Cultural Competence
CULTURAL CARE

http://evolve.elsevier.com/Jarvis/
Who am I? Where do I come from? What is my heritage—my cultural background—my ethnicity and religion? What is my primary language? Do I understand, speak, and read a language other than English? What are my HEALTH* and ILLNESS* beliefs and practices? You must also ask, WHO is the person whom I am meeting for the first time? Where does he or she come from? What is the person’s heritage? What is the person’s cultural background—his or her ethnicity and religion? Does the person understand, speak, and read English? What language does the person understand, speak, and read? What are the person’s HEALTH and ILLNESS beliefs and practices?
Over the course of your professional education, you will study the physical examination and health promotion across the life span and learn to conduct numerous assessments, such as a complete health history, a mental health assessment, a domestic violence assessment, a nutritional assessment, a pain assessment, and a physical examination, on a patient. However, depending on the heritage of the person, there may be wide variations in the information you gather in the assessments and in the findings of the physical examination. Therefore a Heritage Assessment must be an integral component of a complete physical and health assessment.
The purpose of this chapter is:
1. To discuss the demographic profile of the United States
2. To describe the National Standards for Culturally and Linguistically Appropriate Services in Health Care
3. To discuss the background of the heritage assessment
4. To describe the methods for conducting the heritage assessment
5. To provide examples of traditional HEALTH and ILLNESS beliefs and practices
Demographic Profile of the United States
The population of the United States approached 310 million people in the summer of 2010.22 About 1 in 8 people was an immigrant, and about 1 in 3 U.S. residents was part of a group other than single-race non-Hispanic white. The nation’s minority, actually emerging majority, population totaled 102.5 million people, or 34% of the country’s total population, in 2007. Of these, Hispanics, 15.1%, are the largest and fastest growing population. The second largest population is Asians, followed by Blacks, American Indians and Alaska natives, and Native Hawaiians and other Pacific Islanders. The findings from estimates of the U.S. population illustrate the increasing diversity in the population and contribute to the rationale for learning about the cultural aspects of health and illness from the point of view of the person seeking health care.3
The median age of the total population in 2007 was 36.6 years, and one fourth of these were younger than 18 years. Some population groups were younger than the total population as a whole. The median ages of those younger groups were Hispanics (27.6 years), Blacks (31.1 years), American Indians and Alaskan Natives (30.3 years), and Native Hawaiian/Pacific Islanders (30.2 years). These younger population groups also had close to one third of their members younger than 18 years of age. On the other hand, the non-Hispanic single-race white population was older than the population as a whole: the respective median ages were 40.8 and 36.6 years. About 21% of the population of this group were younger than 18 years, compared with 25% of the total population.3
Immigration
The 21st century began with the country in the midst of the greatest wave of immigration in its history.5 The largest numbers of people ever to enter this nation happened during the 1990s, and the numbers of immigrants have more than tripled since the 1990s. The growth in immigration has been driven in part by legislative increases in legal admissions in 1965, 1976, and 1990 when refugees were admitted from Southeast Asia and other war-torn nations. The question “Can we accommodate this number of people?” is not much different from questions raised during other large waves of immigration. Other critical questions to ask are “What will be the impact on health care delivery and nursing practice?” and “How do the health care system and nursing meet the health care needs of people from diverse backgrounds?”
Immigrants are people who were not U.S. citizens at birth. In March 2003, the population in the United States included 33.5 million foreign-born people, representing 11.7% of the U.S. population. In 2008, a total of 1,107,126 people became legal permanent residents of this country. Among the foreign born, 44.4% were born in Central and South America, 34.6% in Asia, 10.8% in Europe, and the remaining 10.2% in other regions of the world.17 The foreign-born population from Central America and Mexico accounted for more than two thirds of the foreign born from Latin America and more than one third of the total foreign born. It was estimated in January 2008 that there are also 11.6 million people who were foreign born and living here without legal documents. The sociopolitical questions that are constantly raised about the undocumented segment of the overall population relate to issues such as rights to health care and education.9
There are several terms and categories of immigrant populations that are of interest to health care providers10:
• Legal Resident—All persons who were granted lawful permanent residence
• Naturalization—The conferring, by any means, of citizenship upon a person after birth
• Non-immigrant—An alien who seeks temporary entry to the United States for a specific purpose
• Parolee—An alien, appearing to be inadmissible to the inspecting officer, allowed into the United States for urgent humanitarian reasons or when that alien’s entry is determined to be for significant public benefit
• Permanent Resident Alien—An alien admitted to the United States as a lawful permanent resident
• Refugee—Any person who is outside his or her country of nationality who is unable or unwilling to return to that country because of persecution or a well-founded fear of persecution
• Unauthorized Residents—All foreign-born non-citizens who are not legal residents
Many new immigrants have minimal understanding of the modern health care delivery system and modern medical and nursing practices, and they speak and understand minimal or no English. Yet, it is imperative that your care be tailored to meet these immigrants’ perceived needs.
New National Standards
In response to the demographic change and with knowledge that immigration was going to remain at high levels, the Office of Minority Health, an office with the Cabinet of Health and Human Services, published the National Standards for Culturally and Linguistically Appropriate Services in Health Care in 2001. The first and landmark standard states: “Health care organizations should ensure that patients receive from all staff members effective, understandable, and respectful care that is provided in a manner compatible with their cultural health beliefs and practices and preferred language”14 (Table 2-1).
• EFFECTIVE CARE results in positive outcomes and satisfaction for the patient.
• RESPECTFUL CARE takes into consideration the values, preferences, and expressed needs of the patient.
• CULTURAL AND LINGUISTIC COMPETENCE is a set of congruent behaviors, attitudes, and policies that come together in a system among professionals that enables work in cross-cultural situations (Fig. 2-1).

2-1
Linguistic Competence
Under the provisions of Title VI of the Civil Rights Act of 1964, when people with limited English proficiency (LEP) seek health care in health care settings such as hospitals, nursing homes, clinics, daycare centers, and mental health centers, services cannot be denied to them. There are many forms of illegal discrimination based on race or national origin that frequently limit the opportunities of people to gain equal access to health care services. It is said that “language barriers have a deleterious effect on health care, patients are less likely to have a usual source of health care, and have an increased risk of nonadherence to medication regimens.”6
The United States is home to millions of people from different national origins. English is the predominant language of the United States. However, 12% of the people living in the United States from 2005 to 2007 were foreign born. Among people at least 5 years old living in the United States from 2005 to 2007, 20% spoke a language other than English at home. Of those speaking a language other than English at home, 62% spoke Spanish and 38% spoke some other language; 44% reported that they did not speak English “very well.” The most common non-English languages spoken by people older than 5 years at home are Spanish, Chinese, French, German, and Tagalog (2.6%). Vietnamese, Italian, Korean, and Russian and Polish are next among the top 10 languages.21
People who are limited in their ability to speak, read, write, and understand the English language encounter countless language barriers that can result in limiting their access to critical public health, hospital, and other medical and social services to which they are legally entitled. Many health and social service programs provide information about their services in English only. When LEP persons seek health care at hospitals or medical clinics, they are frequently faced with receptionists, nurses, and physicians who speak English only. The language barrier faced by LEP persons in need of medical care or social services severely limits the ability to gain access to these services and to participate in these programs. In addition, the language barrier often results in the denial of medical care or social services, delays in the receipt of such care and services, or the provision of care and services on the basis of inaccurate or incomplete information. Services denied, delayed, or provided under such circumstances could have serious consequences for a LEP person as well as for a provider of medical care. Some states (e.g., California, Massachusetts, New York) recognize the seriousness of the problem and require providers to offer language assistance to patients in health care settings.
Chapter 3 describes in more detail how to communicate with people who do not understand English, how to interact with interpreters, and what services are available when no interpreter is available. It is vital that interpreters be present who not only serve to verbally translate the conversation but who also can describe to you the cultural aspects and meanings of the person’s situation.
