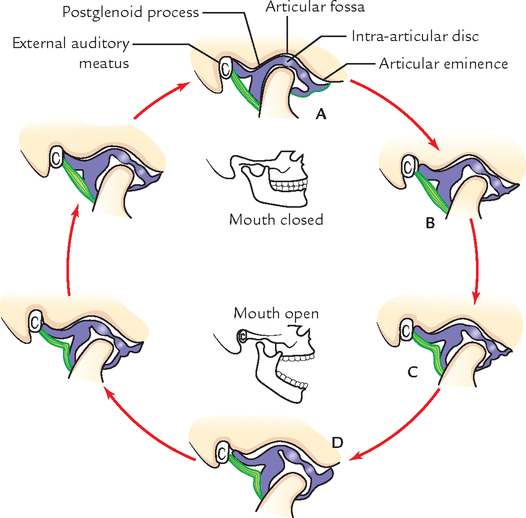
The movements occurring at the temporomandibular joints are:
1. Depression (lowering of jaw to open mouth): During depression, the head of mandible along with an articular disc glide forward in the upper meniscotemporal compartment on both the sides by the contraction of lateral pterygoid muscle. At the same time head rotates forward underneath the articular disc by the contraction of suprahyoid muscles, viz. digastric geniohyoid, and mylohyoid. The gravity also helps in opening the mouth.
2. Elevation (elevating of jaw to close the mouth): During elevation the movements take place in a reverse order to that of depression, i.e., first the head of mandible along with an articular disc glide backward in the upper meniscotemporal compartment by temporalis, masseter, and medial pterygoid, and then head rotates backward on the lower surface of the disc by posterior fibres of temporalis.
3. Protrusion/Protraction: During this movement, mandibular teeth move forward in front of maxillary teeth. In this act, head of mandible along with articular disc glide forwards in the upper meniscotemporal compartment on both sides by simultaneous action of medial and lateral pterygoids of both sides.
4. Retraction: During this movement, the head of mandible along with articular disc glide backwards in the upper meniscotemporal compartment by the contraction of the posterior fibres of temporalis muscle and bring the joint in the resting position. The forceful retraction is assisted by deep fibres of masseter, digastric, and geniohyoid muscles. At the end of this movement the head of the mandible comes to lie underneath the articular tubercle.
5. Side-to-side (Chewing) movements: These movements occur alternately in the right and left temporomandibular joints. In chewing movements, the head of the mandible on one side glides forwards along with the disc (as in protraction), but the head of the mandible on the opposite side merely rotates on the vertical axis. As a result, the chin moves forwards and to one side, i.e., towards the side on which no gliding has taken place.
During this movement, the medial and lateral pterygoids of one side contract alternatively with those of opposite sides.
The alternate movements of this kind on the two sides result in side-to-side movements of the lower jaw.
Muscles Producing Movements
Side-to-side (Chewing) Movements
These movements are performed by alternate contraction of medial and lateral pterygoids on each side.
Movements of the temporomandibular joint and muscles producing them are summarized in Table 10.3.
Table 10.3
Movements of the mandible and muscles producing them
| Movement | Muscle |
| Depression | Lateral pterygoid |
| Digastric | |
| Geniohyoid | |
| Mylohyoid | |
| Gravity | |
| Elevation | Masseter Medial pterygoid Temporalis |
| Protrusion (Protraction) | Medial pterygoid |
| Lateral pterygoid | |
| Retraction | Posterior fibres of temporalis |
| Side-to-side (chewing) movement | Medial and lateral pterygoids of one side contracting alternatively with that of opposite Side |
• Palpation of the temporomandibular joint and associated muscles: The bilateral palpation is must to assess the entire joint and its associated muscles. First, the patient is asked to open and close the mouth several times. Then he is asked to move the opened jaw to left, and to right, and finally he is asked to move the jaw forward. For digital palpation of condyle of moving mandible place a finger into the outer portion of the external auditory meatus.
