Anterior Region of the Neck
The triangular area on the front of the neck between the two sternocleidomastoid muscles is called anterior region of the neck. It is limited above by lower border of the body of mandible and line extending on either side from the angle of the mandible to the mastoid process, and below by the suprasternal notch. This area includes both anterior triangles, and suprahyoid and infrahyoid areas (Fig. 6.1).
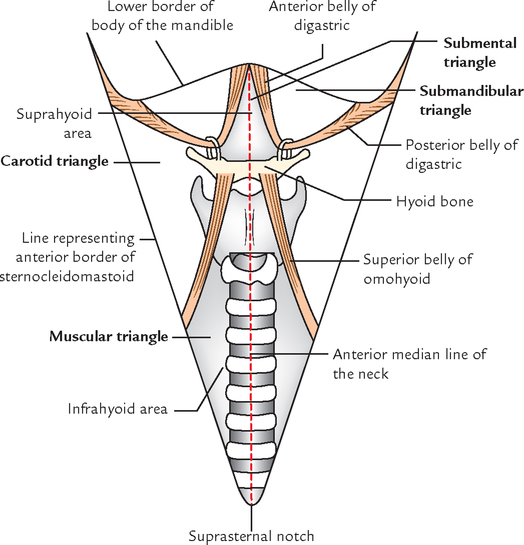
The anterior region of the neck is divided by the anterior median line (extending from symphysis menti to the jugular notch) into two anterior triangles of the neck.
Before going into details of anterior triangles of the neck, it is of great clinical importance to know the structures in the anterior median line of the neck. The identification of these structures is essential while performing tracheostomy. It is also useful in clinical examination of midline swellings of the neck.
STRUCTURES IN THE ANTERIOR MEDIAN REGION OF THE NECK
The anterior median region of the neck is 2–3 cm wide strip extending from symphysis menti to the suprasternal notch. Deep to skin and underlying the superficial and deep cervical fasciae, the anterior median region presents the following structures from above downwards (Fig. 6.2):

1. Symphysis menti: Its lower border can be felt where the two halves of the body of the mandible unite in the midline.
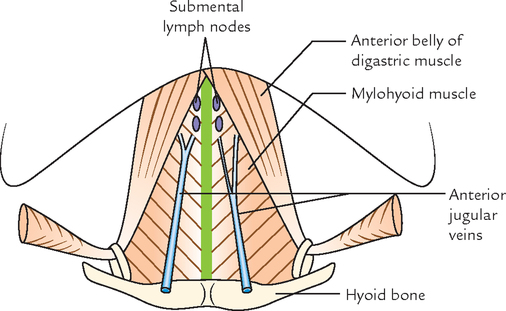
2. Fibrous raphe: It extends from symphysis menti to the hyoid bone. Mylohyoid muscles of both sides meet along this raphe to form the floor of the mouth (diaphragma oris).
3. Hyoid bone: It is a horseshoe-shaped bone suspended inferior to mandible by stylohyoid ligaments like children’s swing. Hyoid bone does not articulate with any other bone and has only muscular and ligamentous attachments. It lies at the level of C3 vertebra. The regions above and below the hyoid bone are called suprahyoid region and infrahyoid region, respectively.
4. Median thyrohyoid ligament: It is the midline thickening of the thyrohyoid membrane that connects the upper border of thyroid cartilage to the lower border and greater cornu of the hyoid bone. The membrane is separated from the hyoid bone by a subhyoid bursa.
5. Upper border of the thyroid cartilage: It is notched and can be felt. It lies opposite the body of T4 vertebra.
6. Angle of the thyroid cartilage: It forms the laryngeal prominence, which is more prominent in adult males and is called Adam’s apple.
7. Median cricothyroid ligament: It is the midline thickening of the cricothyroid membrane extending between upper border of cricoid cartilage and lower border of the thyroid cartilage.
