Nose, Mouth, and Throat
Outline

http://evolve.elsevier.com/Jarvis/
• Bedside Assessment Summary Checklist
• Physical Examination Summary Checklist
Structure and Function
Nose
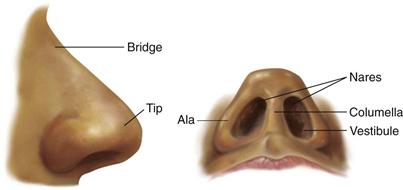
The nose is the first segment of the respiratory system. It warms, moistens, and filters the inhaled air, and it is the sensory organ for smell. The external nose is shaped like a triangle with one side attached to the face (Fig. 16-1). On its leading edge, the superior part is the bridge and the free corner is the tip. The oval openings at the base of the triangle are the nares; just inside, each naris widens into the vestibule. The columella divides the two nares and is continuous inside with the nasal septum. The ala is the lateral outside wing of the nose on either side. The upper third of the external nose is made up of bone; the rest is cartilage.
Inside, the nasal cavity is much larger than the external nose would indicate (Fig. 16-2). It extends back over the roof of the mouth. The anterior edge of the cavity is lined with numerous coarse nasal hairs, or vibrissae. The rest of the cavity is lined with a blanket of ciliated mucous membrane. The nasal hairs filter the coarsest matter from inhaled air, whereas the mucous blanket filters out dust and bacteria. Nasal mucosa appears redder than oral mucosa because of the rich blood supply present to warm the inhaled air.
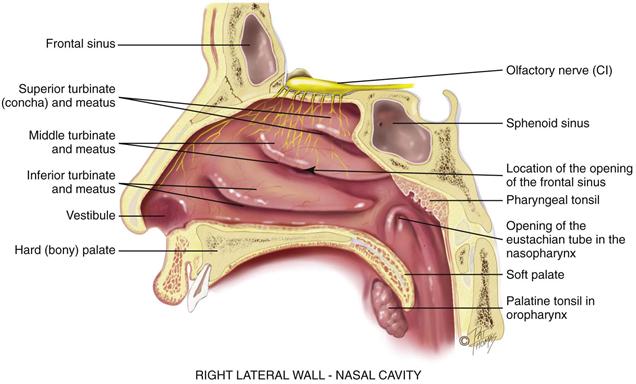
16-2 Copyright © (2006) © Pat Thomas, 2006.
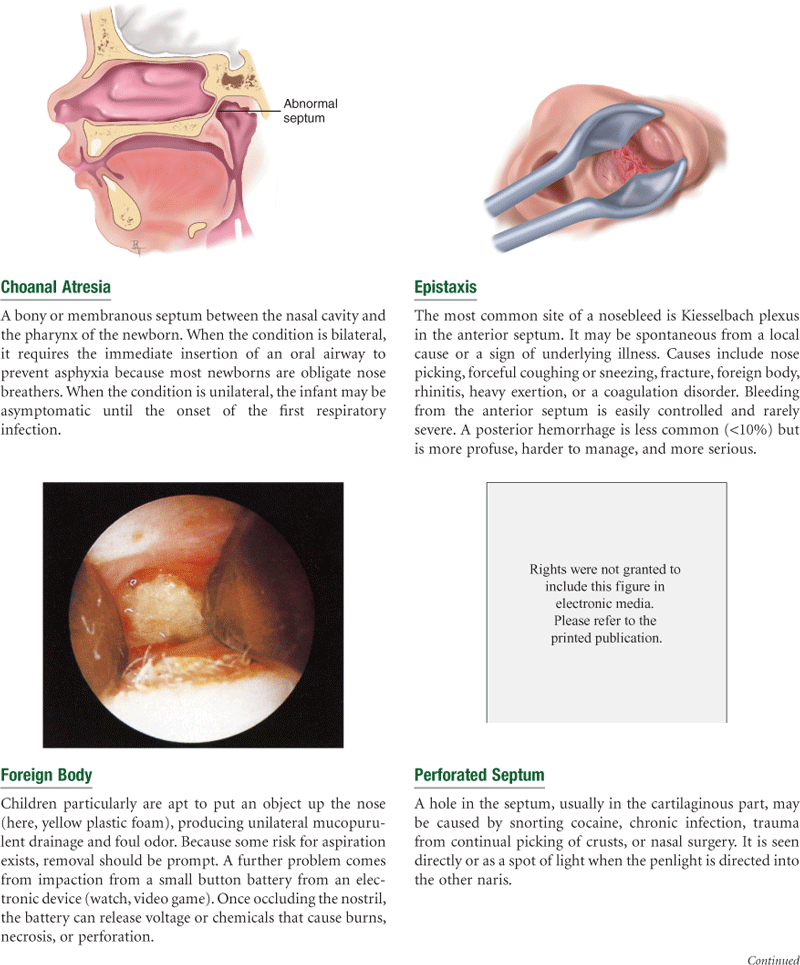
The nasal cavity is divided medially by the septum into two slitlike air passages. The anterior part of the septum holds a rich vascular network, Kiesselbach plexus, the most common site of nosebleeds. In many people, the nasal septum is not absolutely straight and may deviate toward one passage.
The lateral walls of each nasal cavity contain three parallel bony projections—the superior, middle, and inferior turbinates. They increase the surface area so that more blood vessels and mucous membranes are available to warm, humidify, and filter the inhaled air. Underlying each turbinate is a cleft, the meatus, which is named for the turbinate above. The sinuses drain into the middle meatus, and tears from the nasolacrimal duct drain into the inferior meatus.
The olfactory receptors (hair cells) lie at the roof of the nasal cavity and in the upper one third of the septum. These receptors for smell merge into the olfactory nerve, cranial nerve I, which transmits to the temporal lobe of the brain. Although it is not necessary for human survival, the sense of smell adds to nutrition by enhancing the pleasure and taste of food.
The paranasal sinuses are air-filled pockets within the cranium (Fig. 16-3). They communicate with the nasal cavity and are lined with the same type of ciliated mucous membrane. They lighten the weight of the skull bones, serve as resonators for sound production, and provide mucus, which drains into the nasal cavity. The sinus openings are narrow and easily occluded, which may cause inflammation or sinusitis.
