CHAPTER 32 Electromyographic Activity During Upper Extremity Sports
Electromyography (EMG) is the science of quantifying muscle activity. Understanding when and how much the shoulder muscles are active during upper extremity sports is helpful to physicians, physical therapists, athletic trainers, and coaches in providing appropriate treatment, training, and rehabilitation protocols to these athletes, as well as helping us to better understand the injury mechanism. EMG data do not always correlate well with muscle force, especially as muscle contraction velocities increase. Nevertheless, EMG is helpful in determining the timing and amount of muscle activation throughout a given movement.
The focus of this chapter is on shoulder muscle activity during upper extremity sports. Most of the shoulder movements in the sports discussed here involve overhead throwing–type movements, which are commonly associated with shoulder injuries. Shoulder EMG data are far more extensive for overhead throwing activities, such as baseball pitching and football passing, and therefore much of this chapter focuses on shoulder EMG during activities that involve the overhead throwing motion. Where appropriate and available, shoulder muscle activity is integrated with shoulder joint kinematics (linear and angular shoulder displacements, velocities, and accelerations) and kinetics (shoulder forces and torques) to help better understand why certain muscles are active during different phases of an activity, and the type of muscle action (eccentric or concentric) that occurs. Also, when EMG is integrated with shoulder kinematics and kinetics, it provides insight into the injury mechanism. For a review of shoulder kinetics and kinematics in upper extremity sports, the reader should refer to Chapter 31.
OVERHEAD BASEBALL PITCH
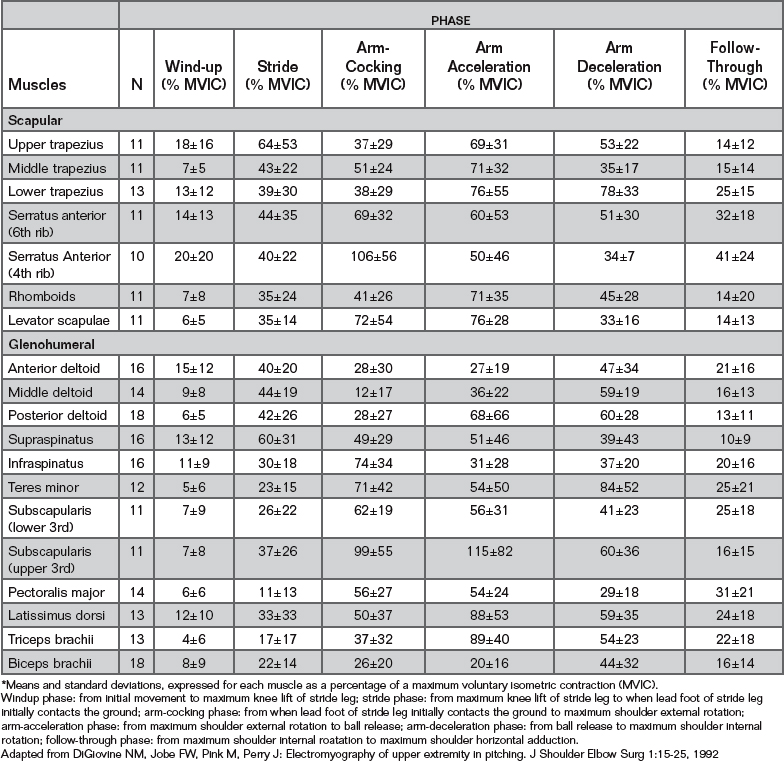
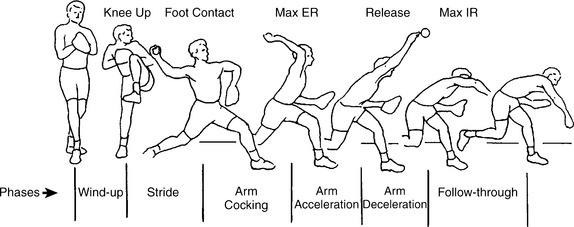
Shoulder muscle activity during baseball pitching has been studied extensively by Jobe and others.1-5 Using 56 healthy male college and professional baseball pitchers, DiGiovine and colleagues1 quantified shoulder muscle activity during baseball pitching, and these EMG data are summarized in Table 32-1. To help generalize phase comparisons in muscle activity from Table 32-1, 0% to 20% of a maximum voluntary isometric contraction (MVIC) is considered low muscle activity, 21% to 40% MVIC is considered moderate muscle activity, 41% to 60% MVIC is considered high muscle activity, and greater than 60% MVIC is considered very high muscle activity.1 From these initial reports, the baseball pitch was divided into several phases, which later were slightly modified by Escamilla and colleagues6 and Fleisig and colleagues7 as wind-up, stride, arm cocking, arm acceleration, arm deceleration, and follow-through (Fig. 32-1).
Wind-up Phase
Shoulder activity during the wind-up phase, which is from initial movement to maximum knee lift of the stride leg, is generally very low due to the slow movements that occur. As shown in Table 32-1, the greatest activity is from the upper trapezius, serratus anterior, and anterior deltoids, which all contract concentrically to upwardly rotate and elevate the scapula and abduct the shoulder as the arm is initially brought overhead, and then contract eccentrically to control downward scapular rotation and shoulder adduction as the hands are lowered to approximately chest level. The muscles of the rotator cuff, which have a dual function as glenohumeral joint compressors and rotators, have their lowest activity during this phase. Low shoulder activity is not surprising given that the shoulder forces and torques generated during this phase are also low.6,7
Stride Phase
There is a dramatic increase in shoulder activity during the stride phase (see Table 32-1), which is from the end of the balance phase to when the lead foot of the stride leg initially contacts the ground. During the stride the hands separate; the scapula upwardly rotates, elevates, and retracts; and the shoulders abduct, externally rotate, and horizontally abduct due to concentric activity from several muscles, including the deltoids, supraspinatus, infraspinatus, serratus anterior, and upper trapezius. It is not surprising that many more muscles are activated and to a higher degree during the stride compared with the wind-up. Interestingly, the supraspinatus has its highest activity during the stride as it works not only to abduct the shoulder but also to help compress and stabilize the glenohumeral joint. The deltoids also exhibit high activity to initiate and maintain the shoulder in an abducted position.
Arm-Cocking Phase
The arm-cocking phase begins at lead foot contact and ends at maximum shoulder external rotation. During this phase the kinetic energy that is generated from the larger lower extremity and trunk segments is transferred up the body to the smaller upper extremity segments. The pitching arm lags behind as the trunk rapidly rotates forward to face the hitter, generating a peak pelvis angular velocity around 600 deg/sec, occurring 0.03 to 0.05 sec after lead foot contact, followed by a peak upper torso angular velocity of nearly 1200 deg/sec, occurring 0.05 to 0.07 sec after lead foot contact.8 Consequently, high to very high shoulder muscle activity is needed during this phase to keep the arm moving with the rotating trunk as well as to control the resulting shoulder external rotation (see Table 32-1), which peaks near 180 degrees.8 Moderate activity is needed by the deltoids (see Table 32-1) to maintain the shoulder at approximately 90 degrees of abduction throughout the phase.8
Activity from the pectoralis major and anterior deltoid is needed during this phase to horizontally adduct the shoulder to a peak angular velocity of approximately 600 deg/sec, from a position of approximately 20 degrees of horizontal abduction at lead foot contact to a position of approximately 20 degrees of horizontal adduction at maximum shoulder external rotation.8 Moreover, a large compressive force of approximately 80% of body weight is generated by the trunk onto the upper extremity (UE) at the shoulder to resist the large centrifugal force that is generated as the arm rotates forward with the trunk.7 The rotator cuff muscles (supraspinatus, infraspinatus, teres minor, and subscapularis) achieve high to very high activity to resist glenohumeral distraction and enhance glenohumeral stability. The posterior cuff muscles (infraspinatus and teres minor) and latissimus dorsi also generate a posterior force to the humeral head, which helps resist anterior humeral head translation and perhaps helps unload the anterior capsule and anterior band of the inferior glenohumeral ligament. Although it is widely accepted that strength and endurance in the posterior musculature are very important during the arm-deceleration phase to slow down the UE, they are also important during the arm-cocking phase.
