Ears
Outline

http://evolve.elsevier.com/Jarvis/
• Bedside Assessment Summary Checklist
• Physical Examination Summary Checklist
Structure and Function
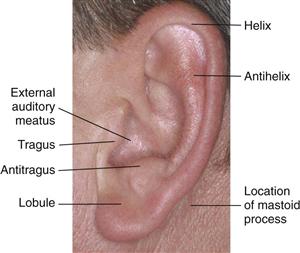
The ear is the sensory organ for hearing and maintaining equilibrium. The ear has three parts: the external ear, the middle ear, and the inner ear. The external ear is called the auricle or pinna and consists of movable cartilage and skin (Fig. 15-1). Note the landmarks of the auricle, and use these terms to describe your findings. The mastoid process, the bony prominence behind the lobule, is not part of the ear but is an important landmark.
15-1
External Ear
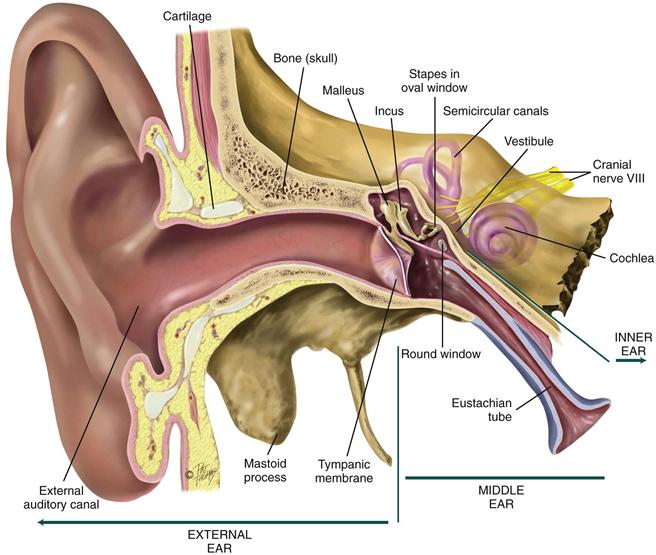
The external ear has a characteristic shape and serves to funnel sound waves into its opening, the external auditory canal (Fig. 15-2). The canal is a cul-de-sac 2.5 to 3 cm long in the adult and terminates at the eardrum, or tympanic membrane. The canal is lined with glands that secrete cerumen, a yellow, waxy material that lubricates and protects the ear. The wax forms a sticky barrier that helps keep foreign bodies from entering and reaching the sensitive tympanic membrane. Cerumen migrates out to the meatus by the movements of chewing and talking.
15-2 Copyright © (2006) © Pat Thomas, 2010.
The outer one third of the canal is cartilage; the inner two thirds consists of bone covered by thin, sensitive skin. The canal has a slight S-curve in the adult. The outer one third curves up and toward the back of the head, whereas the inner two thirds angles down and forward toward the nose.
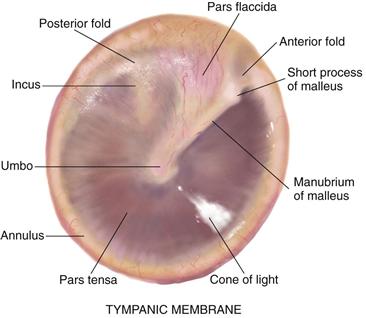
The tympanic membrane (TM), or eardrum, separates the external and the middle ear and is tilted obliquely to the ear canal, facing downward and somewhat forward. It is a translucent membrane with a pearly gray color and a prominent cone of light in the anteroinferior quadrant, which is the reflection of the otoscope light (Fig. 15-3). The drum is oval and slightly concave, pulled in at its center by one of the middle ear ossicles, the malleus. The parts of the malleus show through the translucent drum; these are the umbo, the manubrium (handle), and the short process. The small, slack, superior section of the tympanic membrane is called the pars flaccida. The remainder of the drum, which is thicker and more taut, is the pars tensa. The annulus is the outer fibrous rim of the drum.
15-3
Lymphatic drainage of the external ear flows to the parotid, mastoid, and superficial cervical nodes.
Middle Ear
The middle ear is a tiny air-filled cavity inside the temporal bone (see Fig. 15-2). It contains tiny ear bones, or auditory ossicles: the malleus, incus, and stapes. The middle ear has several openings. Its opening to the outer ear is covered by the tympanic membrane. The openings to the inner ear are the oval window at the end of the stapes and the round window. Another opening is the eustachian tube, which connects the middle ear with the nasopharynx and allows passage of air. The tube is normally closed, but it opens with swallowing or yawning.
The middle ear has three functions: (1) it conducts sound vibrations from the outer ear to the central hearing apparatus in the inner ear; (2) it protects the inner ear by reducing the amplitude of loud sounds; and (3) its eustachian tube allows equalization of air pressure on each side of the tympanic membrane so that the membrane does not rupture (e.g., during altitude changes in an airplane).
Inner Ear
The inner ear is embedded in bone. It contains the bony labyrinth, which holds the sensory organs for equilibrium and hearing. Within the bony labyrinth, the vestibule and the semicircular canals compose the vestibular apparatus and the cochlea (Latin for “snail shell”) contains the central hearing apparatus. Although the inner ear is not accessible to direct examination, you can assess its functions.
Hearing
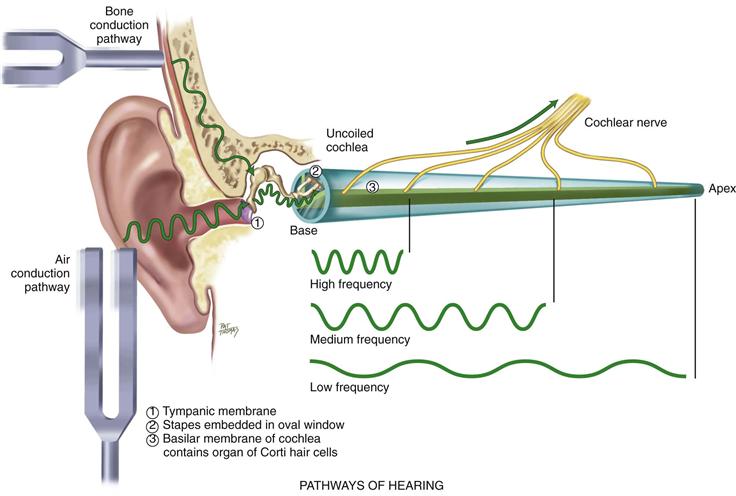
The function of hearing involves the auditory system at three levels: peripheral, brainstem, and cerebral cortex. At the peripheral level, the ear transmits sound and converts its vibrations into electrical impulses, which can be analyzed by the brain. For example, you hear an alarm bell ringing in the hall. Its sound waves travel instantly to your ears. The amplitude is how loud the alarm is; its frequency is the pitch (in this case, high) or the number of cycles per second. The sound waves produce vibrations on your tympanic membrane. These vibrations are carried by the middle ear ossicles to your oval window. Then the sound waves travel through your cochlea, which is coiled like a snail’s shell, and are dissipated against the round window. Along the way, the basilar membrane vibrates at a point specific to the frequency of the sound. In this case, the alarm’s high frequency stimulates the basilar membrane at its base near the stapes (Fig. 15-4). The numerous fibers along the basilar membrane are the receptor hair cells of the organ of Corti, the sensory organ of hearing. As the hair cells bend, they mediate the vibrations into electric impulses. The electrical impulses are conducted by the auditory portion of cranial nerve VIII to the brainstem.