Health Disparities
A health disparity is the unusual and disproportionate frequency of a given health problem (e.g., diabetes, hypertension, certain cancers) within a population when compared with other populations. Disparities occur in a broader social and economic context. The factors that contribute to this phenomenon are multilevel and complex and include the health care system, health care providers, health care managers, and patients/families/communities. It is expected that, over time, this major problem in the delivery of health care in the United States will be overcome with the increasing knowledge and research necessary for the provision of culturally competent health care.8
Cultural Competence and CULTURAL CARE
One response to the government mandates for cultural competency is the development of CULTURAL CARE, a concept that describes professional health care that is culturally sensitive, appropriate, and competent. There is a discrete body of knowledge relevant to this, and much of the content is introduced in this chapter.
• Culturally sensitive implies that caregivers possess some basic knowledge of and constructive attitudes toward the diverse cultural populations found in the setting in which they are practicing.
• Culturally appropriate implies that the caregivers apply the underlying background knowledge that must be possessed to provide a given person with the best possible HEALTH CARE.
• Culturally competent implies that the caregivers understand and attend to the total context of the individual’s situation, including awareness of immigration status, stress factors, other social factors, and cultural similarities and differences.20
CULTURAL CARE is critical to meeting the complex nursing care needs of a given person, family, and community. It is the provision of health care across cultural boundaries and takes into account the context in which the patient lives as well as the situations in which the patient’s health problems arise.20 Each chapter in this text will include information necessary for delivery of CULTURAL CARE.
More and more institutions are mandating that those who practice must be culturally competent; there are countless ways by which this can be achieved. However, it is NOT a one-lesson program but, rather, a lifetime journey of study and learning. Given the changes in the demographic profile of the United States and the enormous impact that immigration is having in this situation, it becomes imperative that a body of knowledge must be developed to meet this challenge. There are several discrete areas in which you must have knowledge:
Heritage
A given person’s heritage is predicated on the concept of heritage consistency. Heritage consistency is a concept that describes “the degree to which one’s lifestyle reflects his or her respective American Indian tribal culture.”4 The theory has been expanded in an attempt to study the degree to which a person’s lifestyle reflects his or her traditional heritage, whether it is American Indian, European, Asian, African, or Hispanic. The values indicating heritage consistency exist on a continuum, and a person can possess value characteristics of both a heritage consistent (traditional—that is, living within the norms of the traditional culture) and a heritage inconsistent (modern—that is, acculturated to the norms of the dominant society). The concept of heritage consistency includes a determination of a person’s cultural, ethnic, and religious background and socialization experiences.20
Culture
There is no single definition of culture, and too often, definitions tend to omit salient aspects of culture or are too general to have any real meaning. One example of a definition of culture is that it is the thoughts, communications, actions, beliefs, values, and institutions of racial, ethnic, religious, or social groups. Culture is a complex whole in which each part is related to every other part. It is learned, and the capacity to learn culture is genetic, but the subject matter is not genetic and must be learned by each person in his or her family and social community. Culture also depends on an underlying social matrix, and included in this social matrix are knowledge, belief, art, law, morals, and customs. Culture is also a web of communication, and much of culture is transmitted nonverbally.20
In addition, culture has four basic characteristics in that it is (1) learned from birth through the processes of language acquisition and socialization, (2) shared by all members of the same cultural group, (3) adapted to specific conditions related to environmental and technical factors and to the availability of natural resources, and (4) dynamic and ever changing.
Culture is a universal phenomenon without which no person exists. Yet the culture that develops in any given society is always specific and distinctive, encompassing all the knowledge, beliefs, customs, and skills acquired by members of that society. Within cultures, groups of people share different beliefs, values, and attitudes. Differences occur because of ethnicity, religion, education, occupation, age, and gender. When such groups function within a large culture, they are referred to as subcultural groups.
Ethnicity
Cultural background is a fundamental component of your ethnic background. Ethnicity pertains to a social group within the social system that claims to possess variable traits such as a common geographic origin, migratory status, religion, race, language, shared values, traditions, or symbols, and food preferences.
The term ethnic has aroused strongly negative feelings and often is rejected by the general population. In a nation as large as the United States and comprising as many different peoples as it does—with the American Indians being the only true native population—we find ourselves still reluctant to speak of ethnicity and ethnic differences. This stance stems from the fact that most foreign groups that came to this land often shed the ways of the “old country” and quickly attempt to assimilate themselves into the mainstream, or the so-called melting pot.15 There are at least 106 ethnic groups and more than 500 American Indian nations in the United States. People from every nation on earth are now residing in this country20 (Fig. 2-2).

2-2
Religion
The third major component of a person’s heritage is religion. Religion is the belief in a divine or superhuman power or powers to be obeyed and worshipped as the creator(s) and ruler(s) of the universe. A system of beliefs, practices, and ethical values is a major reason for the development of ethnicity.1 Religion may be seen as a shared experience of spirituality or as the values, beliefs, and practices that people are either born into or may adopt to meet their personal spiritual needs through communal actions such as religious affiliation; attendance and participation in a religious institution, prayer, or meditation; and religious practices.
On the other hand, spirituality may be seen as focusing more on the self and includes belief systems other than religion.18 The practice of religion is revealed in numerous cults, sects, denominations, and churches. Ethnicity and religion are clearly related, and religion quite often is the determinant of ethnic group. Religion gives a person a frame of reference and a perspective with which to organize information. Religious teachings vis-á-vis health help present a meaningful philosophy and system of practices within a system of social controls having specific values, norms, and ethics. These are related to health in that adherence to a religious code is conducive to spiritual harmony and health. Illness is sometimes seen as the punishment for the violation of religious codes and morals.
Religion plays a most significant role in the ways people practice their health care. Too often, this aspect of the person is ignored, and in many settings, the question “What is your religious preference?” is not asked. This may be to protect against discrimination based on religion. Yet, religion is seen as the domain of life beyond the body and mind.12 The following are examples of how religion influences the health practices of countless people:
1. Religious affiliation and membership benefit health by promoting health behavior and lifestyles.
2. Regular religious fellowship benefits health by offering social support that buffers and affects stress and isolation.
3. Faith benefits health by leading to thoughts of hope, optimism, and positive expectation.
There are countless health-related behaviors promoted by nearly all religions. The following list presents selected examples. Not every religion speaks to each point: meditating, exercising and maintaining physical fitness, getting enough sleep, being vaccinated, being willing to have the body examined, undertaking a pilgrimage for HEALTH reasons, telling the truth about how you feel, maintaining family viability, hoping for recovery, coping with stress, undergoing genetic screening and counseling, being able to live with a handicap, and caring for children.12
As an integral component of the person’s culture, religious beliefs may influence the person’s explanation of the cause(s) of illness, perception of its severity, and choice of healer(s). In times of crisis, such as serious illness and impending death, religion may be a source of consolation for the person and for his or her family. Religious dogma and spiritual leaders may exert considerable influence on the person’s decision making concerning acceptable medical and surgical treatment, choice of healer(s), and other aspects of the illness.
Spirituality and Religion
Religious concerns evolve from and respond to the mysteries of life and death, good and evil, and pain and suffering. In health care settings, you frequently encounter people who find themselves searching for a spiritual meaning to help explain their illnesses or disabilities. Some health care providers find spiritual assessment difficult because of the abstract and personal nature of the topic, whereas others feel quite comfortable discussing spiritual matters. Comfort with your own spiritual beliefs is the foundation for effective assessment of spiritual needs in others.
An important distinction needs to be made between spirituality and religion. Spirituality is borne out of each person’s unique life experience and his or her personal effort to find purpose and meaning in life.18 Although the religions of the world offer various interpretations to many of life’s mysteries, most people seek a personal understanding and interpretation at some time in their lives. Ultimately, this personal search becomes a pursuit to discover a supreme being (called by names such as Allah, God, Yahweh, and Jehovah) or some unifying truth that will render meaning, purpose, and integrity to existence.
