19 ANALYSIS: WHITE OUT
When assessing a white out it is essential to be aware of the possible causes (Table 19.1).
Table 19.1 Causes of a white out.
| Common | |
| Uncommon | Extensive pneumonia involving the entire lung. |
| Extremely uncommon | Extensive tumour infiltration of the lung. |
| Extraordinarily rare | Congenital absence of a lung. |
WHITE OUT—ANALYSING THE CXR1-4
 The key to analysing a white out is determining whether the mediastinum is displaced. This requires assessment of the position of the heart and the position of the trachea.
An occasional dilemma: a white out but: (a) there is no displacement of the mediastinum and (b) the trachea is central.
The key to analysing a white out is determining whether the mediastinum is displaced. This requires assessment of the position of the heart and the position of the trachea.
An occasional dilemma: a white out but: (a) there is no displacement of the mediastinum and (b) the trachea is central.
 The most likely cause: a large pleural effusion associated with or causing major collapse of the lung. The net effect is no displacement. Much less common: an extensive lobar pneumonia affecting all the lobes of the lung. An air bronchogram (p. 227) may be visible.
The most likely cause: a large pleural effusion associated with or causing major collapse of the lung. The net effect is no displacement. Much less common: an extensive lobar pneumonia affecting all the lobes of the lung. An air bronchogram (p. 227) may be visible.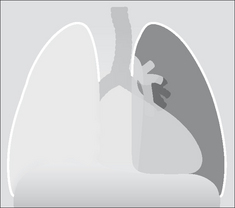
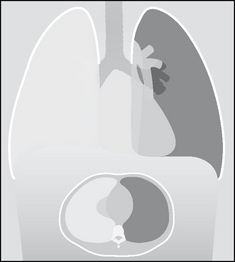
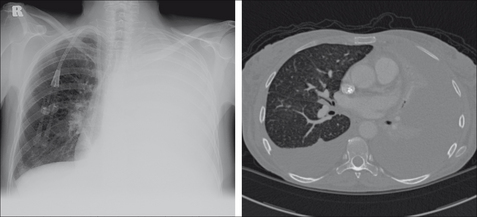
Figure 19.3 White out. The mediastinum is central and so is the trachea. Large effusion with collapse of the underlying lung. The CT section shows the major compression collapse of the right lung caused by the large volume of fluid in the pleural space.

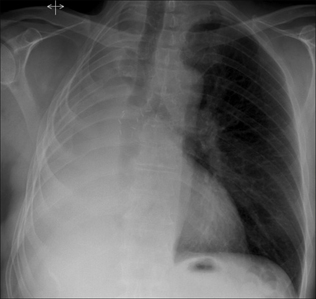
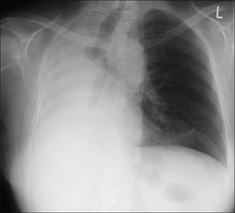
Figure 19.4 White out. The mediastinum and trachea are displaced to the right side. Major collapse of the entire right lung.

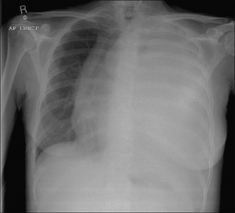
Figure 19.5 White out. The mediastinum and the trachea are displaced to the right side. Several of the underlying ribs are abnormal. A previous right pneumonectomy accounts for the white out.
| CXR findings | Most likely cause | |
|---|---|---|
| A | Large pleural effusion with minimal secondary compression collapse of the underlying lung. | |
| B* | Large effusion with major collapse of the underlying lung. | |
| C | Collapse of the entire lung. Minimal or no pleural fluid. | |
| D | Features as for C above, and: | Pneumonectomy. The clinical history is conclusive. |
* Exceptionally…these findings may be due to an extensive pneumonia affecting all the lobes of a lung, or to extensive tumour infiltration of the entire lung.
Answer to Fig. 19.1 on p. 264
Analysis: Trachea and mediastinum are shifted to the right indicating a major loss of lung volume. But…always assess the bones. In this patient note the rib changes as well as the surgical clips.
Conclusion: A previous right pneumonectomy explains the white out.
1. Ruskin JA, Gurney JW, Thorsen MK, et al. Detection of pleural effusions on supine chest radiographs. AJR. 1987;148:681-683.
2. Dee PM. The radiology of chest trauma. Radiol Clin North Am. 1992;30:291-306.
3. Leung AN, Muller NL, Miller RR. CT in differential diagnosis of diffuse pleural disease. AJR. 1990;154:487-492.
4. Kawashima A, Libshitz HI. Malignant pleural mesothelioma: CT manifestations in 50 cases. AJR. 1990;155:965-969.