15-4 Copyright © (2006) © PAT THOMAS, 2006.
The function at the brainstem level is binaural interaction, which permits locating the direction of a sound in space as well as identifying the sound. How does this work? Each ear is actually one half of the total sensory organ. The ears are located on each side of a movable head. The cranial nerve VIII from each ear sends signals to both sides of the brainstem. Areas in the brainstem are sensitive to differences in intensity and timing of the messages from the two ears, depending on the way the head is turned.
Finally, the function of the cortex is to interpret the meaning of the sound and begin the appropriate response. All this happens in the split second it takes you to react to the alarm.
Pathways of Hearing
The normal pathway of hearing is air conduction (AC), described earlier; it is the most efficient. An alternate route of hearing is by bone conduction (BC). Here, the bones of the skull vibrate. These vibrations are transmitted directly to the inner ear and to cranial nerve VIII.
Hearing Loss
Anything that obstructs the transmission of sound impairs hearing. A conductive hearing loss involves a mechanical dysfunction of the external or middle ear. It is a partial loss because the person is able to hear if the sound amplitude is increased enough to reach normal nerve elements in the inner ear. Conductive hearing loss may be caused by impacted cerumen, foreign bodies, a perforated tympanic membrane, pus or serum in the middle ear, and otosclerosis (a decrease in mobility of the ossicles).
Sensorineural (or perceptive) loss signifies pathology of the inner ear, cranial nerve VIII, or the auditory areas of the cerebral cortex. A simple increase in amplitude may not enable the person to understand words. Sensorineural hearing loss may be caused by presbycusis, a gradual nerve degeneration that occurs with aging, and by ototoxic drugs, which affect the hair cells in the cochlea. A mixed loss is a combination of conductive and sensorineural types in the same ear.
Equilibrium
The labyrinth in the inner ear constantly feeds information to your brain about your body’s position in space. It works like a plumb line to determine verticality or depth. The ear’s plumb lines register the angle of your head in relation to gravity. If the labyrinth ever becomes inflamed, it feeds the wrong information to the brain, creating a staggering gait and a strong, spinning, whirling sensation called vertigo.
 Developmental Competence
Developmental Competence
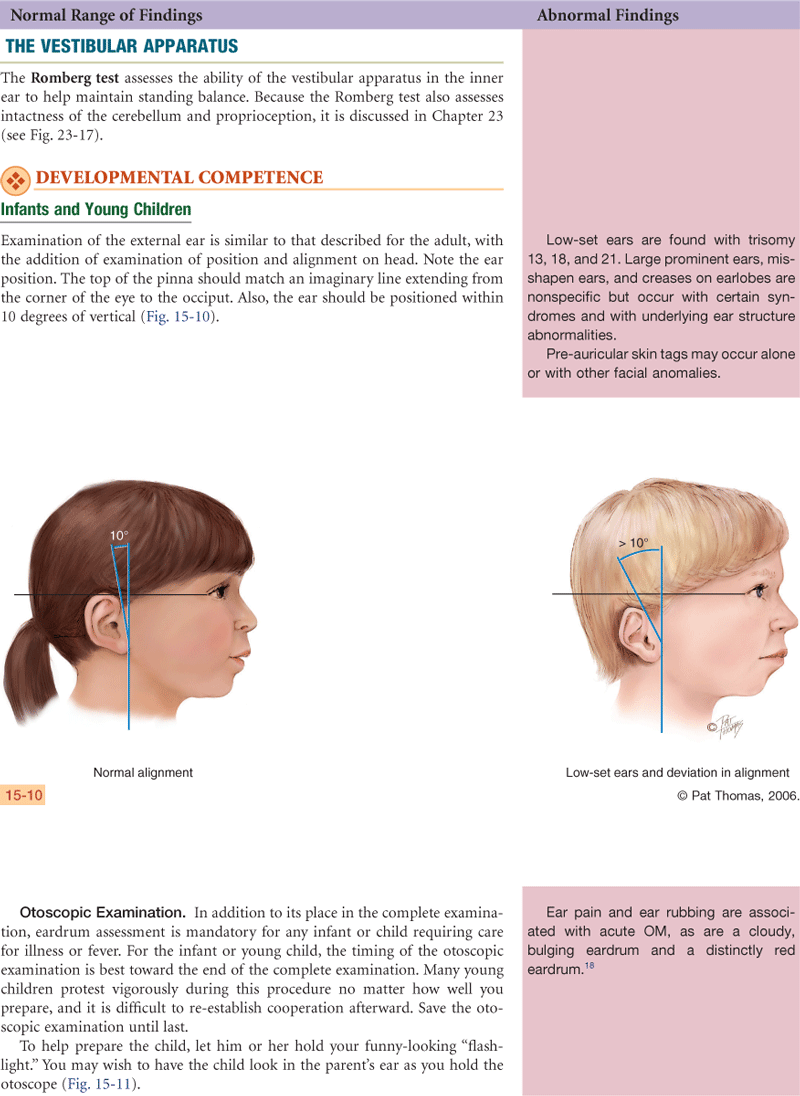
Infants and Children
The inner ear starts to develop early in the fifth week of gestation. In early development, the ear is posteriorly rotated and low set; later it ascends to its normal placement around eye level. If maternal rubella infection occurs during the first trimester, it can damage the organ of Corti and impair hearing.