Religion, on the other hand, refers to an organized system of beliefs concerning the cause, nature, and purpose of the universe, especially belief in or the worship of God or gods. An extensive new survey by the Pew Forum on Religion and Public Life details statistics on religion in America.16 The study found that religious affiliation in the United States is both very diverse and extremely fluid. The number of people who say they are unaffiliated with any particular faith is now 16.1%. Those reporting religious affiliation with a Christian church number 78.4%. The Christian denominations include Roman Catholic (23.9%); Protestant (51.3%), which includes Mainline Protestant (18.1%), Evangelical Churches (26.3%), and Historical Black Churches (6.9%); Mormon or Church of Jesus Christ of Latter-Day Saints (1.3%); Jehovah’s Witness (0.7%); and others. Those belonging to non-Christian and other religions total 4.7% of the U.S. population; of these, the largest group is Jewish (1.7%), followed by Buddhist (0.7%), Muslim (0.6%), and Hindu (0.4%).
The Landscape Survey also found that among the foreign-born adult population, Catholics outnumbered Protestants by nearly a two-to-one margin (46% Catholic vs. 24% Protestant) and that immigrants are also disproportionately represented among several world religions in the United States, including Islam, Hinduism, and Buddhism.16 Religious identification among people from different racial and ethnic groups is important because religion and culture are interconnected and play a critical role in HEALTH beliefs and practices.
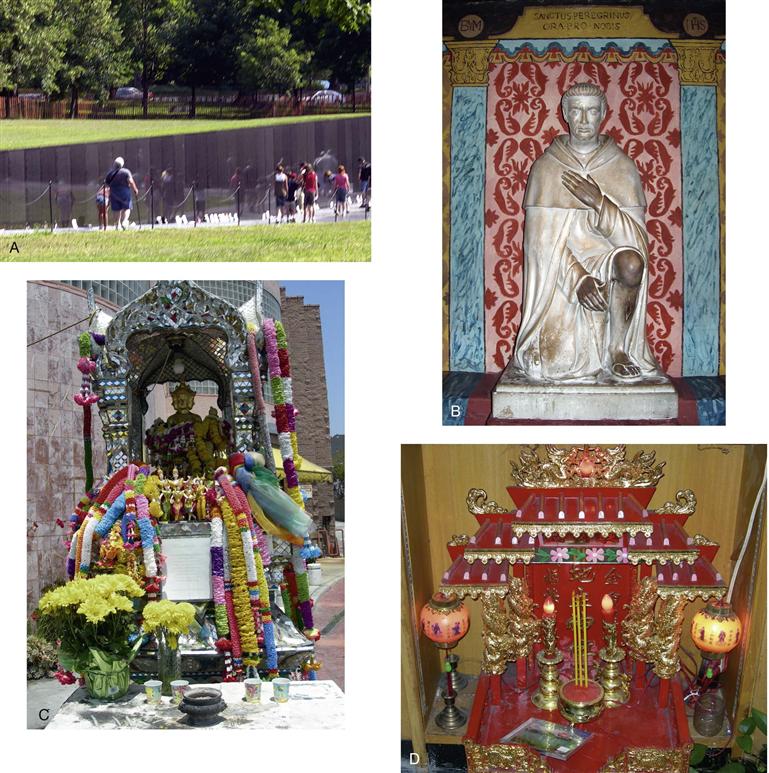
There are many examples of how spirituality and religion are apparent in daily life and frequently play a role in one’s HEALTH. Shrines are an essential component of this. There are countless shrines, both secular and from a religious tradition, where people visit to remember and/or to pray for favors or healing. Fig. 2-3, A is an image of the Vietnam Memorial Wall in Washington, DC, an example of a secular/spiritual shrine where people go to remember loved ones who died in the Vietnam War. Fig. 2-3, B is a statue of Saint Peregrine, the patron saint of people with cancer. This statue is in the chapel in the Mission San Juan Capistrano in California. Fig. 2-3, C is the Thai Spirit House, in Los Angeles, California. The shrine is on a public street and visited by believers; offerings such as flowers and food are frequently left at the base. Fig. 2-3, D is an example of a sacred Buddhist shrine that can be found in a store or in a home.
Just as the trends in immigration have influenced our newest citizens, there has been a growing interest in the religious preferences of the oldest group, the American Indians. The religious profile of American Indians is similar to that of non-Hispanic whites: 20% identified themselves as Baptist, 17% as Catholic, and 17% indicated no religious preference. Only 3% indicated their primary religious identification as a tribal Indian religion, perhaps a reflection of the growing number of native people who reside in non-reservation urban centers.1a
Socialization
Socialization is the process of being raised within a culture and acquiring the characteristics of that group. Education—be it elementary school, high school, college, or professional school—is a form of socialization. For many people who have been socialized within the boundaries of a “traditional culture” or a non-modern culture (usually associated with the East or with developing nations), modern “American,” or Western, first-world culture becomes a second cultural identity. Those who immigrate here (legally or illegally) from non-Western or non-modern countries may find socialization into the American culture, whether in schools or in society, to be an extremely difficult and painful process. As time passes, many people experience biculturalism, which is a dual pattern of identification and often of divided loyalty.11 In addition, many people who have been socialized in cultures in which traditional health care resources are used may prefer to use this type of care even when residing in a modern cultural setting with modern health care resources available.
It is not possible to isolate the aspects of culture, religion, ethnicity, and socialization that shape a person’s worldview. Each is part of the other, and all are united within the person. When we write of religion, we cannot eliminate culture or ethnicity but descriptions and comparisons can be made.
There are several other terms related to socialization:
• Acculturation—the process of adapting to and acquiring another culture
• Assimilation—the process by which a person develops a new cultural identity and becomes like the members of the dominant culture
• Biculturalism—dual pattern of identification and often of divided loyalty
Not only is it vital that you develop the skills for conducting heritage assessments, but also it is equally important that, as you learn these concepts, you understand that the first step in developing CULTURAL COMPETENCY is to know yourself. Thus, as you examine the factors related to heritage consistency and the assessment questions used in a heritage assessment, ask these questions of yourself and your family.
Heritage Assessment
The following are the factors indicative of heritage consistency, with examples, that may be explored to determine the depth to which you and the given patient identify with a traditional heritage; that is, the cultural beliefs and practices of the family, the extended family, and an ethnoreligious community20:
1. Childhood development occurred in the country of origin or in an immigrant neighborhood in the United States of like ethnic and religious group: Where were you born? Where did you grow up?
Both you and the person were raised in a specific ethnic neighborhood, such as an Italian, Black, Hispanic, or Jewish one, in a given part of a city and were exposed only to the culture, language, foods, and customs of that particular group.
2. Extended family members encouraged participation in traditional religious and cultural activities: Did your parents encourage you to participate in religious or ethnic activities? What kind of school did you go to? Did you go to a special religious school after regular school hours?
Parents and members of the extended family and ethnoreligious community encouraged the person to know his or her ethnocultural heritage and sent the person to religious (parochial) school, and most social activities were church related.
3. The person engages in frequent visits to the country of origin or returns to the “old neighborhood” in the United States: Have you visited the nation(s) or neighborhoods where your family originated?
The desire to return to the old country or to the old neighborhood is expressed by many people; however, many people, for various reasons, cannot return to the “old country or neighborhood.” The people who came here to escape religious persecution or whose families were killed during World War II, during the Holocaust, in the killing fields of Cambodia, or other recent massacres may not want to return to European or other homelands. Other reasons why people may not return to their native countries include political conditions in the homeland or lack of relatives or friends in that land.
4. The person’s family home is within the ethnic community of which he or she is a member: Who are the people living in the neighborhood where you now live?
As an adult, the person has elected to live with his or her family in the ethnic neighborhood or community wherein the people are from a similar heritage.
5. The person participates in ethnic cultural events, such as religious festivals or national holidays, sometimes with singing, dancing, and costumes: Do you participate in ethnic celebrations from your heritage?
The person is active in social and cultural groups and participates in festivities of his or her family. One example is the August festival of Saint Anthony that is celebrated by people of Italian descent in the Northeast.