• Dislocation of the mandible (Fig. 10.19): The mandible is dislocated only anteriorly. When the mouth is open, the mandibular condyles move forward and lie underneath the articular eminences. This is the most unstable position of the temporomandibular joint. In this position, if there is excessive opening of mouth as during yawning, sudden violence or convulsive spasm of lateral pterygoid muscles, the head of mandible of one or both sides may slip anteriorly and get locked into the infratemporal fossa; as a result the mouth cannot be closed anymore and any passive effort to do that will invariably fracture the neck of the mandible on one or both sides.
To reduce dislocation, the condyle must be lowered and pushed back behind the summit of articular eminence into the articular fossa. Thus the reduction is done by depressing the jaw with thumb placed on the last molar teeth, and simultaneously elevating the chin.
• Temporomandibular joint syndrome: This syndrome consists of group of symptoms arising from temporomandibular joints and their associated masticatory muscles. The typical presenting symptoms are:
– Diffuse facial pain, due to spasm of masseter muscle.
These symptoms may be associated with clicking and pain in the joint. The clicking is often audible when the patient is chewing. It occurs when the posterior attachment of the disc becomes stretched or detached, allowing the disc to become temporarily or permanently trapped anteriorly. The derangement of articular disc results from an overclosure or malocclusion.
• During surgery of temporomandibular joints, the facial nerve should be preserved with utmost care.
MUSCLES OF MASTICATION
The muscles of mastication are concerned with movements of mandible at the temporomandibular joints during mastication (Fig. 10.20).
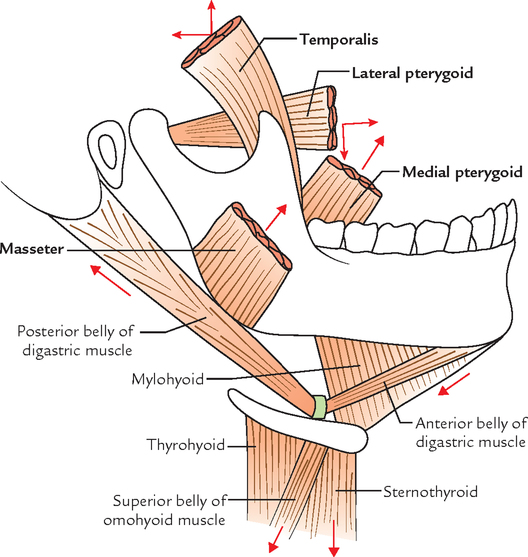
They are divided into two groups:
Principal Muscles of Mastication
The characteristic features of the principal muscles of mastication are as follows:
1. All are located in or around the infratemporal fossa.
2. All are inserted into the ramus of the mandible.
3. All are innervated by the mandibular division of the trigeminal nerve.
4. All are concerned with movements of the mandible on the temporomandibular joints.
Temporalis (Fig. 10.21)
It is a fan-shaped muscle located in the temporal fossa. It is covered by tough temporal fascia which is attached above to the temporal line and below to the zygomatic arch.

The fibres converge and descend to form a tendon, which passes through the gap between the zygomatic arch and the side of the skull. The muscle is inserted into:
1. The medial surface, apex, anterior, border of the coronoid process of ramus of mandible.
2. The anterior border of the ramus of mandible, almost up to the last molar tooth.
N.B. The temporalis muscle is fan shaped. The anterior fibres are oriented vertically, the posteriormost fibres are disposed almost horizontally and intervening intermediate fibres are placed obliquely.
Masseter (Fig. 10.22)
The masseter (Greek: masseter = a chewer) is a thick quadrilateral muscle covering the lateral surface of the ramus of the mandible including its coronoid process. The condylar process is left uncovered.