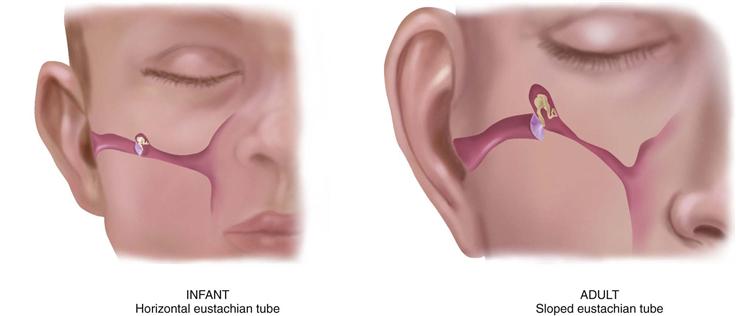
The infant’s eustachian tube is relatively shorter and wider and its position is more horizontal than the adult’s, so it is easier for pathogens from the nasopharynx to migrate through to the middle ear (Fig. 15-5). The lumen is surrounded by lymphoid tissue, which increases during childhood; thus the lumen is easily occluded. These factors place the infant at greater risk for middle ear infections than the adult.
15-5
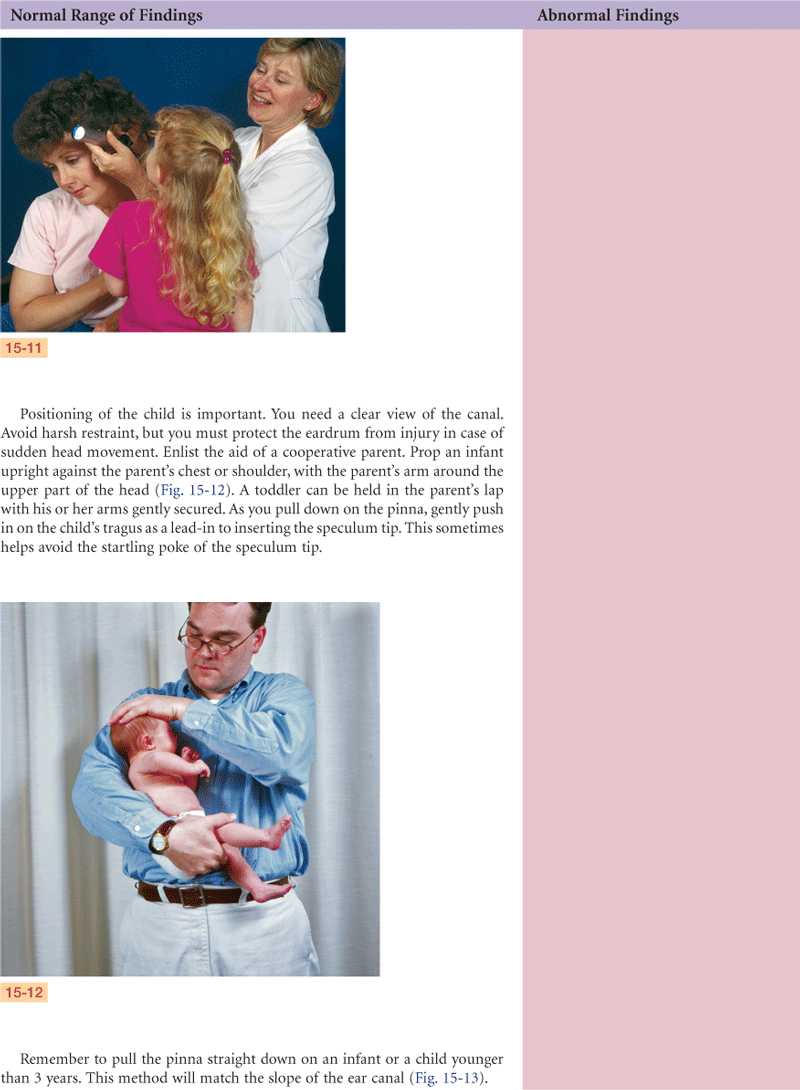
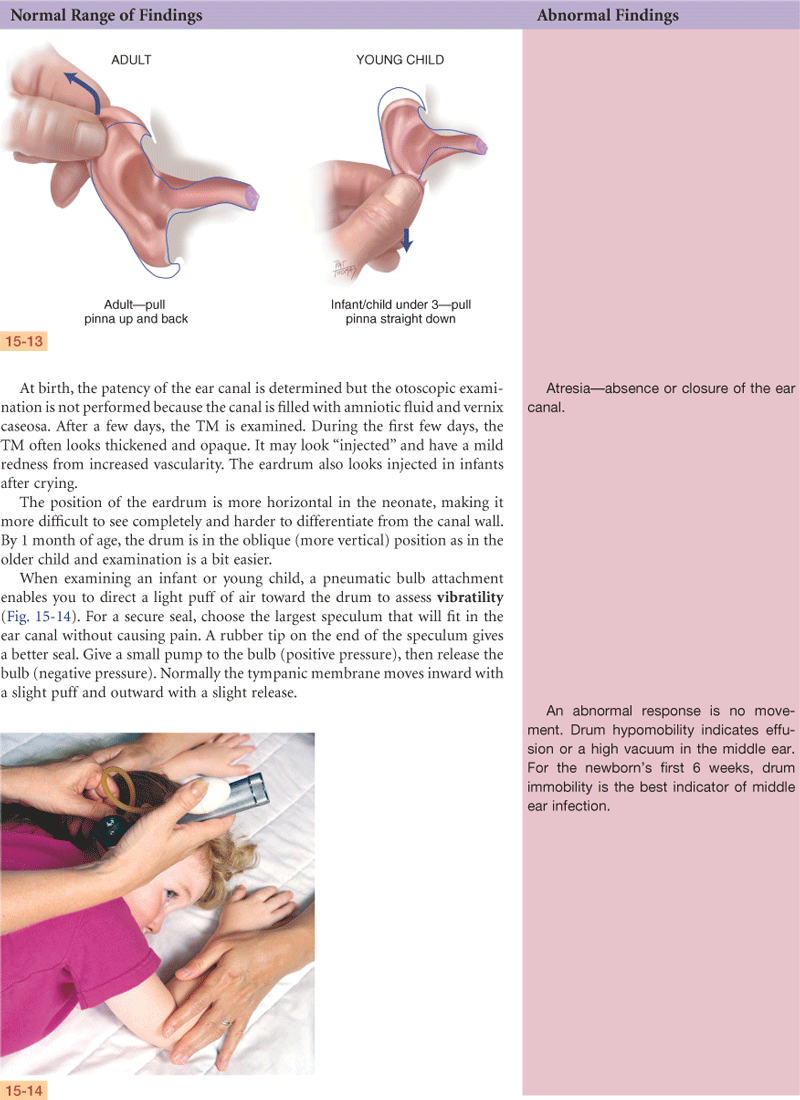
The infant’s and the young child’s ear canal is shorter and has a slope opposite to that of the adult’s (see Fig. 15-13 on p. 336).