During the arm-cocking phase a peak shoulder internal rotation torque of 65 to 70 N•m is generated near the time of maximum shoulder external rotation, which implies that shoulder external rotation is progressively slowing down as maximum shoulder external rotation is approached.7,9 High to very high activity is generated by the shoulder internal rotators (pectoralis major, latissimus dorsi, and subscapularis), which contract eccentrically during this phase to control the rate of shoulder external rotation.
The multiple functions of muscles are clearly illustrated during arm cocking. For example, the pectoralis major contracts concentrically to horizontally adduct the shoulder and eccentrically to control shoulder external rotation. This dual function helps this muscle maintain an appropriate length-tension relationship by simultaneously shortening and lengthening, which implies that this muscle might not be changing length much throughout this phase but rather maintaining a more constant length and in effect contracting isometrically. Another example is the subscapularis, which contracts concentrically to aid in horizontal adduction, eccentrically to help control external rotation, and may also contract isometrically to help resist glenohumeral joint distraction.
The importance of scapular muscles during arm cocking is demonstrated in Table 32-1. High activity from these muscles is needed to stabilize the scapula and properly position the scapula in relation to the horizontally adducting and rotating humerus. The scapular protractors are especially important during this phase in order to resist scapular retraction by contracting eccentrically and isometrically during the early part of this phase, and contracting concentrically during the latter part of this phase to protract the scapula. The serratus anterior generates maximum activity during this phase.
Because both the triceps brachii (long head) and biceps brachii (both heads) cross the shoulder, they both generate moderate activity during this phase to provide additional stabilization to the shoulder. In contrast to the triceps EMG reported by DiGiovine,1 which reported only moderate activity during this phase and much higher activity during the arm-acceleration phase, Werner and colleagues10 reported the highest triceps EMG during the arm-cocking phase and relatively little triceps EMG during the arm-acceleration phase. Because elbow extensor torque peaks during this phase,10,11 high eccentric contractions by the triceps brachii are needed to help control the rate of elbow flexion that occurs throughout the initial 80% of this phase.8 High triceps activity is also needed to initiate and accelerate elbow extension, which occurs during the final 20% of this phase as the shoulder continues externally rotating.8 Therefore, during arm cocking, the triceps initially contracts eccentrically to control elbow flexion early in the phase and contracts concentrically to initiate elbow extension later in the phase.
Gowan and colleagues3 demonstrated that subscapularis activity is nearly twice as great in professional baseball pitchers compared with amateur pitchers during this phase. In contrast, muscle activity from the pectoralis major, supraspinatus, serratus anterior, and biceps brachii was approximately 50% greater in amateur pitchers compared with professional pitchers. From these data it can be concluded that better throwing efficiency by professional pitchers might require less muscle activity compared with amateurs.
Glousman and colleagues2 compared shoulder muscle activity between pitchers with chronic anterior shoulder instability due to anterior glenoid labral tears with healthy pitchers with no shoulder pathology. Pitchers with chronic anterior instability exhibited greater muscle activity from the biceps brachii and supraspinatus and less muscle activity from the pectoralis major, subscapularis, and serratus anterior. Chronic anterior instability results in excessive stretch of the anterior capsular, which can stimulate mechanoreceptors within the capsule, resulting in excitation in the biceps brachii and supraspinatus and inhibition in the pectoralis major, subscapularis, and serratus anterior. Increased activity from the biceps brachii and supraspinatus helps compensate for anterior shoulder instability because these muscles enhance glenohumeral stability. Decreased activity from the pectoralis major and subscapularis, which contract eccentrically to decelerate the externally rotating shoulder, can accentuate shoulder external rotation and further increase stress on the anterior capsule. Decreased activity from the serratus anterior can cause the scapula to be abnormally positioned relative to the externally rotating and horizontally adducting humerus. A deficiency in scapular upward rotation can decrease the subacromial space and increase the risks of impingement and rotator cuff pathology.
Interestingly, infraspinatus activity was less in pitchers with chronic anterior shoulder instability compared with healthy pitchers. During arm cocking, the infraspinatus not only helps externally rotate and compress the glenohumeral joint but also helps generate a small posterior force on the humeral head due to a slight posterior orientation of its fibers as they run from the inferior facet of the greater tubercle to the infraspinous fossa. This posterior force on the humeral head helps resist anterior humeral head translation and unloads strain on the anterior capsule during arm cocking.
Arm-Acceleration Phase
The arm acceleration phase only lasts 0.03 to 0.05 sec. It begins at maximum shoulder external rotation and ends at ball release. Like the arm-cocking phase, high to very high activity is generated from the glenohumeral and scapular muscles during this phase in order to accelerate the arm forward (see Table 32-1).
Although DiGiovine and colleagues1 reported that the triceps had its highest activity during this phase,1 Werner and colleagues10 reported relatively little triceps EMG during the arm-acceleration phase. In addition, elbow extensor torque is very low during this phase compared with the arm-cocking phase.10,11 Elbow extension initially begins during the arm-cocking phase.6 Kinetic energy that is transferred from the lower extremities and trunk to the arm is used to help generate a peak elbow extension angular velocity of approximately 2300 deg/sec during this phase.6 In fact, a concentric contraction from the triceps brachii alone could not come close to generating this 2300 deg/sec elbow extension angular velocity. This observation is supported by findings by Dobbins and reported by Roberts,12 who had found that subjects who threw with paralyzed triceps muscles could obtain ball velocities greater than 80% of the ball velocities obtained before the triceps were paralyzed.
This observation is further supported by Toyoshima and colleagues,13 who demonstrated that normal throwing using the entire body generated almost twice the elbow extension angular velocity compared with extending the elbow by throwing without lower extremity, trunk, and shoulder movements. These authors concluded that during normal throwing, the elbow is swung open like a whip, primarily due to linear and rotary contributions from the lower extremity, trunk, and shoulder and, to a lesser extent, a concentric contraction of the triceps. Nevertheless, the triceps help extend the elbow during this phase, as well as contributing to shoulder stabilization by the triceps long head.
Moderate activity is generated by the deltoids1 to help produce a fairly constant shoulder abduction of approximately 90 to 100 degrees,8 which is maintained regardless of throwing style (e.g., overhand, sidearm). The glenohumeral internal rotators (subscapularis, pectoralis major, and latissimus dorsi) have their highest activity during this phase1 as they contract concentrically to generate a peak internal rotation angular velocity of approximately 6500 deg/sec near ball release.6 With these rapid arm movements, which are generated to accelerate the arm forward, it is not surprising that the scapular muscles also generate high activity,1 to help maintain proper position of the glenoid relative to the rapidly moving humeral head. Strengthening the scapular musculature is very important. Poor position and movement of the scapula can increase the risk of impingement and other related injuries, as well as reducing the optimal length-tension relationship of both scapular and glenohumeral musculature.
Gowan and colleagues demonstrated that rotator cuff and biceps brachii activity were 2 to 3 times higher in amateur pitchers compared with professional pitchers during this phase.3 In contrast, subscapularis, serratus anterior, and latissimus dorsi activity was much greater in professional pitchers. These results imply that professional pitchers better coordinate their body segment movements to increase throwing efficiency. Enhanced throwing mechanics and efficiency can minimize glenohumeral instability during this phase. This may help explain why professional pitchers generate less activity from the rotator cuff and biceps muscles which help compress the glenohumeral joint and enhance stability.
