Occupational Performance Model (Australia)
A Description of Constructs, Structure and Propositions
Chris Chapparo; Judy L. Ranka; Melissa Therese Nott
Abstract
This chapter describes how the Occupation Performance Model (Australia) (OPM(A)) is structured around eight interacting constructs: occupational performance (the central construct) and its conceptual elements, which include occupational roles, occupational performance areas, occupational performance capacities, core elements of occupational performance, context, space, and time. The constructs outlined in this chapter can be applied to people and groups. Practice stories of people who have a physical impairment are included in the chapter to illustrated how reduced physical capacity or impairment may affect all constructs of the OPM(A). Considerations for identifying performance strengths and evaluating the impact of physical impairments on occupational performance are provided.
▪ The OPM(A) is a conceptual framework that simultaneously explains occupational performance and scope of occupational therapy practice.
▪ The focus of the OPM(A) is the relationship between people and their contexts relative to performance of occupations throughout life.
▪ The OPM(A) is a self-organising, interactive system comprising eight major constructs: occupational performance, occupational roles, occupational performance areas, occupational performance capacities, core elements of occupational performance, context, space and time.
▪ Performance, as defined in this model, extends the usual notions from that of motor action only to include antecedent and subsequent physical, cognitive, sensory, mental and emotional processes relevant to the task performed.
▪ The relationship between constructs is strategic in nature. Tasks and routines are configured strategically by people to comply with their occupational role performance needs. People use their performance capacities strategically to support performance of relevant tasks and routines.
▪ The external context can afford or inhibit performance.
▪ Personal interpretations of time and space are embedded in the performance of all occupations throughout life.
▪ Notions of ‘normal’ and ‘typical’ are rejected in favour of the ‘specific’ and ‘particular’.
▪ The constructs can be applied to individuals and groups.
▪ People with reduced physical capacity can experience difficulty engaging in occupational performance within any construct.
Introduction
Models of occupation and therapy are used by researchers and practitioners in a variety of ways so it is not surprising that one single model has been unable to meet the range of theoretical, practice and explanatory demands of the profession. This chapter describes how one model, the Occupational Performance Model (Australia) (OPM(A)) (Chapparo & Ranka, 1997; Jurkowitsch & Ranka, 2009) conceptualises both elements of occupation and the performance of occupations and can be used in practice to explain, delineate and make decisions about the scope and focus of occupational therapy for individuals and groups.
A conceptual model must be developed in such a way as to provide an easily understood interpretation for the model users. A conceptual model, when implemented properly, should satisfy the following four fundamental objectives (Gemino & Wand, 2004):
1. Enhance a person’s understanding of the representative system. In this instance the OPM(A) contributes to students’, therapists’ and others’ understanding of occupational performance and occupational therapy.
2. Facilitate communication of elements of the system between relevant people. The OPM(A) provides a common, well-defined and easy-to-use language system that can assist with communication of occupation-centred issues among all people in the system where it is used (e.g. therapists, people who receive occupational therapy services, researchers and other stakeholders).
3. Provide a point of reference for system designers to extract system specifications. This means that constructs and propositions within the OPM(A) can be used by occupational therapists and students to develop and explain the nature and focus of practices used.
4. Document the system for future reference and provide a means for collaboration. Publication of the constructs within the OPM(A) (such as the information contained in this chapter) and propositions about how they may be related provides a vehicle for further research and development within the profession.
Discussion of the OPM(A) in this chapter is limited to outlining (1) the structure of the model by defining the major constructs, (2) propositions about the relationship between constructs and (3) examples of how the constructs and propositions can be used by practitioners. Although some aspects of the constructs are not unique to the OPM(A) and reflect a synthesis of decades of ideas about the nature of human occupations (e.g. Christensen, Bass, & Baum, 2015; Kielhofner, 2002, 2009; Meyer, 1922), those emphasised in this chapter form a configuration of occupational performance that differs from other performance-focused models and reflects concepts in the OPM(A) outlined originally by Chapparo & Ranka (1997).
OPM(A): philosophical basis and assumptions
The OPM(A) is considered a conceptual framework that simultaneously explains occupational performance and scope of occupational therapy practice. The overarching philosophy that informs its structure and use is pragmatism, a defining philosophy of practice underpinning early and contemporary occupational therapy (Meyer, 1922; Morgan, 2007). The focus of pragmatism is on addressing issues that are relevant to people and that result in action (Glasgow & Steiner, 2012). Pragmatists believed that knowledge is generated by personal experience through ‘knowing’ and ‘doing’ (Hooper & Wood, 2002). Early pragmatists emphasised the following two perspectives that are aligned with the assumptions, focus and use of the OPM(A):
1. People construct visions of desired futures and direct their everyday activity towards realising those futures. The focus of occupational therapy for people who experience reduced physical capacity is on their needs and the practical, active ways those needs can be met.
2. The daily activity of people is inextricably interwoven with their biology and their physical and social environments, and each of these may pose possible barriers or enablers to desired activity in unique ways (Dewey, 1930). Mirroring Meyer’s (1922) original ideas about the focus and methods used in occupational therapy, the OPM(A) proposes that people harness their physical, mental and psychological capacities strategically to carry out their daily occupations. Occupational therapy is not solely interested in people’s physical, cognitive or psychosocial capacity per se, but rather how people can develop and use their capacities in a way that is demanded by the occupations they do and in the contexts where they live.
Although the OPM(A) uses general terms to describe its constructs and processes, its application to each situation by therapists is specific and unique to each person or group. Notions of ‘typical’ and ‘normal’ are rejected in favour of the ‘specific’ and ‘particular’. To this end, the OPM(A) provides a template that can be used to assist practitioners and researchers discover the experiences of people (unique particularities) when they engage in activities (occupations) that may pose difficulty (problems of moving, sensing, thinking, feeling and communicating) and the ways that these can be addressed (through the use of personal and other resources) in their own contexts. Key features of pragmatism in occupational therapy practice that uses the OPM(A) as a guiding framework include the following:
▪ The perspectives, practices and outcomes of therapy are those that are important to the person or group receiving occupational therapy.