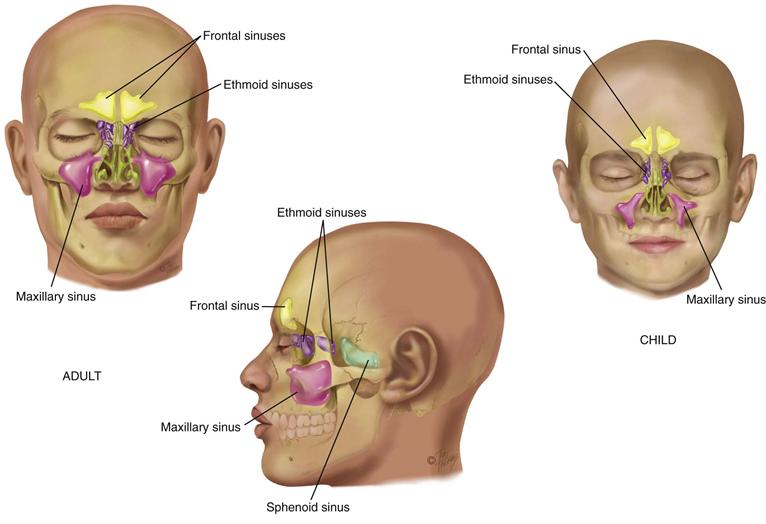
Two pairs of sinuses are accessible to examination: the frontal sinuses in the frontal bone above and medial to the orbits; and the maxillary sinuses in the maxilla (cheekbone) along the side walls of the nasal cavity. The other two sets are smaller and deeper: the ethmoid sinuses between the orbits; and the sphenoid sinuses deep within the skull in the sphenoid bone.
Only the maxillary and ethmoid sinuses are present at birth. The maxillary sinuses reach full size after all permanent teeth have erupted. The ethmoid sinuses grow rapidly between 6 and 8 years of age and after puberty. The frontal sinuses are absent at birth, are fairly well developed between 7 and 8 years of age, and reach full size after puberty. The sphenoid sinuses are minute at birth and develop after puberty.
Mouth
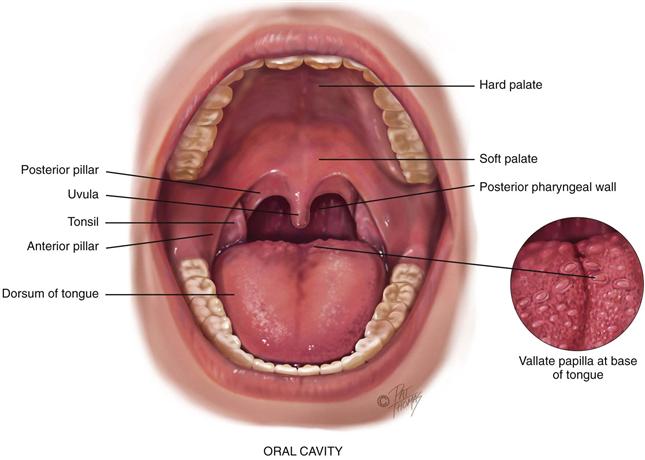
The mouth is the first segment of the digestive system and an airway for the respiratory system. The oral cavity is a short passage bordered by the lips, palate, cheeks, and tongue. It contains the teeth and gums, tongue, and salivary glands (Fig. 16-4).
16-4 Copyright © (2006) © Pat Thomas, 2010.
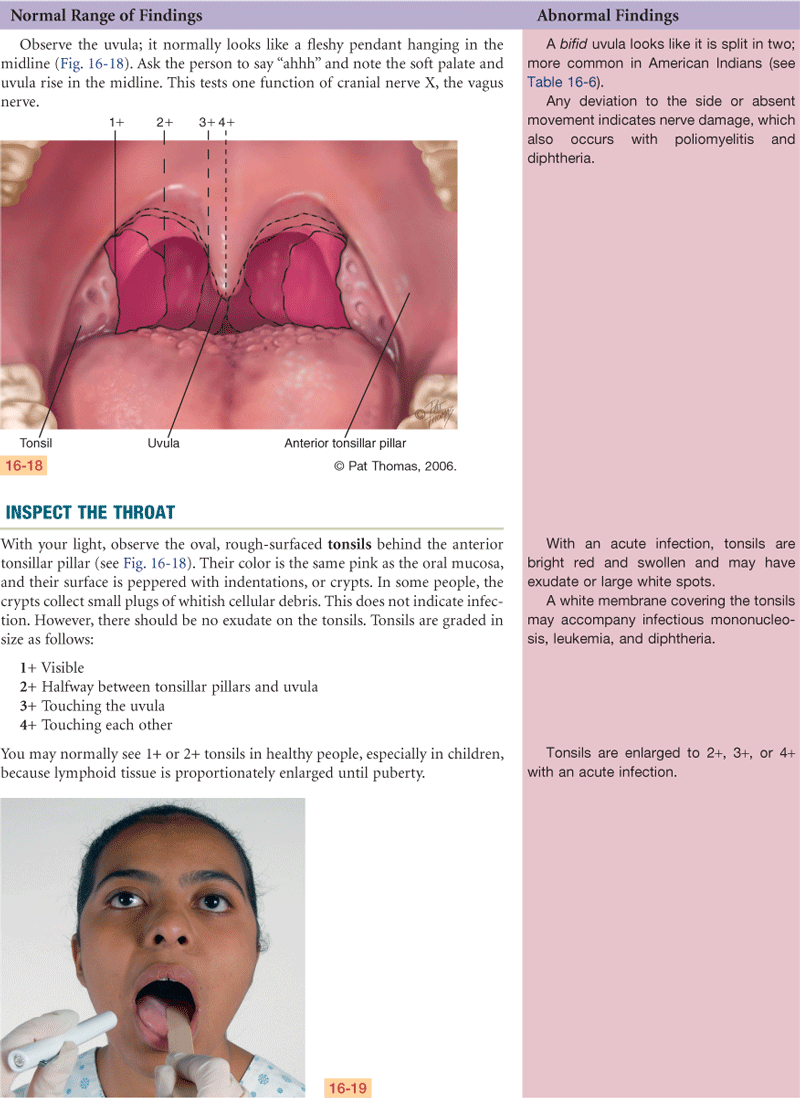
The lips are the anterior border of the oral cavity—the transition zone from the outer skin to the inner mucous membrane lining the oral cavity. The arching roof of the mouth is the palate; it is divided into two parts. The anterior hard palate is made up of bone and is a whitish color. Posterior to this is the soft palate, an arch of muscle that is pinker in color and mobile. The uvula is the free projection hanging down from the middle of the soft palate. The cheeks are the side walls of the oral cavity.