Compared with healthy pitchers, pitchers with chronic anterior shoulder instability due to anterior labral injuries exhibit greater muscle activity from the biceps brachii, supraspinatus, and infraspinatus and less muscle activity from the latissimus dorsi, subscapularis, and serratus anterior.2 The increased activity from rotator cuff and biceps musculature in pitchers with chronic anterior instability is needed to provide additional glenohumeral stability that is lacking in these pitchers due to a compromised anterior labrum.
With shoulder internal rotation, the long biceps tendon is repositioned anteriorly at the shoulder, providing compressive and posterior forces to the humeral head, which enhance anterior stability. Therefore, throwers with chronic anterior instability activate their biceps to a greater extent (32% vs 12% MVIC), as well as their supraspinatus and infraspinatus (37% vs 13% MVIC), compared with asymptomatic throwers.2 However, increased and excessive biceps activity due to anterior instability results in increased stress to the long biceps anchor at the superior labrum, which over time can result in pathology of the superior labrum anterior to posterior in direction (SLAP [superior anterior-posterior] lesions). In addition, chronic anterior shoulder instability inhibits normal contributions from the internal rotators and serratus anterior, which can adversely affect throwing mechanics and efficiency and increase injury risks at the shoulder.
Arm-Deceleration Phase
The arm deceleration phase lasts 0.03 to 0.05 sec. It begins at ball release and ends at maximum shoulder internal rotation. Large loads are generated at the shoulders to slow the forward acceleration of the arm. Posterior shoulder musculature, such as the infraspinatus, teres minor and major, posterior deltoid, and latissimus dorsi, contract eccentrically not only to decelerate horizontal adduction and internal rotation of the UE but also help resist shoulder distraction and anterior subluxation forces. A shoulder compressive force slightly greater than body weight is needed to resist shoulder distraction, and a posterior shear force between 40% and 50% of body weight is generated to resist shoulder anterior subluxation.6,7 Therefore, high activity is generated by posterior shoulder musculature,1 in particular the rotator cuff muscles. In addition, scapular muscles also exhibit high activity to control scapular elevation, protraction, and rotation during this phase. For example, the lower trapezius, which generates a force on the scapula in the direction of depression, retraction, and upward rotation, generates its highest activity during this phase (see Table 32-1). High EMG activity from glenohumeral and scapular musculature illustrates the importance of strength and endurance training of the posterior musculature in the overhead-throwing athlete. Weak or fatigued posterior musculature can lead to multiple injuries, such as tensile overload undersurface cuff tears, labral and biceps pathology, capsule injuries, and internal impingement of the infraspinatus and supraspinatus tendons on the posterosuperior glenoid labrum.7
Compared with healthy pitchers, pitchers with chronic anterior shoulder instability exhibited less muscle activity from the pectoralis major, latissimus dorsi, subscapularis, and serratus anterior, which is similar to what occurred in the arm-cocking and acceleration phases.2 However, muscle activity from the rotator cuff and biceps brachii are similar between healthy pitchers and pitchers with chronic anterior shoulder instability during this phase, which is in contrast to the greater rotator cuff and biceps brachii activity demonstrated in pitchers with chronic anterior shoulder instability during the arm-cocking and acceleration phases.2 This difference in muscle activity may be partially explained by the very high compressive forces that are needed during arm deceleration to resist shoulder distraction, which is a primary function of the rotator cuff and to a lesser extent the biceps brachii.
The biceps brachii generate their highest activity during arm deceleration (see Table 32-1). The function of this muscle during this phase to twofold. First, it must contract eccentrically along with other elbow flexors to help decelerate the rapid elbow extension that peaks during arm acceleration. This is an important function because weakness or fatigue in the elbow flexors can result in elbow extension being decelerated by impingement of the olecranon in the olecranon fossa, which can lead to bone spurs and subsequent loose bodies within the elbow. Second, the biceps brachii works synergistically with the rotator cuff muscles to resist distraction and anterior subluxation at the glenohumeral joint. Interestingly, during arm deceleration biceps brachii activity is greater in amateur pitchers compared with professional pitchers,3 which may imply that amateur pitchers employ a less-efficient throwing pattern compared with professional pitchers. Excessive activity from the long head of the biceps brachii can lead to labral pathology.
OVERHEAD FOOTBALL THROW:
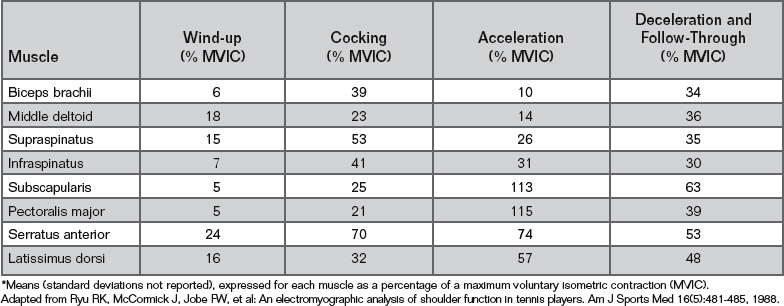
Only one known study has quantified muscle activity during the football throw.14 Using 14 male recreational and college athletes, these authors quantified activity from nine glenohumeral muscles throughout throwing phases specific for football, and their results are summarized in Table 32-2. The defined phases for football throwing are similar but slightly different than the defined phases for baseball pitching (see Table 32-1). Early arm cocking in the football throw was similar to the stride phase in baseball, and late cocking in the football throw was the same as arm cocking in baseball. The acceleration phase was the same for both the football throw and the baseball pitch. The arm deceleration and follow-through phases in the baseball pitch were combined into a single arm-deceleration and follow-through phase in the football throw.
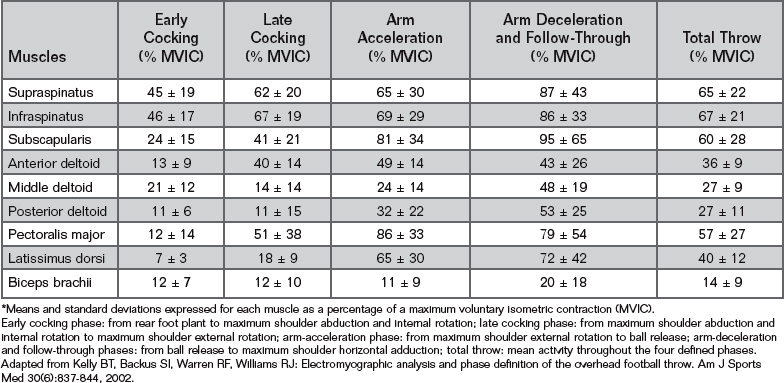
Rotator cuff activity progressively increased in each phase of football throwing, being least in the early cocking phase and peaking in the arm-deceleration and follow-through phases. This is a different pattern than the baseball pitch, where rotator cuff activity was generally greatest during either the arm-cocking phase or the arm-deceleration phase. For baseball pitching and football throwing, deltoid and biceps brachii activity were generally greatest during the arm-deceleration phase. The pectoralis major and latissimus dorsi had their greatest activity during arm-cocking and arm-acceleration in baseball pitching, whereas peak activity occurred in these muscles during arm acceleration and arm deceleration in football throwing. The greatest activity occurred in the rotator cuff muscles, pectoralis major, and latissimus dorsi during the arm-deceleration and follow-through phases of the football throw. These muscles all work to generate a shoulder-compressive force during this phase to resist shoulder distraction. In fact, the greatest force generated during the football throw is a shoulder-compressive force that occurs during arm deceleration with a magnitude of approximately 80% body weight.15
The different muscle activity patterns between baseball pitching and football throwing are largely because a football weighs three times greater than a baseball. Although there are several kinematic and kinetic similarities between football throwing and baseball pitching, there are also several differences.15 Compared with throwing a football, throwing a baseball produces significantly greater trunk, shoulder, and elbow angular velocities during the arm-cocking and arm-acceleration phases, which lead to significantly greater shoulder forces and torques generated in baseball pitching, especially during the arm-deceleration phase, in order to slow down the rapidly moving arm.15
WINDMILL SOFTBALL PITCHING
Maffet and colleagues conducted the only known study that quantified shoulder muscle firing patterns during the softball pitch.16 These authors used 10 female collegiate softball pitchers who all threw the fast pitch and quantified muscle activity in the anterior and posterior deltoid, supraspinatus, infraspinatus, teres minor, subscapularis, pectoralis major, and serratus anterior.