8. Cricoid cartilage: It lies at the lower border of C6 vertebra and is the most important surface landmark on the front of the neck because a number of important structures are located at this level, such as (a) junction of larynx and trachea, (b) junction of pharynx and esophagus, and (c) anterior tubercle of transverse process of C6 vertebra (carotid tubercle) against which common carotid artery can be compressed.
9. First tracheal ring: It can be felt by gentle pressure just above the isthmus of the thyroid gland.
10. Isthmus of the thyroid gland: It lies in front of the 2nd, 3rd, and 4th tracheal rings.
11. Inferior thyroid veins: After emerging from isthmus they run downwards to lie in front of the 5th, 6th, and 7th tracheal rings.
12. Thyroidea ima artery: When present, it ascends in front of the trachea to the isthmus of the thyroid; it usually arises from the brachiocephalic artery.
13. Jugular venous arch: This traverses the venous arch, which connects the anterior jugular veins just above the suprasternal notch.
14. Suprasternal notch: It can be felt between the anterior ends of the clavicle. It lies opposite the lower border of the body of T2 vertebra. Occasionally, left brachiocephalic vein and brachiocephalic artery may lie in front of trachea in the suprasternal notch.
• The most common anterior midline swellings of the neck are: (a) enlarged submental lymph nodes, (b) thyroglossal cyst, and (c) goitre.
• The tracheostomy is most commonly done in the retrothyroid region after cutting the isthmus of thyroid gland (for detail see ![]() page 164).
page 164).
• The cut-throat wounds are most commonly observed just above or below the hyoid bone. The main vessels of the neck, viz. common carotid, internal and external carotid arteries, and internal jugular vein, usually escape the injury as they are automatically pushed backwards to the deeper plane, when neck is inadvertently extended by the culprit, before being cut.
ANTERIOR TRIANGLE OF THE NECK
The anterior triangle of the neck is a large triangular space on each side of the neck, in front of sternocleidomastoid with its apex directed downwards and base directed upwards (Fig. 6.3).

Boundaries (Fig. 6.3)
| Anterior: | Anterior median line of the neck. |
| Posterior: | Anterior border of the sternocleidomastoid muscle. |
| Base: | Lower border of the body of mandible and a line extending from the angle of mandible to the mastoid process. |
| Apex: | Suprasternal notch at the meeting point between anterior border of sternocleidomastoid and anterior median line. |
| Roof: | Investing layer of deep cervical fascia. |
The superficial fascia over the fascial roof contains platysma in the upper and anterior parts. The cervical branch of facial nerve and ascending and descending branches of transverse cervical cutaneous nerve traverse the plane between the platysma and the fascial roof of the triangle.
SUBDIVISIONS
For convenience of description, the anterior triangle has been subdivided, by the digastric muscle and superior belly of omohyoid muscle, into the following 3½ triangles (Fig. 6.3):
Before studying the subdivisions of anterior triangle, it is appropriate for students to know the attachments of digastric and omohyoid muscles, which are used for its subdivision.
Digastric muscle (Fig. 6.5A): It has two bellies – posterior and anterior. The triangular posterior belly arises from the digastric notch on the medial surface of the base of the mastoid process, and runs downwards and forwards, towards the hyoid bone. The narrow anterior belly arises from digastric fossa on the base of the mandible near symphysis menti and runs downwards and backwards, towards the hyoid bone. Above the hyoid bone the two bellies are connected by an intermediate tendon, which is anchored to the hyoid bone by a fascial sling of investing layer of deep cervical fascia.

Omohyoid muscle (Fig. 6.9): It consists of superior and inferior bellies joined at an angle by an intermediate tendon. The inferior belly arises from upper border of scapula, near the suprascapular notch, it then passes behind the sternocleidomastoid and ends there in an intermediate tendon. The superior belly begins at the intermediate tendon and passes almost vertically upwards to be attached to the lower border of the hyoid bone. The intermediate tendon lies at the level of arch of cricoid cartilage and anchored to the clavicle by fascial sling derived from investing layer of deep cervical fascia.

