Gait Disorders
Philip D. Thompson, John G. Nutt
The maintenance of an upright posture and the act of walking are among the first, and ultimately most complex, motor skills humans acquire. From an early age, walking skills are modified and refined. In later years, the interplay between voluntary and automatic control of posture and gait provides a rich and complex repertoire of motion that ranges from walking to running to complex sports and dancing. An individual's pattern of walking may be so distinctive they can be recognized by the characteristics of their gait or even the sound of their steps. Many diseases of the nervous system are identified by the disturbances of gait and posture they produce.
Physiological and Biomechanical Aspects of Gait
Humans assume a stable upright posture before beginning to walk. Stability when standing is based on mechanical musculoskeletal linkages between the trunk and legs and neurological control detecting and correcting body sway. Coordinated synergies of axial and proximal limb muscle contraction and a hierarchy of postural responses maintain standing or static postural control. Postural responses encompass automatic righting reflexes keeping the head upright on the trunk, supporting reactions controlling antigravity muscle tone, anticipatory (feed-forward) postural reflexes occurring before limb movement, and reactive (feedback) postural adjustments counteracting body perturbations during movement. Postural responses are also modified by voluntary control according to the circumstances in which balance is threatened. For example, rescue reactions such as a step or windmill arm movements preserve the upright posture and protective reactions such as an outstretched arm break a fall to prevent injury. Postural reflexes and responses are generated by the integration of visual, vestibular, and proprioceptive inputs in the context of voluntary intent and the environment in which the subject is moving.
Once the trunk is upright and stable, locomotion can begin. The initiation of gait is heralded by a series of shifts in the center of pressure beneath the feet during the course of an anticipatory postural adjustment—first posteriorly, then laterally toward the stepping foot, and finally toward the stance foot to allow the stepping foot to swing forward. This sequence is then followed by the stereotyped stance, swing, and step phases of the gait cycle. Dynamic equilibrium during walking, turning, and avoiding obstacles pose even more challenges to the postural system and the effects of disease or aging on postural control commonly first appear when walking (Earhart, 2013).
Anatomical Aspects of Gait
The neuroanatomical structures responsible for equilibrium and locomotion in humans, inferred from studies in lower species, indicate two basic systems (Takakusaki, 2008, 2013). First, brainstem (subthalamic, midbrain) and cerebellar locomotor regions project through descending reticulospinal pathways from the pontomedullary reticular formation into the ventromedial spinal cord. Stimulation of brainstem locomotor centers leads to an increase in axial and limb muscle tone followed by the adoption and maintenance of an upright posture before stepping begins. Second, descending pontomedullary reticular projections activate assemblies of spinal interneurons (central pattern generators or spinal locomotor centers) that drive motoneurons of limb and trunk muscles in a patterned and repetitive manner to produce stepping movements. Propriospinal networks link motoneurons of the trunk and limbs, facilitating synergistic coordinated limb and trunk movements during locomotion. In quadrupeds, spinal locomotor centers are capable of maintaining and coordinating rhythmic stepping movements after spinal transection. The cerebral cortex and corticospinal tract are not necessary for experimentally induced locomotion in quadrupeds but are required for precision stepping. In monkeys, descending ventromedial brainstem and ventrolateral spinal motor pathways are necessary for stepping and balance. Lesions of the medial brainstem in monkeys interrupt descending reticulospinal, vestibulospinal, and tectospinal systems, producing marked postural dysequilibrium. The control of posture and locomotion in humans appears to be mediated by similar networks. The isolated spinal cord in humans with spinal cord transection can produce spontaneous movements but cannot generate rhythmic stepping, indicating that brainstem and higher cortical connections are necessary for bipedal walking in humans. Neuroimaging of imagined gait suggests that the prefrontal cortex via corticobulbar and indirectly via corticostriatal tracts modulates midbrain and cerebellar locomotor regions (Zwergal, 2012). Frontal motor projections to the pontomedullary reticular formation that innervate axial muscles modulate postural responses associated with stepping and spinal motoneurons, enabling precision foot movements. The parietal cortex integrates sensory inputs indicating position and orientation in space, the relationship to gravitational forces, the speed and direction of movement, and the characteristics of the terrain and environment. The cerebellum modulates the rate, rhythm, amplitude, and force of stepping and also contributes to the medial brainstem efferent system controlling truncal posture and equilibrium through projections from the flocculonodular and anterior lobes. Although the neuroimaging reveals locomotor circuitry, the means by which these control the automatic and voluntary movements of walking remains unknown.
History: Common Symptoms and Associations
A detailed history of the walking difficulty provides the first clues to diagnosis. It is helpful to note the circumstances in which walking difficulty occurs, the leg movements most affected, and any associated symptoms, especially falls (that may be the presenting feature). Walking over uneven ground exacerbates most walking difficulties, leading to tripping, stumbling, and falls. Fear of falling may lead to a variety of voluntary protective measures to minimize the risk of injury. In some patients, particularly the elderly, compensatory strategies and a fear of falling lead to a “cautious” gait that dominates the clinical picture. Often an individual is unaware of their gait abnormality, and family or friends note altered cadence, shuffling, veering, or slowness. Because disorders at many levels of the musculoskeletal, peripheral, and central nervous systems give rise to difficulty walking, it is necessary to consider whether orthopedic, muscle weakness, a neurological defect of motor control, or sensory disturbance is contributing to the gait problem.
Weakness
Many patients attribute any gait or balance problem to leg weakness even though none is detected on examination. However, weakness of certain muscle groups produces characteristic difficulties during particular movements of the gait cycle. Catching or scraping a toe on the ground and a tendency to trip may be the presenting symptom of hemiplegia (causing a spastic equinovarus foot posture) or foot drop caused by weakness of ankle dorsiflexion. Weakness of knee extension presents with a sensation that the legs will give way while standing or walking down stairs. Weakness of ankle plantar flexion interferes with the ability to stride forward, resulting in a shallow stepped gait. Difficulty in climbing stairs or rising from a seated position is suggestive of proximal muscle weakness. Axial muscle weakness due to peripheral neuromuscular diseases may also interfere with truncal mobility. Fatigue during walking accompanies muscular weakness of any cause and is a frequent symptom of the extra effort required to walk in upper motor neuron syndromes and basal ganglia disease.
Slowness and Stiffness
Slowness of walking is encountered in the elderly and in most gait disorders. Walking slowly is a normal reaction to unstable or slippery surfaces that cause postural insecurity and threaten balance. Similarly, those who feel their balance is less secure because of any musculoskeletal or neurological disorder walk slowly. In Parkinson disease (PD) and other basal ganglia diseases, slowness of walking is due to shuffling with short, shallow steps. Difficulty initiating stepping when starting to walk (start hesitation) and when encountering an obstacle or turning (freezing) are common in advanced stages of parkinsonian syndromes.
Difficulty rising from a chair or turning in bed and a general decline in agility may be clues to loss of truncal mobility in diffuse cerebrovascular disease, hydrocephalus, and basal ganglia diseases. Complaints of stiffness, heaviness, or “legs that do not do what they are told” may be the presenting symptoms of a spastic paraparesis or hemiparesis. Patients with spastic paraparesis frequently report that they drag their legs, catch the toes of their shoes on any surface irregularity and their legs suddenly give way, causing stumbling and falls. The circumstances in which leg stiffness occurs when walking may be revealing. It is important to remember that leg muscle tone in some upper motor neuron syndromes and dystonia may be normal when the patient is examined in the supine position but is increased during walking. In childhood, an action dystonia of the foot is a common initial symptom of primary dystonia with stiffness, inversion, and plantar flexion of the foot and walking on the toes only becoming evident after walking or running. In adults, exercise-induced foot dystonia when running may be the presenting symptom of PD. Patients with dopa-responsive dystonia typically develop symptoms in the afternoon (“diurnal fluctuation”).