▪ The focus of therapy practice is on real-world events rather than artificial or manipulated scenarios.
Occupational performance: constructs and structure
Consistent with other existing and evolving models in occupational therapy, the primary focus of the OPM(A) is the lifelong person–context relationship and its activation through occupation. Eight major constructs form the theoretical structure of this model. These are occupational performance, occupational roles, occupational performance areas, occupational performance capacities, core elements of occupational performance, context, space and time. Each of these constructs incorporates many interrelating elements.
In addressing a person–context–performance relationship, the structural framework of the model considers the interactions between two contexts relative to people and occupation: the internal context and the external context (Fig. 10.1).
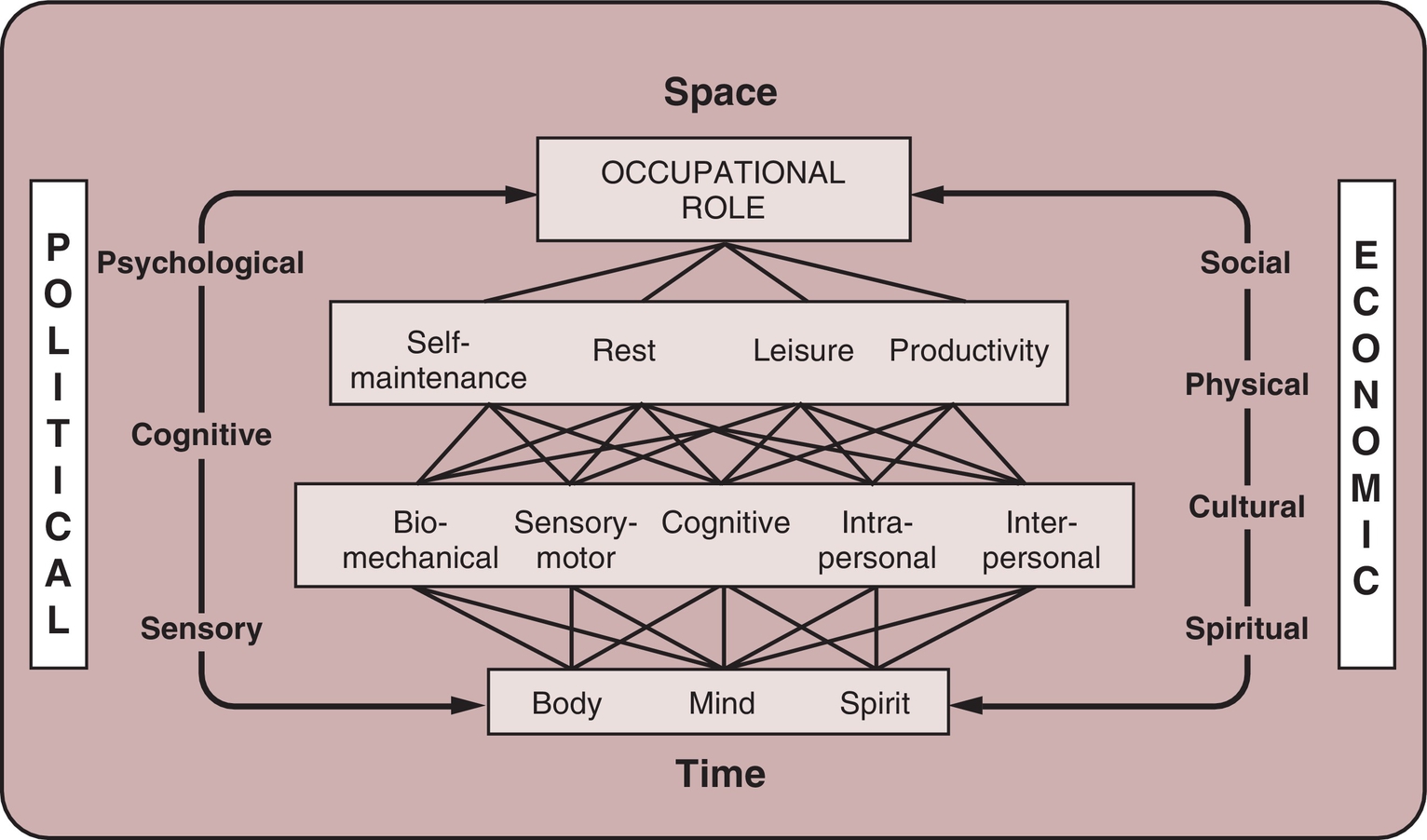
The internal context is the central core of the model and reflects both the person or people (the performer) and the occupation being performed. The OPM(A) does not separate person and occupation constructs, emphasising the assumption that occupation does not exist as a separate entity, but is only actualised through engagement of the performer (the performance). The internal context comprises four layers that reflect the increasing complexity of occupations and their performance: the core elements of occupational performance, occupational performance capacities, occupational performance areas and occupational roles. The external context is composed of structures, conditions and influences that are outside of the person within which occupations are performed. The external context has several layers consisting of sensory, physical, cognitive, social, cultural, spiritual, economic and political dimensions. Functions of the internal and external contexts operate in time and space (see Fig. 10.1).