The floor of the mouth consists of the horseshoe-shaped mandible bone, the tongue, and underlying muscles. The tongue is a mass of striated muscle arranged in a crosswise pattern so that it can change shape and position. The papillae are the rough, bumpy elevations on its dorsal surface. Note the larger vallate papillae in an inverted V shape across the posterior base of the tongue, and do not confuse them with abnormal growths. Underneath, the ventral surface of the tongue is smooth and shiny and has prominent veins. The frenulum is a midline fold of tissue that connects the tongue to the floor of the mouth.
The tongue’s ability to change shape and position enhances its functions in mastication, swallowing, cleansing the teeth, and the formation of speech. The tongue also functions in taste sensation. Microscopic taste buds are in the papillae at the back and along the sides of the tongue and on the soft palate.
The mouth contains three pairs of salivary glands (Fig. 16-5). The largest, the parotid gland, lies within the cheeks in front of the ear extending from the zygomatic arch down to the angle of the jaw. Its duct, Stensen’s duct, runs forward to open on the buccal mucosa opposite the second molar. The submandibular gland is the size of a walnut. It lies beneath the mandible at the angle of the jaw. Wharton’s duct runs up and forward to the floor of the mouth and opens at either side of the frenulum. The smallest, the almond-shaped sublingual gland, lies within the floor of the mouth under the tongue. It has many small openings along the sublingual fold under the tongue.
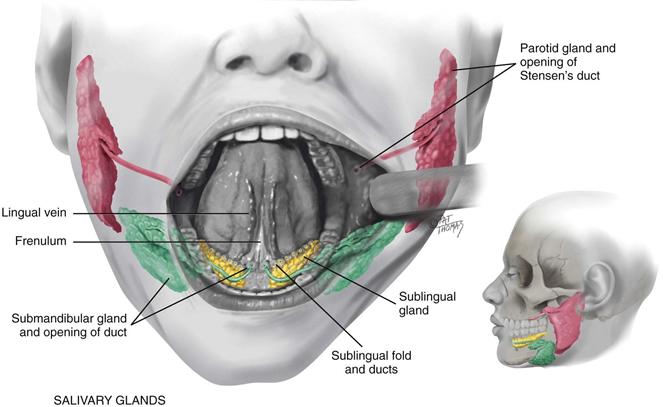
16-5 Copyright © (2006) © Pat Thomas, 2010.
The glands secrete saliva, the clear fluid that moistens and lubricates the food bolus, starts digestion, and cleans and protects the mucosa.
Adults have 32 permanent teeth—16 in each arch. Each tooth has three parts: the crown, the neck, and the root. The gums (gingivae) collar the teeth. They are thick, fibrous tissues covered with mucous membrane. The gums are different from the rest of the oral mucosa because of their pale pink color and stippled surface.
Throat
The throat, or pharynx, is the area behind the mouth and nose. The oropharynx is separated from the mouth by a fold of tissue on each side, the anterior tonsillar pillar (see Fig. 16-4). Behind the folds are the tonsils, each a mass of lymphoid tissue. The tonsils are the same color as the surrounding mucous membrane, although they look more granular and their surface shows deep crypts. Tonsillar tissue enlarges during childhood until puberty and then involutes. The posterior pharyngeal wall is seen behind these structures. Some small blood vessels may show on it.
The nasopharynx is continuous with the oropharynx, although it is above the oropharynx and behind the nasal cavity. The pharyngeal tonsils (adenoids) and the eustachian tube openings are located here (see Fig. 16-2).
The oral cavity and throat have a rich lymphatic network. Review the lymph nodes and their drainage patterns in Chapter 13 and keep this in mind when evaluating the mouth.
 Developmental Competence
Developmental Competence
Infants and Children
In the infant, salivation starts at 3 months. The baby will drool for a few months before learning to swallow the saliva. This drooling does not herald the eruption of the first tooth, although many parents think it does.
The teeth, both sets, begin development in utero. Children have 20 deciduous, or temporary, teeth. These erupt between 6 months and 24 months of age. All 20 teeth should appear by  years of age. The deciduous teeth are lost beginning at age 6 years through age 12 years. They are replaced by the permanent teeth, starting with the central incisors (Fig. 16-6). The permanent teeth appear earlier in girls than in boys, and they erupt earlier in Black children than in white children.
years of age. The deciduous teeth are lost beginning at age 6 years through age 12 years. They are replaced by the permanent teeth, starting with the central incisors (Fig. 16-6). The permanent teeth appear earlier in girls than in boys, and they erupt earlier in Black children than in white children.
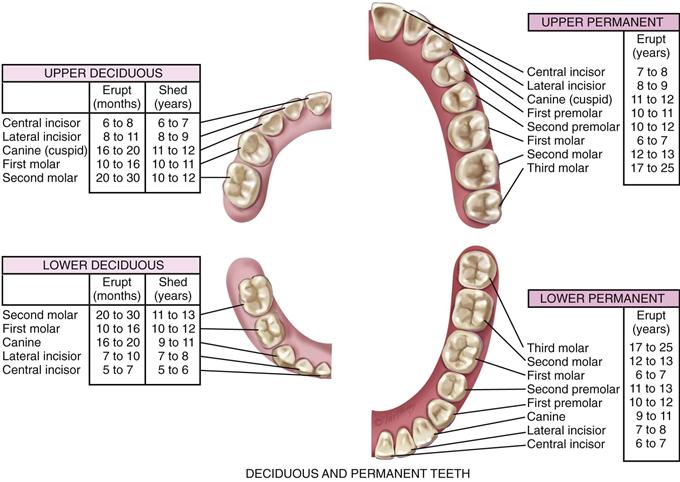
16-6 Copyright © (2006) © Pat Thomas, 2006.