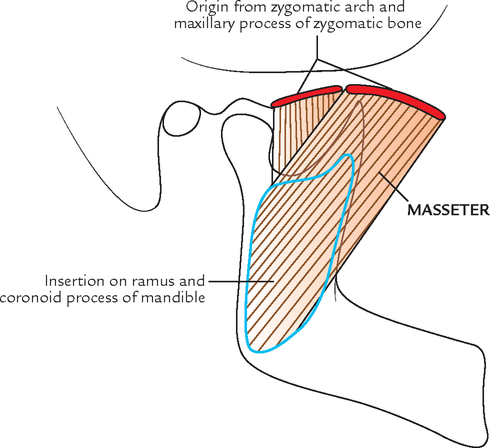
The masseter consists of the following three layers:
Superficial layer is largest of the three layers of masseter and arises by a thick aponeurosis from: maxillary process of zygomatic bone and anterior two-third of the inferior border of the zygomatic arch.
Middle layer arises from lower border of the posterior one-third of the zygomatic arch.
1. Superficial fibres pass downwards and backwards at 45° to be inserted into the angle and lower posterior half of the lateral surface of the ramus of the mandible.
2. Middle fibres pass vertically downwards to insert into the central part of the ramus.
3. Deep fibres pass vertically downwards to insert into the upper part of the mandibular ramus and its coronoid process.
Accessory Muscles of Mastication
They are described in detail in ![]() Chapter 9.
Chapter 9.
The origin, insertion, nerve supply, and actions of chief muscles of mastication are summarized in Table 10.4.
Table 10.4
Origin, insertion, nerve supply, and actions of the muscles of the mastication
| Muscles | Origin | Insertion | Nerve supply | Actions |
| Temporalis (fan shaped) | Mandibular division of trigeminal nerve | |||
| Masseter (quadrilateral) | Zygomatic arch adjoining part of zygomatic process of maxilla | Mandibular division of trigeminal nerve | Elevation of mandible to occlude the teeth for forceful bite | |
| Lateral pterygoid (Short, thick conical) | Mandibular division of trigeminal nerve | |||
| Medial pterygoid (quadrilateral) | Medial surface of angle adjoining ramus of mandible | Mandibular division of trigeminal nerve | ||

N.B. The chief muscles of mastication are often termed muscles of mastication.
PTERYGOPALATINE FOSSA
The pterygopalatine fossa is a pyramidal space situated deeply below the apex of the orbit, between the pterygoid process of sphenoid behind and the perpendicular plate of palatine in front. More laterally, the back of maxilla replaces the palatine bone as the anterior boundary of the entrance of the fossa—the pterygomaxillary fissure.
BOUNDARIES (Fig. 10.23)

| Anterior: | Perpendicular plate of the palatine and posterior surface of the maxilla (superomedial part). |
| Posterior: | Pterygoid process and adjoining part of the anterior surface of the greater wing of the sphenoid. |
| Medial: | Upper part of the perpendicular plate of palatine orbital and sphenoidal process of the palatine. |
| Lateral: | The fossa opens into the infratemporal fossa through pterygomaxillary fissure. |
| Superior: | Under surface of the body of the sphenoid and orbital process of the palatine. The lateral part of the roof is open and here fossa opens into the orbit through inferior orbital fissure. |
| Inferior: | Pyramidal process of the palatine bone in the angle between the maxilla and the pterygoid process. |
COMMUNICATIONS
Anteriorly: With the orbit through the medial end of the inferior orbital fissure.
1. With the middle cranial fossa through foramen rotundum.
Medially: With the nose through sphenopalatine foramen.
Laterally: With the infratemporal fossa through pterygomaxillary fissure.
Inferiorly: With the oral cavity through greater and lesser palatine canals.
CONTENTS
The following are the main contents of the pterygopalatine fossa:
MAXILLARY NERVE (Fig. 10.24)
The maxillary nerve, the second division (V2) of the trigeminal nerve is purely sensory.

