Head, Face, and Neck, Including Regional Lymphatics

http://evolve.elsevier.com/Jarvis/
• Bedside Assessment Summary Checklist
Structure and Function
The Head
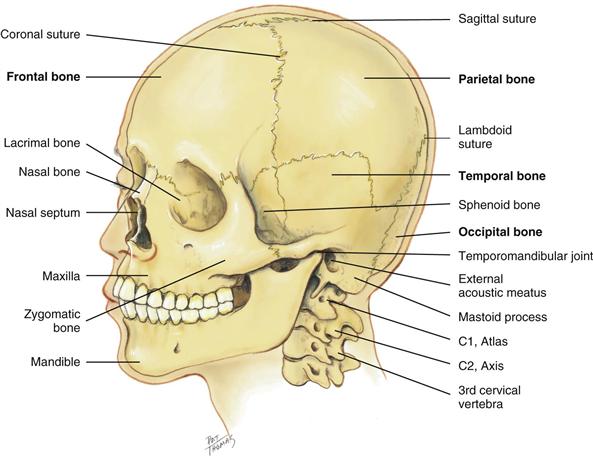
The skull is a rigid bony box that protects the brain and special sense organs, and it includes the bones of the cranium and the face (Fig. 13-1). Note the location of these cranial bones: frontal, parietal, occipital, and temporal. Use these names to describe any of your clinical findings in the corresponding areas.
13-1
The adjacent cranial bones unite at meshed immovable joints called the sutures. The bones are not firmly joined at birth; this allows for the mobility and change in shape needed for the birth process. The sutures gradually ossify during early childhood. The coronal suture crowns the head from ear to ear at the union of the frontal and parietal bones. The sagittal suture separates the head lengthwise between the two parietal bones. The lambdoid suture separates the parietal bones crosswise from the occipital bone.
The 14 facial bones also articulate at sutures (note the nasal bone, zygomatic bone, and maxilla), except for the mandible (the lower jaw). It moves up, down, and sideways from the temporomandibular joint, which is anterior to each ear.
The cranium is supported by the cervical vertebra: C1, the “atlas”; C2, the “axis”; and down to C7. The C7 vertebra has a long spinous process that is palpable when the head is flexed. Feel this useful landmark, the vertebra prominens, on your own neck.
The human face has myriad appearances and a large array of facial expressions that reflect mood. The expressions are formed by the facial muscles (Fig. 13-2), which are mediated by cranial nerve VII, the facial nerve. Facial muscle function is symmetric bilaterally, except for an occasional quirk or wry expression.
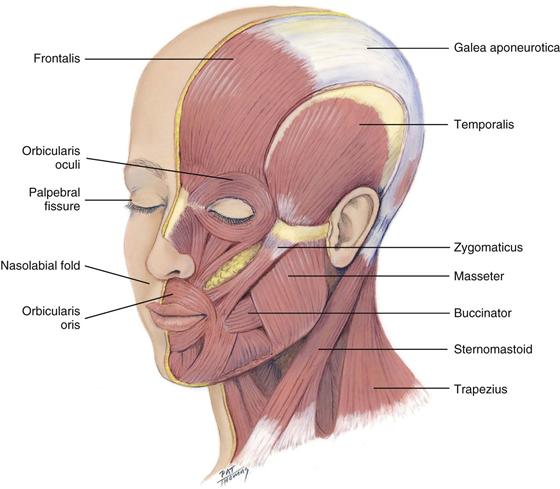
Facial structures also are symmetric; the eyebrows, eyes, ears, nose, and mouth appear about the same on both sides. The palpebral fissures—the openings between the eyelids—are equal bilaterally. Also, the nasolabial folds, the creases extending from the nose to each corner of the mouth, should look symmetric. Facial sensations of pain or touch are mediated by the three sensory branches of cranial nerve V, the trigeminal nerve. (Testing for sensory function is described in Chapter 23.)