6. The person was raised in an extended family setting: Who lived in your home? Were they related to you?
When the person was growing up, there may have been grandparents living in the same household or aunts and uncles living in the same house or close by. The person’s social frame of reference was the family and the extended family.
7. The person maintains regular contact with the extended family: Do you maintain ties to family?
The person maintains close ties, either with visits or telephone contact, with family members of the same generation, surviving members of the older generation, and members of the younger generation. This includes aunts, uncles, and cousins.
8. The person’s name has not been Americanized: Was your family name changed when the family came to the United States? Was the name changed to facilitate assimilation?
Many people’s surnames were changed, either by immigration officials when they entered the country or by personal choice to make their names more “American” as an attempt to assimilate to the dominant culture more fully.
9. The person was educated in a parochial (nonpublic) school with a religious or ethnic philosophy similar to the family’s background: What school did you go to? Was it public or private?
The person’s education plays an enormous role in socialization, and the major purpose of education is to socialize a given person into the dominant culture. Children learn English and the customs and norms of American life in the schools. In the parochial or private schools, they not only learn English but also are socialized in the culture and norms of the particular religious or ethnic group that is sponsoring the school.
10. The person engages in social activities primarily with others of the same religious or ethnic background: Who are your friends, and how often do you spend time with them?
For example, the major portion of the person’s personal time is spent with family and friends from his or her ethnocultural or religious community.
11. The person has knowledge of the culture and language of origin: Do you speak or read the language of your parents or grandparents?
For example, the person has been socialized in the traditional ways of the family and expresses this as a central theme of life.
12. The person expresses pride in his or her heritage: Do you identify as an ethnic American or as an American?
For example, the person may identify himself or herself as ethnic American and be supportive of ethnic activities to a great extent.
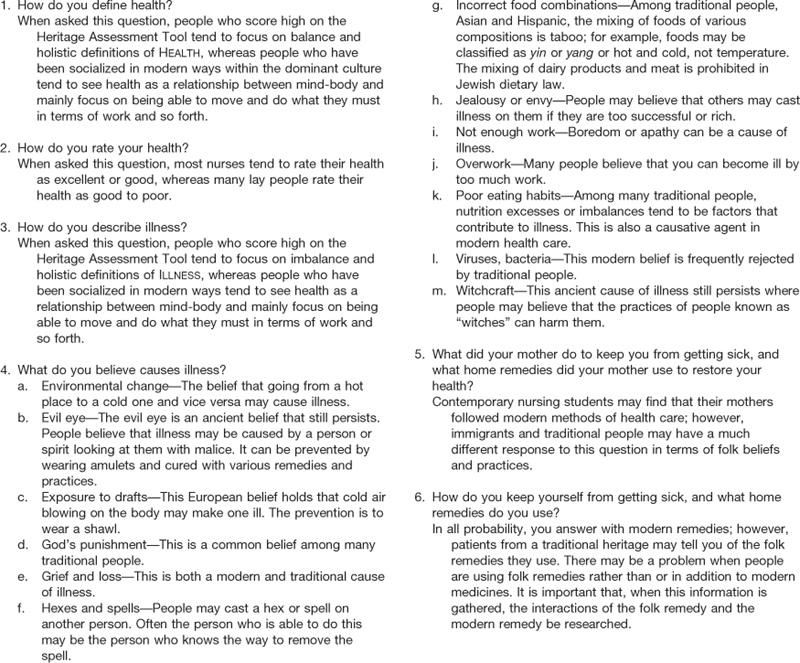
Fig. 2-4, the Heritage Assessment tool, lists all of the questions that may be asked. It is important to ask the questions slowly over time. If the person appears anxious, it is best to postpone asking the questions or to weave the questions into other parts of the health history. The responses can be scored, and an image arises as to whether the person identifies with his or her traditional heritage or whether the person is acculturated and assimilated into the mainstream of modern American culture.
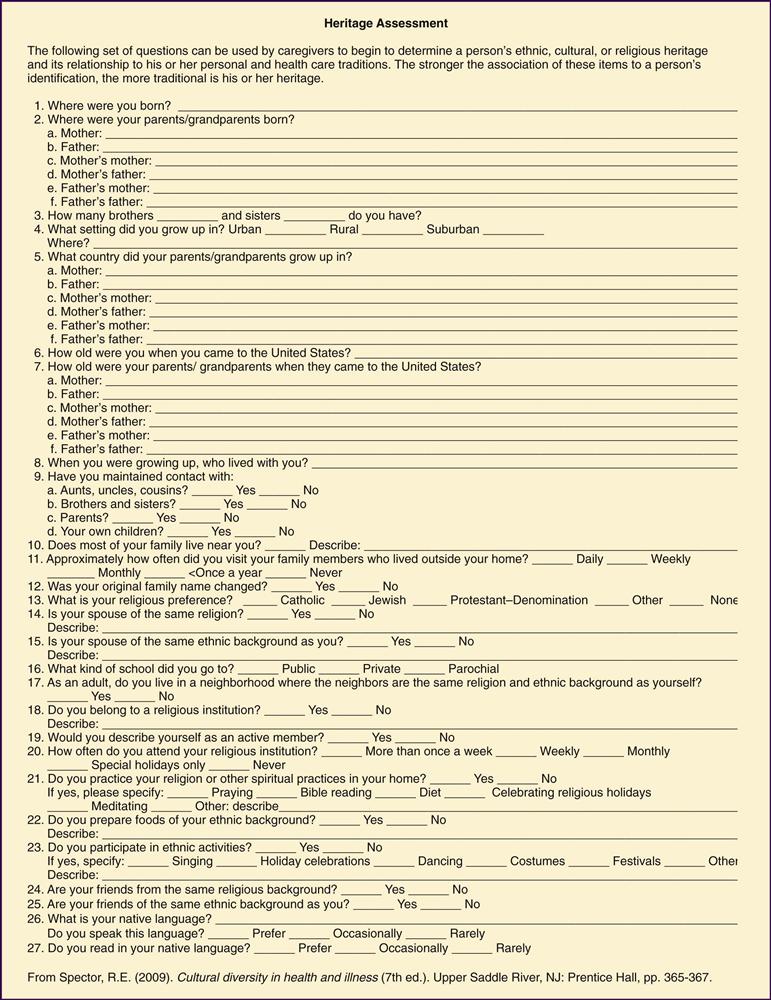
2-4
There are four short questions that may be asked in addition to the background information:
1. Do you mostly participate in social activities with members of your family?
2. Do you mostly have friends from a similar cultural background as you?
3. Do you mostly eat the foods of your family’s tradition?
4. Do you mostly participate in the religious traditions of your family?
If the person answers two to four of these questions positively, the probability of being more likely to use health practices relevant to their traditional heritage is high.
Health-Related Beliefs and Practices
Earlier in this chapter, HEALTH was defined as the balance of the person, both within one’s being (physical, mental, or spiritual) and in the outside world (natural, communal, or metaphysical) as a complex, interrelated phenomenon. Before determining whether cultural practices are helpful, harmful, or neutral, you must first understand the logic of the traditional belief systems underlying the beliefs and practices that are derived from a person’s heritage; then be certain that you fully grasp the nature and meaning of the HEALTH practice from the person’s cultural perspective.
Wide cultural variation exists in the manner in which certain symptoms and disease conditions are perceived, diagnosed, labeled, and treated. You should not assume that the perceived symptoms or complaints of patients are equivalent to the names of recognized diseases or syndromes familiar to nurses, physicians, and other health care professionals.23 The same disease that is considered grounds for social ostracism in one culture may be reason for increased status in another. For example, epilepsy is seen as contagious and untreatable among Ugandans, as a cause for family shame among Greeks, as a reflection of a physical imbalance among Mexican Americans, as the entry of a “spirit” into the person’s body by the Hmong, and as a sign of having gained favor by enduring a trial by God among the Hutterites.