Imbalance
Complaints of poor balance and unsteadiness are cardinal features of cerebellar ataxia and sensory ataxia (due to proprioceptive sensory loss). The patient with a cerebellar gait ataxia complains of unsteadiness, staggering, inability to walk in a straight line, and near falls. Turning and suddenly changing direction results in veering to one side or staggering as if intoxicated. Symptoms are exacerbated by an uneven support surface. A sensory ataxia presents with unsteadiness when walking in the dark, because visual compensation for the proprioceptive loss is not possible. Patients with impaired proprioception and sensory ataxia complain of being uncertain of the exact position of their feet when walking. They are unable to appreciate the texture of the ground beneath their feet and may describe abnormal sensations in the feet that give the impression of walking on a spongy surface or cotton wool. Acute vestibulopathy is associated with vertigo and severe imbalance. More chronic vestibular dysfunction often causes veering and problems in an environment with many moving objects such as walking in shopping malls or crowded streets with pedestrians and vehicles. Chronic vestibular lesions may be well compensated and only revealed when visual or proprioceptive input is compromised. Acute disturbances of balance and loss of truncal equilibrium also occur in vascular lesions of the cerebellum, thalamus, and basal ganglia. A wide-based unsteady gait also is a feature of frontal lobe diseases such as normal pressure hydrocephalus, diffuse small vessel ischemia of frontal subcortical white matter, and as will be discussed, higher level gait disorders. Imbalance in subcortical cerebrovascular disease and basal ganglia disorders commonly manifests when turning while walking, stepping backwards, bending over to pick up something, or performing several tasks simultaneously, such as walking and carrying an object.
Falls
Falls may be classified according to whether muscle tone is retained (“falling like a tree trunk” or toppling) or tone is lost (collapsing falls). Collapsing falls with loss of muscle tone imply a loss of consciousness characteristic of syncope or seizures. Toppling falls with retained muscle tone are due to impaired static and dynamic postural responses that control body equilibrium during standing and walking. Accordingly, it is important to establish the circumstances in which falls occur, whether consciousness was retained, and any clear precipitants or associated symptoms.
Since many people attribute falls to tripping when in fact tripping did not occur, details of how tripping occurred are important. Tripping may be due to foot drop or shallow steps and this tendency is exaggerated when walking on uneven ground. Tripping may also be a consequence of carelessness secondary to inattention, dementia, or poor vision. Proximal muscle weakness may result in the legs giving way and falls. Unsteadiness and poor balance in an ataxic syndrome may lead to falls. More commonly, apparently spontaneous falls, falls associated with postural adjustments, or falls occurring when performing multiple tasks suggest an impairment of postural responses. In the early stages of an akinetic-rigid syndrome, spontaneous falls, especially backward, are an important clue to diagnoses such as multiple system atrophy and progressive supranuclear palsy (Steele–Richardson–Olszewski syndrome) rather than PD. Falls do occur in PD but are a late feature and a number of causes must be considered. These include festinating steps that are too small to restore balance, tripping or stumbling over rough surfaces because shuffling steps fail to clear small obstacles, and failure to step because of start hesitation or freezing. In each of these examples, falling stems from locomotor hypokinesia and a lack of normal-sized, rapid, compensatory voluntary movements. These falls are forward onto knees and outstretched arms (indicating preservation of rescue reactions). Other falls, in any direction, occur when changing posture or turning in small spaces and result from loss of postural and righting responses, either spontaneously when multitasking or after minor perturbations. It is also important to consider collapsing falls related to orthostatic hypotension, a common finding in PD.
Sensory Symptoms and Pain
The distribution of any accompanying sensory complaints provides a clue to the site of the lesion producing walking difficulties. A common example is cervical spondylotic myelopathy with cervical radicular pain or paresthesias, sensations of tight bands around the trunk (due to spinal sensory tract compression), and a spastic paraparesis. Distal symmetrical paresthesias of the limbs suggest peripheral neuropathy. It is important to determine whether leg pain and weakness during walking are caused by focal pathology (a radiculopathy or neurogenic claudication of the cauda equina) or whether the pain is of musculoskeletal origin and exacerbated by walking. Neurogenic intermittent claudication of the cauda equina should be distinguished from vascular intermittent claudication in which ischemic leg muscle pain typically affects the calves and interrupts walking. Skeletal pain due to degenerative joint disease is aggravated by movement of the affected joints and often persists at rest (in contrast to claudication). The normal pattern of walking is frequently modified by joint disease (especially of the hip). Voluntary strategies to minimize pain by avoiding full weight bearing on the affected limb or by limiting its range of movement are a common cause of antalgic gait patterns, i.e., limping.
Urinary Incontinence
A spastic paraparesis with loss of voluntary control of sphincter function suggests a spinal cord lesion. Parasagittal cerebral lesions such as frontal lobe tumors (parasagittal meningioma), frontal lobe infarction caused by anterior cerebral artery occlusion, and hydrocephalus should also be considered. Impairment of higher mental function and incontinence may be important clues to a cerebral cause of paraparesis. Urinary urgency and urge incontinence are also common in parkinsonism and subcortical white-matter ischemia.
Cognitive Changes
Cognitive deterioration is associated with slowing of gait speed. Slowing of gait may be a marker of impending cognitive impairment and dementia (Mielke et al., 2013). Conversely, executive dysfunction including inattention, impaired multitasking, and set switching may predict later development of falls in older adults without dementia or impaired mobility (Mirelman et al., 2012). Dementia with disinhibition and impulsivity are associated with reckless gait problems and falls.
Examination of Posture and Walking
A scheme for the examination of posture and walking is summarized in Box 24.1. A convenient starting point is to observe the overall pattern of limb and body movement during walking. Normal walking progresses in a smooth and effortless manner. The truncal posture is upright, and the legs swing in a fluid motion with a regular stride length. Synergistic head, trunk, and upper-limb movement flow with each step. Observation of the pattern of body and limb movement during walking also helps the examiner decide whether the gait problem is caused by a focal abnormality (e.g., leg shortening, hip disease, muscle weakness) or a generalized disorder of movement, and whether the problem is unilateral or bilateral. After the overall walking pattern is observed, the specific aspects of posture and gait should be examined (see Box 24.1).
Arising from Sitting
Watching the patient arise from a chair without using the arms informs about pelvic girdle strength, control of truncal movement, coordination, and balance. Inability to arise when the feet are appropriately placed under the body while sitting and the trunk is leaning forward may indicate proximal weakness. An abnormally wide stance base when standing from a seated position often signals incoordination or imbalance. Inappropriate strategies in which the feet are not positioned directly under the body or the trunk leans backwards while trying to stand are seen in frontal lobe disease and higher level gait disorders.