The nose develops during adolescence, along with other secondary sex characteristics. This growth starts at age 12 or 13 years, reaching full growth at age 16 years in females and age 18 years in males.
The Pregnant Woman
Nasal stuffiness and epistaxis may occur during pregnancy as a result of increased vascularity in the upper respiratory tract. Also, the gums may be hyperemic and softened and may bleed with normal toothbrushing. Contrary to superstitious folklore, pregnancy does not cause tooth decay or loss.
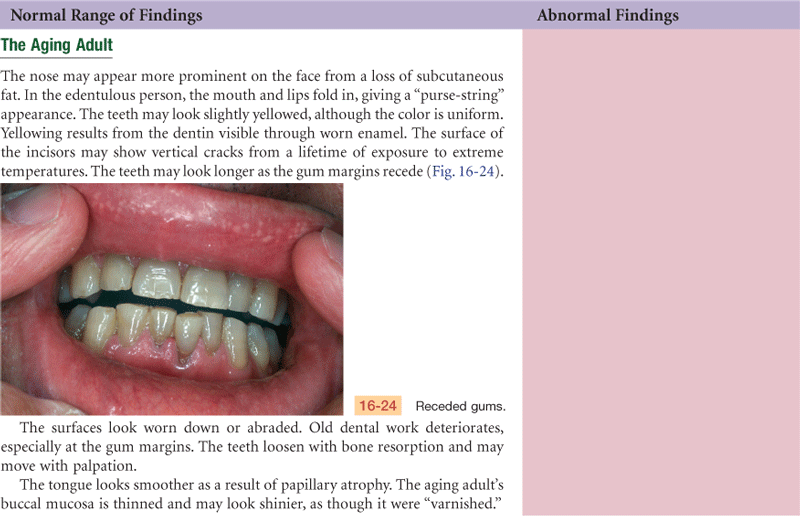
The Aging Adult
A gradual loss of subcutaneous fat starts during later adult years, making the nose appear more prominent in some people. The nasal hairs grow coarser and stiffer and may not filter the air as well. The hairs protrude and may cause itching and sneezing. Many older people clip these hairs, thinking them unsightly, but this practice can cause infection. The sense of smell may diminish because of a decrease in the number of olfactory nerve fibers. The decrease in the sensation of smell begins after age 60 years and continues progressively with age.
In the oral cavity, the soft tissues atrophy and the epithelium thins, especially in the cheeks and tongue. This results in loss of taste buds, with about an 80% reduction in taste functioning. Further impairments to taste include a decrease in salivary secretion that is needed to dissolve flavoring agents and the presence of upper dentures that cover secondary taste sites.
Atrophic tissues ulcerate easily, which increases risk for infections such as oral moniliasis. The risk for malignant oral lesions also increases.
Many dental changes occur with aging. The tooth surface is abraded. The gums begin to recede, and the teeth begin to erode at the gum line. A smooth V-shaped cavity forms around the neck of the tooth, exposing the nerve and making the tooth hypersensitive. Some tooth loss may occur from bone resorption (osteoporosis), which decreases the inner tooth structure and its outer support. Natural tooth loss is exacerbated by years of inadequate dental care, decay, poor oral hygiene, and tobacco use.
If tooth loss occurs, the remaining teeth drift, causing malocclusion. The stress of chewing with maloccluding teeth causes further problems: (1) further tooth loss; (2) muscle imbalance from a mandible and maxilla now out of alignment, which produces muscle spasms, tenderness of muscles of mastication, and chronic headaches; and (3) stress on the temporomandibular joint, leading to osteoarthritis, pain, and inability to fully open the mouth.
A diminished sense of taste and smell decreases the aging person’s interest in food and may contribute to malnutrition. Saliva production decreases; saliva acts as a solvent for food flavors and helps move food around the mouth. Decreased saliva also reduces the mouth’s self-cleaning property. The major cause of decreased saliva flow is not the aging process itself but, rather, the use of medications that have anticholinergic effects. More than 250 medications have a side effect of dry mouth.
The absence of some teeth and trouble with mastication encourage the older person to eat soft foods (usually high in carbohydrates) and to decrease meat and fresh vegetable intake. This produces a risk for nutritional deficit for protein, vitamins, and minerals.