Bodily symptoms are also perceived and reported in a variety of ways. For example, people of Mediterranean descent tend to report common physical symptoms more often than persons of Northern European or Asian heritage. Among Chinese, no translation exists for the English word “sadness,” yet all people experience the feeling of sadness at some time in life. To express emotion, Chinese patients somaticize their symptoms, or convert mental experiences or states into bodily symptoms (e.g., complain of cardiac symptoms because the center of emotion in the Chinese culture is the heart). You may collect in-depth data about the cardiovascular system only to learn subsequently that all diagnostic tests are negative. On further assessment, you may determine that the person has experienced a loss and is grieving (e.g., has experienced the death of a close relative or friend or has been divorced or separated). This is recognized as a culturally acceptable somatic expression of emotional disharmony.
For patients, symptom labeling and diagnosis depend on the degree of difference between the person’s behaviors and those the group has defined as normal, beliefs about the causation of illness, level of stigma attached to a particular set of symptoms, prevalence of the pathologic condition, and the meaning of the illness to the person and his or her family.
Throughout history, humankind has attempted to understand the cause of illness and disease. Theories of causation have been formulated on the basis of ethnic identity, religious beliefs, social class, philosophic perspectives, and level of knowledge. You need to determine what the person believes has caused the illness. Many people who maintain traditional beliefs would define HEALTH in terms of balance and ILLNESS a loss of this balance. The understanding tends to include the balance of mind, body, and spirit in the overall definitions of HEALTH and ILLNESS.
 Developmental Competence
Developmental Competence
Illness during childhood may be an especially difficult clinical situation. Children and adults have spiritual needs that vary according to the child’s developmental level and the religious climate that exists in the family. Parental perceptions about the illness of the child may be partially influenced by religious beliefs. For example, some parents may believe that a transgression against a religious law is responsible for a congenital anomaly in their offspring. Other parents may delay seeking medical care because they believe that prayer should be tried first. Certain types of treatment (e.g., administration of blood; medications containing caffeine, pork, or other prohibited substances) and selected procedures may be perceived as cultural taboos—that is, practices to be avoided (by both children and adults).
Values held by the dominant United States and Canadian culture, such as emphasis on independence, self-reliance, and productivity, influence aging members of society. North Americans define people as old at the chronologic age of 65 years and then limit their work, in contrast to other cultures in which persons are first recognized as being unable to work and then are identified as being “old.” The generation born just before or at the end of World War II (1940-1949) comprises the early range of older adults who are eligible for Social Security and Medicare.
In adopting a cultural perspective in working with aging individuals from culturally diverse backgrounds, you should consider that the main task of the person is to achieve a sense of integrity in accepting responsibility for his or her own life and in gaining a sense of accomplishment. Individuals who achieve integrity see aging as a positive experience, make adjustments in their personal space and social relationships, maintain a sense of usefulness, and begin closure and life review.
Older persons may develop their own means of coping with illness through self-care, assistance from family members, and support from social groups. Some cultures have developed attitudes and specific behaviors for older adults that may include humanistic care and identification of family members as care providers. The older adults may have special family responsibilities—for example, providing hospitality to visitors among Amish cultures and communicating to members of younger generations skills and accrued wisdom among Filipinos.
Older immigrants who have made major lifestyle adjustments in their move from their homelands to the United States or from a rural to an urban area (or vice versa) may not be aware of health care alternatives, preventive programs, health care benefits, and screening programs for which they are eligible. The people may also be in various stages of culture shock; that is, the state of disorientation or inability to respond to the behavior of a different cultural group because of its sudden strangeness, unfamiliarity, and incompatibility to the newcomer’s perceptions and expectations. For example, in order to maintain ties with their native heritage, people may seek to purchase food in stores that specialize in selling products from their homelands.
Traditional Causes of ILLNESS
Disease causation may be viewed in three major ways: from a biomedical or scientific, a naturalistic or holistic, or a magicoreligious perspective.
Biomedical
The first, called the biomedical or scientific theory of illness causation, is based on the assumption that all events in life have a cause and effect, that the human body functions more or less mechanically (i.e., the functioning of the human body is analogous to the functioning of an automobile), that all life can be reduced or divided into smaller parts (e.g., the reduction of the human person into body, mind, and spirit), and that all of reality can be observed and measured (e.g., intelligence tests and psychometric measures of behavior). Among the biomedical explanations for disease is the germ theory, which posits that microscopic organisms such as bacteria and viruses are responsible for specific disease conditions. Most educational programs for physicians, nurses, and other health care providers embrace the biomedical or scientific theories that explain the causes of both physical and psychological illnesses.
Naturalistic
The second way in which people explain the cause of illness is from the naturalistic or holistic perspective, found most frequently among American Indians, Asians, and others who believe that human life is only one aspect of nature and a part of the general order of the cosmos. The people may believe that the forces of nature must be kept in natural balance or harmony.
Some Asians believe in the yin/yang theory, in which health is believed to exist when all aspects of the person are in perfect balance. Rooted in the ancient Chinese philosophy of Tao, the yin/yang theory states that all organisms and objects in the universe consist of yin and yang energy forces. The seat of the energy forces is within the autonomic nervous system where balance between the opposing forces is maintained during health. Yin energy represents the female and negative forces, such as emptiness, darkness, and cold, whereas yang forces are male and positive, emitting warmth and fullness. Foods are classified as hot and cold in this theory and are transformed into yin and yang energy when metabolized by the body. Yin foods are cold, and yang foods are hot. Cold foods are eaten with a hot illness, and hot foods are eaten with a cold illness. The yin/yang theory is the basis for Eastern or Chinese medicine and is commonly embraced by many Asian Americans.
The naturalistic perspective posits that the laws of nature create imbalances, chaos, and disease. People embracing the naturalistic view use metaphors such as the healing power of nature, and they call the earth “Mother.” From the perspective of the Chinese, for example, illness is not seen as an intruding agent but as a part of life’s rhythmic course and as an outward sign of disharmony within.
Many Hispanic, Arab, Black, and Asian groups embrace the hot/cold theory of health and illness, an explanatory model with origins in the ancient Greek humoral theory. The four humors of the body—blood, phlegm, black bile, and yellow bile—regulate basic bodily functions and are described in terms of temperature, dryness, and moisture. The treatment of disease consists of adding or subtracting cold, heat, dryness, or wetness to restore the balance of the humors.
Beverages, foods, herbs, medicines, and diseases are classified as hot or cold according to their perceived effects on the body, not on their physical characteristics. Illnesses believed to be caused by cold entering the body include earache, chest cramps, paralysis, gastrointestinal discomfort, rheumatism, and tuberculosis. Among those illnesses believed to be caused by overheating are abscessed teeth, sore throats, rashes, and kidney disorders.
According to the hot/cold theory, the person is whole, not just a particular ailment. Those who embrace the hot/cold theory maintain that health consists of a positive state of total well-being, including physical, psychological, spiritual, and social aspects of the person. Paradoxically, the language used to describe this artificial dissection of the body into parts is itself a reflection of the biomedical/scientific perspective, not a naturalistic or holistic one.
Magicoreligious
The third major way in which people explain the causation of ILLNESS is from a magicoreligious perspective. The basic premise is that the world is seen as an arena in which supernatural forces dominate. The fate of the world and those in it depends on the action of supernatural forces for good or evil. Examples of magical causes of illness include belief in voodoo or witchcraft among some African Americans and others from circum-Caribbean countries. Faith healing is based on religious beliefs and is most prevalent among certain Christian religions, including Christian Scientists, whereas various healing rituals may be found in many other religions such as Roman Catholicism and Mormonism.
Of course, it is possible to have a combination of worldviews, and many people are likely to offer more than one explanation for the cause of their illness, the means of protecting themselves from such an illness, and the means to recovery. As a profession, nursing largely embraces the scientific/biomedical worldview, but some other aspects are gaining popularity, including techniques for management of chronic pain, such as acupuncture, herbal therapies, hypnosis, therapeutic touch, and biofeedback.