Stance
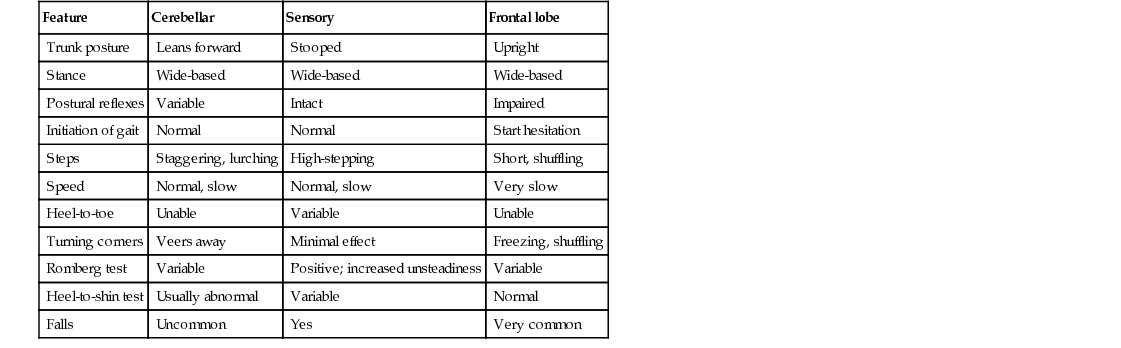
The width of the stance base (the distance between the feet) when arising from sitting, standing, and walking gives an indication of balance. Wide-based gaits are typical of cerebellar or sensory ataxia but also may be seen in diffuse cerebrovascular disease and frontal lobe lesions (Table 24.1). In mild ataxia, a widened base may only be evident with turning and disappear with walking in a straight line. Widening the stance base is an efficient method of reducing body sway in the lateral and anteroposterior planes. Persons whose balance is insecure for any reason tend to adopt a wider stance and a posture of mild generalized flexion and to take shorter steps. Those who have attempted to walk on ice or other slippery surfaces will recognize these strategies to avoid falls. Eversion of the feet is a strategy to increase stability and is particularly common in patients with diffuse cerebrovascular disease. Spontaneous sway, drift of the body in any direction, actively pushing the body out of balance to one side or backward, and ability to stay upright without seeking the support of furniture or assistance of another person are important clues to imbalance. Tandem (heel to toe) walking is a good objective measure of walking stability.
TABLE 24.1
Summary of Clinical Features Distinguishing Different Types of Gait Ataxia
| Feature | Cerebellar | Sensory | Frontal lobe |
| Trunk posture | Leans forward | Stooped | Upright |
| Stance | Wide-based | Wide-based | Wide-based |
| Postural reflexes | Variable | Intact | Impaired |
| Initiation of gait | Normal | Normal | Start hesitation |
| Steps | Staggering, lurching | High-stepping | Short, shuffling |
| Speed | Normal, slow | Normal, slow | Very slow |
| Heel-to-toe | Unable | Variable | Unable |
| Turning corners | Veers away | Minimal effect | Freezing, shuffling |
| Romberg test | Variable | Positive; increased unsteadiness | Variable |
| Heel-to-shin test | Usually abnormal | Variable | Normal |
| Falls | Uncommon | Yes | Very common |
Trunk Posture
The trunk is normally upright during standing and walking. Flexion of the trunk and a stooped posture are characteristic features in PD. Slight flexion at the hips to lower the trunk and shift the center of gravity forward to minimize posterior body sway and reduce the risk of falling backward is common in many unsteady or cautious gait syndromes. In contrast, an upright posture with neck and trunk extension is typical of progressive supranuclear palsy. Neck flexion occurs with weakness of the neck extensors in motor neuron disease and myasthenia gravis. It is also a dystonic manifestation (antecollis) in multiple system atrophy and PD. Dystonia and parkinsonism also may alter truncal posture, leading to camptocormia or lateral truncal flexion (Pisa syndrome). Tilt of the trunk to one side in dystonia is accompanied by muscle spasms, the most common being an exaggerated flexion movement of the trunk and hip with each step. Paraspinal muscle spasm and rigidity also produces an exaggerated lumbar lordosis in the stiff person syndrome.
An exaggerated lumbar lordosis, caused by hip-girdle weakness, is typical of proximal myopathies. Truncal tilt away from the side of the lesion is observed in some acute vascular lesions of the thalamus and basal ganglia. Misperception of the vertical posture and truncal tilt in posterolateral thalamic vascular lesions results in inappropriate movements to correct the perceived tilt in the “pusher syndrome” (Karnath et al., 2005). Acute vestibular imbalance in the lateral medullary syndrome leads to tilt toward the side of the lesion (lateropulsion).
Truncal flexion (camptocormia) may occur in paraspinal myopathies that produce weakness of trunk extension. Abnormal thoracolumbar postures also result from spinal ankylosis and spondylitis. A restricted range of spinal movement and persistence of the abnormal spinal posture when supine or during sleep are useful pointers toward a bony spinal deformity as the cause of an abnormal truncal posture. Truncal postures, particularly in the lumbar region, can be compensatory for shortening of one lower limb, lumbar or leg pain, or disease of the hip, knee, or ankle.
Postural Responses
Reactive postural responses are examined by “the pull test” sharply pulling the upper trunk backward or forward while the patient is standing (Hunt and Sethi, 2006). The pull should be sufficient to require the patient to step to regain their balance. The examiner must be prepared to prevent the patient from falling. A few short, shuffling steps backward (retropulsion) or an impending fall backward or forward (propulsion) suggests impairment of righting reactions. Falls after postural changes such as arising from a chair or turning while walking suggest impaired anticipatory postural responses. Falls without rescue arm movements or stepping movements to break the fall indicate loss of protective postural responses. Injuries sustained during falls provide a clue to the loss of these postural responses. A tendency to fall backward spontaneously is a sign of impaired postural reflexes in progressive supranuclear palsy and gait disorders associated with frontal lobe diseases.
Walking
Initiation of Gait
Difficulty initiating the first step (start hesitation) ranges in severity from a few short, shuffling steps, to small shallow steps on the spot without forward progress (slipping clutch phenomenon), to complete immobility with the feet seemingly glued to the floor (magnetic foot phenomenon). Patients may make exaggerated upper-body movements or alter the step pattern, such as stepping sideways or lifting the feet very high in an effort to engage their legs in motion. Isolated start hesitation is seen in the syndrome of gait ignition failure. Magnetic feet suggest frontal lobe disease, diffuse cerebrovascular disease, or hydrocephalus. Start hesitation is a feature of the “freezing gait” of PD when starting to walk.
Stepping
Once walking is underway, the length and trajectory of each step and the rhythm of stepping should be noted. Short, regular, shallow steps or shuffling and a slow gait are characteristic of the akinetic-rigid syndromes. Shuffling is most evident when starting to walk, stopping, or turning corners. Specifically examining these maneuvers may reveal a subtle tendency to shuffle and freezing. Once underway, freezing may interrupt walking, with further shuffling and start hesitation. Freezing typically occurs when turning, when walking has been interrupted by an obstacle, or visual distraction such as walking through a doorway. The small shuffling steps of freezing are often accompanied by trembling of the knees, standing on the toes, and forward tilt of the trunk. Festination (increasingly rapid, small steps) is common in PD but rare in other akinetic-rigid syndromes, which frequently are associated with poor balance and falls rather than festination. A slow gait also is seen in ataxia (sensory and cerebellar), spasticity and cautious gait syndromes but the stepping patterns differ. Jerky steps of irregular variable rhythm, length, and direction suggest ataxic or choreic syndromes. Subtle degrees of cerebellar ataxia may be unmasked by asking the patient to walk heel to toe in a straight line (tandem gait), to stand on one leg, or to walk and turn quickly. When vision is important in helping maintain balance, as in sensory ataxia caused by proprioceptive loss, the removal of vision greatly exaggerates the ataxia. This is the basis of the Romberg test, in which eye closure leads to a dramatic increase in unsteadiness and even falls in the patient with sensory ataxia. When performing the Romberg test, it is important the patient is standing comfortably before eye closure and to remember that a modest increase in body sway is a normal response to eye closure. Distinctive leg postures and foot trajectories occur during stepping in sensory ataxia, foot drop, spasticity, and dystonia. It may be necessary to examine the patient running to identify an action dystonia of the legs in the early stages of primary torsion dystonia.
Turning
Turning while walking stresses balance more than walking in a straight line and is often where gait abnormalities first appear. Slowing on turns may be the first abnormality in walking in a patient with PD. Multiple steps on turning are common in PD and diffuse cerebrovascular disease. An extra step or mild widening of the base on turning may herald the onset of ataxia.