In the OPM(A), use of the word context rather than environment is proposed for conceptual and semantic reasons. Participation in any life task requires that people assign meaning to the contexts in which they perform occupations. Although concrete aspects of the environment are common to all, individuals create their own view of it. As a part of every daily task people do, they make interpretations of what they are able to do (internal context), what they want to do (internal context) and what they see are the affordances or limitations that surround them (external context). The OPM(A) refers to this process as contextualising, bringing the external context into the mind. People’s internal and external contexts become fused to form an understanding of their own performance and its place in the world around them. Context is both a place and a process in occupational performance.
Construct 1: occupational performance
The major construct around which the Occupational Performance Model (Australia) is conceptualised is occupational performance. The central proposition in this model is that all goal-oriented behaviour related to daily living is occupational in nature. Performance, as defined in this model, extends the usual notions from that of motor action only to include antecedent and subsequent physical, cognitive, sensory, mental and emotional processes relevant to the task performed. Performance is the ability to perceive, desire, recall, plan and carry out occupations in response to demands of the internal and/or external contexts, and is characterised by changes that can be physical, cognitive or psychosocial. Occupation refers to meaningful roles, routines, tasks and subtasks performed for the purpose of self-maintenance, productivity, leisure (Reed, 2005) and rest (Meyer, 1922).
Occupational performance is the ability to perceive, desire, recall, plan and carry out roles, routines, tasks and subtasks for the purpose of self-maintenance, productivity, leisure and rest in response to demands of the internal and/or external context (Chapparo & Ranka, 1997).
Construct 2: occupational roles
Occupational roles are patterns of occupational behaviour composed of configurations of self-maintenance, productivity, leisure/play and rest occupations. Occupational roles are determined by each unique person–context–performance relationships. They are established through need and/or choice and are modified with age, ability, experience, circumstance and time (Chapparo & Ranka, 1997).
Humans are active in the process of creating their occupational being or identity through active participation in tasks and with others. Active participation can be intrinsically driven by choice or need or externally imposed by contextual factors. This occupational identity is expressed through a person’s occupational performance and defined by peoples’ occupational roles. Occupational roles comprise patterns of occupational performance that are determined by a person’s unique daily routines of self-maintenance, productivity, leisure and rest within that person’s particular contexts (Chapparo & Ranka, 1997; Hillman & Chapparo, 2008; Kielhofner, 2002).
Occupational role behaviour is complex, probably because roles are content specific and tied to the context in which they are embedded. People adopt a number of roles that become functionally interlocked. For example, people are expected to be workers at work. However, they simultaneously behave in the roles of ‘friend’ when talking to others with whom they have a close relationship, ‘worker’ when working on tasks that are directed by the job, ‘learner’ when learning new work skills, ‘player’ when socialising during breaks and out-of-work hours, ‘self-carer’ when eating lunch and looking after themselves while going to and from work, and ‘community member’ when engaging in activities that support the particular work institution that employs them and when helping others. Premium value may be assigned to any of these roles. For example, a person might value the role of friend over other interlocking roles at work. Assessment of role performance of people with reduced physical capacity should therefore pay attention to all interlocking roles and identify those that are most important to the person or group.
Each role has its own repertoire of behaviours that support it. Roles are lost, gained and changed throughout the lifespan in a process of transition (Chapparo & Ranka, 1997; Forsberg-Wärleby & Möller, 1996; Hillman & Chapparo, 2008). Challenges occur when people experience life and health events that disrupt their ability to carry out their roles in a manner that is expected or desired. Role change that is imposed rather than chosen may be accompanied by stress. People who sustain reduced physical capacity may experience permanent or temporary role loss (e.g. inability to engage in self-care activities after a stroke). They may have difficulty with resuming or acquiring new roles (e.g. resuming work in a different capacity after back or hand injury; becoming a carer for a spouse with significant physical impairment), or they may have difficulty identifying which role is the most appropriate in a specific situation and making the transition between different roles. For example, people who have significantly reduced physical capacity because of a fluctuating disorder such as rheumatoid arthritis or chronic fatigue syndrome may have difficulty making the transition from a self-maintainer role (managing physical fatigue and joint pain at work) to a worker role when returning to the work station after resting during lunch break.
Roles appear to be governed by a complex relationship between demands placed upon people in their contexts and their own personal choices (Hillman & Chapparo, 2008; Landis, 1995). Over time, people learn to balance their roles between what others expect them to do and what they want to do. Sudden onset of reduced physical capacity results in a period of role change during which people learn to understand and balance personal and expected roles in light of their physical capacity and the resources available to them.
Although personal choice is thought to motivate adoption of roles throughout life, the OPM(A) also recognises that, as both a construct and a personal/social system of values, individual choice is alien to a number of social groups whose sociocultural identity is collectivistic (Manstead & Hewstone, 1995). Occupational role performance can therefore be determined by the individual, the social group or combinations of both.
Consistent with the pragmatist view outlined earlier, the OPM(A) conceptualises occupational roles as having three dimensions. One is knowing. Knowing is having an intuitive or concrete understanding of roles people want to enact and what roles are expected by their physical-sensory-sociocultural context. The second involves a process of doing and usually entails action. The third dimension addresses the interpersonal and socioemotional aspects of role identity and acknowledges the notion of being as a fulfilment or satisfaction component of occupational performance roles (Rowles, 2009). It is possible that this dimension is linked to personal meaning, which contributes to valuing one’s occupational roles (Hillman & Chapparo, 2008).
People participate fully or partially in the performance of occupational roles. For example, full participation in the occupational role of homemaker (work role) produces occupational behaviour involving physical activity during the performance of many tasks and routines (doing). This may be carried out with family members requiring interpersonal interaction (social context) and knowledge of their needs (knowing). The role carries with it aspects of satisfaction and fulfilment that are linked both to personal notions of competence in the performance of the role and personal perceptions of its sociocultural worth (being).