Submental Triangle (Fig. 6.4)
It is actually a median triangle on the front of neck below the chin and above the hyoid bone. It thus occupies the upper portions of both the anterior triangles.
Digastric (Submandibular) Triangle (Fig. 6.5 A, B)
It is so named because it is located between the two bellies of the digastric muscle and below the base of the mandible.
Boundaries
| Anteroinferiorly: | Anterior belly of digastric muscle. |
| Posteroinferiorly: | Posterior belly of digastric muscle, supplemented by stylohyoid muscle. |
| Base: | It is formed by the base of the mandible and imaginary line joining the angle of the mandible to the mastoid process. |
| Apex: | It is formed by the intermediate tendon of the digastric muscle, being bound down to hyoid bone by a fascial sling derived from investing layer of deep cervical fascia. |
Contents
The digastric triangle is subdivided into anterior and posterior parts by the stylomandibular ligament, which extends from the tip of the styloid process to the angle of the mandible. The posterior part of the triangle is continuous above with the parotid region.
Contents in the anterior part of the triangle:
1. Submandibular salivary gland.
4. Facial vein (lies superficial to the gland).
Contents in the posterior part of the triangle:
2. Carotid sheath and its contents.
3. Structures passing between the external and internal carotid arteries (for details refer to ![]() page 241).
page 241).
All these structures are discussed in detail in the submandibular region (![]() Chapter 9,
Chapter 9, ![]() p. 131).
p. 131).
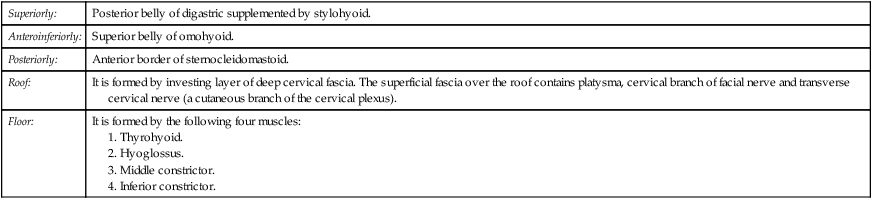
Carotid Triangle (Fig. 6.6)
It is so called because it contains all the three carotid arteries, viz. common carotid, internal carotid, and external carotid.

Boundaries
| Superiorly: | Posterior belly of digastric supplemented by stylohyoid. |
| Anteroinferiorly: | Superior belly of omohyoid. |
| Posteriorly: | Anterior border of sternocleidomastoid. |
| Roof: | It is formed by investing layer of deep cervical fascia. The superficial fascia over the roof contains platysma, cervical branch of facial nerve and transverse cervical nerve (a cutaneous branch of the cervical plexus). |
| Floor: | It is formed by the following four muscles: |
Contents
N.B. The major contents of carotid triangle are common carotid artery, internal carotid artery, external carotid artery, internal jugular vein, and last three cranial nerves, all overlapped by sternocleidomastoid.
The carotid triangle provides good view of all its contents only if sternocleidomastoid is retracted slightly backwards.
Relevant Features of the Contents of the Carotid Triangle
It ascends from just behind the inferior angle of the carotid triangle in the carotid sheath under cover of anterior border of sternocleidomastoid and in front of lower 4 cervical transverse processes and at the level of the upper border of the thyroid cartilage divides into external and internal carotid arteries. The common carotid artery gives no other branches in the neck (for details see ![]() page 237).
page 237).
It ascends anteromedial to the internal carotid artery and gives the following five branches in the triangle:
• Ascending pharyngeal artery: It is a slender artery that arises from the medial aspect of external carotid artery near its lower end. It ascends in the deeper plane on the side of the pharynx (for details see ![]() page 240).
page 240).
• Superior thyroid artery: It arises from the front and descends downwards and forwards to pass deep to the infrahyoid muscles to reach the upper part of the thyroid gland (for details see ![]() page 238).
page 238).