The Adult
Otosclerosis is a common cause of conductive hearing loss in young adults between the ages of 20 and 40 years. It is a gradual hardening that causes the footplate of the stapes to become fixed in the oval window, impeding the transmission of sound and causing progressive deafness.
The Aging Adult
In the aging person, cilia lining the ear canal become coarse and stiff. This may cause cerumen to accumulate and oxidize, which greatly reduces hearing. The cerumen itself is drier because of atrophy of the apocrine glands. Also, a life history of frequent ear infections may result in scarring on the drum.
Impacted cerumen is common in aging adults (up to 57%) and in other at-risk groups (e.g., institutionalized and mentally disabled) who may underreport the associated hearing loss. Cerumen impaction also blocks conduction in those wearing hearing aids and accounts for 70% of the malfunction in hearing aids returned to the manufacturer.12 Cerumen should be removed when it leads to conductive hearing loss or interferes with full assessment of the ear. Ceruminolytics are wax-softening agents that expedite removal with electric or manual irrigators. After removal, those persons with hearing loss have shown improvement by 5 to 36 dB.12
A person living in a noise-polluted area (e.g., near an airport or a busy highway) has a greater risk for hearing loss. But presbycusis is a type of hearing loss that occurs with 60% of those older than 65 years, even in people living in a quiet environment. It is a gradual sensorineural loss caused by nerve degeneration in the inner ear that slowly progresses after the fifth decade.13 The person first notices a high-frequency tone loss; it is harder to hear consonants than vowels. Much speech information is lost, and words sound garbled. The ability to localize sound is impaired also. This communication dysfunction is accentuated when unfavorable background noise is present (e.g., with music, with dishes clattering, or at a large, noisy party).
 Culture and Genetics
Culture and Genetics
Otitis media, or OM (middle ear infection), occurs because of obstruction of the eustachian tube or passage of nasopharyngeal secretions into the middle ear. Otitis media is one of the most common illnesses in children. It is so common that 90% of all children younger than 2 years have had at least one episode of OM.17 The incidence and severity are increased in indigenous children from North America, Australia, New Zealand, and Northern Europe, although genetic factors have not been determined. Rather, the most important cause is environmental; children in high-risk groups usually have multiple pathogens, and the total bacterial load is high.16
Predisposing factors for OM include absence of breastfeeding in the first 3 months of age, exposure to tobacco smoke, daycare attendance, male gender, pacifier use, seasonality (fall and winter), and underlying diseases.17 Feeding by bottle in the supine position increases risk because the effects of gravity and sucking draw the nasopharyngeal contents directly into the middle ear. Urge parents to breastfeed whenever possible. But when bottle-feeding, do not prop the bottle or let the baby take a bottle to bed.
The most important side effect of acute otitis media is the persistence of fluid in the middle ear after treatment. This middle ear effusion can impair hearing, placing the child at risk for delayed cognitive development.
Genetic variations. Cerumen is genetically determined to be of two major types: (1) dry cerumen, which is gray and flaky and frequently forms a thin mass in the ear canal; and (2) wet cerumen, which is honey brown to dark brown and moist. Chromosome 16 holds one gene trait determining the wet or dry phenotype.19 The wet cerumen phenotype occurs more often in Caucasians and African Americans, whereas the dry cerumen is more frequent in Asians and American Indians.11 The presence and composition of cerumen are not related to poor hygiene. Take caution to avoid mistaking the flaky, dry cerumen for eczematous lesions.
Objective Data
| Preparation | Equipment needed |
| Position the adult sitting up straight with his or her head at your eye level. Occasionally the ear canal is partially filled with cerumen, which obstructs your view of the TM. If the eardrum is intact and no current infection is present, a preferred method of cleaning the adult canal is to soften the cerumen with a warmed solution of mineral oil and hydrogen peroxide. Then the canal is irrigated with warm water (body temperature) with a bulb syringe or a low-pulsatile dental irrigator (WaterPik). Direct fluid to the posterior wall. Leave space around the irrigator tip for water to escape. Do not irrigate if the history or the examination suggests perforation or infection. | Otoscope with bright light (fresh batteries give off white—not yellow—light). Pneumatic bulb attachment, sometimes used with infant or young child. |
 Documentation and Critical Thinking
Documentation and Critical Thinking
Sample Charting
Subjective
States hearing is good, no earaches, infections, discharge, hearing loss, tinnitus, or vertigo.
Objective
Pinna: Skin intact with no masses, lesions, tenderness, or discharge.
Otoscope: External canals are clear with no redness, swelling, lesions, foreign body, or discharge. Both tympanic membranes are pearly gray in color, with light reflex and landmarks intact, no perforations.
Hearing: Responds appropriately to conversation. Whispered words heard bilaterally.
Focused Assessment: Clinical Case Study 1
Jamal K. is a 9-month-old Black infant who is brought to the clinic by his mother because he “feels hot and was up crying all night.”
History: Jamal is the third child of Mr. and Mrs. K. Mrs. K. received regular prenatal care. Jamal was born at 37 weeks’ gestation; labor and delivery were uncomplicated. Jamal weighed 3200 g at birth and was discharged 2 days after delivery. Jamal has been bottle-fed, with solids introduced at 5 months. Well-baby care has been regular; immunizations are up to date. Jamal has had two prior episodes of otitis media, no other illnesses.
Social History: Jamal lives with his family in a two-bedroom apartment over their grocery store and shares a bedroom with a 4-year-old brother and a 2-year-old brother. Mr. K. works full time in their grocery store; Mrs. K. provides childcare in her own home for her children and for her sister’s two young children. Both parents smoke cigarettes, 1 to 2 packs per day.
Subjective
1 day PTA—Mrs. K. put Jamal down for nap with a bottle of juice, as is usual for her. Jamal woke up in the middle of the nap crying furiously. Quieted somewhat when held upright but still fussy. Took juice from bottle, refused solid baby food. Temperature 38° C rectally. Crying and fussy all night. Mrs. K. has given no medications to Jamal.
Objective
Vital signs: Temp 38.4° C (tympanic), pulse 152, resp 36, Wt. 9.2 kg (50th percentile), Ht. 29 in. (75th percentile).