More Challenging Tests of Walking
Walking on toes and heels may bring out abnormal movements as well as deficits in the strength of dorsiflexion and plantar flexion of the ankle. Walking backward will sometimes reduce or abolish the dystonic foot posturing observed walking forward in action dystonia of the foot.
Associated and Synergistic Limb Movements While Walking
Unilateral loss of synergistic arm swing while walking is a valuable sign of early PD but also may be seen in acute unilateral cerebellar lesions and hemiparesis. Dystonic posturing of an arm or leg may be indicative of dystonia, parkinsonism, and old hemiparesis. Choreiform movements are more prominent during walking than at rest in most chorea syndromes, levodopa-induced dyskinesia, and tardive dyskinesia. Parkinsonian tremor of the dependent upper limb is often observed while walking.
Motor and Sensory Examination
After observing the patient walk, motor and sensory function in the limbs is examined with the patient sitting or supine. The size and length of the limbs should be measured in any child presenting with a limp. Asymmetry in leg size suggests a congenital malformation of the spinal cord or brain, or (rarely) local overgrowth of tissue. The spinal column should be inspected for scoliosis, and the lumbar region for skin defects or hairy patches indicative of spinal dysraphism.
Muscle bulk and tone are examined. Changes in muscle tone such as spasticity, lead-pipe or cogwheel rigidity, or paratonic rigidity (gegenhalten) point toward diseases of the upper motor neuron, basal ganglia, and frontal lobes, respectively. In the patient who complains of symptoms in only one leg, a detailed examination of the other leg is important. If signs of an upper motor neuron syndrome are present in both legs, a disorder of the spinal cord or parasagittal region is likely. Muscle bulk and strength are examined for evidence of muscle wasting and the presence and distribution of muscle weakness. Examination reveals whether the abnormal leg and foot posture in a patient with foot drop (Box 24.2) is caused by spasticity or weakness of ankle dorsiflexors due to anterior horn cell disease, a peripheral neuropathy, a peroneal compression neuropathy, or an L5 root lesion. Joint position sense should be examined for defects of proprioception in the ataxic patient or awkward posturing of the foot. Other signs such as a supranuclear gaze palsy, ataxia, and frontal lobe release signs should be sought where relevant. The inability to tap the foot rapidly and regularly is a sign of bradykinesia. Inability to draw a circle with the foot may indicate dyspraxia as seen in corticobasal syndromes.
Discrepancies on Examination of Gait
Several conditions are notable for producing minimal abnormal signs on physical examination of the recumbent patient, in contrast to the observed difficulty when walking. A patient with cerebellar gait ataxia caused by a vermis lesion may perform the heel-to-shin test normally when supine but is ataxic when walking. The finding of normal muscle strength, muscle tone, and tendon reflexes is common in dystonic syndromes in which an action dystonia causes abnormal posturing of the feet only when walking. A dystonic gait may be evident only when running or walking forward but not when walking backward. Gegenhalten (paratonia), with or without brisk tendon reflexes, may be the only abnormal sign in the recumbent patient with a frontal lobe lesion, hydrocephalus, or diffuse cerebrovascular disease who is totally unable to walk when standing. Such patients perform the heel-shin test and make bicycling movements of their legs normally when lying on a bed. A similar discrepancy can be seen in spastic paraplegia caused by hereditary spastic paraplegia, cerebral palsy (Little disease), or cervical spondylotic myelopathy. Minor changes in muscle tone, strength, and tendon reflexes are evident during the supine examination, in contrast to profound leg spasticity when standing and attempting to walk. The leg tremor of orthostatic tremor only appears during weight bearing, especially when standing still. Incongruous signs and “give way” weakness along with bizarre sensory disturbances that do not correlate with the gait pattern often signal psychogenic disorders.
Classification of Gait Patterns
The goal of classifying gait patterns is to develop a scheme reflecting the physiological basis of human gait and help clinicians recognize the level of nervous system derangement. A scheme based on Hughlings Jackson's three orders of neurological function—lower (simplest), middle, and higher (complex, integrative)—enables a classification according to function. Each level contributes sensory and motor function, but that of higher centers is more complex and dispersed within the nervous system.
Lower Level Gait Disorders
Lower level disorders manifest physical signs such as weakness or sensory loss. Lower level motor gait disorders are due to diseases of the muscle and peripheral nerves that produce muscle weakness. Lower level sensory gait disorders follow loss of one of the three basic senses important for gait and balance: proprioception, vision, and vestibular sensation.
Myopathic Weakness and Gait
Weakness of proximal leg and hip-girdle muscles interferes with stabilizing the pelvis and legs on the trunk during all phases of the gait cycle. Failure to stabilize the pelvis produces exaggerated rotation of the pelvis with each step and a waddling gait. The hips are slightly flexed as a result of weakness of hip extension, and an exaggerated lumbar lordosis occurs. Weakness of hip extension interferes with standing from a squatting or lying position and patients push themselves up with their arms (Gower's sign). A myopathy is the most common cause of proximal muscle weakness, but neurogenic weakness of proximal muscles can also produce this clinical picture.
Neurogenic Weakness and Gait
Muscle weakness of peripheral nerve origin, as in a neuropathy, typically affects distal leg muscles and results in a steppage gait. The patient lifts the leg and foot high above the ground with each step because of weakness of ankle dorsiflexion and foot drop. When this clinical picture is confined to one leg (unilateral foot drop), a common peroneal or sciatic nerve palsy or an L5 radiculopathy is the usual cause. Less common is foot drop caused by myopathic weakness, as in the scapuloperoneal syndromes. Weakness of ankle plantar flexion produces a shallow stepped gait. A femoral neuropathy, as in diabetes mellitus, produces weakness of knee extension and buckling of the knee when walking or standing. This may first be evident when walking down stairs. Progressive muscular atrophy in motor neuron disease or a quadriceps myopathy caused by inclusion body myositis may result in similar focal weakness.
Sensory Ataxia
Loss of proprioceptive input and joint position sense from the lower limbs deprives the patient of knowledge of the position of the legs and feet in space, the progress of ongoing movement, the state of muscle contraction, and finer details of the texture of the surface on which the patient is walking. Walking on uneven surfaces is particularly difficult. Patients with sensory ataxia adopt a wide base and advance cautiously, taking slow steps under visual guidance. During walking, the feet are thrust forward with variable direction and height. The sole of the foot strikes the floor forcibly with a slapping sound (slapping gait). The absence of visual information when walking at night or during the Romberg test leads to imbalance and falls. Sensory ataxia is the result of deafferentation due to interruption of large-diameter proprioceptive afferent fibers in peripheral neuropathies, posterior root or dorsal root ganglionopathies, and dorsal column lesions.
Vestibular Imbalance, Vertigo, and Gait
Acute peripheral vestibular disorders result in leaning and unsteady veering to the side of the lesion (depending on the position of the head). Paradoxically, unsteadiness and veering while running may be less evident than when walking in acute vestibulopathy. In general, patients with an acute vestibulopathy prefer to lie still to minimize the symptoms of acute vestibular imbalance. In chronic vestibular failure, gait may be normal, though unsteadiness can be unmasked during eye closure and rotation of the head from side to side while walking. Acute vestibular imbalance in the lateral medullary syndrome leads to tilt and veering toward the side of the lesion (lateropulsion).
Middle-Level Gait Disorders
Gait disorders related to abnormalities of the middle-level motor disorders include: (1) spasticity from corticospinal tract lesions, (2) ataxia arising from disturbances of the cerebellum and its connections, (3) hypokinetic gaits associated with parkinsonism, and (4) hyperkinetic gaits associated with chorea, dystonia, and other movement disorders.