• Lingual artery: It arises from the front aspect of external carotid artery, opposite the tip of greater cornu of hyoid bone. It then runs upwards and forwards forming a characteristic loop over the greater cornu of the hyoid and disappear deep to the hyoglossus muscle. Before disappearing it gives rise to suprahyoid artery, which runs superficial to hyoglossus above the hyoid (for details see ![]() page 238).
page 238).
N.B. The loop of lingual artery above the greater cornu of hyoid bone permits free movements of hyoid bone without damaging the artery.
• Facial artery: It arises from the front aspect of external carotid artery just above the lingual artery and runs upwards on the superior constrictor deep to digastric and stylohyoid muscles (for details see ![]() page 239).
page 239).
• Occipital artery: It arises from the posterior aspect of external carotid artery at the lower border of posterior belly of digastric muscle and runs backwards superficial to internal carotid artery, internal jugular vein, and last three cranial nerves along the lower border of posterior belly of digastrics (for details see ![]() page 239).
page 239).
It descends between the internal jugular vein and internal carotid artery. Then just above the level of greater cornu of hyoid bone, it hooks around the origin of the occipital artery, runs forwards, crossing in front of internal carotid artery, external carotid artery, and loop of lingual artery to run on the hyoglossus muscle above the hyoid bone.
As it crosses the internal carotid artery, it gives off the superior root of ansa cervicalis (also called descendens hypoglossi), which descends on the anterior wall of the internal and common carotid arteries and becomes embedded in the anterior wall of the carotid sheath.
They lie on and along the internal jugular vein (for details see ![]() page 249).
page 249).
It is partly hidden by the posterior edge of the sternocleidomastoid. It descends posterolateral to common and internal carotid arteries and receives the following three veins in the region of carotid triangle:
• The lingual vein lies just below and parallel to the hypoglossal nerve, crosses external and internal carotid arteries to join the internal jugular vein.
• The common facial vein after crossing the digastric triangle, crosses the upper part of carotid triangle to drain into the internal jugular vein.
• The superior thyroid vein crosses the lower part of the triangle to end into the internal jugular vein.
It descends vertically downwards, first between the internal carotid artery and internal jugular vein and then between common carotid artery and internal jugular vein. It gives the following two branches in the carotid triangle.
1. Pharyngeal branch: It runs inferomedially between the external and internal carotid arteries to join the pharyngeal plexus on the superior constrictor of the pharynx.
2. Superior laryngeal nerve: It runs on a deep plane, deep to both internal and external carotid arteries, where it divides into internal and external laryngeal nerves. The internal laryngeal nerve (sensory) passes forwards to disappear deep to thyrohyoid muscle; there it pierces the thyrohyoid membrane to supply the laryngeal mucosa.
The external laryngeal nerve (motor) descends to supply the inferior constrictor and cricothyroid muscles after passing deep to the superior belly of the omohyoid.
It is a facial sheath which encloses internal jugular vein, and internal and common carotid arteries. The vagus nerve lies in between the vein and the artery on a deeper plane (for details refer to ![]() Chapter 4). The ansa cervicalis is embedded in its anterior wall whereas the cervical sympathetic chain lies just deep to its posterior wall on the prevertebral fascia.
Chapter 4). The ansa cervicalis is embedded in its anterior wall whereas the cervical sympathetic chain lies just deep to its posterior wall on the prevertebral fascia.
It is a fusiform dilatation at the terminal end of common carotid artery or at the beginning of internal carotid artery. It has rich innervation from glossopharyngeal, vagus, and sympathetic nerves. The carotid sinus acts as a baroreceptor (pressure receptor) and regulates the blood pressure in the cerebral arteries.
It is a small oval structure situated behind the bifurcation of the common carotid artery. It is reddish-brown and receives rich nerve supply from glossopharyngeal, vagus, and sympathetic nerves. It acts as a chemoreceptor and responds to the changes in the oxygen and carbon dioxide content of the blood. The excess of CO2 and reduced O2 tension in blood stimulates it causing increase in blood pressure and heart rate.