 Culture and Genetics
Culture and Genetics
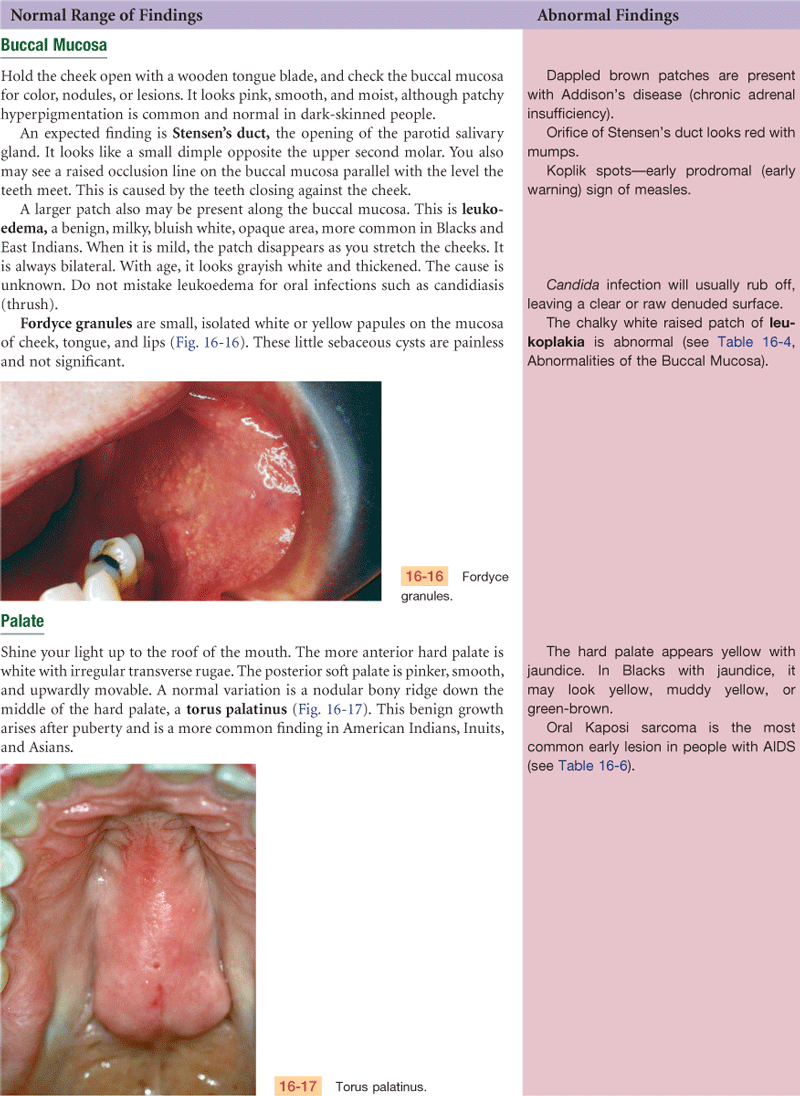
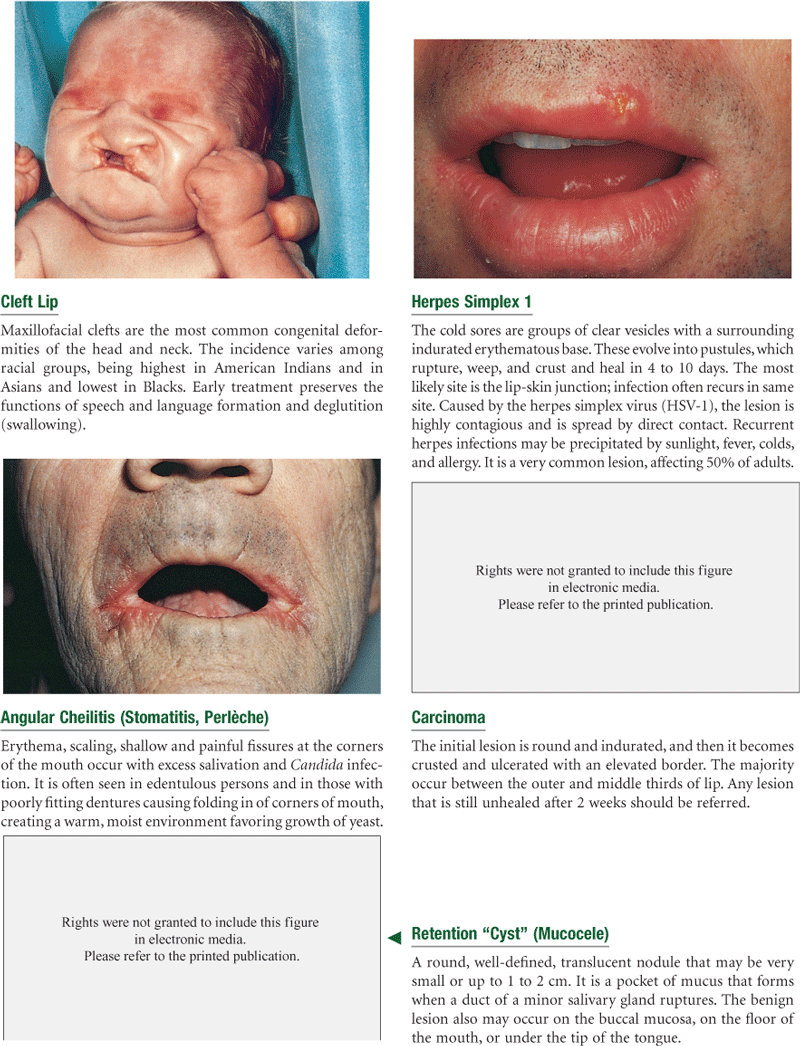
Bifid uvula, a condition in which the uvula is split either completely or partially, occurs in 18% of some American Indian groups and in 10% of Asians. The occurrence in whites and Blacks is rare. Cleft lip and cleft palate are most common in Asian-American newborns (1/800) and American Indians, less common in Caucasians (1/1000), and least common among African Americans (1/1200).28 Both genetic and environmental factors contribute to the emergence of torus palatinus, a benign bony ridge running in the middle of the hard palate (see Fig. 16-17). The prevalence of torus palatinus and torus mandibularis is higher in Asians than in Caucasians14 and is higher in women than in men.4 Leukoedema is a milky, bluish-white, opaque appearance of the buccal mucosa. It occurs more often in darkly pigmented persons and is seen most often in African Americans.3 The incidence of natal teeth (baby born with teeth) is rare, about 1:2000 to 1:3500 live births, but is more common among American Indian infants.18
Throughout life, whites have more tooth decay than Blacks. The differences in tooth decay between Blacks and whites occur because Blacks have harder and denser tooth enamel, which makes their teeth less susceptible to the organisms that cause caries.
The incidence of tooth loss and edentulism has decreased substantially in the United States over the past several decades because of fluoridation, improved dental treatment, and better personal care. Although the overall prevalence of edentulism has dropped to 10.5% of the population, significant variations remain among subgroups in the population. Blacks, Hispanics, American Indians, and Alaska Natives have the poorest oral health of all racial and ethnic groups in the United States.
In the United States, the incidence and mortality rates for oral and pharyngeal cancer have declined since the mid-1980s. However, some racial disparity persists. The incidence rate was 20% higher for African-American men than for white men, while the difference between women was small. The mortality rates were 82% higher for African-American men compared with white men, but rates were similar for African-American and white women.19 The disparity in survival rate may be attributed to racial differences in stage at diagnosis, age, gender, socioeconomic status, and treatment received.