Course and Relations
It arises from the convex anterior border of the trigeminal ganglion, pierces the trigeminal cave of dura to reach the lower part of the lateral wall of the cavernous sinus. The nerve leaves the middle cranial fossa through foramen rotundum to reach the pterygopalatine fossa. It traverses straight in the upper part of the fossa and enters the orbit through inferior orbital fissure, hence it is called infraorbital nerve. The infraorbital nerve (in fact a continuation of maxillary nerve) runs forward along the floor of the orbit in the infraorbital groove and canal in succession and appears on the face, through infraorbital foramen. Therefore in its course the maxillary nerve traverses four regions in succession: the middle cranial fossa, the pterygopalatine fossa, the orbit and the face.
N.B. In the pterygopalatine fossa the pterygopalatine ganglion is suspended from the maxillary nerve by two roots.
Branches and Distribution
The maxillary nerve gives off the following branches:
B In the Pterygo-palatine Fossa
1. Ganglionic (communicating) branches, two in number to pterygopalatine ganglion.
2. Zygomatic nerve enters the orbit through inferior orbital fissure and divides on the lateral wall of the orbit into:
(a) a zygomaticotemporal branch, which passes through a foramen in the zygomatic bone to supply the skin of the temple, and
(b) a zygomaticofacial branch, which passes through the foramen in the zygomatic bone to supply the skin of the face.
3. Posterior superior alveolar nerve enters the one or two foramina on the posterior surface of the body of maxilla and supplies the mucus membrane of the maxillary air sinus. Then it breaks up to form superior dental plexus, which supplies the molar teeth and adjoining part of the gum.
C In the Orbit (infraorbital canal)
1. Middle superior alveolar nerve passes downward and forward along the lateral wall of the maxillary sinus, joins superior dental plexus and supplies the premolar teeth.
2. Anterior superior alveolar nerve runs in the anterior wall of the maxillary sinus through a bony canal called canalis sinuosus and divides into dental and nasal branches:
D On the Face
1. Palpebral branches turn upwards and supply the skin of the lower eyelid.
2. Nasal branches supply the skin of the side of nose and the mobile part of the nasal septum.
3. Superior labial branches supply the skin and mucus membrane of the upper lip.
N.B. The superior dental plexus is formed by posterior, middle, and anterior superior alveolar nerves. It is situated in the alveolar process of the maxilla above the sockets of the teeth.
The branches of maxillary nerve are summarized in the Table 10.5.

PTERYGOPALATINE GANGLION
The pterygopalatine ganglion (ganglion of hay fever) is the largest parasympathetic peripheral ganglion. It serves as a relay station for the secretomotor fibres to the lacrimal gland and mucus glands of the nose, palate, pharynx, and paranasal sinuses. Topographically, it is related to the maxillary nerve, but functionally it is connected to the facial nerve through greater petrosal nerve (Fig. 10.25).

Roots
The roots of pterygopalatine ganglion are as follows:
1. Motor or parasympathetic root: It is derived from the nerve of pterygoid canal. It carries preganglionic parasympathetic fibres from superior salivatory nucleus (located in the lower part of the pons). These fibres relay in the ganglion. The postganglionic fibres arise from the cells in the ganglion and supply secretomotor fibres to the lacrimal gland, glands of the nose, palate, nasopharynx, and paranasal sinuses.
2. Sympathetic root: It is derived from sympathetic plexus around internal carotid artery via nerve of pterygoid canal. It contains postganglionic fibres from superior cervical sympathetic ganglion. These fibres pass through the ganglion without relay and provide vasomotor supply to the mucus membrane of the nose, palate, pharynx, and paranasal air sinuses.
3. Sensory root: It is derived from maxillary nerve and passes through the ganglion without interruption to be distributed through the branches of the ganglion.
Branches of Distribution
The branches of the ganglion are actually the branches of maxillary nerve, which passes through the ganglion without relaying. While passing through the ganglion, they incorporate the parasympathetic and sympathetic fibres of the ganglion.
The ganglion provides the following four sets of branches:
The orbital branches (2 or 3 in number) enter the orbit through inferior orbital fissure and supply orbital periosteum, ethmoidal air sinuses, and secretomotor fibres to the lacrimal gland.
