

 Dysfunctional Uterine Bleeding
Dysfunctional Uterine Bleeding
Mandeep K. Brar, M.D., and Ruben Alvero, M.D.
 Basic Information
Basic Information
Definition
Dysfunctional uterine bleeding (DUB) describes abnormal uterine bleeding in the absence of disease in the pelvis, pregnancy, or medical illness. Parameters of normal menstrual function are described in Box 1D-5. Specific types of abnormal bleeding include the following:
• Hypermenorrhea: excessive bleeding amount during normal duration of regular menstrual cycles
• Hypomenorrhea: decreased bleeding amount in regular menstrual cycles
• Menorrhagia: regular normal intervals, excessive flow and duration
• Metrorrhagia: irregular intervals, excessive flow and duration
• Menometrorrhagia: irregular or excessive bleeding during menstruation and between periods
• Oligomenorrhea: intervals >> 35 days
• Polymenorrhea: intervals <<21 days
These terms, while commonly used in practice, increasingly are felt to be confusing. In fact, The FIGO Menstrual Disorders Working Group has been working since 2009 to eliminate many of the confusing and overlapping terms and create simpler definitions that can be intuitively understood by medical professionals and lay people alike. The term dysfunctional uterine bleeding was initially used in 1935 but has never been clearly defined and has been used as both a diagnosis and a symptom. It is generally understood to be a term of exclusion when no other cause of bleeding has been established. FIGO recommends that the three diagnoses (disturbances of molecular control of menses, HPO axis abnormalities, and disorders of hemostasis) be grouped under the nonstructural causes of abnormal uterine bleeding. However, these new FIGO terms have not yet made their way into common usage.
Synonyms
DUB
Epidemiology & Demographics
• Most cases of DUB occur in postmenarchal and perimenopausal age groups.
• During reproductive age, <20% of abnormal bleeding results from anovulatory DUB.
Physical Findings & Clinical Presentation
• A clinical diagnosis of exclusion
• Thorough physical and pelvic examination to exclude the other causes of abnormal bleeding
1. Includes thyroid, breast, liver, presence or absence of ecchymotic lesions
2. Patient possibly obese and hirsute (polycystic ovarian disease)
3. No evidence of any vulvar, vaginal, cervical lesions, uterine (fibroid) or ovarian tumor, urethral caruncle, urethral diverticula, hemorrhoids, anal fissure, colorectal lesions
4. Bimanual pelvic examination: normal-sized or slightly enlarged uterus
Etiology
• 90% is caused by anovulation.
• 10% is ovulatory in origin; can be caused by dysfunction of corpus luteum or midcycle (estrogen withdrawal) bleeding.
• Section II describes the various causes of abnormal uterine bleeding.
 Diagnosis
Diagnosis
Differential Diagnosis
• Pregnancy-related cause
• Anatomic uterine causes:
1. Leiomyomas
2. Adenomyosis
3. Polyps
4. Endometrial hyperplasia
5. Cancer
6. Sexually transmitted diseases
7. Intrauterine contraceptive devices
• Anatomic nonuterine causes:
1. Cervical neoplasia, cervicitis
2. Vaginal neoplasia, adhesions, trauma, foreign body, atrophic vaginitis, infections, condyloma
3. Vulvar trauma, infections, neoplasia, condyloma, dystrophy, varices
4. Urinary tract: urethral caruncle, diverticulum, hematuria
5. Gastrointestinal tract: hemorrhoids, anal fissure, colorectal lesions
• Systemic diseases:
1. Exogenous hormone intake
2. Coagulopathies: von Willebrand’s disease, thrombocytopenia, hepatic failure
3. Endocrinopathies: thyroid disorder, hypothyroidism and hyperthyroidism, diabetes mellitus
4. Renal diseases
• Section II describes a differential diagnosis of vaginal bleeding abnormalities.
Workup
• A detailed history and thorough physical examination, including a pelvic examination to exclude causes mentioned above.
• Clinical algorithms for the evaluation of vaginal bleeding are described in Section III, “Bleeding, Vaginal.”
Laboratory Tests
• Complete blood count with platelets; possible iron-deficiency anemia or thrombocytopenia
• Prothrombin; partial thromboplastin and bleeding time if coagulopathy is suspected
• Serum human chorionic gonadotropin
• Chemistry profile, including liver function tests
• Thyroid profile
• Stool testing for occult blood
• Urinalysis for hematuria
• Pap smear
• Cultures for gonorrhea and Chlamydia
• Serum gonadotropins and prolactin
• Serum androgens
• Endometrial biopsy in women, especially if there exists a longstanding history of anovulatory bleeding with fewer than three menstrual cycles per year or a high risk of endometrial neoplasia in women with prolonged unopposed estrogen exposure
• Hysterogram and hysteroscopy
• von Willebrand’s panel, particularly in perimenarchal women
Imaging Studies
• Pelvic ultrasound, including measurement of endometrial thickness and assessment of myometrial or endometrial defects
• Fluid contrast ultrasound (also called saline sonogram, sonohysterogram, saline infusion sonogram, and various other names). Distends the uterine cavity so that “filling defects” of the endometrium can be assessed. Such a filling defect may represent an endometrial polyp, uterine fibroid, or neoplasm.
 Treatment
Treatment
Nonpharmacologic Therapy
Increase iron intake in the form of pills and a diet rich in iron.