General: Alert, active, crying, and fussy. Developmentally appropriate for age.
Skin: Warm and dry, no rashes or lesions.
Head: Anterior fontanel flat, 1 × 1.5 cm; posterior fontanel closed.
Eyes: No exudate, conjunctivae clear, sclerae white, red reflex present bilaterally.
Ears: Both tympanic membranes dull red and bulging, no light reflex, no mobility on pneumatic otoscopy.
Mouth/throat: Oral mucosa pink, no lesions or exudate, tonsils 1+.
Neck: Supple, no lymphadenopathy.
Heart: Regular rate and rhythm, no murmurs.
Lungs: Breath sounds clear and equal bilaterally, unlabored.
Abdomen: Bowel sounds present, abdomen soft, nontender.
Assessment
Acute otitis media, both ears
Pain R/T inflammation in TMs
Risk for ear infection injury R/T supine bottle-feeding, group childcare, secondhand smoke
Deficient knowledge (parents) R/T risk factors for otitis media
Focused Assessment: Clinical Case Study 2
Todd R. is a 15-year-old high school student who comes to the health center to seek care for “cough off and on all winter and earache since last night.”
Subjective
6 weeks PTA—nonproductive cough throughout day, no fever, no nasal congestion, no chest soreness. Todd’s father gave him an over-the-counter decongestant, which helped, but cough continued off/on since. Does not smoke.
1 day PTA—intermittent cough continues, nasal congestion and thick white mucus. Also earache R ear, treated self with heating pad, pain unrelieved. Pain is moderate, not deep and throbbing. Says R ear feels full, “hollow headed,” voices sound muffled and far away, switches telephone to L ear to talk. No sore throat, no fever, no chest congestion or soreness.
Objective
Vital signs: T 37° C oral, P 76, BP 106/72.
Ears: L ear, canal, TM normal. R ear and canal normal, R TM retracted, with multiple air bubbles, drum color is yellow/amber. No sinus tenderness.
Nose: Turbinates bright red and swollen, mucopurulent discharge.
Throat: Not reddened, tonsils 1+.
Neck: One R anterior cervical node enlarged, firm, movable, tender. All others not palpable.
Lungs: Breath sounds clear to auscultation, resonant to percussion throughout.
Hearing: Weber lateralizes to R.
Assessment
Serous otitis media, R ear, with mild URI