Ansa cervicalis (Figs 6.7 and 6.8)
The ansa cervicalis (ansa hypoglossi) is a U-shaped nerve loop present in the region of the carotid triangle embedded in the anterior wall of the carotid sheath. It is derived from ventral rami of C1, C2, and C3 spinal nerves. It supplies all the infrahyoid muscles except thyrohyoid, which is supplied by nerve to thyrohyoid (C1) from hypoglossal nerve.
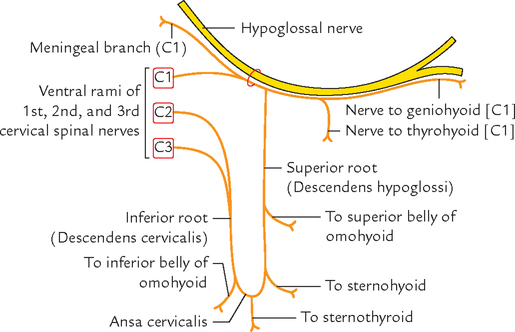

Roots:
Ansa cervicalis has the following two roots:
1. Superior root (descendens hypoglossi) is formed by the descending branch of the hypoglossal nerve carrying C1 spinal nerve fibres. It descends downwards over internal and common carotid arteries.
2. Inferior root (descendens cervicalis) is derived from C2 and C3 spinal nerves. As this root descends, it first winds round the internal jugular vein and then continues anteroinferiorly to join the superior root in front of the common carotid artery at the level of cricoid cartilage.
Muscular Triangle (Figs 6.1 and 6.3)
Contents
Infrahyoid muscles, viz. sternothyroid, sternohyoid, and thyrohyoid.
The important deeper structures in the region of muscular triangle are thyroid gland, trachea, and esophagus. They are studied separately.
N.B. Supra and infrahyoid areas: These are the areas on the front of neck above and below the hyoid bone, respectively.
Suprahyoid area corresponds to submental triangle (for details see submental triangle on page 88).
Infrahyoid area is bounded superolaterally by the superior bellies of the omohyoid muscles and inferolaterally by the sternocleidomastoid muscles. It includes muscular triangles of both anterior triangles.
The infrahyoid area contains strap (ribbon-like) muscles of the neck. Underneath these muscles lie all important structures. From superficial to deep, these are:
SUPRAHYOID AND INFRAHYOID MUSCLES OF THE NECK
Suprahyoid Muscles of the Neck
The suprahyoid muscles comprise following four paired muscles.
These muscles are described in detail in ![]() Chapter 9.
Chapter 9.
Infrahyoid Muscles of the Neck (Strap Muscles of the Neck)
The infrahyoid muscles are ribbon-like and comprise following four paired muscles (Fig. 6.9).
N.B. Developmentally, the infrahyoid muscles are the derivatives of the longitudinal muscle sheet that extends vertically from the symphysis menti to pubic symphysis. This sheet ultimately divides into different segments; some of them disappear altogether. The remaining segments are represented by:
(a) geniohyoid, above the hyoid,
(b) infrahyoid muscles, between the hyoid and sternum,
(c) sternalis (occasional) in front of sternum, and
(d) rectus abdominis and pyramidalis (occasional) in the anterior abdominal wall.
The attachment of inferior belly of omohyoid to scapula is secondary to its migration from its initial attachment to medial end of the clavicle.
The infrahyoid muscles are arranged into two layers with two muscles in each layer, viz.
Nerve Supply
All are supplied by ventral rami of C1, C2, and C3 spinal nerves.
The sternohyoid, omohyoid, and thyrohyoid are supplied by the ansa cervicalis and its superior root. The thyrohyoid is innervated directly by a branch from the hypoglossal nerve carrying fibres of ventral ramus of C1. The origin, insertion, and actions of individual muscles are presented in Table 6.1.