Amulets are objects, such as charms, that may be worn on a string or chain around the neck, wrist, or waist to protect the wearer from the “evil eye” or the “evil spirits” that could be transmitted from one person to another or that could have supernatural origins. They may also be hung in the home, car, or workplace. Natural folk medicine uses remedies from the natural environment—herbs, plants, minerals, and animal substances—to treat illnesses. Amulets and remedies have come to the United States from every corner of the world, the East and the West. They may be purchased in pharmacies, markets, and natural food stores. Fig. 2-5 illustrates the interior of a botanica, a store in which a person can purchase amulets and remedies used by people from many Latino heritages. Others may be objects or substances used externally. Fig. 2-6 presents samples of traditional amulets.

2-5 The interior of a botanica.20

2-6 A, The glass blue eye from Turkey, seen here, is an example of an amulet that may be hung in the home.20 B, A seed with a red string may be placed on the crib of a baby of Mexican heritage.20 C, These bangles may be worn for protection by a person of Caribbean heritage.20 D, This small packet is placed on a crib or baby’s room of a baby of Japanese heritage.20
Healing and Culture
When self-treatment is unsuccessful, the person might turn to the lay or folk healing systems, to spiritual or religious healing, or to scientific biomedicine. All cultures have their own preferred lay or popular healers, recognized symptoms of ill health, acceptable sick role behavior, and treatments. In addition to seeking help from you as a biomedical/scientific health care provider, patients may also seek help from folk or religious healers. Some people, such as those of Hispanic or American Indian origins, may believe that the cure is incomplete unless healing of body, mind, and spirit are all carried out. The division of the person into parts is itself a Western concept. For example, a Hispanic person with a respiratory infection may take the antibiotics prescribed by a physician or nurse practitioner and herbal teas recommended by a curandero and may say prayers for healing suggested by a Catholic priest. Many people from different faith traditions practice prayer or visit healing shrines, as discussed earlier in this chapter. There are countless shrines in the United States and the rest of the world where people make pilgrimages for this purpose, including Chimayo in New Mexico, Fatima in Portugal, and Lourdes in France.
The variety of healing beliefs and practices used by the many ethnocultural populations found in this country far exceeds the limitations of this chapter. It is important, however, that you be aware of the existence of traditional practices and recognize that, in addition to folk practices, many other complementary healing practices exist. Although it is dangerous to assume that all indigenous approaches to healing are innocuous, the majority of practices are quite harmless, regardless of whether they are effective cures. Fig. 2-7 presents samples of traditional remedies used for recovery.
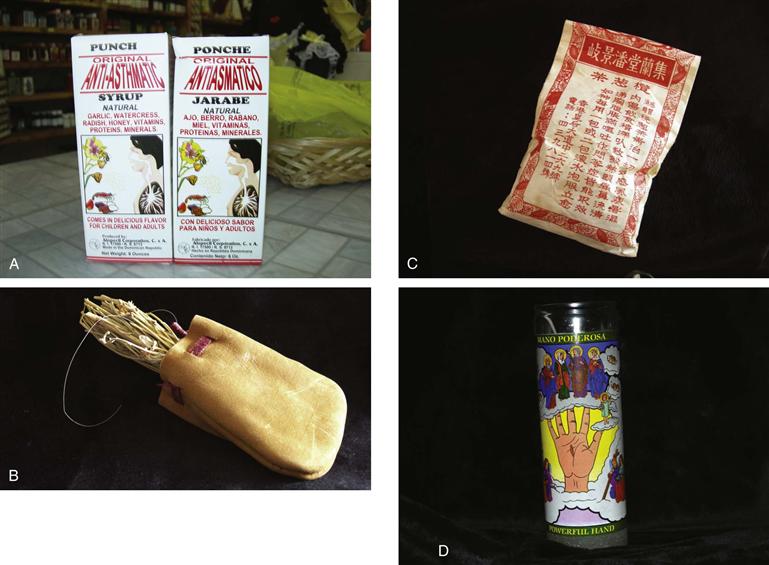
2-7 A, This “tonic” sold in a botanica is used to treat asthma.20 B, The traditional medicine bag of an American Indian shaman is used to carry necessary medicines.20 C, The leaves in this package may be used by a person of Chinese heritage to treat indigestion.20 D, This candle may be burned for cleansing by a person of Mexican heritage.20
Table 2-2 lists questions to ask and sample answers for this phase of assessment.
Folk Healers
People from most traditional heritages tend to use traditional healers from their own background. Although numerous folk healers exist, you may find Hispanics turning to a curandero(ra), espiritualista (spiritualist), yerbo(ba) (herbalist), partera (lay midwife), or sabedor (healer who manipulates bones and muscles). African Americans may mention having received assistance from a hougan (a voodoo priest or priestess), spiritualist, or “old lady” (an older woman who has successfully raised a family and who specializes in childcare and folk remedies). American Indians may seek assistance from a shaman or medicine (wo)man. Asians may mention that they have visited herbalists, acupuncturists, or bone setters. Among the Amish, the term braucher refers to folk healers who use herbs and tonics in the home or community context. Brauche, a folk healing art, refers to sympathy curing, which is sometimes called powwowing in English.
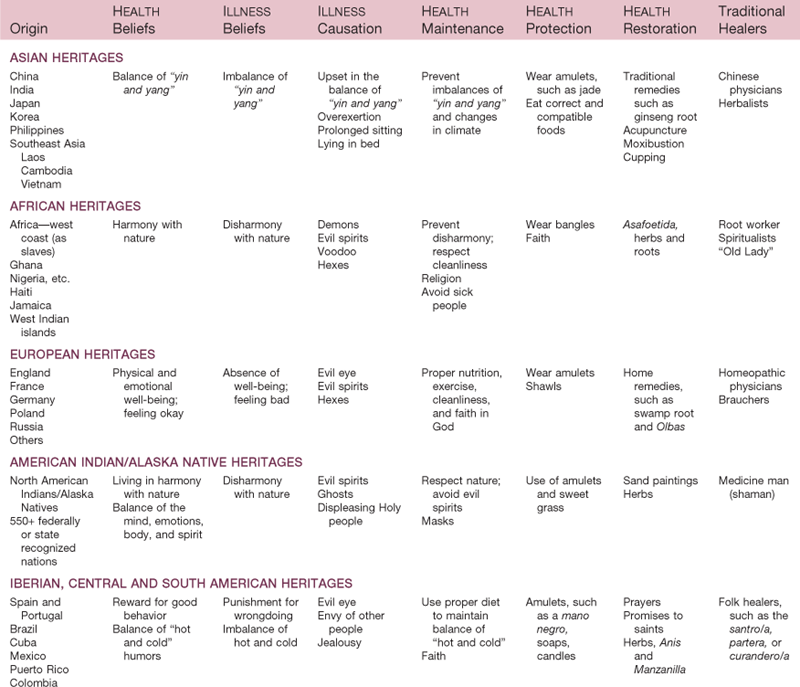
The treatments used by a traditional healer may be provided in conjunction with massage; foot treatments; acupressure; reflexology; or, less frequently, iridology.20 Each culture has its own healers, most of whom speak the person’s native tongue, make house calls, understand the person’s cultural HEALTH beliefs, and cost significantly less than healers practicing in the biomedical/scientific health care system. Table 2-3 lists examples of traditional HEALTH and ILLNESS beliefs and practices, causes of illness, and examples of traditional healers.
In some religions, spiritual healers may be found among the ranks of the ordained and official religious hierarchy and may be known by a variety of names such as priest, bishop, elder, deacon, rabbi, brother, and sister. In other religions, a separate category of healer may be found—e.g., Christian Science “nurses” (not licensed by states) or practitioners. Spirituality is included in the perceptions of health and illness.
Transcultural Expression of Illness
Transcultural Expression of Pain
To illustrate the manner in which symptom expression may reflect the person’s cultural background, let us use an extensively studied symptom—pain. Pain is a universally recognized phenomenon, and it is an important aspect of assessment for people of various ages. Pain is a very private, subjective experience that is greatly influenced by cultural heritage. Expectations, manifestations, and management of pain are all embedded in a cultural context. The definition of pain, like that of health or illness, is culturally determined.