Transient conductive hearing loss
Disturbed sensory perception (auditory) R/T excessive fluid in middle ear
Pain R/T middle ear pressure
Focused Assessment: Clinical Case Study 3
Emma S., 78 years old, has a medical diagnosis of angina pectoris, which has responded to nitroglycerin PRN and periods of rest between activity. She has been independent in her own home, is coping well with activity restrictions through help from neighbors and family. Now hospitalized for evaluation of acute chest pain episode; MI has been ruled out, pain diagnosed as anginal, to be released to own home with a beta-blocking medication and nitroglycerin PRN.
Just before this hospitalization, Mrs. S. received a hearing aid after evaluation by audiologist at senior center. Mrs. S. was born in Germany, immigrated to U.S. at age 5 years, considers English her primary language.
Subjective
Since this hospitalization, feels “irritable and nervous.” Relates this to worry about heart and also, “I get so mixed up in here, this room is so strange, and I just can’t hear the nurses. They talk like cavemen, ‘oo-i-ee-uou.’” Tried using her new hearing aid but no relief. “It just kept screeching in my ear, and it made the monitor beep so loud it drove me crazy.” States no tinnitus, no vertigo.
Objective
Ears: Pinna with elongated lobes, but no tenderness to palpation, no discharge, no masses or lesions. Both canals clear of cerumen. Both TM appear gray-white, slightly opaque and dull, although all landmarks visible. No perforation.
Hearing: Difficulty hearing room conversation. Unable to hear whispered voice bilaterally.
Assessment
Chest pain/angina pectoris
Deficient knowledge R/T lack of teaching on hearing aid
Disturbed sensory perception (auditory) R/T effects of aging
Anxiety R/T change in cardiovascular health status and inability to communicate effectively
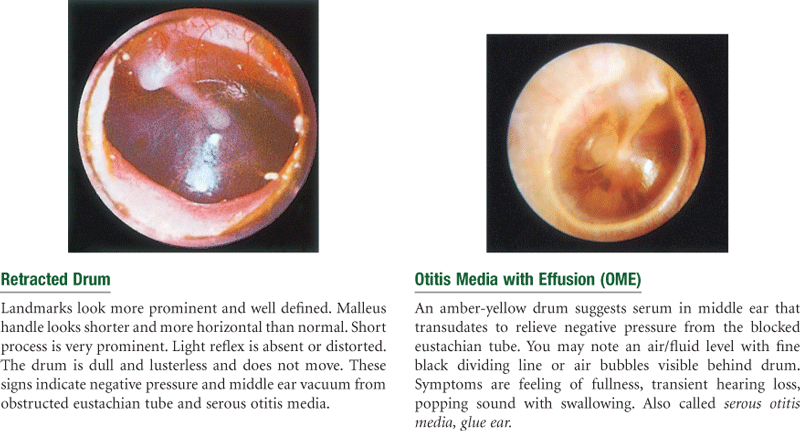
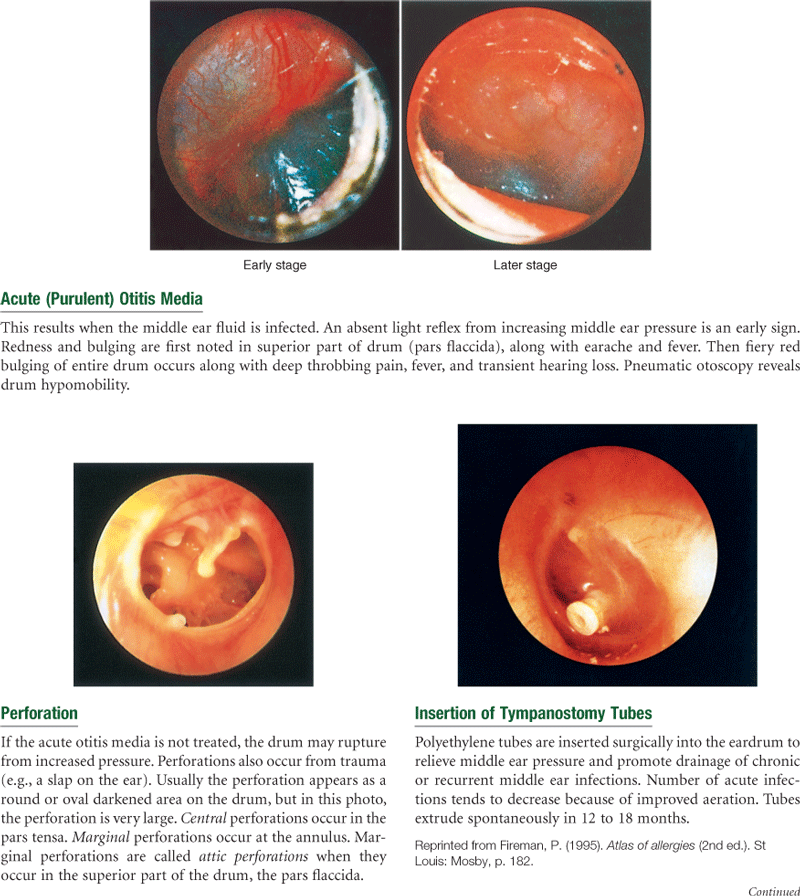
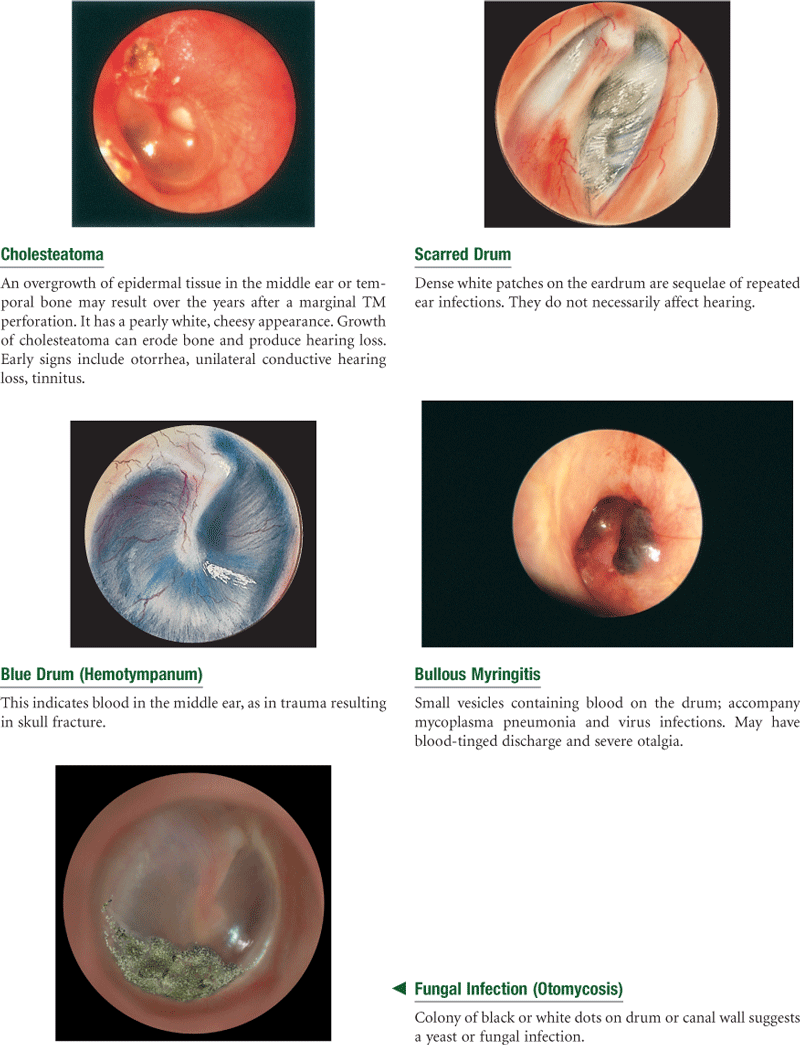
Abnormal Findings
Abnormal Findings FOR ADVANCED PRACTICE
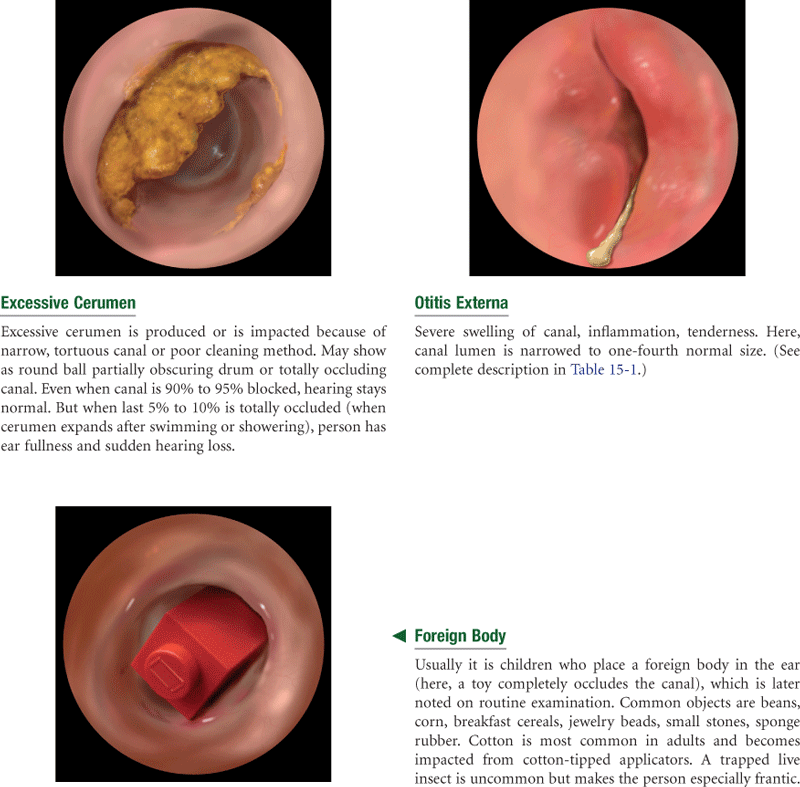
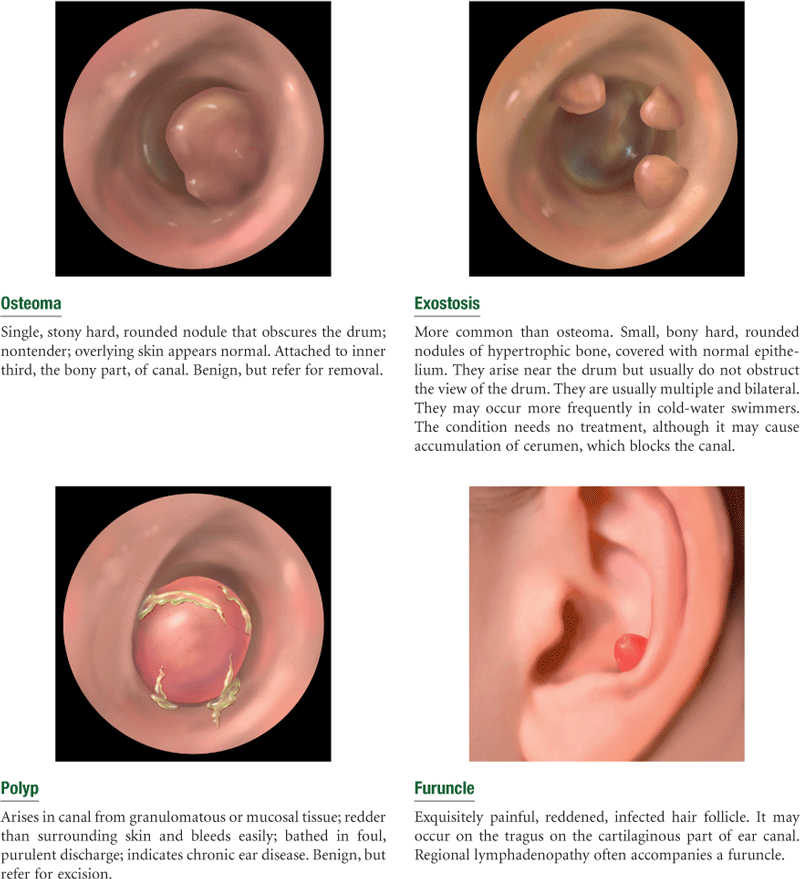
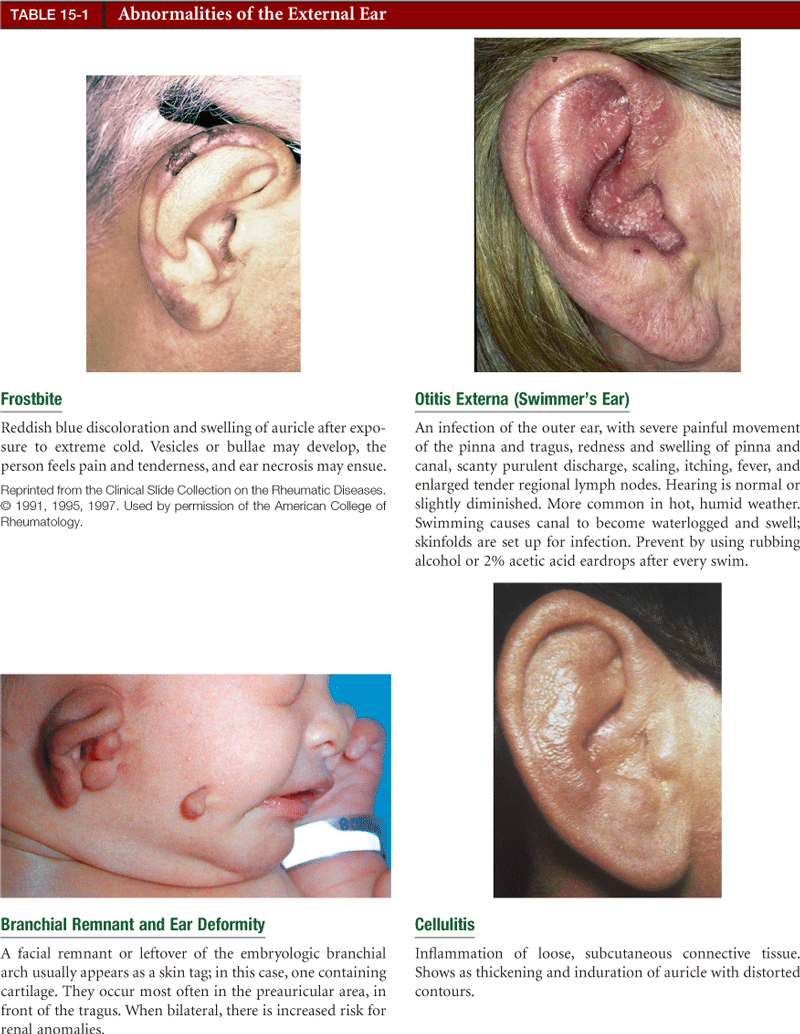