The fast-pitch motion starts with the throwing shoulder extended, and then as the pitcher strides forward the arm fully flexes, abducts, and externally rotates, and then continues in a circular (windmill) motion all the way around until the ball is released near 0 degrees shoulder flexion and adduction. The six phases that define the pitch are as follows: wind-up, from first ball motion to 6-o’clock position (shoulder flexed and abducted approximately 0 degrees); from 6-o’clock position to 3-o’clock position (shoulder flexed approximately 90 degrees); from 3-o’clock position to 12-o’clock position (shoulder flexed and abducted approximately 180 degrees); from 12-o’clock position to 9-o’clock position (shoulder abducted approximately 90 degrees); from 9-o’clock position to ball release; and from ball release to completion of the pitch.
The total circumduction of the arm about the shoulder from the wind-up to the follow-through are approximately 450 to 500 degrees.17 This circumduction occurs while holding a 6.25- to 7-oz ball and with the elbow near full extension, which accentuates the centrifugal distractive force acting at the shoulder.
EMG results by muscle and phase during the softball pitch are shown in Table 32-3. Muscle activity was generally lowest during the wind-up and was increased during the 6-o’clock to 3-o’clock phase as the arm begins accelerating upward. Both the supraspinatus and infraspinatus generated their highest activity during this phase. During the 6-o’clock to 3-o’clock phase, the arm accelerates in a circular motion and achieves a peak shoulder flexion angular velocity of approximately 5000 deg/sec.17 The anterior deltoid was moderately active to help generate this rapid shoulder flexion angular velocity, and the serratus anterior was moderately active in helping to upwardly rotate and protract the scapula. The arm rapidly rotating upward in a circular pattern results in a distractive force of approximately 20% to 40% of body weight, which is resisted in part by the shoulder-compressive action of the supraspinatus and infraspinatus.
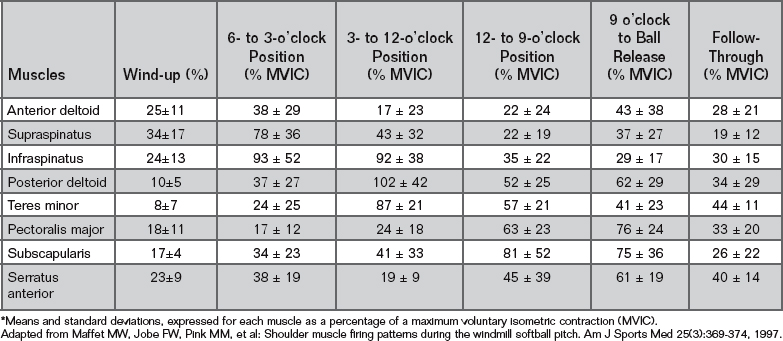
As the arm continues its upward acceleration during the 3-o’clock to 12-o’clock phase, the posterior deltoid, teres minor, and infraspinatus all achieve their peak activity. These muscles not only help externally rotate the shoulder during this phase but also help compress the glenohumeral joint and resist the progressively increasing shoulder-distractive forces, which are approximately 50% of body weight during this phase.17 These muscles are also in good position to resist shoulder-lateral forces, which peak during this phase.17
The arm begins accelerating downward during the 12-o’clock to 9-o’clock phase. It is during this phase that the shoulder begins to rapidly internally rotate 2000 to 3000 deg/sec.17 It is not surprising that the internal rotators (subscapularis and pectoralis major) exhibit high activity during this phase. High activity from the pectoralis major also helps adduct the shoulder during this phase. The subscapularis also helps stabilize the humeral head and can help unload anterior capsule stress caused by the overhead and backward position of the arm as it begins accelerating forward. The serratus anterior exhibited a marked increase in activity to help stabilize the scapula and properly position the glenoid with the rapidly moving humerus.
The subscapularis, pectoralis major, and serratus anterior collectively generat their highest activity during the 9-o’clock to ball release phase. The serratus anterior continues to work to stabilize the scapula and properly position it in relation to the rapidly moving humerus. High subscapularis and pectoralis major activity is needed during this phase to resist distraction at the shoulder, which peaks during this phase with a magnitude of approximately body weight.17,18 These muscles also help generate a peak shoulder internal rotation of approximately 4600 deg/sec17 and help adduct and flex the UE until the UE contacts the lateral thigh.
Not all softball pitchers exhibit the same pattern of motion during this phase, because none of the 53 youth softball pitchers studies by Werner and colleagues18 adopted the release strategy of contacting the lateral thigh at ball release. This might partially explain why the collegiate pitchers in the study by Maffet and colleagues16 generated relatively low posterior cuff activity and relatively low activity in general during the follow-through. With contact of the arm with the lateral thigh near ball release, the deceleration forces and torques generated by muscles to slow down the arm are much less compared with no contact of the arm with the lateral thigh. In the case of no arm contact with the lateral thigh, shoulder-compressive and related forces and torques may be higher during follow-through, and relatively high shoulder forces and torques have been reported.17,18 However, these forces and torques are less during follow-through compared with those for the 9-o’clock–to–ball release acceleration phase. This is one major difference between overhand throwing and the windmill motion. In overhead throwing, the deceleration phase after ball release generates greater shoulder forces and torques compared with the acceleration phase up to ball release of the windmill motion. In softball pitching, the greatest forces and torques occur during the acceleration phase of the delivery.
The rapid shoulder movements and high shoulder forces that are generated during the windmill fast pitch make the shoulder susceptible to injury. There is also a higher risk of subacromial impingement due to the extreme shoulder flexion and abduction that occurs during the pitch. A significant number of shoulder injuries have been reported in softball pitchers, including bicipital and rotator cuff tendinitis, muscle strain, and impingement.19
VOLLEYBALL SERVE AND SPIKE
The volleyball serve and spike involve an overhead throwing motion that is similar to baseball pitching and football throwing. Unlike baseball pitching and football passing, there are no known studies that have quantified the shoulder forces and torques that are generated during the volleyball serve and spike. Nevertheless, because the motion is overhead and extremely rapid, similar to baseball pitching, it is hypothesized that high shoulder forces and torques are generated, especially during the volleyball spike. To support this hypothesis, numerous injuries occur each year in volleyball, primarily involving muscle, tendon, and ligament injuries during blocking and spiking.20 It has been reported that approximately one quarter of all volleyball injuries involve the shoulder.20-23 Moreover, in athletes who engage in vigorous upper-arm activities, shoulder pain ranks highest in volleyball players, which is largely due to the repetitive nature of the hitting motion.20-23 Therefore, understanding muscle-firing patterns of the shoulder complex is helpful in developing muscle-specific treatment and training protocols, which may minimize injury and enhance performance.