The word pain is derived from the Greek word for penalty, which helps explain the long association between pain and punishment in Judeo-Christian thought. The meaning of painful stimuli, the way people define their situation, and the impact of personal experience all help determine the experience of pain.
Much cross-cultural research has been conducted on pain. Pain has been found to be a highly personal experience, depending on cultural learning, the meaning of the situation, and other factors unique to the person. Silent suffering has been identified as the most valued response to pain by health care professionals. The majority of nurses have been socialized to believe that in virtually any situation, self-control is better than open displays of strong feelings.
In addition to expecting variations in pain perception and tolerance, you also should expect variations in the expression of pain. It is well known that people turn to their social environment for validation and comparison. A first important comparison group is the family, which transmits cultural norms to its children.
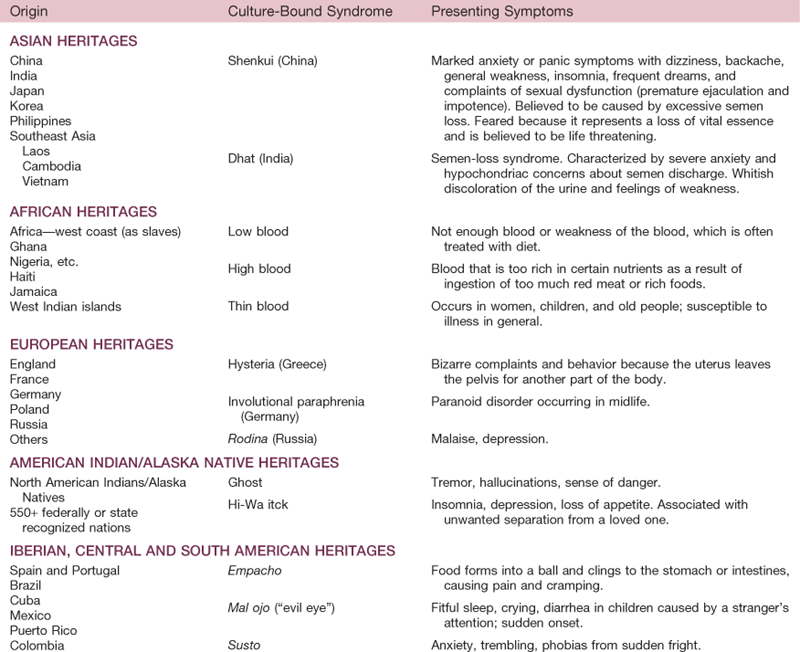
Culture-Bound Syndromes
Some people may have a condition that is culturally defined, known as a culture-bound syndrome. Some of these conditions have no equivalent from a biomedical/scientific perspective, whereas others, such as anorexia nervosa and bulimia, are examples of the cultural aspects of illness among members of a dominant cultural population in North America. Table 2-4 summarizes selected examples from among the more than 150 culture-bound syndromes that have been documented by medical anthropologists, mental health providers, or community spokespeople.
Culture and Treatment
After a symptom is identified, the first effort at treatment is often self-care. In the United States, an estimated 38% of adults use some form of complementary therapy to treat an illness. Furthermore, U.S. adults spent $33.9 billion out-of-pocket on visits to complementary and alternative medicine practitioners and the purchase of related products.13a The availability of over-the-counter medications, the relatively high literacy level of Americans, the growing availability of herbal remedies, and the influence of the Internet and mass media in communicating health-related information to the general population have contributed to the high percentage of cases of self-treatment. Home treatments are attractive for their accessibility, especially compared with the inconvenience associated with traveling to a physician, nurse practitioner, or pharmacist, particularly for people from rural or sparsely populated areas. Furthermore, home treatment may mobilize the person’s social support network and provide the sick person with a caring environment in which to convalesce. You should be aware, however, that not all home remedies are inexpensive. For example, urban Black populations in the Southeast sometimes use medicinal potions that cost much more than the equivalent treatment with a biomedical intervention.
A wide variety of alternative, complementary, or traditional interventions are gaining the recognition of health care professionals in the biomedical/scientific health care system. Acupuncture, acupressure, therapeutic touch, massage, therapeutic use of music, biofeedback, relaxation techniques, meditation, hypnosis, distraction, imagery, iridology, reflexology, herbal remedies, and others are interventions that people may use either alone or in combination with other treatments. Many pharmacies and grocery stores routinely carry herbal treatments for a wide variety of common illnesses. The efficacy of complementary and alternative interventions for specific health problems has been studied extensively (see National Center for Complementary and Alternative Medicine at www.nccam.nih.gov). The frequency of use of traditional remedies, such as herbs purchased in botanicas and Chinese herbal drugs, is unknown at this time. However, personal observations in these settings indicate great popularity within the traditional members of the ethnocultural community. Fig. 2-7 illustrates examples of the remedies.
Culture and Disease Prevalence
For the past generation, the United States and Canada have enjoyed improvement in the health status of the population. Despite this fact, there continues to be disparities in deaths and illnesses experienced by racial and ethnic emerging majority populations, and it is well known that diseases are not distributed equally among all segments of the population. Abnormal biocultural variations may be genetic or acquired. Information about disease prevalence for various racial and ethnic groups is useful because you are able to focus your assessment according to the increased statistical probability that a particular condition may occur. For example, if you are examining an African-American child with gastrointestinal symptoms, you may focus more on the possibility of lactose intolerance or sickle-cell anemia while considering cystic fibrosis, known primarily among white children, a much less likely source of the problem. Poverty also plays a role in the disparities. Thus, in your assessment, you will want to be certain that you have gathered the appropriate data needed to support or to refute your suspicions. Information regarding several health disparities is included in the CULTURE AND GENETICS section of chapters in this text.
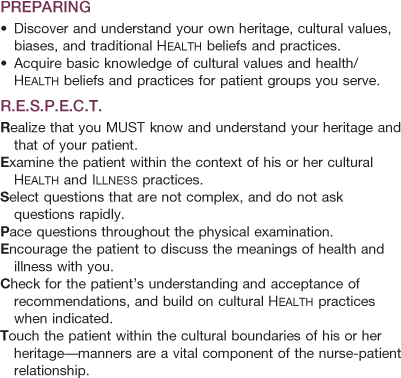
Steps to CULTURAL COMPETENCY
There are several steps that you must climb on the journey to CULTURAL COMPETENCY. The integration of this knowledge into day-to-day practice will take time because many practitioners in the health care system are hesitant to adopt new ideas. CULTURAL COMPETENCY does not come instantly, certainly not after reading a chapter or several chapters or books on this highly specialized area. It is complex and multifaceted, and many facets change over time. The areas of knowledge include sociology, psychology, theology, cultural anthropology, demography, folklore, and immigration history and policies. One must also have an understanding of poverty and environmental health. CULTURAL COMPETENCY also involves soul searching about your own heritage and HEALTH.
The first step in understanding the HEALTH care needs of others is to understand your own heritage based on cultural values, beliefs, attitudes, and practices that are relevant to HEALTH and ILLNESS (Table 2-5). Sometimes this requires considerable searching and necessitates that you explore your family’s heritage and traditional beliefs and practices. Your mother or maternal grandmother is a familial resource whom you may want to interview to determine the meaning of these terms within your family. The reason for suggesting that you interview your maternal side is that, in the past, mothers tended to be the family gatekeepers and the persons who determined whether you were healthy or sick.
You are now learning the modern, scientific meanings of health and illness, and at the same time, you must develop a frame of reference as to the traditional beliefs and practices relevant to these concepts. In addition, many of your patients will come from socioeconomic and religious backgrounds different from your own, so you must confront your own biases, preconceptions, and prejudices about specific racial, ethnic, religious, sexual, or socioeconomic groups.