Alternatively, a man who is elderly, and who requires considerable physical assistance may be deemed to have no occupational role as a self-maintainer because he can no longer ‘do’ self-maintenance routines or tasks (for example, getting dressed). However, he does ‘know’ what he wants done and how he wants it done, thereby participating in the ‘knowing’ dimensions of role performance. He can also experience satisfaction when the self-maintenance routines are carried out to his directions and experience the ‘being’ dimensions of role function in terms of fulfilment.
Someone with severe and multiple physical impairments may not be able to contribute to the ‘doing’ or ‘knowing’ aspects of an occupational role such as self-maintainer. Personal and family expectation may be related to ‘being’ cared for in a safe, comfortable situation that provides satisfaction and contentment to the level needed by that person. In this instance a person who lacks the ability to organise the ‘doing’ or ‘knowing’ aspects of occupational roles has the right to ‘being’ cared for in a way that supports the person’s role as a family member whose existence is valued.
The OPM(A) is thought to function as a self-organising, interactive system, in which occupational role is the central organising construct (Chapparo & Ranka, 1997). Roles influence and are influenced by other parts of the system, a relationship that is depicted by the recursive arrows in Fig. 10.1. For example, a person’s occupational role as a worker determines the balance of time and activity allotted to self-maintenance, productivity, leisure and rest areas of occupational performance. These, in turn, determine the personal capacities necessary for engagement in work. Alternatively, when circumstance allows a person to choose an occupational role, the choice may be based on the presence or absence of particular capacities they have, such as the outstanding motor coordination of an athlete or the cognitive creativity of an artist. When illness strikes core elements of a person (e.g. a stroke affecting the body and mind function), relationships throughout the system are disturbed, affecting role function.
Analysis of Occupational Role Performance
Given the doing, knowing, being, view of occupational roles, the OPM(A) asserts that identification of important roles should not be limited simply to interpretation of observable actions (what the person does) or by an external source (such as a predetermined role checklist) (see, e.g., Crepeau & Schell, 2009 for summary). The unique construction of occupational roles assumes that there is not just one meaning (shared by everyone) for a named role (such as ‘gardener’, or ‘churchgoer’). Theorists warn against imposing normative interpretations or expectations while obtaining information about occupational role performance during assessment (Jackson, 1998). Any analysis of occupational role performance relative to the OPM(A) definition of occupational roles would include examples of questions such as those listed in Box 10.1.
Construct 3: occupational performance areas
Occupational performance areas comprise self-maintenance, work, play and rest, and their relationship to other constructs in the OPM(A) is illustrated by arrows in Fig. 10.1. Occupational therapy has traditionally categorise performance of daily occupations to three areas: self-maintenance occupations, productivity/school occupations and leisure/play occupations. The OPM(A) proposes a fourth area: rest occupations (Chapparo & Ranka, 1997). Others, including early pragmatists, have also recognised its importance as a dimension of occupational performance (American Occupational Therapy Association [AOTA], 2008; Meyer, 1922).
Rest occupations refer to the purposeful pursuit of nonactivity. This can include time devoted to sleep as well as routines, tasks, subtasks and rituals undertaken in order to relax (Chapparo & Ranka, 1997).
Inclusion of this category as separate from self-maintenance occupations acknowledges that there are sociocultural, daily and lifespan reasons for the degree to which people are, or wish to be, passive and contemplative rather than active and productive. People who experience reduced physical capacity find that planned periods of rest become important to sustaining occupational performance in other areas (Matuska & Barrett, 2014).
Self-maintenance occupations are routines, tasks and subtasks done to preserve a person’s health and well-being in the environment (Reed, 2005). These routines, tasks and subtasks can be in the form of habitual routines (dressing, eating) or occasional nonhabitual tasks (taking medication) that are demanded by circumstance (Chapparo & Ranka, 1997).
Productivity/school occupations are routines, tasks and subtasks which are done to enable a person to engage in learning, provide support for self, family or community through the production of goods or provision of services (Chapparo & Ranka, 1997) (Reed, 2005).
Leisure/play occupations are those routines, tasks and subtasks that are done for purposes of entertainment, creativity and celebration (Chapparo & Ranka, 1997).
Occupational Performance Areas: Subtask, Tasks and Routine Units of Performance
Although activity has been a term traditionally used in occupational therapy to denote purposeful action (Christiansen, 1991; Cynkin, 1979; Fidler & Fidler, 1978; Meyer, 1922; Mosey, 1981), meanings attributed to the term have become so broad and flexible that it has lost its power to describe elements of occupations and performance at varying levels (Nelson, 1988). In the OPM(A), occupations in each occupational performance area have been classified into subtask, task and routine units according to their size and complexity (Fig. 10.2).