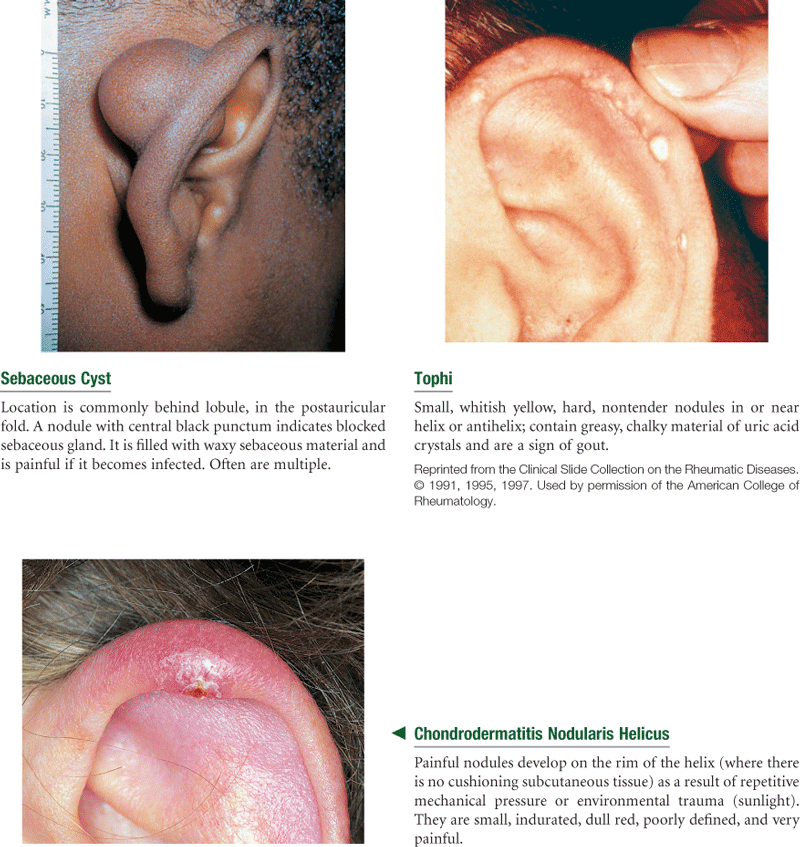
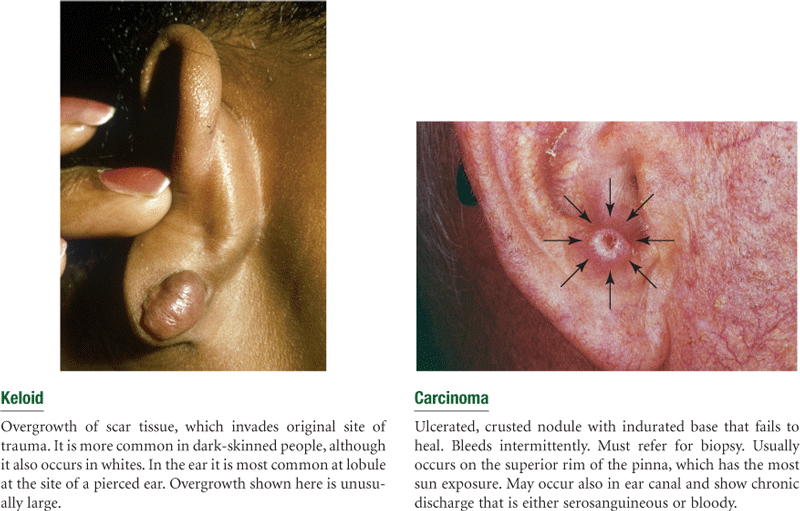
TABLE 15-4
Abnormal Views Seen on Otoscopy
| Appearance of Eardrum | Indicates | Suggested Condition |
| Yellow-amber color | Serum or pus | Serous otitis media or chronic otitis media |
| Prominent landmarks | Retraction of drum | Negative pressure in middle ear from an obstructed eustachian tube |
| Air/fluid level or air bubbles | Serous fluid | Serous otitis media |
| Absent or distorted light reflex | Bulging of eardrum | Acute otitis media |
| Bright red color | Infection in middle ear | Acute purulent otitis media |
| Blue or dark red color | Blood behind drum | Trauma, skull fracture |
| Dark oval areas | Perforation | Drum rupture |
| White dense areas | Scarring | Sequelae of infections |
| Diminished or absent landmarks | Thickened drum | Chronic otitis media |
| Black or white dots on drum or canal | Colony of growth | Fungal infection |
From Sherman, J. L., Fields, S. K. (1988). Guide to patient evaluation (5th ed.). New York: Medical Examination Publishing. Reprinted by permission of Elsevier Inc.
TABLE 15-5
Images © Pat Thomas, 2010. Reprinted from Fireman, P. (1995). Atlas of allergies (2nd ed.). St Louis: Mosby, p. 182.
Summary Checklist: Ear Examination
 For a PDA-downloadable version, go to http://evolve.elsevier.com/Jarvis/.
For a PDA-downloadable version, go to http://evolve.elsevier.com/Jarvis/.
Position and alignment on head
Note skin condition—color, lumps, lesions
Check movement of auricle and tragus for tenderness
Evaluate external auditory meatus—note size, swelling, redness, discharge, cerumen, lesions, foreign bodies
Cerumen, discharge, foreign bodies, lesions
Redness or swelling of canal wall
Note position (flat, bulging, retracted)
Bibliography
1. Askin DF. Physical assessment of the newborn: minor congenital anomalies. Nursing for Women’s Health. 2009;13(2):140–149.
2. Bagai A, Thavendiranathan P, Detsky A. Does this patient have hearing impairment? JAMA: Journal of the American Medical Association. 2006;29:416–428.
3. Brook I, Gober AE. Recovery of potential pathogens in the nasopharynx of healthy and otitis media–prone children and their smoking and nonsmoking parents. Annals of Otology, Rhinology, and Laryngology. 2008;117(10):727–730.