In 2007, 62.7% of adults ages 18 to 64 years visited a dentist. Some racial disparity exists: for whites, it was 64.2%; for African Americans, 55%; and for Hispanics, 48.9%. The percentage of adults who had untreated caries between 2001 and 2004 was 26.8%. By origin, the breakdown was 21.5% for whites; 42.9% for African Americans; and 40.1% for Hispanics.21 Poverty and access to care are factors in this disparity.

Objective Data
| Preparation | Equipment needed |
| Position the person sitting up straight with his or her head at your eye level. If the person wears dentures, offer a paper towel and ask the person to remove them. | Otoscope with short, wide-tipped nasal speculum attachment Penlight Two tongue blades Cotton gauze pad (4 × 4 inches) Gloves |
 Documentation and Critical Thinking
Documentation and Critical Thinking
Sample Charting
Subjective
Nose: No history of discharge, sinus problems, obstruction, epistaxis, or allergy. Colds 1-2/yr, mild. Fractured nose during high school sports, treated by MD.
Mouth and Throat: No pain, lesions, bleeding gums, toothache, dysphagia, or hoarseness. Occasional sore throat with colds. Tonsillectomy, age 8. Smokes cigarettes 1 PPD × 9 years. Alcohol-1-2 drinks socially, about 2×/month. Visits dentist annually, dental hygienist 2×/year, flosses daily. No dental appliance.
Objective
Nose: Symmetric, no deformity or skin lesions. Nares patent. Mucosa pink; no discharge, lesions, or polyps; no septal deviation or perforation. Sinuses—no tenderness to palpation.
Mouth: Can clench teeth. Mucosa and gingivae pink, no masses or lesions. Teeth are all present, straight, and in good repair. Tongue smooth, pink, no lesions, protrudes in midline, no tremor.
Throat: Mucosa pink, no lesions or exudate. Uvula rises in midline on phonation. Tonsils out. Gag reflex present.
Assessment
Structures intact and appear healthy
Focused Assessment: Clinical Case Study 1
Brad D., a 34-year-old electrician, seeks care for “sore throat for 2 days.”
Subjective
2 days PTA—experienced sudden onset of sore throat, swollen glands, fever 101° F, occasional shaking chills, extreme fatigue.
Today—symptoms remain. Cough productive of yellow sputum. Treated self with aspirin for minimal relief. Unable to eat past 2 days because “throat on fire.” Taking adequate fluids, on bedrest. Not aware of exposure to other sick persons. Does not smoke.
Objective
Ears: Tympanic membranes pearl gray with landmarks intact.
Nose: No discharge. Mucosa pink, no swelling.
Mouth: Mucosa and gingivae pink, no lesions.
Throat: Tonsils 3+. Pharyngeal wall bright red with yellow-white exudate, exudate also on tonsils.
Neck: Enlarged anterior cervical nodes bilaterally, painful to palpation. No other lymph adenopathy.
Chest: Resonant to percussion throughout. Breath sounds clear anterior and posterior. No adventitious sounds.
Assessment
Pharyngitis
Pain R/T inflammation
Imbalanced nutrition: less than body requirements R/T dysphagia
Focused Assessment: Clinical Case Study 2
Calvin W., a 53-year-old white businessman, is in the hospital awaiting coronary bypass surgery for coronary artery disease. He is allergic to dust and animal hair. As part of a preoperative teaching plan for coughing and deep breathing, a respiratory assessment is performed.
Subjective
States understanding of reason for admission to hospital and extent of coronary artery disease. Unaware of details of surgical procedure and postoperative care. Interested: “I do better when I know what I’m dealing with.” History of exertional angina after walking one short block or climbing one flight of stairs, treats self with nitroglycerin. Does not smoke. Chronic watery nasal discharge, “comes and goes, but present most of time.”
Objective
Nose: Only R naris patent. Mucosa gray and boggy bilaterally. L naris has mobile, gray, nontender mass, obstructing view of turbinates and rest of nasal cavity.
Mouth and Throat: Mucosa pink, no lesions. Uvula midline, rises on phonation. Tonsils absent. No lumps or lesions on palpation.
Chest: Thorax symmetric; AP < transverse diameter; respirations 18/min, effortless. Resonant to percussion. Breath sounds are clear. No adventitious sounds.
Assessment
L nasal mass, possibly polyp
Deficient knowledge for surgery and expected postop course R/T lack of exposure
Focused Assessment: Clinical Case Study 3
Esther V. is a 61-year-old professor who has been admitted to the hospital for chemotherapy for carcinoma of the breast. This is her 5th day in the hospital. An oral assessment is performed when she complains of “soreness and a white coating” in the mouth.
Subjective
Felt soreness on tongue and cheeks during night. Now pain persists, and E.V. can see a “white coating” on tongue and cheeks. “I’m worried. Is this more cancer?”
Objective
E.V. generally appears restless and overly aware.
Oral mucosa pink. Large white, cheesy patches covering most of dorsal surface of tongue and buccal mucosa. Will scrape off with tongue blade, revealing red eroded area beneath.
Bleeds with slight contact. Posterior pharyngeal wall pink, no lesions. Patches are soft to palpation. No palpable lymph nodes.
Assessment
Oral lesion, appears as candidiasis
Impaired oral mucous membrane R/T effects of chemotherapy
Pain R/T infectious process
Anxiety R/T threat to health status
Summary Checklist: Nose, Mouth, and Throat Examination
 For a PDA-downloadable version, go to http://evolve.elsevier.com/Jarvis/.
For a PDA-downloadable version, go to http://evolve.elsevier.com/Jarvis/.