No known studies have quantified muscle activity from the scapular muscles during the volleyball serve or spike. This is surprising given the importance of the scapular muscles in maintaining proper position of the scapula with the humerus. Volleyball players with shoulder pain often have muscle imbalances of the scapular muscles.24 The firing pattern of the scapular muscles during the volleyball serve and spike should be the focus of future research studies.
Rokito and colleagues conducted the only known study that quantified muscle-firing patterns of glenohumeral muscles during the volleyball serve and spike.25 These authors used 15 female college and professional volleyball players, who all performed the volleyball serve and spike. The shoulder muscles quantified included the anterior deltoid, supraspinatus, infraspinatus, teres minor, subscapularis, teres major, latissimus dorsi, and pectoralis major. The serve and spike motions were divided into five phases, which collectively are 1.95 sec for the serve25 and 1.11 sec for the spike:25 wind-up, cocking, acceleration, deceleration, and follow-through. The wind-up accounts for 39% of total serve time and 33% of total spike time. It begins with the shoulder abducted and extended and ends with the initiation of shoulder external rotation. Cocking accounts for 20% of total serve time and 23% of total spike time and begins with initiation of shoulder external rotation and ends with maximum shoulder external rotation. Acceleration accounts for 6% of total serve time and 8% of total spike time and comprises maximum shoulder external rotation to ball impact. Deceleration accounts for 8% of total serve time and 9% of total spike time and lasts from ball impact to when the upper arm is perpendicular to the trunk. Follow-through accounts for 28% of total serve time and 27% of total spike time and lasts from when the upper arm is perpendicular to the trunk to the end of arm motion.
Shoulder EMG results by muscle and phase during the volleyball serve and spike are shown in Table 32-4. Similar to other overhead throwing activities, muscle activity during the serve were relatively low during the wind-up and follow-through phases. However, during the wind-up phase of the spike, peak activity was recorded in the anterior deltoid, infraspinatus, and supraspinatus. These muscles are important to help rapidly elevate the arm overhead (anterior deltoid and supraspinatus) and initiate external rotation (infraspinatus). The rotator cuff muscles are also active to help stabilize the humeral head in the glenoid fossa.
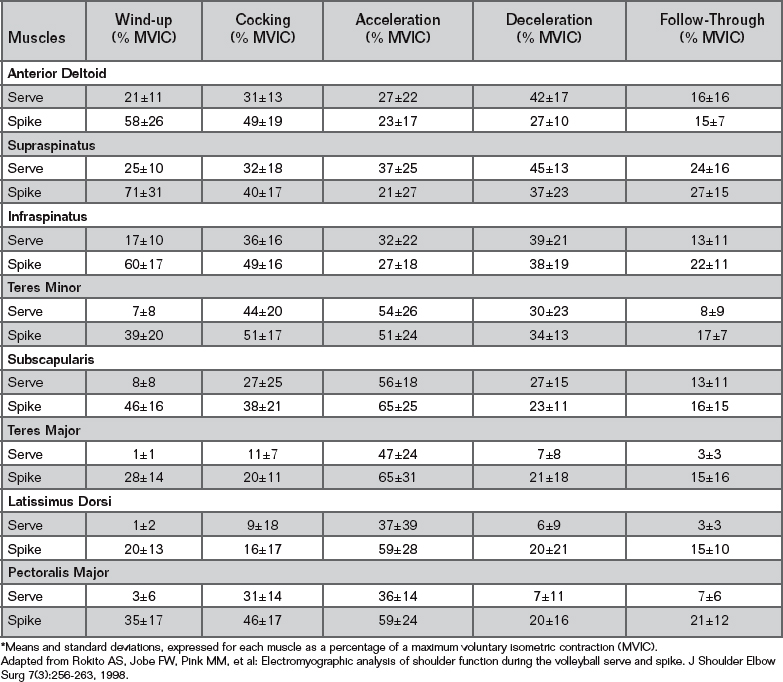
During the cocking phase, the shoulder rapidly externally rotates, which helps explain the high activity in the infraspinatus and teres minor during the serve and spike. As in baseball pitching, these muscles also produce a posterior force on the humerus that might help unload the anterior capsule as the humeral head attempts to translate anteriorly while the shoulder externally rotates. Also, the rotator cuff muscles have high activity to generate glenohumeral compression and resist distraction. The relatively high activity from the subscapularis and pectoralis major help provide support to the anterior shoulder (without such support anterior instability can ensue), as these muscles also contract eccentrically to slow down and control the rate of the rapid shoulder external rotation.
An important distinction between the serve and spike occurs during the acceleration phase. During the serve, the objective is not to impart maximum velocity to the ball but rather to hit the ball so it floats over the net with a parabolic trajectory in an area that would be most difficult for the opponent to return. In contrast, during the spike the objective typically is to hit the ball as hard as possible so as to impart maximum velocity. Consequently, muscle activity is higher in the powerful acceleratory muscles during the spike compared with the serve. Because overhead throwing motions such as baseball pitching, football passing, and the tennis serve achieve shoulder internal rotation angular velocities between 4000 and 7000 deg/sec,6,15,26 it is reasonable to assume that similar internal rotation angular velocities occur during the volleyball spike. The shoulder internal rotators (teres major, subscapularis, pectoralis major, and latissimus dorsi) all generated their highest activity for both the serve and the spike in order to both internally rotate the shoulder and accelerate the arm forward.
During the acceleration phase, teres minor activity peaks to provide a stabilizing posterior restraint to anterior translation. In contrast, infraspinatus activity is relatively low. The differing amounts of EMG activity between the teres minor and infraspinatus throughout the different phases of the serve and spike are interesting to note, especially because the teres minor and infraspinatus provide similar glenohumeral functions and they are located adjacent to each other anatomically. However, the spatial orientations of these two muscles are different: The teres minor is in a better mechanical position to extend the shoulder in a sagittal plane and the infraspinatus is in a better mechanical position to extend the shoulder in a transverse plane. There are also clinical differences between these two muscles; they are typically not injured together, but rather one or the other is injured.1,25 This different clinical observation between the teres minor and infraspinatus is consistent with the different muscle-firing patterns that occur within any given phase of overhead throwing, such as what also occurs during baseball pitching (see Table 32-1).1
During the deceleration phase, infraspinatus and supraspinatus activity is greatest during the serve but not during the spike. In fact, rotator cuff activity is generally lower in the spike compared with the serve, which may be counterintuitive. For example, because a primary function of the rotator cuff is to generate shoulder-compressive force to resist shoulder distraction, and because shoulder-compressive forces from similar overhead throwing motions (such as baseball pitching and football passing) generate large shoulder-compressive forces during this phase,6,15 it is plausible to assume that large compressive forces are also needed during the spike. The relatively low activity from the rotator cuff muscles during the spike is a different pattern compared with the moderate to high rotator cuff activity generated during the baseball pitch and football pass (see Tables 32-1 and 32-2). The higher rotator cuff activity during baseball pitching and football passing is needed during this phase to resist the large distractive forces that occur at the shoulder, which are near or in excess of body weight.
The EMG differences between varying overhead throwing motions may be due to mechanical differences between different activities. For example, in baseball pitching and football passing a weighted ball (5-oz baseball and 15-oz football) is carried in the hands throughout throwing phases but is released just before the beginning of the deceleration phase. With these weighted balls no longer in hand, the arm can travel faster just after ball release (beginning of deceleration phase), and thus more posterior shoulder forces and torques may be generated by the posterior musculature to slow down the rapidly moving arm. In the volleyball spike there is no weighted implement in the hand throughout the entire motion. Moreover, when the hand contacts the ball, the ball generates an equal and opposite force on the hand, which acts to slow down the forward-moving hand. Therefore, a slower-moving arm may result in smaller forces and torques at the shoulder to decelerate the arm and less muscle activity. This explanation might partially explain the lower rotator cuff activity in the volleyball spike compared with baseball pitching and football passing, especially from the posterior musculature (see Table 32-4). However, a biomechanical analysis of the volleyball spike is needed to quantify shoulder forces and torques to help confirm this hypothesis.