4. Carlson L. Otitis media: new information on an old disease. Nurse Practitioner. 2005;30:31–43.
5. Chantry C, Howard C, Auinger P. Full breastfeeding duration and associated decrease in respiratory tract infection in U.S children. Pediatrics. 2006;117:425–432.
6. Daugherty JA. The latest buzz on tinnitus. Nurse Practitioner. 2007;32(10):42–47.
7. Ely JW, Hansen MR, Clark EC. Diagnosis of ear pain. American Family Physician. 2008;77(5):621–628.
8. Feldman HM, Paradise JL. OME and child development: rethinking management. Contemporary Pediatrics. 2009;26(5):40–47.
9. Fischer T, Singer AJ, Chale S. Observation option for acute otitis media in the emergency department. Pediatric Emergency Care. 2009;25(9):575–578.
10. Gates G, Mills J. Presbycusis. Lancet. 2005;366:1111–1120.
11. Guest JF, Greener MJ, Robinson AC, Smith AF. Impacted cerumen: composition, production, epidemiology and management. Quarterly Journal of Medicine. 2004;97:477–488.
12. Holcomb SS. Get an earful of the new cerumen impaction guidelines. Nurse Practitioner. 2009;34(4):14–19.
13. Kane RL, Ouslander JG, Abrass IE. Essentials of clinical geriatrics. 6th ed New York: McGraw-Hill; 2009.
14. Kerschner JE. Bench and bedside advances in otitis media. Current Opinion in Otolaryngology & Head and Neck Surgery. 2008;16:543–547.
15. Lieu J, Feinstein A. Effect of gestational and passive smoke exposure on ear infections in children. Archives of Pediatrics & Adolescent Medicine. 2007;156:147–154.
16. Morris PS, Leach AJ. Acute and chronic otitis media. Pediatric Clinics of North America. 2009;56:1383–1399.
17. Oncel S. Acute otitis media in children. Journal of Pediatric Infections. 2009;3(Suppl. 1):39–42.
18. Singh A, Bond BL. Does this child have acute otitis media? Annals of Emergency Medicine. 2006;47:113–116.
19. Tomita H, Yamada K, Ghadami M, et al. Mapping of the wet/dry locus to the pericentromeric región of chromosome 16. Lancet. 2002;359(99322):2000–2002.
20. Wallhagen M, Pettengill E, Whiteside M. Sensory impairment in older adults Part 1 Hearing loss. American Journal of Nursing. 2006;106:40–49.