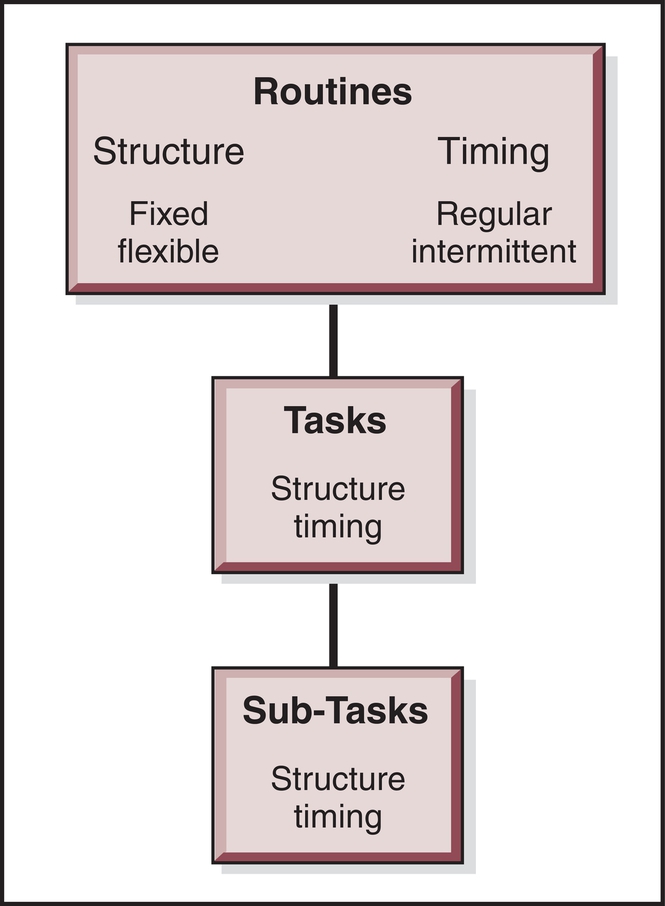
Subtasks consist of steps or single units of the total task and are stated in terms of observable behaviour (e.g. putting an arm in a sleeve) (Romiszowski, 1984). Tasks are a sequence of subtasks that are ordered from the first step performed to the last performed to accomplish a specific purpose (e.g. putting on a jacket). Tasks can be carried out in action (doing) or thought (planned) and have definite beginning and end points. For example, drinking can be divided into subtasks such as locating the glass, reaching for the glass, grasping the glass, lifting the glass and taking a mouthful of liquid. All of these subtasks, when put together in an orderly sequence, result in execution of the total task: drinking. Routines are larger ‘chunks’ of occupation that are made up of a number of tasks that are sequenced to achieve a specific function (Brown, 1987). For example, drinking is one of the tasks involved in the routines of preparing and eating a meal.
Patterns of performance can be fixed or flexible. Many routines are fixed, determined by the prevailing sociocultural or physical context (such as using an escalator or lift, using the entry gates at a train station). A flexible routine is one that can be accomplished in many different ways, as long as it is accomplished in a way that is acceptable to the performer and others. For example, there are many ways to complete morning routines. When someone sustains physical injury, one of the functions of occupational therapy is to explore alternative or more flexible patterns for task performance that may be quite different from those previously used by the person.
The classification of subtasks, tasks and routines can also be described according to their temporal patterns. Routines can be regular or intermittent. Regular routines occur on a daily basis and are usually critical to a person’s function relative to the demands of his or her context. Intermittent routines do not have to be accomplished every day but may still be crucial to independent or satisfying function in life. For example, sudden illness prompts a person to engage in the routine of going to the doctor. Other intermittent routines have a qualitative impact on a person’s life. For example, going to the movies is not a critical routine for most people but may be perceived by people as life enriching.
The extent to which people participate in performance of subtasks, tasks and routines is dependent on age, circumstance and ability. People with reduced physical capacity because of injury or illness are often unable to complete routines without assistance from others. Many may never be able to master the performance of daily routines. However, having the opportunity to choose to participate in part of the routine (a task or a subtask) contributes to establishing an occupational identity that is linked to an occupational role. For example, a young man who uses a wheelchair, has reduced upper limb physical capacity, and who is unable to complete the whole routine of shopping need not be excluded from family shopping excursions. His participation in those tasks and subtasks of the shopping routine which he is able to master, such as selecting items, transporting them on his lap and paying for them, confirms his occupational identity by participating in the occupational role performance of shopper and family member.
Classification of Occupational Performance Areas: An Idiosyncratic Process
Naming a task as either self-maintenance or work is an idiosyncratic function that can only be done by the performer, and the way a person classifies any one occupation as work, leisure, rest or self-maintenance may change day to day relative to its purpose. For example, reading may be classified by a person at one time as self-maintenance (to read medication instructions), or work (to read a computer screen), or leisure (to read a book for enjoyment), or rest (reading to get to sleep). Moreover, classification of occupations varies among sociocultural groups. Similarly, the pattern of time spent or value afforded each of the occupational performance areas are individually determined relative to desired or expected occupational role performance. Contrived notions of the balance of occupational performance cannot be externally imposed. The absence of lines separating the occupational performance areas of self-maintenance, rest, leisure and productivity in Fig. 10.1 illustrate that in the OPM(A), any division that is externally imposed is artificial.
Analysis of Occupational Performance Areas
Occupations at this level can be analysed and described using standard task analysis methods. Elements of the routine, task or subtask to be performed can be examined using a task demands analysis. The performance can be measured using behavioural task analysis. For example, cooking a meal can be described as a routine that requires performance of the tasks and subtasks of cutting, reading, stirring, tasting and grasping objects in such a way that a meal is produced within a specific time frame (task demands analysis). The performance of the person producing the meal can be analysed according to how successful the performance of each step of these routines, tasks and subtasks is relative to goals (behavioural task analysis). Errors in performance usually fall into one or more of four categories: errors of accuracy (does the wrong thing: for example, putting the wrong ingredients in a cake mix), errors of omission (leaves part of the performance out: such as forgetting to turn on the oven when cooking), errors of repetition (perseverates on steps: such as repeating steps in cooking that have already been completed) and errors of timing (too slow or quick such that performance is affected: for example, not cooking ingredients for long enough).
Questions listed in Box 10.2 represent examples of analysis and intervention that would be addressed in occupational performance areas.