The second phase is to identify the meaning of HEALTH to the other person, remembering that concepts are derived, in part, from the way in which members of a cultural group define health. Considerable research has been conducted on the various definitions of HEALTH that may be held by various groups. For example, one traditional American Indian belief is that HEALTH reflects living in total harmony with nature; illness is the result of a lack of prevention. Some Jamaicans may define health as having a good appetite, feeling strong and energetic, performing activities of daily living without difficulty, and being sexually active and fertile. For Italian women, health may mean the ability to interact socially and to perform routine tasks such as cooking, cleaning, and caring for self and others. On the other hand, some people of Mexican heritage believe that coughing, sweating, and diarrhea are a normal part of living, not symptoms of ill health—perhaps because of the high frequency of these conditions in the country of origin. Thus individuals may define themselves or others in their group as healthy even though you identify them as having symptoms of disease.
Third, you must understand the health care delivery system, how it works, what it does, the meanings of various procedures, and the costs and consequences to the patients and to you as a nurse. Fourth, you must be knowledgeable about the social backgrounds of your patients—the meanings of immigration, racism, socioeconomic status, welfare reform, and aging. Fifth, you must be familiar with the language people speak, the resources available to help with interpretation, and the resources within the community.
The bibliography lists several books and selected websites that can provide you with introductory material related to this content. Remember, everything is connected to CULTURAL COMPETENCY: heritage, culture, ethnicity, religion, socialization, population diversity, immigration, religion, demographic change, globalization, health and illness, modern and traditional beliefs and practices, sociopolitical issues, sanitation, housing, and infrastructure. CULTURAL CARE is the goal to strive for. As stated in the beginning of the chapter, it is a long journey.
Bibliography
1. Abramson HJ. Religion. In: Thernstrom S, ed. Harvard encyclopedia of American ethnic groups. Cambridge: Harvard University Press; 1980.
1a. American Religious Identification Survey 2001. http://www.gc.cuny.edu/faculty/research_studies/aris.pdf; 2001; The City University of New York. Accessed June 9, 2009, from.
2. Andrews MM, Boyle JS. Transcultural concepts in nursing care. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2003.
3. Bernstein R. U S Hispanic population surpasses 45 million: now is 15 percent of total. Public Information Office. Accessed June 9, 2009, from www.census.gov/PressRelease/www/releases/archives/population/011910.html.
4. Estes, G., & Zitzow, D. (1980). Heritage consistency as a consideration in counseling Native Americans. Presented at the National Indian Education Association Convention, Dallas: The Association.
5. Fix ME, Passel JS. U.S. immigration at the beginning of the 21st century: Testimony before the Subcommittee on Immigration and Claims Hearing on “The U.S Population and Immigration”. Committee on the Judiciary U.S. House of Representatives Accessed August 2, 2001, from www.urban.org/url.cfm?ID=900417; 2001.
6. Flores G. Language barriers to health care in the United States. New England Journal of Medicine. 2006;355:229–231.
7. Giger JN, Davidhizar RE. Transcultural nursing: assessment and intervention. 5th ed. St. Louis: Mosby; 2008.
8. Giger J, Davidhizar R, Purnell L, et al. American Academy of Nursing Expert Panel Report: Developing cultural competence to eliminate health disparities in ethnic minorities and other vulnerable populations. Journal of Transcultural Nursing. 2007;18(2):95–102.
9. Hoefer M, Rytina N, Baker BB. Estimates of the unauthorized immigrant population residing in the United States: January, 2008. Accessed June 8, 2009, from www.dhs.gov/xlibrary/assets/statistics/publications/ois_ill_pe_2008.pdf; 2008.
10. Homeland Security. Definition of terms, 2008. Accessed June 5, 2009, from www.dhs.gov/ximgtn/statistics/stdfdef.shtm#11; 2008.
11. LaFrombose T, Coleman LK, Gerton J. Psychological impact of biculturalism: Evidence and theory. Psychological Bulletin. 1993;114:395.
12. Levin J. God, faith and health: Exploring the spirituality-healing connection. New York: John Wiley & Sons; 2001.
13. Ludwig-Beymer PA. Transcultural aspects of pain. In: Andrews MM, Boyle JS, eds. Transcultural concepts in nursing care. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2002.
13a. Nahin RL, Barnes PM, Stussman BJ, et al. Costs of complementary and alternative medicine (CAM) and frequency of visits to CAM practitioners: United States, 2007. National health statistics reports; no 18 Hyattsville, MD: National Center for Health Statistics; 2009.
14. National standards for culturally and linguistically appropriate services in health care, final report, March 2001, Washington, DC, Office of Minority Health, Department of Health and Human Services.
15. Novak M. The rise of the unmeltable ethnics. New York: Macmillan; 1972.
16. Pew Forum on Religion and Public Life. U S Religious Landscape Survey, 2007. Accessed June 9, 2009, from http://religions.pewforum.org/pdf/report2religious-landscape-study-key-findings.pdf.
17. Randall M, Rytina N. U.S legal permanent residents, 2008. Accessed June 7, 2009, from www.dhs.gov/xlibrary/assets/statistics/publications/lpr_fr_2008.pdf.
18. Skalla KA, McCoy JP. Spiritual assessment of patients with cancer: The mortal authority, vocational, aesthetic, social, and transcendent model. Oncology Nursing Forum. 2006;33:752.
19. Spector RE. Culture care: Guide to heritage assessment and health traditions. 3rd ed. Upper Saddle River, NJ: Prentice Hall; 2004.
20. Spector RE. Cultural diversity in health and illness. 7th ed. Upper Saddle River, NJ: Prentice Hall; 2009.
21. U.S. Census Bureau, Public Information Office. U.S Census 2008 Population and housing narrative profile: 2005-2007. Accessed June 8, 2009, from (301) 763-3030 http://factfinder.census.gov/servlet/NPTable?_bm=y&-qr_name=ACS_2007_3YR_G00_NP01&-geo_id=01000US&-ds_name=ACS_2007_3YR_G00_&-_lang=en.
22. U.S. Census Bureau. Home page. Accessed June 3, 2009, from www.census.gov/.
23. Wenger AF. Cultural meaning of symptoms. Holistic Nursing Practice. 1993;7:22–35.
24. Wenger AF. Cultural context, health, and health care decision making. Journal of Transcultural Nursing. 1995;7:3–14.
Websites of Interest
1. www.census.gov/; —A complete demographic profile at national, state, and local levels.
2. www.tcns.org/; —The Transcultural Nursing Society.
3. www.healthpowerforminorities.org/resources/national.cfm; —A directory and links to resources for minority health programs.
4. www.hhs-stat.net/omh/index.htm; —Links to programs developed to reduce health disparities.
5. www.hhs.gov/ocr/hospitalcommunication.html; —Information regarding Title VI of the Civil Rights Act.
6. www.thinkculturalhealth.org/ccnm/; —Self-study program in cultural competency.
7. www.omhrc.gov/; —The division in the government that is developing standards and educational programs in cultural competency.
8. www.census.gov/hhes/www/poverty/poverty.html; —Facts and figures regarding economic poverty.
9. In: http://nccam.nih.gov/news/camstats/costs/.
10. www.kaiseredu.org/topics_index.asp; —An online health policy resource that includes the following topics: Health and the Law, Health System, HIV/AIDS, Medicare, Minority Health, Uninsured, and Women’s Health.
11. www.cdc.gov/nchs/data/hus/hus08.pdf; —This publication, Health United States: 2008, is the 32nd report on the health status of the Nation. The report is published annually and is an invaluable resource for health statistics in four major areas—health status and determinants, health care utilization, health care resources, and health care expenditures.
*HEALTH: “The balance of the person, both within one’s being—physical, mental, and/or spiritual—and in the outside world—natural, communal, and/or metaphysical, is a complex, interrelated phenomenon.”20
*ILLNESS: “The loss of the person’s balance, both within one’s being—physical, mental, and/or spiritual—and in the outside world—natural, communal, and/or metaphysical.”20