Spastic Gait
Spasticity of the arm and leg on one side produces the characteristic clinical picture of a spastic hemiparesis in which the arm is adducted, internally rotated at the shoulder, and flexed at the elbow, with pronation of the forearm and flexion of the wrist and fingers. The leg is slightly flexed at the hip and extended at the knee, with plantar flexion and inversion of the foot. The swing phase of each step is accomplished by slight lateral flexion of the trunk toward the unaffected side and hyperextension of the hip on that side to allow slow circumduction of the extended paretic leg as it swings forward from the hip, dragging the foot or catching the toe on the ground beneath. Minimal associated arm swing occurs on the affected side. The stance may be slightly widened, and the speed of walking is slow. Balance may be poor because the hemiparesis interferes with corrective postural adjustments on the affected side. Muscle tone in the affected limbs is increased, clonus may be present, and tendon reflexes are abnormally brisk, with an extensor plantar response. Examination of the sole of the shoe may reveal wear of the toe and outer borders of the shoe, suggesting that the spastic gait is of long standing. After identifying a spastic hemiparesis the site of the corticospinal tract lesion is determined by magnetic resonance imaging (MRI) of the brain (and where indicated, the spinal cord).
Spasticity of both legs gives rise to a spastic paraparesis. The legs are stiffly extended at the knees, plantar flexed at the ankles, and slightly flexed at the hips. Both legs circumduct, and the toes of the plantar flexed feet catch on the floor with each step. The gait is slow and labored as the legs are dragged forward with each step. There is a tendency to adduct the legs, particularly when the disorder begins in childhood, an appearance described as scissors gait. The causes of a spastic paraparesis include hereditary spastic paraplegia, in which the arms and sphincters are unaffected and there may be little or no leg weakness, and other myelopathies. An indication of the extent and level of the spinal cord lesion can be obtained from the presence or absence of weakness or sensory loss in the arms, a spinothalamic sensory level or posterior column sensory loss, and alterations in sphincter function. Patients with paraparesis of recent onset should be investigated with MRI of the spinal cord to exclude potentially treatable causes such as spinal cord compression.
Occasionally, bilateral leg dystonia (dystonic paraparesis) mimics a spastic paraparesis. This typically occurs in dopa-responsive dystonia in childhood and may be misdiagnosed as hereditary spastic paraplegia or cerebral diplegia. Clinical differentiation between these conditions can be difficult. Brisk tendon reflexes occur in both, and spontaneous extension of a great toe in patients with striatal disorders may be interpreted as a Babinski response. Fanning of the toes and knee flexion suggest spastic paraplegia. Other distinguishing features include changes in muscle tone, such as spasticity in hereditary spastic paraparesis and rigidity in dystonic paraparesis. In young children, the distinction is important because a proportion of such patients can be treated successfully with levodopa (discussed in the following sections).
Cerebellar Ataxia
Disease of the midline cerebellar structures, the vermis, and anterior lobe produces loss of truncal balance, increased body sway, dysequilibrium, and gait ataxia. When standing, the patient adopts a wide-based stance; the legs are stiffly extended and the hips slightly flexed to crouch forward and minimize truncal sway. The truncal gait ataxia of midline cerebellar pathology has a lurching and staggering quality that is more pronounced when walking on a narrow base or during heel-to-toe walking. A pure truncal ataxia may be the sole feature of a midline (vermis) cerebellar syndrome and escape notice if the patient is not examined when standing, because leg coordination during the heel-to-shin test may be relatively normal when examined supine. Midline cerebellar pathologies include structural lesions (masses, hemorrhage), paraneoplastic syndromes, and malnutrition in alcoholism. Patients with anterior lobe atrophy develop a 3-Hz anteroposterior sway of the trunk and a rhythmic truncal and head tremor (titubation) that is superimposed on the gait ataxia. This combination of truncal gait ataxia and truncal tremor is characteristic of some late-onset anterior lobe cerebellar degenerations.
Lesions of the cerebellar flocculonodular lobe (the vestibulocerebellum) exhibit multidirectional body sway, dysequilibrium, and severe impairment of body and truncal motion. Standing and even sitting can be impossible, although when lying down, the heel-shin test may appear normal, and upper limb function may be relatively preserved.
Limb ataxia due to involvement of the cerebellar hemispheres is characterized by a decomposition of normal leg movement. Steps are irregular and variable in timing (dyssynergia), length, and direction (dysmetria). Steps are taken slowly and carefully to reduce the tendency to lurch and stagger. These defects are accentuated when attempting to walk heel to toe in a straight line. With lesions confined to one cerebellar hemisphere, ataxia is limited to the ipsilateral limbs, and there is little postural instability or truncal imbalance if the vermis is not involved. Vascular disease and mass lesions are generally responsible for hemisphere lesions.
Cerebellar gait ataxia is exacerbated by the rapid postural adjustments needed to change direction, turn a corner or avoid obstacles, and when stopping or starting to walk. Minor support, such as holding the patient's arm during walking, and visual compensation reduce body sway in cerebellar ataxia. Eye closure may heighten anxiety about falling and increase body sway, but not to the extent observed in a sensory ataxia. Episodic ataxias produce periods of impaired gait that typically last seconds to hours. Alcohol and drug use must be considered in the differential of episodic ataxia.
Spastic Ataxia
A combination of spasticity and ataxia produces a distinctive “bouncing” gait. Such gaits are seen in multiple sclerosis, the Arnold-Chiari malformation, and hydrocephalus in young people. Gait is wide based and clonus is precipitated by standing or walking, creating a bouncing motion. Compensatory movements, made in an effort to regain balance, set up a vicious cycle of ataxic movements, clonus, and increasing unsteadiness, rendering the patient unable to stand or walk. Bouncing gaits must be distinguished from action myoclonus of the legs and cerebellar truncal tremors.
Hypokinetic (Parkinsonian) Gait
The most common hypokinetic-bradykinetic gait disturbance is that encountered in PD. In early PD, an asymmetrical reduction of arm swing and slight slowing in gait, particularly when turning, is characteristic. In more advanced PD, the posture is stooped, with flexion of the shoulders, neck, trunk, and knees. During walking, there is little associated or synergistic limb and body movement and the arms are held immobile at the sides or slightly forward of the trunk. Parkinsonian tremor of the upper limbs is often apparent when walking but leg tremor is rare during walking. A characteristic feature of a parkinsonian gait is the tendency to begin walking with a few rapid, short, shuffling steps (start hesitation) before breaking into a more normal stepping pattern with small, shallow steps on a narrow base. Once underway, walking may be interrupted by shuffling or even cessation of movement (freezing) if an obstacle is encountered, when walking through doorways, or when attempting to undertake multiple tasks at once. These signs may be alleviated by levodopa treatment. In the long term, levodopa therapy may induce dyskinesias, resulting in choreic and dystonic gaits as described later.
The posture of generalized flexion of the patient with PD exaggerates the normal tendency to lean forward when walking. To maintain balance when walking and avoid falling forward, the patient may advance with a series of rapid, small steps (festination). Retropulsion and propulsion are similar manifestations of a flurry of small, shuffling steps made in an effort to preserve equilibrium. Instead of a single large step, a series of small steps are taken to maintain balance. Freezing becomes increasingly troublesome in the later stages of PD, at which time sensory cues may be more useful in triggering a step than medication. The shuffling gait of PD that is responsive to levodopa characterizes the mid-level gait pattern. As the disease progresses, dysequilibrium and falls emerge as features of a higher level gait disorder (discussed later).