Construct 4: occupational performance capacities
Accomplishment of routines and tasks in the occupational performance areas is predicated on the ability to use a variety of personal capacities or attributes in a way that is determined by the occupation and the performance context. This aspect of the model is conceptualised as being comprised of the capacities of the performer as well as the capacity requirements of occupations. There are motor, sensory, cognitive and psychosocial dimensions to any task performed that prompt a person to use motor, sensory, cognitive, interpersonal and intrapersonal capacities in a particular or strategic manner. Observation and analysis of occupational performance capacities focuses on task demands, the performance capacities of the person, and the relationship between them. For example, if a person with reduced motor capacity in the upper limbs had to dress, a task demands analysis would identify the specific range, strength, coordination and control needed for dressing in that person’s context. Observation of the person’s performance would be used to assess whether the person’s motor capacities (range, strength, coordination and control) were sufficient for successful performance or whether there was poor ‘fit’ between the physical demands of the task and the physical capacity of the person. This approach differs from using standard methods of assessing physical capacity per se. The OPM(A) categorises occupational performance capacities into five areas: motor, sensory, cognitive, intrapersonal and interpersonal (see Fig. 10.1).
Motor capacity (move): From the perspective of the performer this component refers to the operation and interaction of and between physical structures of the body during task performance. This can include range of motion, muscle strength, grasp, muscular and cardiovascular endurance, circulation, elimination of body waste, regulation of muscle activity, generation of motor responses and coordination. From the perspective of the task being done this component refers to the physical attributes of the task, such as size, load, dimension and location of objects (Chapparo & Ranka, 1997).
Sensory capacity (sense): From the perspective of the performer this component refers to the registration of sensory stimuli and discrimination required by the task. From the perspective of the task this component refers to the sensory aspects of the task, such as colour, texture, temperature, weight, movement, sound, smell and taste (Chapparo & Ranka, 1997).
Cognitive capacity (think): From the perspective of the performer this component refers to the operation and interaction of and between mental processes used during task performance. This can include thinking, perceiving, recognising, remembering, judging, learning, knowing, attending and problem solving. From the perspective of the task this component refers to the cognitive dimensions of the task. These are usually determined by the symbolic and operational complexity of the task (Chapparo & Ranka, 1997).
Intrapersonal capacity (feel): From the perspective of the performer this component refers to the operation and interaction between internal psychological processes used during task performance. This can include feelings, emotions, self-esteem, mood, affect, rationality and defence mechanisms. From the perspective of the task this component refers to the intrapersonal attributes that can be stimulated by the task and are required for effective task performance such as valuing, satisfaction and motivation (Chapparo & Ranka, 1997).
Interpersonal capacity (communicate): From the perspective of the performer this component refers to the continuing and changing interaction between a person and others during task performance. This can include interaction among individuals in relationships such as partnerships, families, communities and organisations both formal and informal. Interactive examples include sharing, cooperation, empathy, verbal and nonverbal communication. From the perspective of the task this component refers to the nature and degree of interpersonal interaction required for effective task performance (Chapparo & Ranka, 1997).
There is a complex network of interactions between the capacities and other constructs within the model. Influence of one capacity on another is illustrated by the absence of lines between capacities within this level of the model (Fig. 10.1). The interaction between the capacities and other levels of the model is illustrated by the arrows between levels in the Model (Fig. 10.1).
Analysis of Occupational Performance: Occupational Performance Capacities
Occupational therapists use many human capacity assessments that are independent from the tasks and contexts where they are used. For example, goniometry can be used to analyse restrictions in joint range of motion; the Mini Mental State Examination (Folstein, Folstein, & McHugh, 1975) can be used to analyse short- and long-term memory operations; measures of social interaction can be used to analyse interpersonal operations; and loneliness or depression inventories have been used as measures of intrapersonal operations (Borg & Bruce, 1991). The OPM(A) assumes each capacity is only functional if the person can apply existing capacities strategically. For example, people with back injuries may demonstrate strength that is within normal limits and good memory on formal tests of those capacities, but they may not use their motor and cognitive capacity in a strategic way when lifting and handling heavy objects (think then move), resulting in further injury. An elderly woman who has sustained a stroke may score poorly on formal measures of memory but may demonstrate adequate memory for everyday function in her own home environment when assessed using task analysis in her context. Analysis at the capacity level of the OPM(A) requires a criterion-referenced approach, similar to that described earlier. In other words, performance is determined as successful or not depending on how the capacity has to be used for particular tasks, in particular contexts with particular supports.
Successful strategy use implies salience or use of known motor, sensory, cognitive, interpersonal and intrapersonal capacities in the ‘here and now’. It is the ability to choose and apply the ‘best’ strategy to fit a particular situation. Effective strategy use is dependent on having a large repertoire of strategies – in other words, many alternatives from which to choose when faced with a problem of function – and efficiency in the use of strategies (Torbeyns, Verschaffel, & Ghesquiére, 2004). This level of the OPM(A) lends support for three intervention approaches relative to improving occupational performance: capacity building (increasing the number and strength of strategies that are needed for tasks and routines), capacity application (learning how to apply newly learned strategies or residual strategies in different ways), and grading the capacities demanded by occupations to be performed.
Questions listed in Box 10.3 represent considerations to be made during assessment and intervention at this level of occupational performance.
Construct 5: core elements of occupational performance
Construct 5 acknowledges the body–mind–spirit interactionist paradigm that has long been recognised as key to physical and mental health and well-being (Townsend, Brintnell, & Staisey, 1990) and is illustrated at the bottom of the internal construct in Fig. 10.1. Although each of the three aspects of this construct is described separately in this section, they cannot be functionally separated, reduced or understood as independent elements. This is not a new concept in occupational therapy and reflects pragmatist views of an integrated being whose mind, body and soul seek harmony (Meyer, 1922). In the OPM(A), body, mind and spirit are viewed as core elements reflecting the essential ‘makeup’ of humans from a corporeal (physical and tangible) and incorporeal (intangible and without material existence) perspective (Chapparo & Ranka, 1997).
Body element is defined as all of the tangible physical elements of human structure (Chapparo & Ranka, 1997).