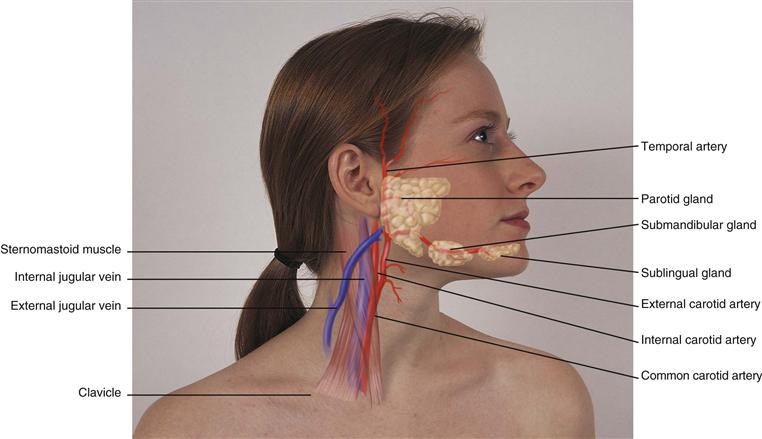
Two pairs of salivary glands are accessible to examination on the face (Fig. 13-3). The parotid glands are in the cheeks over the mandible, anterior to and below the ear. They are the largest of the salivary glands but are not normally palpable. The submandibular glands are beneath the mandible at the angle of the jaw. A third pair, the sublingual glands, lie in the floor of the mouth. (Salivary gland function follows in Chapter 16.) The temporal artery lies superior to the temporalis muscle; its pulsation is palpable anterior to the ear.
13-3
The Neck
The neck is delimited by the base of the skull and inferior border of the mandible above, and by the manubrium sterni, the clavicle, the first rib, and the first thoracic vertebra below. Think of the neck as a conduit for the passage of many structures, which are lying in close proximity: blood vessels, muscles, nerves, lymphatics, and viscera of the respiratory and digestive systems. Blood vessels include the common and internal carotid arteries and their associated veins (see Fig. 13-3). The internal carotid branches off the common carotid and runs inward and upward to supply the brain; the external carotid supplies the face, salivary glands, and superficial temporal area. The carotid artery and internal jugular vein lie beneath the sternomastoid muscle. The external jugular vein runs diagonally across the sternomastoid muscle. (See assessment of the neck vessels beginning on p. 470 in Chapter 19.)
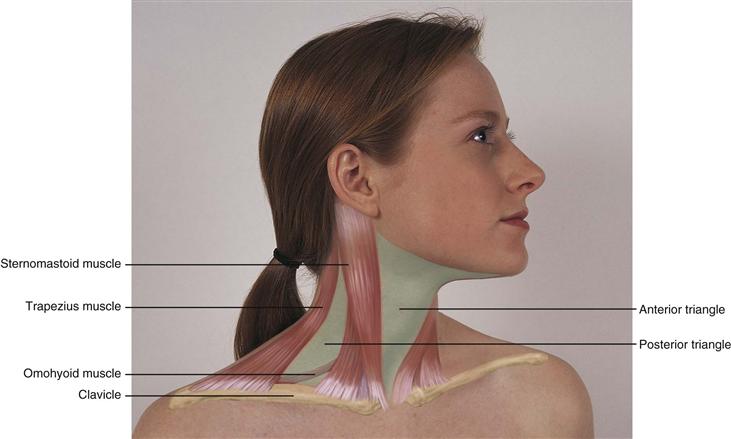
The major neck muscles are the sternomastoid and the trapezius (Fig. 13-4); they are innervated by cranial nerve XI, the spinal accessory. The sternomastoid muscle arises from the sternum and the clavicle and extends diagonally across the neck to the mastoid process behind the ear. It accomplishes head rotation and head flexion. The two trapezius muscles on the upper back arise from the occipital bone and the vertebrae and extend fanning out to the scapula and clavicle. The trapezius muscles move the shoulders and extend and turn the head.