Choreic Gait
The random movements of chorea are accentuated and often most noticeable during walking. The superimposition of chorea on the trunk and leg movements of the walking cycle gives the gait a dancing quality owing to the exaggerated motion of the legs and arm swing. Chorea can also interrupt the walking pattern, leading to a hesitant gait. Additional voluntary compensatory movements appear in response to perturbations imposed by chorea. Chorea in Sydenham chorea or chorea gravidarum may be sufficiently violent to throw patients off their feet. Severe chorea of the trunk may render walking impossible. The chorea of Huntington disease causes a lurching, stumbling, and stuttering gait with steps forward, backward, or to one side. Walking is slow, the stance varies step to step but generally is wide-based and the trunk sways excessively with variable length and timing of steps. These characteristics may be misinterpreted as ataxia. Dystonic posturing such as hip or knee flexion and leg-raising movements commonly punctuate the stepping motion. Balance and equilibrium usually are maintained until the terminal stages of Huntington disease, when an akinetic-rigid syndrome may supervene. Neuroleptics such as haloperidol reduce chorea but do not improve gait in Huntington disease. Other causes of chorea can produce similar changes in gait and balance; a differential for chorea is covered in Chapters 23 and 96.
Dystonic Gait
Of all gait disturbances, dystonic syndromes produce the more bizarre and difficult diagnostic problems. The classic presentation of childhood-onset primary torsion dystonia is an action dystonia of a leg, with sustained abnormal posturing of the foot (typically plantar flexion and inversion) on attempting to run. In contrast, walking forward or backward or even running backward may be normal at an early stage. An easily overlooked sign in the early stages is tonic extension of the great toe (the striatal toe) when walking. This may be a subtle finding but occasionally is so pronounced that a hole is worn in the toe of the shoe. With the passage of time, dystonia may progress to involve the whole leg and then become generalized.
More difficult to recognize are those dystonic syndromes that present with bizarre, seemingly inexplicable postures of the legs and trunk when walking. A characteristic feature common to dystonic gaits is excessive flexion of the hip when walking. Patients may hop or walk sideways in a crab-like fashion. Hyperflexion of the hips and knee produce an attitude of general body flexion in a simian posture, or excessive flexion of the hip and knee and plantar flexion of the foot in a birdlike (peacock) gait during the swing phase of each step. Many patients have been thought to be hysterical because of these unusual gait disturbances particularly when formal neurological examination when supine is normal. Each of these gait patterns is well described in primary and secondary dystonic syndromes. Tardive dystonia following neuroleptic drug exposure may produce similar bizarre abnormalities of gait.
It is important to look for asymmetry in the assessment of childhood-onset dystonia. Hemidystonia and isolated leg dystonia in an adult suggest symptomatic or secondary dystonia, particularly when accompanied by falls due to early loss of postural responses and righting reflexes.
Dopa-responsive dystonia characteristically presents in childhood with walking difficulties and diurnal fluctuations in severity of dystonia. Typically the child walks normally in the early morning but develops increasing rigidity and dystonic posturing of the legs as the day progresses or after exercise. Symptoms may be relieved by a nap (“sleep benefit”). Examination reveals dystonic plantar flexion and inversion of the foot, with brisk tendon reflexes. Some of these patients respond dramatically to levodopa. Indeed, all children presenting with a dystonic foot or leg should have a therapeutic trial of levodopa before other therapies such as anticholinergic drugs are commenced.
Paroxysmal dyskinesias also may present with difficulty walking. Paroxysmal kinesigenic choreoathetosis may present with the sudden onset of difficulty walking as the result of dystonic postures and involuntary movements of the legs, often appearing after standing from a seated position. These attacks are typically brief, lasting a matter of seconds.
Mixed Movement Disorders and Gait
Many conditions, notably athetoid cerebral palsy, produce motor signs reflecting abnormalities at many levels of the nervous system, all of which disrupt normal patterns of walking. These include spasticity of the legs, truncal and gait ataxia, dystonia, and dystonic trunk and limb spasms. Difficulties arise distinguishing this clinical picture from that of primary torsion dystonia, which may begin at a similar age in childhood. The patient with cerebral palsy usually has a history of hypotonia and delayed achievement of developmental motor milestones, especially truncal control (sitting up) and walking. Often there is a history of perinatal injury or birth asphyxia but in a substantial proportion of patients, such an event cannot be identified. A major distinguishing feature is poor balance at an early age, which may be a contributing factor to the delay in sitting and later walking. As the child begins to walk, the first signs of dystonia and athetosis appear. The presence of spasticity and ataxia also help distinguish this condition from primary dystonia. Childhood neurodegenerative diseases may first manifest as difficulty walking with a combination of motor syndromes. A progressive course raises the possibility of a symptomatic or secondary movement disorder.
Tremor of the Trunk and Legs
Leg tremor in benign essential tremor is occasionally symptomatic, but is generally overshadowed by upper limb tremor. Trunk and leg tremor may contribute to unsteadiness in cerebellar disease (see the earlier discussion on cerebellar gait ataxia). Orthostatic tremor has a unique frequency (16 Hz) and distribution, affecting trunk and leg muscles while standing. This rapid tremor produces an intense sensation of unsteadiness often with little obvious shaking of the legs or body, which is relieved by walking or sitting down. Patients avoid standing still (e.g., in a queue) and may shuffle on the spot or pace about in an effort to relieve the unsteadiness experienced when standing still. Falls are rare. Examination reveals a rippling of the quadriceps muscles during standing, and the tremor is often only appreciated by palpation of leg muscles. Recording leg muscle electromyographic activity assists the differential diagnosis of involuntary movements of the legs when standing (Box 24.3).
Action Myoclonus
Postanoxic action myoclonus of the legs is often accompanied by negative myoclonus (asterixis) that disrupts standing and walking. Repetitive action myoclonus produces jerky movements of the legs, throwing the patient off balance. Lapses of muscle activity between the jerks (negative myoclonus) cause the patient to sag toward the ground. This sequence of events gives rise to an exaggerated bouncing appearance, which is sustainable for only a few seconds before falling or seeking relief by sitting down. Difficulty walking is one of the major residual disabilities of post-anoxic myoclonus. Many patients remain wheelchair bound as a result. The stance is wide-based, and there is often an element of cerebellar ataxia, although this may be difficult to distinguish from the effects of severe action myoclonus. Stimulus-sensitive cortical reflex myoclonus also produces a similar disorder of stance and gait, with reflex myoclonus of the quadriceps, resulting in a bouncing posture. Negative myoclonus has been described as an acute phenomenon after vascular lesions in many parts of the brain, particularly of the thalamus and frontal lobes.
Higher Level Gait Disorders
Higher level gait disorders are characterized by varying combinations of dysequilibrium (due to inappropriate or absent postural responses), falls, wide stance base, short shuffling steps, and freezing. In contrast to lower and middle-level gait patterns, formal neurological examination fails to reveal signs that adequately explain the gait disturbance, though brisk tendon reflexes and extensor plantar responses or depressed reflexes and minor distal sensory loss may be encountered. Slowness of sequential leg movement and poor truncal control are often present. Stepping patterns are influenced by environmental cues that induce freezing of gait. Freezing or falling while performing multiple simultaneous tasks is common and are important clues to the diagnosis of higher level gait disorders (Nutt, 2013; Thompson, 2007).
There are many descriptions of similar gait patterns in the literature, often focusing on one element of the gait disturbance. This has generated a variety of terms for higher level gait disorders such as apraxia of gait, magnetic gait, lower half parkinsonism, frontal gait, and marche à petits pas. Because of uncertainty about the pathophysiology of these clinical manifestations, there has been no agreement on the terminology used to describe them.