Table 6.1
Origin, insertion, and actions of the infrahyoid muscles
| Muscle | Origin | Insertion | Actions |
| Sternohyoid (thin narrow strap muscle) | Posterior surface of manubrium and adjoining part of clavicle, and posterior sternoclavicular ligament | Medial part of the lower border of the hyoid bone | Depresses hyoid bone following its elevation during swallowing |
| Sternothyroid (shorter and wider than sternohyoid) | Posterior surface of the manubrium and adjoining part of the first costal cartilage | Oblique line on the lamina of thyroid cartilage | Depresses the larynx following its elevation during swallowing |
| Thyrohyoid (It is an upward extension of the sternothyroid being broken by the oblique line on the thyroid lamina) | Oblique line on the lamina of thyroid cartilage | Lower border of the greater cornu and adjoining part of the body of the hyoid bone | |
| Omohyoid consists of inferior and superior bellies united by an intermediate tendon | Lower border of the body of the hyoid bone lateral to the sternohyoid. The intermediate tendon is bound to the clavicle by a fascial pulley derived from investing layer of deep cervical fascia | Depresses the hyoid bone following its elevation during swallowing |
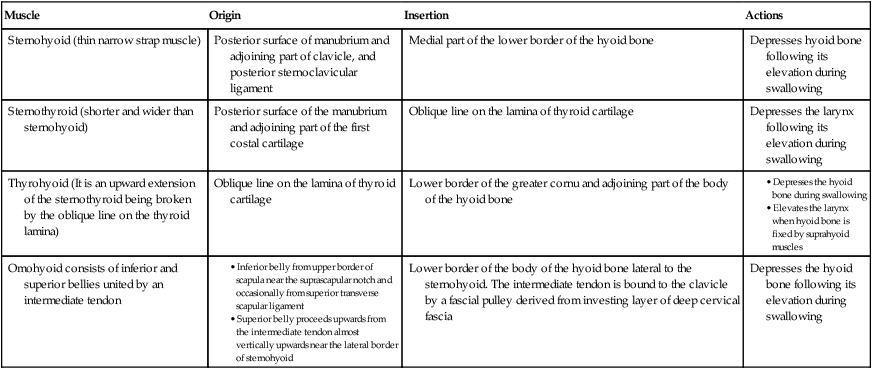
N.B. All the infrahyoid muscles depress the hyoid bone following its elevation during swallowing.
The thyrohyoid also elevates the larynx when the hyoid is fixed by the suprahyoid muscles.
 Most important pressoreceptor in the body Most important pressoreceptor in the body |
Carotid sinus |
| Most important landmark in the neck |
Cricoid cartilage |
| Commonest site of tracheostomy |
Retrothyroid (i.e. behind the isthmus of thyroid gland) |
| Carotid tubercle (Chassaignac’s tubercle) |
Prominent anterior tubercle of the transverse process of sixth cervical vertebra |
| Carotid pulse can be easily palpated |
Just beneath the anterior border of sternocleidomastoid at the level of superior border of thyroid cartilage |
| All the strap muscles of the neck are supplied by the branches of ansa cervicalis except |
Thyrohyoid muscle which is supplied by a branch of hypoglossal nerve carrying C1 fibres |
| Potato tumor |
Tumor arising from carotid body (also called carotid body tumor) |
| Arteriosclerosis of common carotid and/or internal carotid artery can cause |
Cerebrovascular ischemia (cerebral stroke) |


A 35-year-old man complained to his physician that he is a victim of sudden attacks of syncope (fainting) from sudden rotation of his head especially when wearing a tight collar or tie. He was told by the physician that he was suffering from a disease called carotid sinus syndrome and a surgical procedure may be needed to relieve his symptoms.
A 75-year-old man visited his physician and complained that he is having a small painless swelling below his chin and his tip of tongue is ulcerated. On examination the physician found that the swelling was single and located in the submental triangle. It was hard mobile, and not attached to the skin.