The palatine branches include greater and lesser palatine nerves. The greater palatine nerve passes through greater palatine canal and foramen to supply posteroinferior quadrant of the lateral wall of the nose. The lesser palatine nerves pass through lesser palatine canals and foramina to supply secretomotor fibres to mucus membrane and glands on the inferior surface of soft palate and hard palate.
The nasal branches pass through sphenopalatine foramen to enter the nasal cavity. These are called posterior superior nasal nerves. These are divided into two sets lateral and medial. The nerves of lateral set supply lateral wall of the nasal cavity while those of medial set supply roof and nasal septum.
The longest branch of medial set is called nasopalatine/sphenopalatine nerve. It runs anteroinferiorly in a groove on the nasal septum and leaves the nasal cavity through the incisive foramen to enter the oral cavity where it supplies the anterior part of hard palate.
The pharyngeal branch passes through palatovaginal canal and supply the nasopharynx.
THIRD PART OF THE MAXILLARY ARTERY
The third part of the maxillary artery enters the pterygopalatine fossa by passing first between the upper and lower heads of lateral pterygoid and then through the pterygomaxillary fissure. Within the fossa it lies in front of the pterygopalatine ganglion and divides into its terminal branches. The branches of the third part of the maxillary artery and its distribution are described in detail on page 138 of this chapter.
 Key muscle of the infratemporal fossa Key muscle of the infratemporal fossa |
Lateral pterygoid muscle |
| All the principal muscles of mastication close the mouth except |
Lateral pterygoid, which opens the mouth |
| Clinically the most important branch of maxillary artery is |
Middle meningeal artery |
| Peripheral heart in the region of head and neck |
Lateral pterygoid muscle |
| Chief elevator of the lower jaw |
Masseter |
| All the branches of anterior division of mandibular nerve are motor except |
Buccal nerve, which is sensory and supplies mucus membrane and skin of the cheek |
| All the branches of posterior division of mandibular nerve are sensory except |
Mylohyoid nerve, which is motor and supplies mylohyoid muscle and anterior belly of digastric muscle |
| Most common nerve block given in dentistry |
Inferior alveolar nerve block |
| Most common dislocation of temporomandibular joint |
Anterior dislocation |
| Ganglion of hay fever |
Pterygopalatine ganglion |
| Most common cause of dislocation of temporomandibular joint |
Blow to the chin when mouth is widely open (as in laughing or yawning) |


A medical student was yawning in the anatomy lecture. The young lecturer walked to the student and hit him on the chin when he yawned widely again. Following a blow on chin the student got up immediately and wanted to say sorry to the teacher, but he could not say so because he failed to close his jaws. He kept standing with mouth open widely as his jaw got stuck. The lecturer immediately realized that student’s temporomandibular joints are dislocated. He took him to the orofacial surgeon who reduced the dislocation and the student was relieved of his agony.
1. Mention the type of temporomandibular joint and name the bones taking part in its formation.
2. What are the unique features of TMJ?
3. Name the parts of intra-articular disc?
4. Name the commonest variety of TMJ dislocation and how is it reduced?
1. It is a condylar type of synovial joint. The bones taking part are head (condyle) of the mandible and mandibular fossa and articular eminence of squamous part of the temporal bone.
(a) Articular surfaces are covered by plates of articular fibrocartilages.
(b) Joint cavity is divided into two compartments by an intra-articular disc.
(c) Joints of two sides function together concomitantly to accomplish the movements of the lower jaw.
3. From anterior to posterior the parts of the intraarticular disc are: (a) anterior extension, (b) anterior thick band, (c) thin intermediate zone, (d) posterior thick band, and (e) bilaminar posterior extension.
4. Anterior dislocation. It is reduced as follows: The mandible is depressed posteriorly by exerting pressure on last molar teeth with thumbs and simultaneously the assistant elevates the chin (also refer to page 148).