Acknowledging the core element of the physical body affirms that within the boundaries of human understanding, aspects of performance can be described in terms of their smallest known structure such as cells, molecules and tissues. The interaction within and between the physical structures of the body may either contribute to occupational performance by providing the intrinsic physical elements required for occupational performance or inhibit desired occupational performance if affected by ill health, injury or disease (such as degenerative joint disease, musculoskeletal trauma and amputation).
Mind element is defined as the core of a person’s conscious and unconscious intellect that forms the basis of the person’s ability to understand and reason (Chapparo & Ranka, 1997).
The concept of the mind is understood in many different ways by many different cultures. Neurobiological approaches, for example, take a physicalist view of the mind and describe mind–brain relationships on the basis of neurotransmitters, neuronal circuitry and cell function. It is generally agreed that the mind is that which enables a person to have consciousness and the capacity for thought that, in turn, produces individual paradigms of reality from which people plan their daily routines, tasks and subtasks and construct their beliefs. Disorders of the mind (such as acquired brain impairment and schizophrenia) may affect occupational performance at all levels in the OPM(A).
Spirit element is defined loosely as that aspect of humans that seeks a sense of harmony within self and between self, nature, others and in some cases an ultimate other; seeks an existing mystery to life; inner conviction; hope and meaning (Chapparo & Ranka, 1997).
Spirituality is a broad concept with room for many perspectives. In general, it includes a sense of connection to something bigger than oneself. This view mirrors earlier interpretations of spirituality in occupation as expressed by Meyer (1922), who observed that as people live their life through daily occupations, they concern themselves not only with the performance of occupations but with deriving meaning from them. In the OPM(A), spirituality, as distinct from religiosity, is not viewed as separate from everyday occupations, but as a part of every level of occupational performance.
Although many idiosyncratic definitions of spirituality have been derived in health literature, three concepts are recurrent and relate to notions of ‘meaning’, ‘hope’, and a sense of ‘interconnectedness’. The link between human occupations and meaning is at the heart of ‘purposefulness’ of life. Particularly for Aboriginal and Torres Strait Islander peoples of Australia, spirituality is a dynamic, evolving, contemporary expression of indigineity connecting past, present and future (Poroch et al., 2009). For all people, a strong sense of ‘spirit’ is considered an important determinant of health.
The OPM(A) does not view spirituality as one human subsystem, but a fundamental core element that is embedded in all aspects of occupational existence. At the level of occupational performance routines, tasks and subtasks it contributes to the person’s sense of purposefulness when creating, thinking about and doing desired and needed occupations. At the capacity level in the OPM(A), spirituality, when defined as meaning and hope, contributes to using cognitive strategies that involve imagination, decision making and the ability to reflect. Intrapersonal aspects of meaning and hope relate to notions of a personal locus of control, intention, will, motivation. Interconnectedness is fundamental to the desire for and the development of interpersonal strategies that satisfy a personal need to ‘fit’ with the external social world.
Relative to occupational performance, the body–mind–spirit core element of this model translates into the ‘doing–knowing–being’ dimensions at all levels of performance. The influence between the core elements and other levels of the model is reflected by the arrows which link the core elements to the occupational performance capacities (see Fig. 10.1).
Analysis of Occupational Performance: Core Elements of Performance
Aspects of core elements of performance that may be considered during assessment and intervention for occupational performance are listed in Box 10.4.
Construct 6: external context
People participate in occupations that occur in specific contexts. The ecology of their task performance is a critical element of successful participation reinforcing the notion that context-based performance (what a person actually does in his or her own context) may be quite different from clinic-based capacity (a person’s ability to perform a task at the highest level of functioning in a test situation). For this reason an ecological approach to assessment with a focus on the discordance between person/people and context, as well as factors within the person, or people is needed.
In the OPM(A) the external context is an interactive world which has physical, sensory, cognitive, psychological, social, cultural, spiritual, and political-economic elements (Chapparo & Ranka, 1997). Aspects of the external context are labelled and defined briefly here. Their position around the internal context in Fig. 10.1 reflects the scope of ongoing press and affordance they exert on daily performance. An affordance is when the performance context enables opportunities for optimum performance. For example, a handle affords pulling, a quiet room affords reading, and a slippery surface affords balance reactions. Press has to do with the level of demand placed on performance and presents barriers, risks and restrictions to performance. Although all people at various times experience contextual demand that is beyond their capacity to cope, it is usually temporary. People with reduced physical capacity experience greater demand (press) from the external context as their physical capacity changes. It also cannot be assumed which of the contextual elements asserts greatest press. The cumulative effects of all contextual elements affecting performance may be greater than a single element. For example, some people who experience difficulties with the cognitive dimensions of planning movement find the cumulative cognitive load of thinking about how to do the task (cognition) and controlling actions in situ (physical) contributes to reduced physical skills. Each of the contextual elements in Fig. 10.1 assume prominence relative to salient performance demands. For example, the physical context assumes importance when climbing stairs at a railway station, sensory and cognitive contexts assume importance when cooking a meal from a complicated recipe. Their relationship to roles, tasks, capacities and core elements changes constantly.
Physical Context
The physical, tangible elements of situations in which people perform or participate, the location and arrangement of objects in the physical world and the physical characteristics of tools, objects, equipment, materials, supplies, food and liquids used (e.g. size, dimension, position, weight, viscosity). This includes naturally occurring characteristics and those that are built, engineered, manufactured or assembled.
Sensory Context
The sensory characteristics of tools, objects, equipment, materials, supplies, food and liquids used. It also includes sensory aspects of a wider performance context including temperature, texture, sound, light, odour, taste, humidity, movement and vibration.
Cognitive Context
The cognitive and perceptual complexity of situations where people do their everyday occupations, the clarity of information presented and the ease with which information presented can be interpreted in order to know what things are, what to do and how to use items, including tools, objects, equipment, materials, supplies, food and liquids. A virtual context exists when along with displacement of time and place, an alternate reality is contextualised for performance.