13-4
The sternomastoid muscle divides each side of the neck into two triangles. The anterior triangle lies in front, between the sternomastoid and the midline of the body, with its base up along the lower border of the mandible and its apex down at the suprasternal notch. The posterior triangle is behind the sternomastoid muscle, with the trapezius muscle on the other side and with its base along the clavicle below. It contains the posterior belly of the omohyoid muscle. These triangles are helpful guidelines when describing findings in the neck.
The thyroid gland is an important endocrine gland with a rich blood supply. It straddles the trachea in the middle of the neck (Fig. 13-5). This highly vascular endocrine gland synthesizes and secretes thyroxine (T4) and triiodothyronine (T3), hormones that stimulate the rate of cellular metabolism. The gland has two lobes, both conical in shape, each curving posteriorly between the trachea and the sternomastoid muscle. The lobes are connected in the middle by a thin isthmus lying over the second and third tracheal rings.
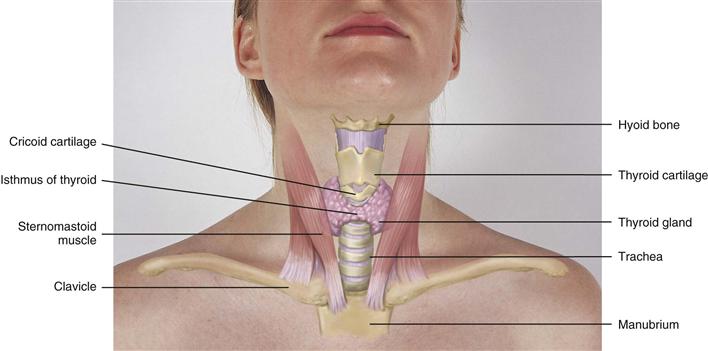
13-5
Just above the thyroid isthmus, within about 1 cm, is the cricoid cartilage or upper tracheal ring. The thyroid cartilage is above that, with a small, palpable notch in its upper edge. This is the prominent “Adam’s apple” in males. The highest is the hyoid bone, palpated high in the neck at the level of the floor of the mouth.
Lymphatics
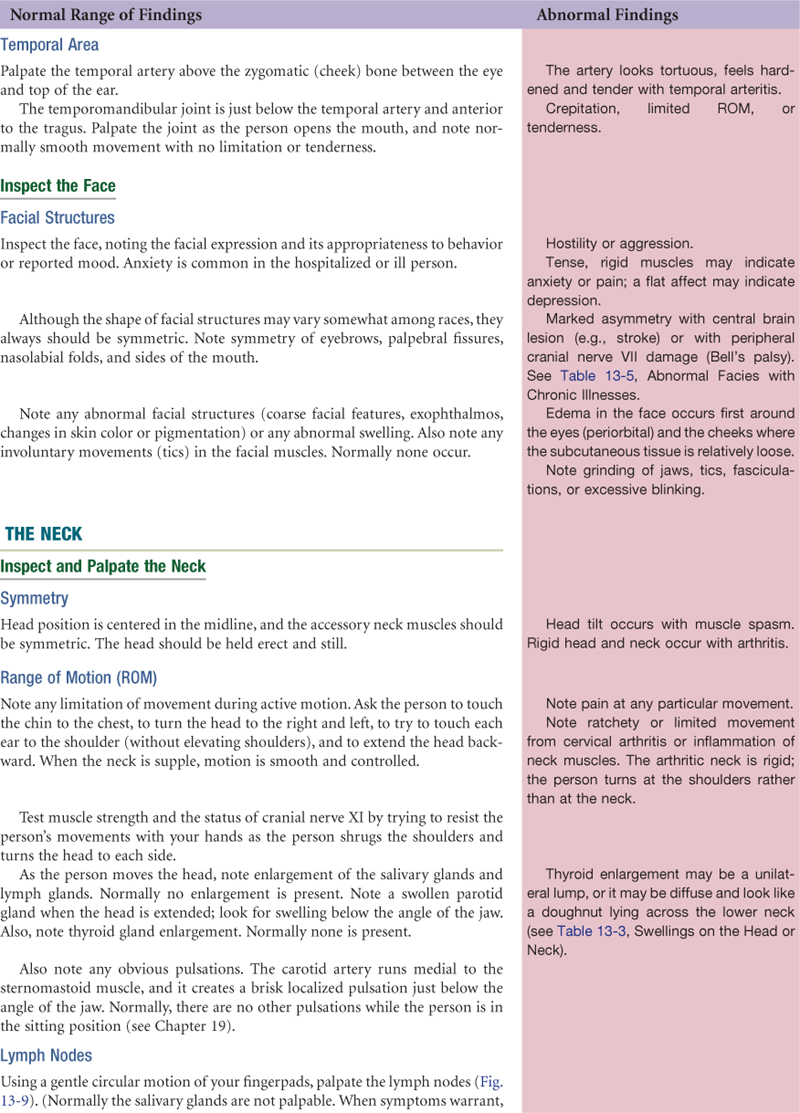
The lymphatic system is developed more fully in Chapter 20, p. 502. However, the head and neck have a rich supply of lymph nodes (Fig. 13-6). Although sources differ as to their nomenclature, one commonly used system is given here. Note that their labels correspond to adjacent structures.