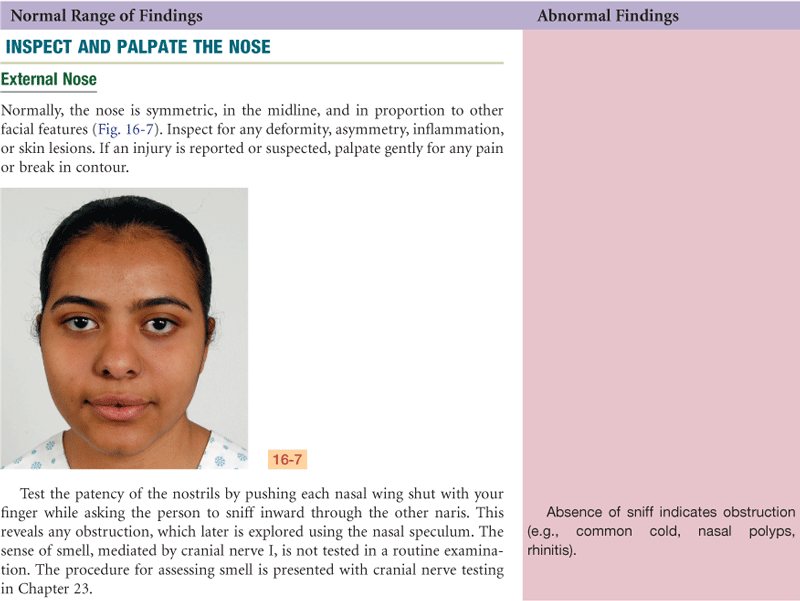
1. Inspect external nose for symmetry, any deformity, or lesions
2. Palpation—test patency of each nostril
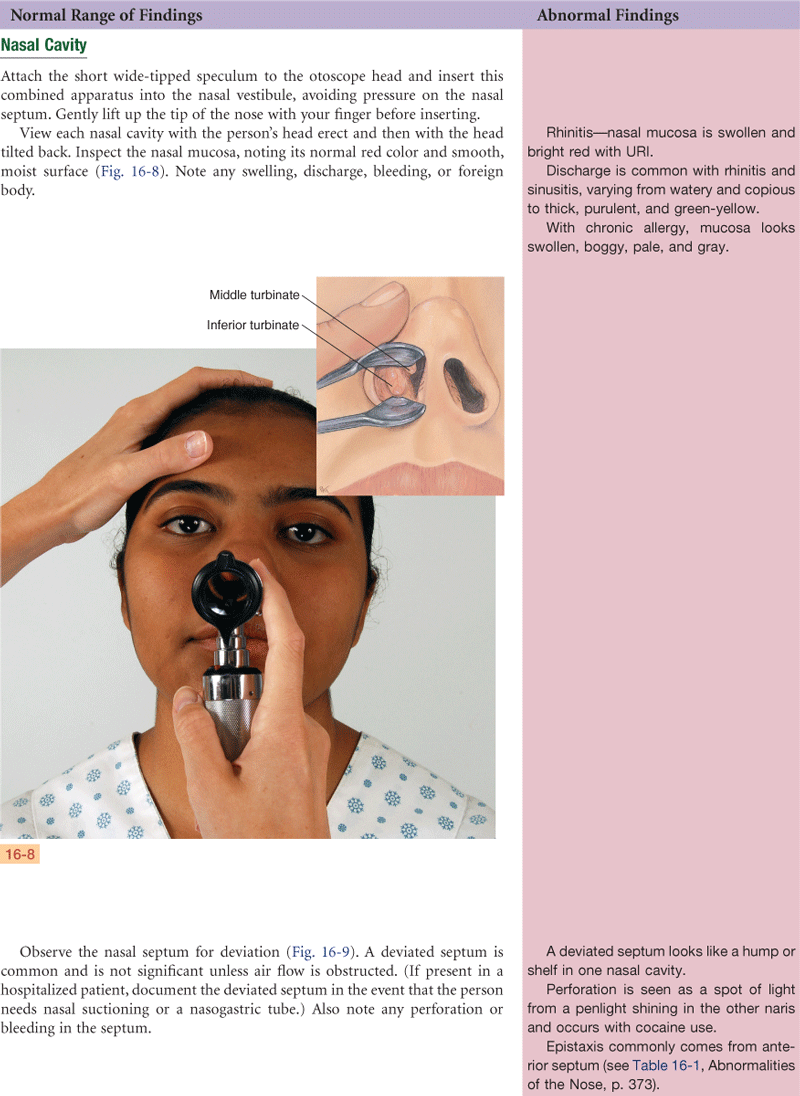
3. Inspect with nasal speculum:
Color and integrity of nasal mucosa
Septum—note any deviation, perforation, or bleeding
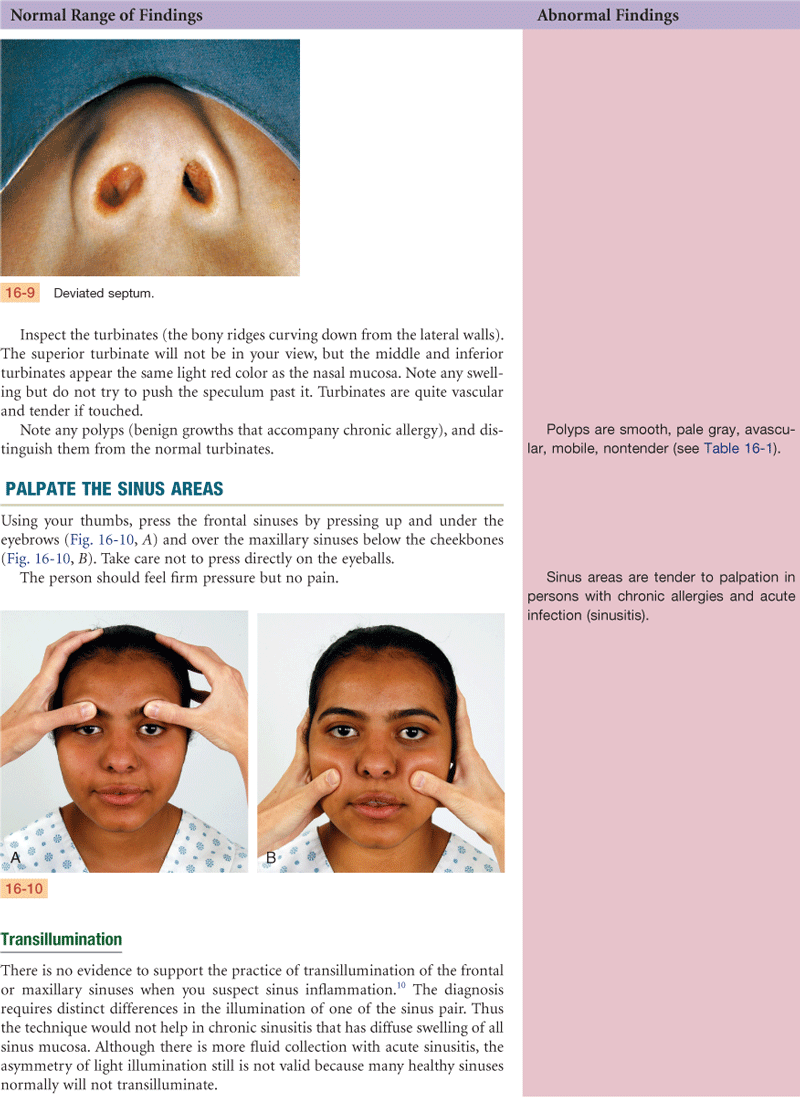
Turbinates—note color, any exudate, swelling, or polyps
4. Palpate the sinus areas—note any tenderness
Lips, teeth and gums, tongue, buccal mucosa—note color; whether structures are intact; any lesions
Palate and uvula—note integrity and mobility as person phonates
Pharyngeal wall—note color, any exudate, or lesions
When indicated in adults, bimanual palpation of mouth
With the neonate, palpate for integrity of palate and to assess sucking reflex
Bibliography
1. Armengol C, Hendley O, Schlager T. An office-based guide to diagnosing streptococcal pharyngitis. Contemporary Pediatrics. 2006;23:64–70.