Acute General Rx
• Progestational agents (see Box 1D-6)
1. Progesterone in oil, 100 to 200 mg
2. Medroxyprogesterone acetate, 20 to 40 mg qd for 15 days
3. Megestrol acetate, 40 to 120 mg daily in divided doses for 15 days
4. Oral contraceptives: any oral contraceptive pill, 1 tablet qid for 5 to 7 days, followed by 1 tablet low-dose estrogen qd for 21 days; causes withdrawal bleeding; should then be on cyclical Provera or continue on oral contraceptives
• Estrogens
• Surgical treatment
1. Hysteroscopy with or without dilation and curettage (D&C)
2. Endometrial ablation
3. Hysterectomy
Chronic Rx
• Progestational agents
1. Medroxyprogesterone acetate 10 mg qd for 12 days, then cyclically to induce monthly withdrawal bleeding
2. Norethindrone 2.5 to 10 mg qd for 12 days
3. Depo-Provera 150 mg IM and then 150 mg every 3 mo
4. Oral contraceptives, 1 tablet qd either cyclically or continuously using only active pills
5. Levonorgestrel-releasing intrauterine device (Mirena, currently has an FDA indication for heavy menstrual bleeding in women who use an IUD for contraception)
• Letrozole or clomiphene citrate: patients with anovulatory bleeding who want to become pregnant. Recent studies suggest that progesterone withdrawal may be counterproductive in patients wishing to start an ovulation induction regimen. Pregnancy rates are lower when patients undergo withdrawal compared to when random ovulation induction start is used. A recent large, multicenter trial demonstrated that letrozole is superior to clomiphene citrate in ovulation induction in women with PCOS. Human menopausal gonadotropin (HMG) can be used for women who do not ovulate with oral agents or who have hypothalamic dysfunction.
• Others.
1. Antiprostaglandins
2. Danazol (rarely used due to side-effect profile).
3. Gonadotropin-releasing hormone analogues (GnRH); often used to reduce bleeding and ameliorate anemia and in preparation for a surgical procedure.
4. Tranexamic acid (Lysteda) is an antifibrinolytic agent FDA approved for cyclic heavy menstrual bleeding. Dosage in normal renal function is 3900 mg daily (650 mg tablets, 2 tablets tid) for up to 5 days during menses.
• Surgical treatment
1. D&C and hysteroscopy
2. Endometrial ablation
3. Hysterectomy
Disposition
Cyclical treatment on birth control pills or Provera for several cycles, then discontinue pill and watch patient for onset of regular menses. If the patient does not want to conceive, continued cycle management with oral contraceptives is commonly used.
Referral
To gynecologist in case of failure of treatment
 Pearls & Considerations
Pearls & Considerations
Comments
• Table 1D-23 describes management options for DUB.
• Patient education material may be obtained from the American College of Obstetricians and Gynecologists, 409 12th Street SW, Washington, DC 20024-2188; phone 202-638-5577.
Related Content
Evaluation of ovulatory bleeding (Algorithm, Section III)
Evaluation of anovulatory bleeding (Algorithm, Section III)
Dysfunctional Uterine Bleeding (Patient Information)
Endometrial Cancer (Related Key Topic)
Uterine Fibroids (Related Key Topic)
TABLE 1D-23
Management of Dysfunctional Uterine Bleeding (DUB)
| Bleeding Pattern | Cause | Treatment |
| Ovulatory DUB | ||
| Heavy menstrual bleeding | Imbalance in endometrial prostacyclins and prostaglandins | Nonsteroidal antiinflammatory drugs Combination oral contraceptive pill Progestin intrauterine device Endometrial ablation |
| Midcycle spotting | Periovulatory estrogen decline | None |
| Delayed menses | Persistent corpus luteum | None (rule out pregnancy) |
| Anovulatory DUB | ||
| Irregular menses | Unopposed estrogen stimulation of endometrium | Combination oral contraceptive pill Cyclic progestins Endometrial ablation |
| Postmenopausal bleeding | Endometrial atrophy | Hormone replacement therapy Endometrial ablation |
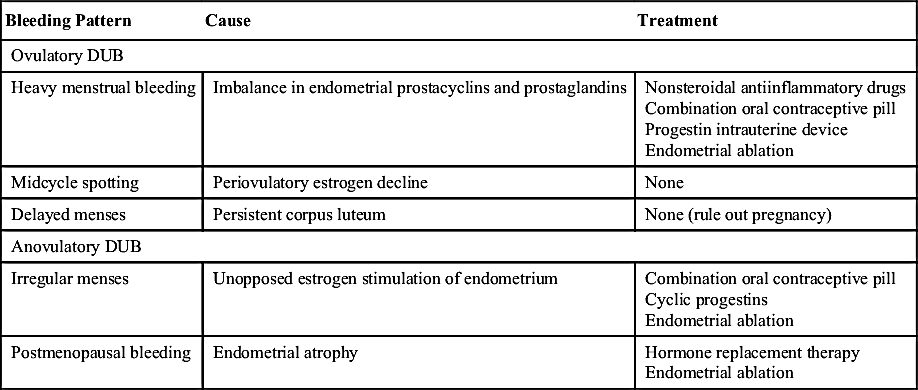
From Carlson KJ, Eisenstat SA, et al: Primary care of women, ed 2, St Louis, 2002, Mosby.