• Preauricular, in front of the ear
• Posterior auricular (mastoid), superficial to the mastoid process
• Occipital, at the base of the skull
• Submental, midline, behind the tip of the mandible
• Submandibular, halfway between the angle and the tip of the mandible
• Jugulodigastric, under the angle of the mandible
• Superficial cervical, overlying the sternomastoid muscle
• Deep cervical, deep under the sternomastoid muscle
• Posterior cervical, in the posterior triangle along the edge of the trapezius muscle
• Supraclavicular, just above and behind the clavicle, at the sternomastoid muscle
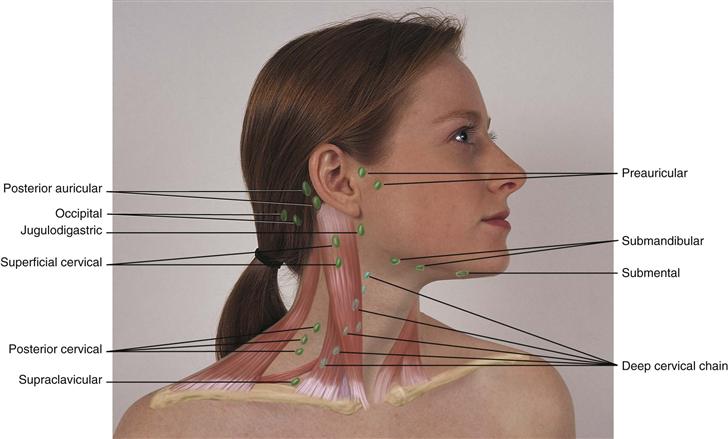
13-6
You also should be familiar with the direction of the drainage patterns of the lymph nodes (Fig. 13-7). When nodes are abnormal, check the area they drain for the source of the problem. Explore the area proximal (upstream) to the location of the abnormal node.
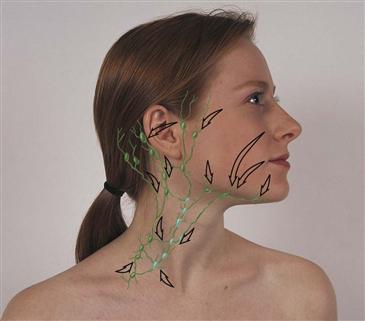
13-7
The lymphatic system is an extensive vessel system, which is separate from the cardiovascular system and is phylogenetically older. The lymphatics are a major part of the immune system, whose job it is to detect and eliminate foreign substances from the body. The vessels allow the flow of clear, watery fluid (lymph) from the tissue spaces into the circulation. Lymph nodes are small, oval clusters of lymphatic tissue that are set at intervals along the lymph vessels like beads on a string. The nodes filter the lymph and engulf pathogens, preventing potentially harmful substances from entering the circulation. Nodes are located throughout the body but are accessible to examination only in four areas: head and neck, arms, axillae, and inguinal region. The greatest supply is in the head and neck.