TENNIS SERVE AND VOLLEY
Tennis Serve
The tennis literature is abundant with studies that have examined EMG activity of the elbow and wrist musculature, but data on shoulder EMG during the tennis serve and volley are sparse. Ryu and colleagues27 conducted the only known study that extensively quantified shoulder EMG during the tennis serve. EMG data were collected during the serve from eight shoulder muscles using six male collegiate tennis players. One of the limitations of this study is that no standard deviations were reported and only a few subjects were used. The serve was divided into four phases: wind-up, cocking, acceleration, and deceleration and follow-through. Wind-up is the phase from start of service motion to ball release, cocking is from ball release to maximum shoulder external rotation, acceleration is from maximum shoulder external rotation to racquet contact with the ball, and deceleration and follow-through are from racquet contact with the ball to completion of the serve.
Shoulder EMG results during the serve are shown in Table 32-5. Mean EMG peaked for the infraspinatus and supraspinatus during the cocking phase. During this phase, the shoulder externally rotates approximately 170 degrees and the peak shoulder internal rotator torque is approximately 65 N•m.28 These kinematic and kinetic data help explain the high activity from the infraspinatus, which is active in initiating shoulder external rotation during the first half of the cocking phase. The infraspinatus and supraspinatus also contract to resist shoulder-distraction forces during the cocking phase. Although not quantified during the tennis serve, shoulder compressive force (to resist distraction) is approximately 80% of body weight during the cocking phase in baseball pitching, which is a motion similar to the tennis serve.7 The biceps brachii can also help generate shoulder compressive force during the cocking phase,2 which might help explain the relatively high activity from this muscle. Pectoralis major, latissimus dorsi, and subscapularis activity were greatest during the acceleration phase, as these muscles contract to help generate a peak shoulder internal rotation angular velocity of approximately 2500 deg/sec26 and accelerate the arm forward. The serratus anterior also peaked during the acceleration phase to properly position the scapula relative to the rapidly moving humerus. These EMG findings during the tennis serve are similar to EMG findings during baseball pitching, which is not surprising considering the numerous kinematic and kinetic similarities between the tennis serve and the baseball pitch.6-8,26,28
EMG activity during arm deceleration and follow-through demonstrated moderate to high activity, but activity was less than the EMG observed during baseball pitching and football passing. One reason for this, as for the volleyball spike, is that the force the ball exerts against the racquet acts to slow down the arm, which may result in lower posterior forces and torques needed from muscle contractions. The relatively high activity from the biceps brachii helps stabilize the shoulder (resist distraction) and decelerate the rapid elbow extension angular velocity, which peaks at approximately 1500 deg/sec.26 The moderate to high activity from the rotator cuff muscles generate compressive force to help resist shoulder-distraction forces, in which peak forces have been quantified at approximately 75% of body weight during the serve.28
Tennis Volley
A few studies have examined shoulder activity during the tennis backhand and forehand.27,29,30 Ryu and colleagues collected EMG data from eight shoulder muscles using six male collegiate tennis players. This study is weakened by a low number of subjects, no standard deviations reported, and no statistical analyses between the forehand and backhand volleys. The forehand and backhand volleys were divided into three phases: racquet preparation, acceleration, and follow-through.27 Racquet preparation is the phase from shoulder turn to initiation of weight transfer to the front foot, acceleration is from initiation of weight transfer to the front foot to racquet contact with the ball, and deceleration and follow-through are from racquet contact with the ball to completion of the stroke.
Shoulder EMG results from Ryu and colleagues27 during forehand and backhand volleys are shown in Table 32-6. Muscle activity was relatively low during the racquet-preparation phase, which is consistent with forehand and backhand shoulder EMG data from Chow and colleagues.30 Relatively large differences in muscle activity have been reported between the forehand and backhand during the acceleration phase.27,30 High activity has been reported in the biceps brachii, anterior deltoid, pectoralis major, and subscapularis during the forehand volley, but these same muscles exhibited low activity during the backhand volley.27,29,30 The high activity during the forehand from the pectoralis major, anterior deltoid, and subscapularis is not surprising given their roles as horizontal flexors and internal rotators. However, the high activity from the biceps brachii is somewhat surprising.
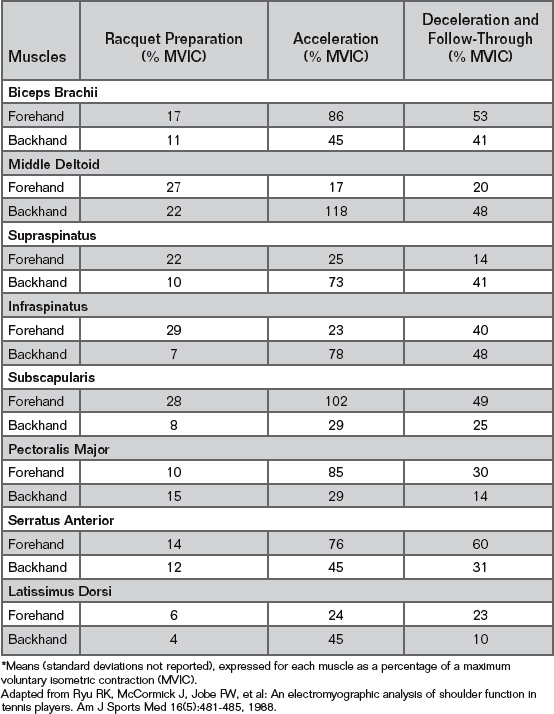
Morris and colleagues31 also reported high biceps activity during the forehand in the acceleration phase. The biceps is in a mechanically advantageous position to horizontally adduct the shoulder during the forehand motion, and they also work to stabilize both the shoulder and elbow. Moreover, they also can help cause the slight amount of elbow flexion that occurs to stabilize the elbow and keep it from extending (due to inertial forces and torques the upper arm applies to the forearm at the elbow as the arm rapidly horizontally adducts). The serratus anterior is also more active during the forehand compared with the backhand to help protract the scapula during the acceleration phase and help properly position the scapula relative to the rapidly moving humerus.
Posterior deltoids, middle deltoids, supraspinatus, infraspinatus, latissimus dorsi, and triceps brachii exhibited high activity during the backhand volley but relatively low activity during the forearm volley.27,30 These muscles all work synergistically during the backhand to horizontally extend and externally rotate the UE. The triceps also work to extend the elbow and help stabilize both the shoulder and elbow. The high activity from the supraspinatus and infraspinatus helps provide shoulder-compression forces to resist shoulder distraction. The supraspinatus and deltoids also help maintain the shoulder in abduction.
BASEBALL BATTING
Only one study has quantified muscle activity of the shoulder during baseball hitting.32 Using the swings of 18 professional male baseball players during batting practice, the investigators quantified posterior deltoid, triceps brachii, supraspinatus, and serratus anterior activity during six phases of batting: wind-up, preswing, early swing, middle swing, late swing, and contact of the bat with the ball. Wind-up is from lead heel off to lead forefoot contact; preswing is from lead forefoot contact to the beginning of the swing; early swing is from the beginning of the swing to when the bat is perpendicular to the ground; middle swing is from when the bat is perpendicular to the ground to when the bat is parallel with the ground; late swing is from when the bat is parallel with the ground to bat contact with the ball; and follow-through is from bat contact with the ball to maximum abduction and external rotation of the lead shoulder.