Psychological Context
The characteristics of situations that support or challenge a person’s psyche. This includes dimensions that may invoke high levels of arousal, strong emotions, stress responses or have a calming effect.
Social Context
The characteristics of situations that require interactions with others and the expectations and supportiveness of people in those interactions. They include a range of social interactions from solitary, dyad, triad and small group to large group membership that may be closed or open.
Cultural Context
The characteristics of situations that reflect the traditions and ways of ‘doing’ that are passed down through generations and are unique to social groups. These include cultural symbols, arrangement of space, tools and materials used, modes of dress, modes of interaction, place for rituals, customs and ceremonies.
Spiritual Context
The characteristics of situations that support people’s spiritual beliefs – for example, places of worship and sacred sites or places to be meditative, tools, materials, clothing and food associated with sacred rites and rituals.
Political Context
The explicit and implicit laws, policies and rules that govern and regulate performance and participation. Disability discrimination legislation, for example, is an aspect of the political context which mandates opportunities for equal participation for people with reduced physical capacity in all performance contexts.
Economic Context
The explicit and implicit financial systems and structures that fund and reward performance and participation. The costs of goods and services, taxation and health insurance, are important to all people, but assume greater importance where the cost of equipment, access and ongoing intervention is required for people with reduced physical capacity.
Analysis of Occupational Performance: External Context
Examples of the focus of analysis and intervention for occupational performance at this level of the OPM(A) include those listed in Box 10.5.
Construct 7: space
Space refers to compositions of physical matter (physical space) as well as a person’s view of experience of space (felt space) (Chapparo & Ranka, 1997).
Space is defined as an expanse that extends in all directions, in which all material objects or forms are located. The OPM(A) extends these notions of surrounding space to incorporate both internal and external components (see Fig. 10.1). External space surrounds people and contains objects in space, but people themselves contain internal space that is filled with objects in the form of body structures. Human understanding of internal and external space is conceptualised in this model as physical space and felt space. Physical space is derived from the technical construct of space as viewed by physics and from this is derived, in part, people’s understanding about body structures, body systems, objects with which they interact and the wider physical world within which they function.
Of more importance to occupational performance is the notion of felt space. Although people are surrounded by physical space, the meaning they attribute to it, the way they use it and their interactions within it are largely determined by how they interpret it. Felt space is a personal, dynamic view of physical space as experienced by individuals. The meaning that is attributed to physical space during occupational performance has representation within all the constructs. For example, external objects and space impinge on people’s various sensory receptors at the level of core elements of occupational performance. This information results in an understanding of the form and space elements of the context through a complicated process of interpretation. Motor, cognitive, sensory, interpersonal and intrapersonal perspectives of form and space are integrated to generate a highly individualised personal schema (body scheme), an account of form and space components of every step of every occupational task that is perceived, remembered, planned or carried out in life. People who experience reduced physical capacity work hard to reorder their personal schema.
Construct 8: time
Time refers to a temporal ordering of physical and other events (physical time) as well as a person’s understanding of time based on the meaning attributed to it (felt time) (Chapparo & Ranka, 1997).
Time is the final construct of the OPM(A) and has been defined as a system of relating one successive event to another. Just as with descriptions of the spatial construct outlined previously, time is conceptualised in this model as physical time and felt time (see Fig. 10.1).
Physical time is also derived from laws of physics which attempt to explain the temporal aspects of physical changes seen during occupational performance. This is usually expressed in terms of sequential or simultaneously occurring events.
Felt time is a person’s understanding of time based on the meaning that is attributed to it. As with felt space, felt time involves highly personal abstractions of time that have representation at all levels of the model. It is an experiential abstraction that is being constantly changed and modified by experience. At the core elements, it is essential to muscle contraction, neuronal transmission and a spiritual feeling of the ‘right’ time. At the capacities level, it is the application of strategies when required by the tasks being performed. At the level of the occupational performance areas, timed ordering of steps in performance is essential to forming sequential routines. At the occupational role performance level, timing of performance links people to their social and environmental circumstances and enables feelings of being in the ‘right place’ at the ‘right time’. As with the concept of felt space, notions of felt time vary from person to person and from one culture to another. Before using this model to explain abstractions of time relative to other cultures, therapists would need to investigate the prevailing abstraction of time within that culture and revise its relationship to other constructs within the model.
Analysis of Occupational Performance: Space and Time
As described, elements of space and time are embedded in occupational performance at every level of the model. The implication for analysis of occupational performance is to consider space and time dimensions within all the constructs of occupational performance.
Conclusion
This chapter describes how the OPM(A) is structured around eight constructs: occupational performance (the central construct) and its conceptual elements, which include occupational roles, occupational performance areas, occupational performance capacities, core elements of occupational performance, context, space and time. The proposed interaction between the constructs has been illustrated in Fig. 10.1 by arrows between these constructs. The arrows conceptualise a particular relationship between constructs that is strategic in nature and reflects a self-organising occupational performance system. Tasks and routines are configured strategically by people to comply with their occupational role performance needs. People apply their occupational performance capacities strategically to support relevant tasks and routines to be performed. Core elements comprising human composition are used strategically to develop and maintain performance capacities. These arrows not only link constructs conceptually but propose a place for occupational therapy intervention that centres on how people can gain or regain the most strategic use of self for occupational performance and the place for external affordance. Notions of ‘normal’ and ‘typical’ are rejected in favour of the ‘specific’ and ‘particular’. The constructs outlined in this chapter can be applied to people and groups. The OPM(A) can be used as a means of identifying performance strengths and evaluating the impact of impairments on occupational roles, occupational performance areas and occupational performance capacities.