 Developmental competence
Developmental competence
Infants and Children
The bones of the neonatal skull are separated by sutures and by fontanels, the spaces where the sutures intersect (Fig. 13-8). These membrane-covered “soft spots” allow for growth of the brain during the 1st year. They gradually ossify; the triangle-shaped posterior fontanel is closed by 1 to 2 months, and the diamond-shaped anterior fontanel closes between 9 months and 2 years.
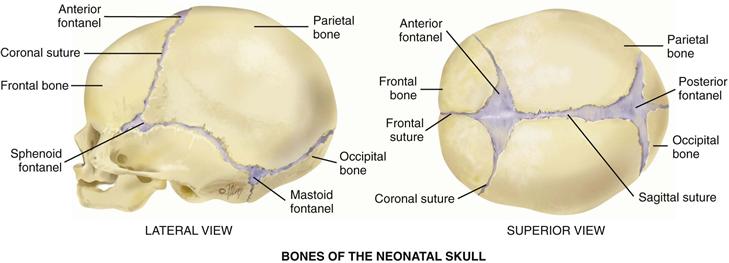
13-8 Copyright © (2006) © Pat Thomas, 2006.
During the fetal period, head growth predominates. Head size is greater than chest circumference at birth. The head size grows during childhood, reaching 90% of its final size when the child is 6 years old. But during infancy, trunk growth predominates so that head size changes in proportion to body height. Facial bones grow at varying rates, especially nasal and jaw bones. In the toddler, the mandible and maxilla are small and the nasal bridge is low, so that the whole face seems small compared with the skull.
Lymphoid tissue is well developed at birth and grows to adult size when the child is 6 years old. The child’s lymphatic tissue continues to grow rapidly until age 10 or 11 years, actually exceeding its adult size before puberty. Then the lymphatic tissue slowly atrophies.
In adolescence, facial hair appears on boys, first above the lip, then on cheeks and below the lip, and last on the chin. A noticeable enlargement of the thyroid cartilage occurs, and with it, the voice deepens.
The Pregnant Woman
The thyroid gland enlarges slightly during pregnancy as a result of hyperplasia of the tissue and increased vascularity.
The Aging Adult