Muscle activity was relatively low during the wind-up and follow-through phases, with EMG magnitudes generally less than 25% of MVIC. The posterior deltoid peaked at 101% of MVIC during preswing and then progressively decreased throughout early swing (88% MVIC), middle swing (82% MVIC), and late swing (76% MVIC). Triceps brachii activity was 46% of MVIC during preswing, peaked at 92% of MVIC during early swing, and then progressively decreased to 73% of MVIC during middle swing and 38% of MVIC during late swing. Both the supraspinatus and serratus anterior generated relatively moderate and constant activity from preswing to late swing, ranging from 28% to 39% of MVIC throughout these four phases.
Compared with overhand throwing, EMG data for hitting are relatively sparse, and thus it is hard to make definite conclusions. There are EMG data for only a few shoulder muscles with which to compare. Nevertheless, it does appear that both glenohumeral and scapular muscles generate high activity during the swing, because both concentric and eccentric muscle actions are needed throughout the swing. To make it even more difficult to develop summaries of muscle-firing patterns in hitting, there are currently no shoulder kinetic data in the hitting literature. The focus of future hitting studies should be on quantifying shoulder forces and torques throughout the swing and on acquiring shoulder EMG data for additional shoulder muscles, such as the infraspinatus, teres minor, pectoralis major, latissimus dorsi, biceps brachii, and trapezius.
GOLF SWING
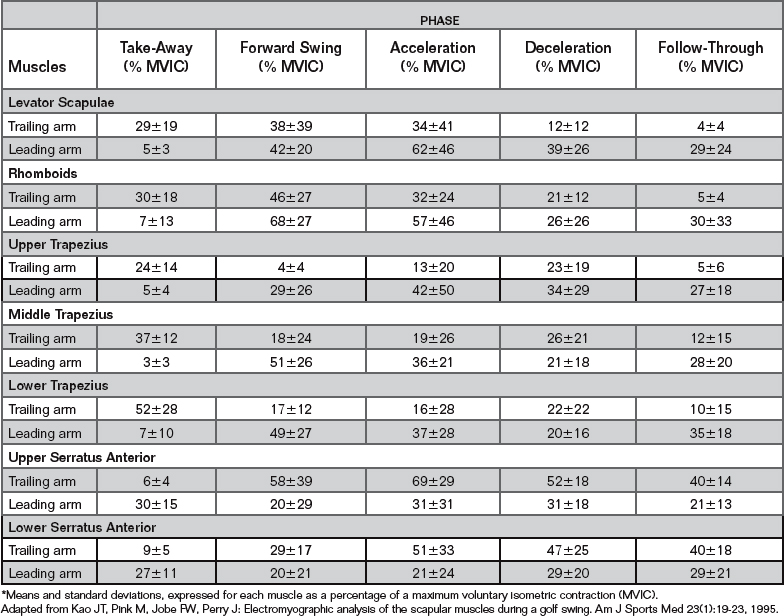
Several studies have examined shoulder muscle activity during the golf swing.33-37 Jobe and colleagues34,35 and Pink and colleagues37 used male and female professional golfers to study shoulder musculature activity. These authors quantified both shoulder34,35 and scapular36 muscles of both the leading arm (left for a right-handed golfer) and trailing arm (right for a right-handed golfer), and also reported no significant differences during the swing in shoulder EMG between male and female professional golfers.35 The golf swing has been divided into five phases:34-36 take-away, forward swing, acceleration, deceleration, and follow-through. Take-away is the phase from ball address to the end of the backswing; forward swing is from the end of backswing to when the club is horizontal; acceleration is from when the club is horizontal to impact with the ball; deceleration is from ball impact to when the club is horizontal; and follow-through is from when the club is horizontal to the end of the motion.
Shoulder muscle activity during the golf swing is shown in Table 32-7,37 and scapular muscle activity is shown in Table 32-8.36 During the take-away phase, muscle activity is relatively low to moderate, suggesting that lifting the arms and club up during the backswing is not a strenuous activity. The levator scapulae and lower and middle trapezius of the trailing arm exhibit moderate activity during this phase to elevate and upwardly rotate the scapula, and moderate activity from the serratus anterior of the leading arm helps protract and upwardly rotate the scapula. Upper, lower, and middle trapezius activities are highest during this phase compared with the other four phases.
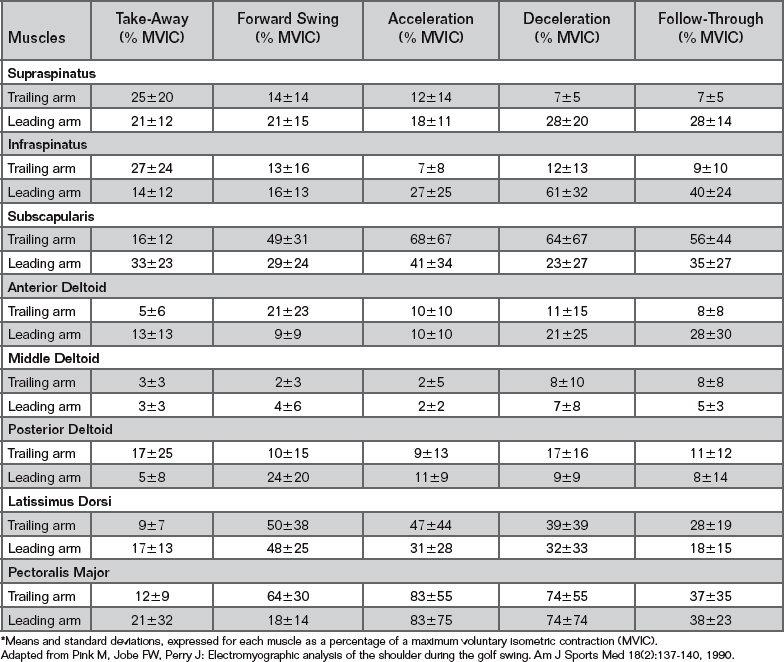
Infraspinatus and supraspinatus activities of the trailing arm are also highest during this phase but only fire approximately 25% of a MVIC, which implies relatively low activity from these rotator cuff muscles throughout the golf swing. This is surprising in part because most shoulder injuries are overuse injuries that typically involve the supraspinatus or infraspinatus.38-41 However, these rotator cuff EMG data are only for the trailing arm, which exhibited less overall rotator cuff activity throughout the swing compared with the leading arm. These data imply that rotator cuff injury risk may be higher in the leading arm, but this conclusion might not be valid because it only takes relative muscle activity into account and not other factors, such as impingement risk between shoulders. Another interesting finding is that anterior, middle, and posterior deltoid activities were all relatively low throughout all phases, implying that these muscles are not used much throughout the swing.
During the forward swing phase, muscle activity was also relatively low to moderate, except there was relatively high activity from the subscapularis, pectoralis major, latissimus dorsi, and serratus anterior of the trailing arm to adduct and internally rotate the trailing arm and protract the scapula. There were also relatively high activity from the rhomboids and middle and lower trapezius of the leading arm to help retract and stabilize the scapula.
Muscle activity during the acceleration phase was higher overall compared with the forward swing phase. The subscapularis, pectoralis major, latissimus dorsi, and serratus anterior of the trailing arm demonstrated high activity during the acceleration phase to continue adducting and internally rotating the trailing arm. These muscles may be the most important power muscles of the upper extremity to help accelerate the arm during the acceleration phase of the downswing. In addition, using a short or long backswing can affect shoulder activity during the acceleration phase. Slightly greater pectoralis major and latissimus dorsi activity has been reported during the acceleration phase when a short backswing was used compared with a long backswing, suggesting that shoulder injury risk might increase over time.33
During the deceleration phase, the subscapularis, pectoralis major, latissimus dorsi, and serratus anterior of the trailing arm continued to demonstrate high activity, although now the muscle action is more eccentric and slightly smaller in magnitude compared with the acceleration phase. Low to moderate activity occurred from the scapular muscles of the leading arm, and high pectoralis major and infraspinatus activity occurred in the leading arm. Muscle activity generally decreased from the deceleration phase to the follow-through phase.