Hypokinetic Higher Level and Freezing Gait Patterns
With progression of PD, freezing of gait, dysequilibrium, loss of postural, and righting responses and falls become increasingly troublesome and, unlike the hypokinetic steps and flexed truncal posture, do not respond to increasing doses of levodopa. There is some evidence from clinical, imaging, and pathological studies to suggest that dysequilibrium in PD is mediated via mechanisms other than dopaminergic deficiency, and subcortical cholinergic projections from the pedunculopontine nucleus have been implicated (Bohnen et al., 2009).
Deep brain stimulation (DBS) of the subthalamic nucleus (STN) or globus pallidus interna (GPi) may improve or worsen gait with increased falls (Weaver et al., 2009). DBS in the region of the pedunculopontine nucleus is under investigation for dysequilibrium and freezing of gait, with mixed results (Ferraye et al., 2010).
Slowness of leg movement and shuffling occur in a variety of akinetic-rigid syndromes other than PD (Box 24.4), the most common of which are multiple system atrophy, corticobasal degeneration, and progressive supranuclear palsy (Jankovic, 2015). A number of clinical signs help distinguish among these conditions (Table 24.2). In progressive supranuclear palsy, the typical neck posture is one of extension, with axial and nuchal rigidity rather than neck and trunk flexion as in PD. A stooped posture with exaggerated neck flexion is sometimes a feature of multiple system atrophy. A distinguishing feature of progressive supranuclear palsy and multiple system atrophy is the early appearance of falls due to loss of postural and righting responses, in comparison to the preservation of these reactions in PD until later stages of the illness. There also may be an element of ataxia in these akinetic-rigid syndromes that is not evident in PD. The disturbance of postural control in progressive supranuclear palsy is coupled with impulsivity due to frontal executive dysfunction leading to reckless lurching movements during postural changes when sitting or arising, and toppling falls. Falls occur in 80% of patients with progressive supranuclear palsy and can be dramatic, leading to injury. Accordingly, the patient who presents with falls and an akinetic-rigid syndrome is more likely to have one of these conditions rather than PD. Finally, the dramatic response to levodopa that is typical of PD does not occur in these other akinetic rigid syndromes, although some cases of multiple system atrophy respond partially for a short period.
TABLE 24.2
Summary of Clinical Features Differentiating Parkinson Disease from Symptomatic Parkinsonism in Patients with an Akinetic-Rigid Gait Syndrome
| Feature | Parkinson disease | Symptomatic parkinsonism |
| Posture | Stooped (trunk flexion) | Stooped or upright (trunk flexion/extension) |
| Stance | Narrow | Often wide-based |
| Initiation of walking | Start hesitation | Start hesitation, magnetic feet |
| Steps | Small, shuffling | Small, shuffling |
| Stride length | Short | Short |
| Freezing | Common | Common |
| Leg movement | Stiff, rigid | Stiff, rigid |
| Speed | Slow | Slow |
| Festination | Common | Rare |
| Arm swing | Minimal or absent | Reduced or excessive |
| Heel-to-toe walking | Normal | Poor (truncal ataxia) |
| Postural reflexes | Preserved in early stages | Absent at early stage |
| Falls | Late (forward, tripping) | Early and severe (backward, tripping, or without apparent reason) |
In addition to the hypokinetic disorders discussed previously, diseases of the frontal lobe including tumors (glioma or meningioma), anterior cerebral artery infarction, obstructive or communicating hydrocephalus (especially normal-pressure hydrocephalus), and diffuse small vessel cerebrovascular disease (multiple lacunar infarcts and Binswanger disease) also produce disturbance of gait and balance. These pathologies interrupt connections among the frontal lobes, other cortical areas, and subcortical structures especially the striatum. The clinical appearance of the gait in frontal lobe lesions varies from a predominantly wide-based unsteady ataxic gait to an akinetic-rigid gait with slow, short steps and a tendency to shuffle. It is common for a patient to present with a combination of these features. In the early stages, the stance base is wide, with an upright posture of the trunk and shuffling when starting to walk or turning corners. There may be episodes of freezing. Arm swing is normal or even exaggerated, giving the appearance of a “military two-step” gait. The normal fluidity of trunk and limb motion is lost. In contrast, voluntary upper limb and hand movements are normal and there is a lively facial expression. This “lower half parkinsonism” is commonly seen in diffuse small vessel cerebrovascular disease. The marche à petits pas of Dejerine and Critchley's atherosclerotic parkinsonism refers to a similar clinical picture. Patients with this clinical syndrome commonly are misdiagnosed as having PD. The normal motor function of the upper limbs, retained arm swing during walking, upright truncal posture, wide-based stance, upper motor neuron signs including pseudobulbar palsy, and the absence of a resting tremor distinguish this syndrome from PD. In addition, the lower half parkinsonism of diffuse cerebrovascular disease generally does not respond to levodopa treatment (see Box 24.4). Walking speed in subcortical arteriosclerotic encephalopathy is slower than in cerebellar gait ataxia or PD (Ebersbach et al., 1999). Slowness of movement and the lack of heel-to-shin ataxia distinguish the wide-based stance of this syndrome from that of cerebellar gait ataxia (see Table 24.1).
As the underlying condition progresses, the unsteadiness and slowness of movement become more pronounced. There may be great difficulty initiating a step (start hesitation, “slipping clutch”) as if the feet were glued to the floor (“magnetic feet”). Attempts to take a step require assistance and the patient seeks support from nearby objects or persons. There may be excessive upper body movement as the patient tries to free the feet to initiate walking. Once walking is underway, steps may be better, but small, shuffling, ineffective steps (freezing) re-emerge when attempting to turn. Such patients rarely exhibit the festination of PD, but a few steps of propulsion or retropulsion may be taken. Postural and righting reactions are impaired and eventually lost. Falls are common and follow the slightest perturbation. In contrast, these patients are often able to make stepping, walking, or bicycling leg movements with the legs when seated or lying supine but cannot step or walk when standing. This discrepancy may reflect poor control of truncal motion and dysequilibrium when standing, making stepping impossible without falling (Thompson, 2007). The inability to stand from sitting or lying and difficulty turning over in bed are other signs of impaired truncal movement in the higher level gait disorder of frontal lobe gait disease. Frontal signs such as paratonic rigidity (gegenhalten) of the arms and legs, grasp reflexes in the fingers and toes, and brisk tendon reflexes with extensor plantar responses are common. Urinary incontinence and dementia frequently occur. Brain imaging with MRI reveals the majority of conditions causing this syndrome, such as diffuse cerebrovascular disease, cortical atrophy, or hydrocephalus.
Some patients display fragments of this clinical picture. Those with the syndrome of gait ignition or gait initiation failure exhibit profound start hesitation and freezing, but step size and rhythm are normal once walking is underway. Sensory cues may facilitate stepping. Balance while standing or walking is normal. These findings are similar to those seen with walking in PD, but speech and upper limb function are normal, and there is no response to levodopa. Brain imaging results are normal. This syndrome has also been described as “pure akinesia” and “primary progressive freezing of gait.” Some cases develop stuttering speech and hypokinetic handwriting. The slowly progressive evolution of symptoms suggests a degenerative condition. Follow-up studies indicate this may be one expression of progressive supranuclear palsy (Riley et al., 1994) or other neurodegenerations (Factor et al., 2006). Occasionally, isolated episodic festination with truncal flexion is encountered. Others complain of a loss of the normal fluency of stepping when walking and a conscious effort is required to maintain a normal stepping rhythm and step size. These symptoms may be associated with subtle dysequilibrium, manifesting as a few brief staggering steps to one side or a few steps of retropulsion after standing up, turning quickly, or making other rapid changes in body position. Finally, some elderly patients experience severe walking difficulties that resemble those described in frontal lobe disease. The history in these syndromes is one of gradual onset, without stroke-like episodes or identifiable structural or vascular lesions of the frontal lobes or cerebral white matter on imaging. The criteria for normal pressure hydrocephalus are not fulfilled, there are no signs of parkinsonism, and levodopa is ineffective. There is no evidence of more generalized cerebral dysfunction, as occurs in Alzheimer disease. Indeed, it is rare for patients with Alzheimer disease to develop difficulty walking until the later stages of the disease. The cause of these syndromes is unknown although it is increasingly recognized that subcortical white-matter pathology may exist without apparent MRI lesions (Jokinen et al., 2013).