The facial bones and orbits appear more prominent, and the facial skin sags as a result of decreased elasticity, decreased subcutaneous fat, and decreased moisture in the skin. The lower face may look smaller if teeth have been lost.


Objective Data

 Documentation and Critical Thinking
Documentation and Critical Thinking
Sample Charting
Subjective
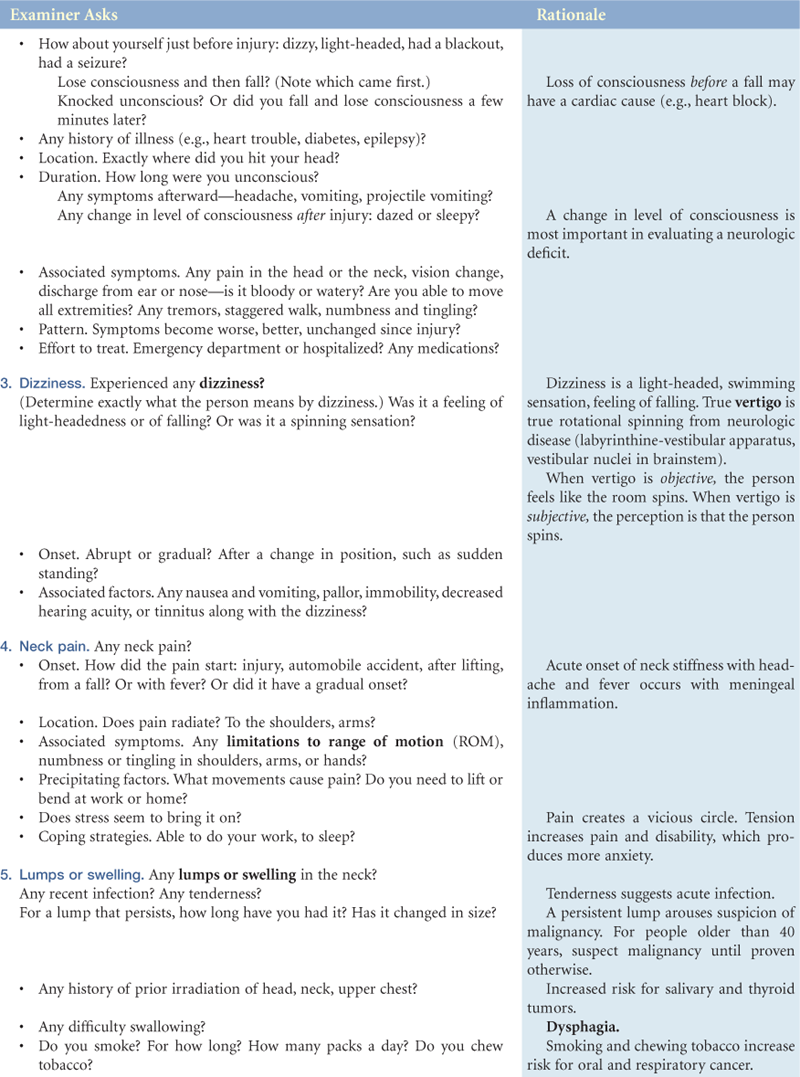
Denies any unusually frequent or severe headache; no history of head injury, dizziness, or syncope; no neck pain, limitation of motion, lumps, or swelling.
Objective
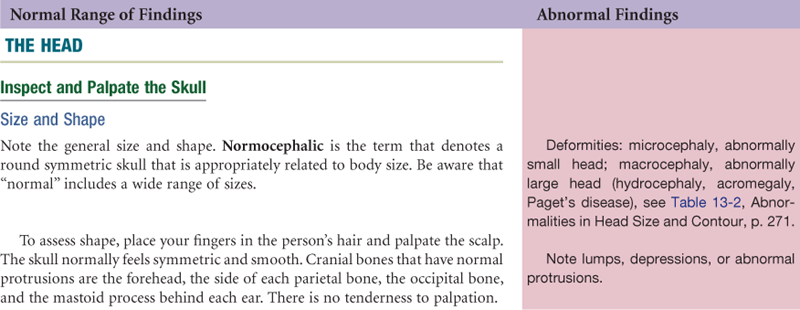
Head: Normocephalic, no lumps, no lesions, no tenderness, no trauma.
Face: Symmetric, no drooping, no weakness, no involuntary movements.
Neck: Supple with full ROM, no pain. Symmetric, no cervical lymphadenopathy or masses. Trachea midline, thyroid not palpable. No bruits.
Assessment
Normocephalic, atraumatic, and symmetric head and neck.
Focused Assessment: Clinical Case Study 1
Frank V. is a 57-year-old insurance executive who is in his fourth postoperative day after a transurethral resection of the prostate gland. He also has chronic hypertension, managed by oral hydrochlorothiazide, exercise, and a low-salt diet.
Subjective
Complaining of dizziness, a light-headed feeling that occurred on standing and cleared on sitting. No previous episodes of dizziness. Denies palpitations, nausea, or vomiting. States urine pink-tinged as it was yesterday, with no red blood. No pain meds today. On second day of same antihypertensive medication he took before surgery.
Objective
BP 142/88 RA sitting, 94/58 RA standing. Pulse 94 sitting and standing, regular rhythm, no skipped beats. Temp 37° C. Color tannish-pink, no pallor, skin warm and dry.