1 DiGiovine NM, Jobe FW, Pink M, Perry J. Electromyography of upper extremity in pitching. J Shoulder Elbow Surg. 1992;1:15-25.
2 Glousman R, Jobe F, Tibone J, et al. Dynamic electromyographic analysis of the throwing shoulder with glenohumeral instability. J Bone Joint Surg Am. 1998;70(2):220-226.
3 Gowan ID, Jobe FW, Tibone JE, et al. A comparative electromyographic analysis of the shoulder during pitching. Professional versus amateur pitchers. Am J Sports Med. 1987;15(6):586-590.
4 Jobe FW, Moynes DR, Tibone JE, Perry J. An EMG analysis of the shoulder in pitching. A second report. Am J Sports Med. 1984;12(3):218-220.
5 Jobe FW, Tibone JE, Perry J, Moynes D. An EMG analysis of the shoulder in throwing and pitching. A preliminary report. Am J Sports Med. 1983;11(1):3-5.
6 Escamilla RF, Barrentine SW, Fleisig GS, et al. Pitching biomechanics as a pitcher approaches muscular fatigue during a simulated baseball game. Am J Sports Med. 2007;35(1):23-33.
7 Fleisig GS, Andrews JR, Dillman CJ, Escamilla RF. Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med. 1995;23(2):233-239.
8 Escamilla RF, Fleisig GS, Barrentine SW, et al. Kinematic comparisons of throwing different types of baseball pitches. J Appl Biomech. 1998;14(1):1-23.
9 Escamilla R, Fleisig G, Barrentine S, et al. Kinematic and kinetic comparisons between American and Korean professional baseball pitchers. Sports Biomech. 2002;1(2):213-228.
10 Werner SL, Fleisig GS, Dillman CJ, Andrews JR. Biomechanics of the elbow during baseball pitching. J Orthop Sports Phys Ther. 1993;17(6):274-278.
11 Feltner M, Dapena J. Dynamics of the shoulder and elbow joints of the throwing arm during a baseball pitch. Inter J Sport Biomech. 1986;22:35-59.
12 Roberts EM. Cinematography in biomechanical investigation. In: In Selected Topics on Biomechanics: Proceedings of the C.I.C. Symposium on Biomechanics, Indiana University, October 19–20, 1970. Chicago: The Athletic Institute; 1971:41-50.
13 Toyoshima S, Hoshikawa T, Miyashita M, Oguri T. Contribution of the body parts to throwing performance. In: Nelson RC, Morehouse CA, editors. Biomechanics IV. Baltimore: University Park Press; 1974:169-174.
14 Kelly BT, Backus SI, Warren RF, Williams RJ. Electromyographic analysis and phase definition of the overhead football throw. Am J Sports Med. 2002;30(6):837-844.
15 Fleisig GS, Escamilla RF, Andrews JR, et al. Kinematic and kinetic comparison between baseball pitching and football passing. J Appl Biomech. 1996;12:207-224.
16 Maffet MW, Jobe FW, Pink MM, et al. Shoulder muscle firing patterns during the windmill softball pitch. Am J Sports Med. 1997;25(3):369-374.
17 Barrentine SW, Fleisig GS, Whiteside JA, et al. Biomechanics of windmill softball pitching with implications about injury mechanisms at the shoulder and elbow. J Orthop Sports Phys Ther. 1998;28(6):405-415.
18 Werner SL, Guido JA, McNeice RP, et al. Biomechanics of youth windmill softball pitching. Am J Sports Med. 2005;33(4):552-560.
19 Loosli AR, Requa RK, Garrick JG, Hanley E. Injuries to pitchers in women’s collegiate fast-pitch softball. Am J Sports Med. 1992;20(1):35-37.
20 Watkins J, Green BN. Volleyball injuries: A survey of injuries of Scottish National League male players. Br J Sports Med. 1992;26(2):135-137.
21 Chandler TJ, Kibler WB, Uhl TL, et al. Flexibility comparisons of junior elite tennis players to other athletes. Am J Sports Med. 1990;18(2):134-136.
22 Schafle MD. Common injuries in volleyball. Treatment, prevention and rehabilitation. Sports Med. 1993;16(2):126-129.
23 Schafle MD, Requa RK, Patton WL, Garrick JG. Injuries in the 1987 national amateur volleyball tournament. Am J Sports Med. 1990;18(6):624-631.
24 Kugler A, Kruger-Franke M, Reininger S, et al. Muscular imbalance and shoulder pain in volleyball attackers. Br J Sports Med. 1996;30(3):256-259.
25 Rokito AS, Jobe FW, Pink MM, et al. Electromyographic analysis of shoulder function during the volleyball serve and spike. J Shoulder Elbow Surg. 1998;7(3):256-263.
26 Fleisig G, Nicholls R, Elliott B, Escamilla R. Kinematics used by world class tennis players to produce high-velocity serves. Sports Biomech. 2003;2(1):51-64.
27 Ryu RK, McCormick J, Jobe FW, et al. An electromyographic analysis of shoulder function in tennis players. Am J Sports Med. 1988;16(5):481-485.
28 Elliott B, Fleisig G, Nicholls R, Escamilia R. Technique effects on upper limb loading in the tennis serve. J Sci Med Sport. 2003;6(1):76-87.
29 Adelsberg S. The tennis stroke: An EMG analysis of selected muscles with rackets of increasing grip size. Am J Sports Med. 1986;14(2):139-142.
30 Chow JW, Carlton LG, Lim YT, et al. Muscle activation during the tennis volley. Med Sci Sports Exerc. 1999;31(6):846-854.
31 Morris M, Jobe FW, Perry J, et al. Electromyographic analysis of elbow function in tennis players. Am J Sports Med. 1989;17(2):241-247.
32 Shaffer B, Jobe FW, Pink M, Perry J. Baseball batting. An electromyographic study. Clin Orthop RelatRes. 1993;292:285-293.
33 Bulbulian R, Ball KA, Seaman DR. The short golf backswing: Effects on performance and spinal health implications. J Manipulative Physiol Ther. 2001;24(9):569-575.
34 Jobe FW, Moynes DR, Antonelli DJ. Rotator cuff function during a golf swing. Am J Sports Med. 1986;14(5):388-392.
35 Jobe FW, Perry J, Pink M. Electromyographic shoulder activity in men and women professional golfers. Am J Sports Med. 1989;17(6):782-787.
36 Kao JT, Pink M, Jobe FW, Perry J. Electromyographic analysis of the scapular muscles during a golf swing. Am J Sports Med. 1995;23(1):19-23.
37 Pink M, Jobe FW, Perry J. Electromyographic analysis of the shoulder during the golf swing. Am J Sports Med. 1990;18(2):137-140.
38 Hamilton CD, Glousman RE, Jobe FW, et al. Dynamic stability of the elbow: Electromyographic analysis of the flexor pronator group and the extensor group in pitchers with valgus instability. J Shoulder Elbow Surg. 1996;5(5):347-354.
39 Choi CH, Kim SK, Jang WC, Kim SJ. Biceps pulley impingement. Arthroscopy. 2004;20(suppl):280-283.
40 McHardy A, Pollard H, Luo K. Golf injuries: A review of the literature. Sports Med. 2006;36(2):171-187.
41 Wiesler ER, Lumsden B. Golf injuries of the upper extremity. J Surg Orthop Adv. 2005;14(1):1-7.