Elderly Gait Patterns, Cautious Gaits, and Fear of Falling
Healthy, neurologically normal elderly people tend to walk at slower speeds than their younger counterparts. The slower speed of walking is related to shorter and shallower steps with reduced excursion at lower limb joints. In addition, stance width may be slightly wider than normal, and synergistic associated arm and trunk movements are less vigorous. The rhythmicity of stepping is preserved. These changes give the normal elderly gait a cautious or guarded appearance. Factors contributing to a general decline in mobility of the elderly include degenerative joint disease, reducing range of limb movement, and decreased cardiovascular fitness, limiting exercise capacity. These changes in the elderly gait pattern provide a more secure base to compensate for a subtle age-related deterioration in balance.
In unselected elderly populations, a more pronounced deterioration in gait and postural control may be seen. Walking speed is slower, steps are shorter, stride length is reduced, stance phase of walking is increased, and variability in stride time is increased. These changes are most marked in those who fall.
Elderly patients with an insecure gait characterized by slow short steps, en bloc turns, and falls often have signs of multiple neurological deficits, such as (1) mild proximal weakness of neuromuscular origin, (2) subtle sensory loss (mild distal light touch and proprioceptive loss, blunted vestibular or visual function), (3) mild spastic paraparesis due to cervical myelopathy, and (4) impaired truncal control as discussed earlier without any one lesion being severe enough to explain the walking difficulty. The cumulative effect of these multiple deficits may account for perceived instability and dysequilibrium. Musculoskeletal disorders, postural hypotension, and loss of confidence (especially after falls) are further factors contributing to a cautious gait pattern. In this situation, brain imaging is valuable to look for frontal and periventricular white-matter ischemic lesions that correlate with imbalance, increased body sway, falls, and cognitive decline (Baezner et al., 2008).
Falls lead to a marked loss of confidence when walking and a cautious or protected gait. A cautious gait is a normal response to the perception of impaired or threatened balance and a fear of falling. Such patients adopt a crouched posture and take short shallow steps. They may be unable to walk without support, holding onto furniture, leaning on walls, and avoiding crowded or open spaces because of a fear of falling. The gait improves dramatically when support is provided. Accordingly, a cautious gait should be interpreted as compensatory and not specific for any level of the gait classification. A formal program of gait retraining may help restore confidence and improve the ability to walk.
Perceptions of Instability and Illusions of Movement
A number of syndromes have been described in which middle-aged individuals complain of unsteadiness and imbalance associated with “dizziness,” sensations or illusions of semicontinuous body motion, sudden brief body displacements, or body tilt. These sensation symptoms develop in open spaces where there are no visible supports (space phobia) or in particular situations such as on bridges, stairs, and escalators or in crowded rooms. Such symptoms are associated with the development of phobic avoidance behavior and the syndrome of phobic postural vertigo (Brandt, 1996). Prolonged illusory swaying and unsteadiness after sea or air travel is referred to as the mal de débarquement syndrome. Past episodes of a vestibulopathy may suggest a subtle semicircular canal or otolith disturbance, but a disorder of vestibular function is rarely confirmed in these syndromes. Fear of falling and anxiety are common accompaniments. These symptoms must be distinguished from the physiological “vertigo” and unsteadiness accompanying visual-vestibular mismatch or conflict when observing moving objects, focusing on distant objects in a large panorama, or looking upward at a moving object.
Reckless Gait Patterns
Reckless gaits are seen in patients with impaired postural responses and poor truncal control who do not recognize their instability and take risks that result in falls and injuries. Such patients make inappropriate movements of the feet and trunk when sitting or standing without due caution or monitoring of body posture. The most striking examples occur in frontal dementias such as progressive supranuclear palsy and frontotemporal dementias in which impulsivity and a failure to adapt to the precarious balance are part of the cognitive decline.
Hysterical and Psychogenic Gait Disorders
A gait disorder is one of the commoner manifestations of a psychogenic, functional or hysterical movement disorder. The typical gait patterns encountered include:
1. transient fluctuations in posture while walking,
2. knee buckling without falls,
3. excessive slowness and hesitancy,
4. a crouched, stooped or other abnormal posture of the trunk,
5. complex postural adjustments with each step,
6. exaggerated body sway or excessive body motion especially brought out by tandem walking, and
7. trembling, weak legs (Hayes et al., 1999).
The more acrobatic hysterical disorders of gait indicate the extent to which the nervous system is functioning normally and capable of high-level coordinated motor skills and postural control to perform complex maneuvers. Suggestibility, variability, improvement with distraction, and a history of sudden onset or a rapid, dramatic, and complete recovery are common features of psychogenic gait (and movement) disorders in general. A classical discrepancy is illustrated by the Hoover sign in the patient with an apparently paralyzed leg when examined supine. As the patient lifts the normal leg, the examiner places a hand under the “paralyzed” leg and feels the presence (and strength) of synergistic hip extension. The general neurological exam often reveals a variety of other signs suggestive of psychogenic origin such as “give way weakness” and nonphysiological sensory disturbances. One must be cautious in accepting a diagnosis of hysteria, however, because a bizarre gait may be a presenting feature of primary torsion dystonia, and unusual truncal and leg postures may be encountered in truncal and leg tremors. Finally, higher level gait disorders often have a disconnect between the standard neurological exam and the gait pattern.
Musculoskeletal Disorders and Antalgic Gait
Skeletal Deformity and Joint Disease
Degenerative osteoarthritis of the hip may produce leg shortening in addition to mechanical limitation of leg movement at the hip, giving rise to a waddling gait or a limp. Leg shortening with limping in childhood may be the presenting feature of hemiatrophy due to a cerebral or spinal lesion or spinal dysraphism. Examination of the legs may reveal lower motor neuron signs, sensory loss with trophic ulcers of the feet, and occasionally, upper motor neuron signs such as a brisk knee reflex. Lumbosacral vertebral abnormalities (spina bifida), bony foot deformities, and a cutaneous hairy patch over the lumbosacral region are clues to the diagnosis. In adult life, spinal dysraphism (diastematomyelia with a tethered cord) may first become symptomatic after a back injury, with the development of walking difficulties, leg and lower back pain, neurogenic bladder disturbances, and sensory loss in a leg. Imaging of the spinal canal reveals the abnormality.
Painful (Antalgic) Gaits
Most people at one time or another experience a limp caused by a painful or an injured leg. Limps and gait difficulties due to joint disease, bone injury, or soft-tissue injury are not usually accompanied by muscle weakness, reflex change, or sensory loss. Limitation of the range of joint movement at the hip, knee, or ankle to reduce pain leads to short steps with a fixed leg posture. Hip disease causes a variety of gait adjustments; it is important to examine the range of hip movements (while supine) and any associated pain during passive movements of the hip in a patient with a gait disorder. Pain due to intermittent claudication of the cauda equina is most commonly caused by lumbar spondylosis and, rarely, by a spinal tumor. Diagnosis is confirmed by spinal imaging. It may be difficult to distinguish this syndrome from calf muscle claudication secondary to peripheral vascular disease. Examination after exercise may resolve the issue by revealing a depressed ankle jerk or radicular sensory loss, with preservation of arterial pulses in the leg. Other painful conditions affecting the spine, lower limbs, and soft tissue, such as plantar fasciitis, can affect gait.