Neuro: Alert and oriented to person, place, and time. Speech clear and fluent. Moving all extremities, no weakness. No nystagmus, no ataxia, past pointing normal. Romberg’s sign negative (normal). Intake/output in balance. Urine faint pink-tinged, no clots.
Lab: Hct 45, serum chemistries normal.
Assessment
Orthostatic hypotension
Risk for injury R/T orthostatic hypotension
Focused Assessment: Clinical Case Study 2
Mara is a 19-year-old single white female college student with a history of good health and no chronic illnesses; she enters the outpatient clinic today looking anxious, stating, “I think I’ve had a stroke!”
Subjective
One day PTA—first noticed at dinner at college cafeteria when joking with friends, started to stick out tongue and roll tongue and could not do it, right side of tongue was not working. Mara left room to look in mirror and became scared; when smiled, noticed right side was not working. Tried to pucker lips, could not. Could not whistle, could not raise eyebrow. “I looked like a Vulcan.” No other movement disorder below neck. Mild pain behind right ear with buzzing in ear. Able to sleep last night, but roommate said Mara’s right eyelid did not close completely during sleep.
Today—still no movement on complete right side of face. Feeling self-conscious in class and during conversations with friends. Now has taste aversion, fluids with high water content taste especially bitter. No hearing loss.
Objective
T 37° C, P 64, R 14, B/P 108/78.
Forehead appears smooth and immobile on right, unable to wrinkle right side. Unable to close right eye, Bell’s phenomenon present when attempts to close (right eyeball rolls upward), right palpebral fissure appears wider. No corneal reflex on right. Unable to whistle or puff right cheek. Absent nasolabial fold on right. Mouth droops on right, sags on right when tries to smile. Slight drooling. Left side of face responds appropriately to all these movements. Superficial sensation intact.
Rest of musculoskeletal system intact: able to hold balance while standing, able to walk, walk heel-to-toe, do knee bend on each knee. Arm strength and ROM intact.
Assessment
Right-sided facial paralysis, consistent with Bell’s palsy
Disturbed body image R/T effects of loss of facial function
Risk for deficient fluid volume R/T taste aversion and dietary alteration
Risk for sensory deficit, visual impairment, R/T effects of neurologic impairment
Summary Checklist: Head, Face, and Neck, Including Regional Lymphatics Examination
 For a PDA-downloadable version, go to http://evolve.elsevier.com/Jarvis/.
For a PDA-downloadable version, go to http://evolve.elsevier.com/Jarvis/.
Bibliography
1. Buse DC, Rupnow MFT, Lipton RB. Assessing and managing all aspects of migraine: migraine attacks, migraine-related functional impairment, common comorbidities, and quality of life. Mayo Clinic Proceedings. 2009;84(5):422–435.
2. Chan Y. Differential diagnosis of dizziness. Current Opinion in Otolaryngology & Head and Neck Surgery. 2009;17(3):200–203.
3. Chen LY, Benditt DG, Shen W. Management of syncope in adults: an update. Mayo Clinic Proceedings. 2008;83(11):1280–1293.
4. Davenport R. The bare essentials: headache. Practical Neurology. 2008;8(5):335–343.
5. Fleener V, Holloway B. Migraines: not just an adult problem. The Nurse Practitioner. 2004;29(11):27–40.
6. Foley AL. The “Grand Slam” triage assessment. Journal of Emergency Nursing. 2009;35(1):76–77.
7. Gladstein J. Controlling pain: understanding headache pain in children. Nursing. 2009;39(7):57–58.
8. Joslin N. Early identification key to scleroderma treatment. The Nurse Practitioner. 2004;29(7):24–41.
8a. Kapustin JF. Hypothyroidism: an evidence-based approach to a complex disorder. The Nurse Practitioner. August 2010;35(8):45–53.
9. Koch J, Alverson E. Lymphadenopathy: a case study in clinical decision-making. The American Journal for Nurse Practitioners. 2003;7(4):21–32.