2. Bernius M, Perlin D. Pediatric ear, nose, and throat emergencies. Pediatric Clinics of North America. 2006;53:195–214.
3. Burkhart N. Leukoedema. Retrieved April 25, 2010, from www.rdhmag.com/display_article/346087/56/none/none/Colum/Leukoedema; 2008.
4. Chohayeb AA, Volpe AR. Occurrence of torus palatinus and mandibularis among women of different ethnic groups. American Journal of Dentistry. 2001;14(5):278–280.
5. Conboy-Ellis K, Braker-Shaver S. Intranasal steroids and allergic rhinitis. Nurse Practitioner. 2007;32(4):44–49.
6. Curtis EK. Meth mouth: a review of methamphetamine use and its oral manifestations. General Dentistry. 2006;54(2):125–129.
7. da Silva CM, Ramos MM, deCarvalho Carrara CF, et al. Oral characteristics of newborns. Journal of Dentistry for Children. 2008;75(1):4–6.
8. Eisenstadt ES. Dysphagia and aspiration pneumonia in older adults. Journal of the American Academy of Nurse Practitioners. 2010;22:17–22.
9. Foster E. Uncovering sleep apnea misconceptions. Nurse Practitioner. 2008;33(6):23–28.
10. Godley FA. Chronic sinusitis: an update. American Family Physician. 1992;45(5):2190–2199.
11. Gonsalves WC, Wrightson AS, Henry RG, et al. Common oral conditions in older persons. American Family Physician. 2008;78(7):845–852.
12. Holcomb SS. Diagnosing rhinosinusitis: know your guidelines. Nurse Practitioner. 2008;33(11):6–9.
13. Hoyle C. Make your strep diagnosis spot on. Nurse Practitioner. 2009;34(10):47–52.
14. Jainkittivong A, Langlais RP. Buccal and palatal exostoses: prevalence and concurrence with tori. Oral Surgery, Oral Medicine, and Oral Pathology. 2000;90(1):48–53.
15. Kamienski M. When sore throat gets serious. American Journal of Nursing. 2007;107(10):35–38.
16. Kane RL, Ouslander JG, Abrass IE. Essentials of clinical geriatrics. 6th ed New York: McGraw-Hill; 2009.
17. Lafreniere D, Mann N. Anosmia: loss of smell in the elderly. Otolaryngologic Clinics of North America. 2009;42(1):123–131.
18. Leung AKC, Robson WLM. Natal teeth: a review. Journal of the National Medical Association. 2006;98(2):226–228.
19. Morse DE, Kerr AR. Disparities in oral and pharyngeal cancer incidence: mortality and survival among Black and White Americans. Journal of the American Dental Association. 2006;137:203–212.
20. Myers NE, Compliment JM, Post JC, et al. Tonsilloliths: a common finding in pediatric patients. The Nurse Practitioner. 2006;31:53–54.
21. National Center for Health Statistics. Health, United States, 2009 with chartbook on trends in the health of Americans (USDHHS Publication No 2009-1232). Hyattsville, MD: Author; 2009.
22. Palmer JL, Metheny NA. Preventing aspiration in older adults with dysphagia. American Journal of Nursing. 2008;108(2):40–48.
23. Parthasarathy P, Ritamarie J. Identification of childhood caries. Nurse Practitioner. 2008;33(9):41–48.
24. Petersen PE. Oral cancer prevention and control: the approach of the World Health Organization. Oral Oncology. 2009;45:454–460.
25. Regan EN. Diagnosing rhinitis: viral and allergic characteristics. Nurse Practitioner. 2008;33(9):20–26.
26. Sieracki RL, Voelz LM, Johannik TM, et al. Development and implementation of an oral care protocol for patients with cancer. Clinical Journal of Oncology Nursing. 2009;13(6):718–722.
27. Stockdell R, Amella EJ. The Edinburgh Feeding Evaluation in Dementia Scale. The American Journal of Nursing. 2008;108(8):46–54.
28. U.S. Department of Health & Human Services, The Office of Minority Health. Cleft lip/palate more prevalent in Asians. Retrieved April 25, 2010, from http://minorityhealth.hhs.gov/templates/content.aspx?ID=7590&lvl=3&lv1ID=287; 2009.
29. Wagner FP, Mathiason MA. Using Centor criteria to diagnose streptococcal pharyngitis. Nurse Practitioner. 2008;33(9):10–12.