10. Lipton RB. Tracing transformation: chronic migraine classification, progression, and epidemiology. Neurology. 2009;72(Suppl. 5):S3–S7.
11. Lipton RB, Bigal ME, Steiner TJ, et al. Classification of primary headaches. Neurology. 2004;63(3):427–435.
12. Mistry N, Wass J, Turner MR. When to consider thyroid dysfunction in the neurology clinic. Practical Neurology. 2009;9(3):145–156.
13. Morris PS. Upper respiratory tract infections (including otitis media). Pediatric Clinics of North America. 2009;56(1):101–117.
13a. National Stroke Association. What is Stroke? Retrieved December 10, 2009, from www.stroke.org/site/PageServer?pagename=STROKE; 2009.
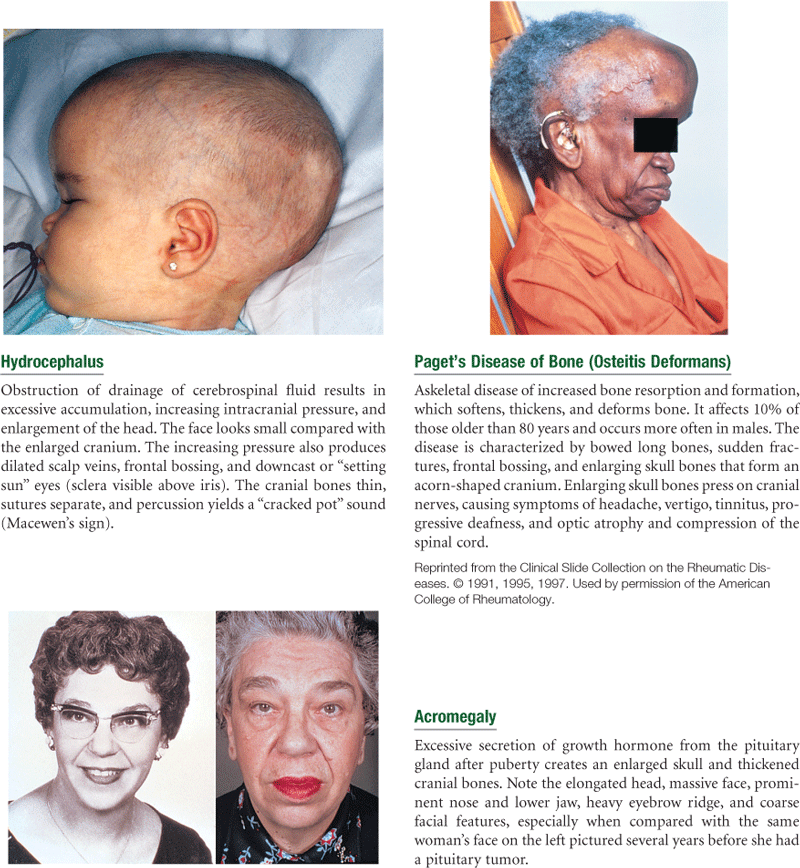
14. Roodman G. Recent developments in Paget’s disease. Advanced Studies in Medicine. 2003;3(5):286–292.
15. Tan MP, Parry SW. Vasovagal syncope in the older patient. Journal of the American College of Cardiology. 2008;51:599–606.
16. Tepper SJ, Zatochill M, Szeto M, Sheftell F, Tepper DE, Bigal M. Development of a simple menstrual migraine screening tool for obstetric and gynecology clinics: the menstrual migraine assessment tool. Headache. 2008;48(10):1419–1425.
17. Thyroid troubles: subtle symptoms with age. Mayo Clinic Health Letter. 2008;26(5):4–5.
18. Uneri A, Polat S. Vertigo, dizziness, and imbalance in the elderly. The Journal of Laryngology and Otology. 2007;122(5):466–469.
19. Weeks B. Graves’ disease: the importance of early diagnosis. The Nurse Practitioner. 2005;30(11):34–47.