24 SUSPECTED AORTIC DISSECTION
 Occasionally the term dissecting aneurysm is used. This is inaccurate terminology. It is more correct to refer to the lesion as a dissecting haematoma. Blood enters the aortic wall through a tear and dissects between the inner and middle layers (intima and media). The haematoma then tracks for a variable distance along the length of the aorta. Side branches supplying the major organs can be occluded. Mortality is high. Untreated, approximately 75% of patients with a dissection involving the ascending aorta will die within two weeks1.
Occasionally the term dissecting aneurysm is used. This is inaccurate terminology. It is more correct to refer to the lesion as a dissecting haematoma. Blood enters the aortic wall through a tear and dissects between the inner and middle layers (intima and media). The haematoma then tracks for a variable distance along the length of the aorta. Side branches supplying the major organs can be occluded. Mortality is high. Untreated, approximately 75% of patients with a dissection involving the ascending aorta will die within two weeks1.TWO DIAGNOSTIC PRIORITIES
CLASSIFICATIONS
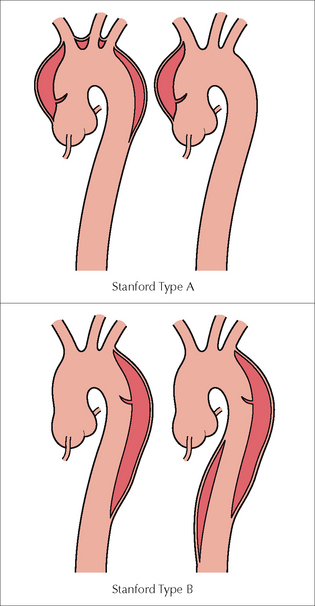
Aortic dissections are classified anatomically. There are two main classifications: the DeBakey classification and the Stanford classification. We describe the Stanford classification as it is currently the one that is most commonly used.
DISSECTION: TYPES AND CLINICAL MANAGEMENT1-10
HOW CAN THE CXR HELP?
The CXR appearance can assist in influencing the physician’s initial estimate of the likelihood of a dissection being present—i.e. it impacts on the post-test probability of aortic dissection (see Chapter 17, p. 249).
In 88% of patients with an acute dissection1, one or more of the following findings will be present: widened mediastinum; abnormal aortic knuckle; left pleural effusion; pericardial effusion.Widened mediastinum1,11-14
Most importantly—whenever possible, compare present and previous CXRs. This is the most reliable way of confirming whether mediastinal widening is due to a dissection. Comparison may show that mediastinal widening is longstanding and likely to be due to simple age related unfolding of the aorta, or that mediastinal widening is new. Widening of the mediastinum in a patient with a suspected aortic dissection has a high sensitivity (81–90%) but a low specificity. The mediastinum enlarges to the right with a dissection of the ascending aorta and to the left with a dissection of the descending aorta. The 8-cm rule2. This is a rough rule of thumb: on a portable AP CXR a widened mediastinum is one that exceeds a diameter of 8 cm at the level of the aortic arch. The overall level of clinical suspicion is decisive. With a low level of clinical suspicion, comparison with previous CXRs will often provide sufficient reassurance that a dissection has not occurred. On the other hand, a high pre-test probability for dissection together with a widened mediastinum on the CXR will lead to a definitive cross-sectional investigation (as illustrated in Table 17.1).Abnormal aortic knuckle…and calcification11
A useful rule of thumb: If calcification within the aortic wall is displaced from the outer aortic margin by 1.0 cm or more…then the probability of a dissection is high. This rule becomes most useful if a lateral CXR shows absence of calcification in the anterior or posterior aortic wall (Fig. 24.2). This calcium sign requires caution. Apparent displacement of intimal calcification from the outer margin of the ascending aortic wall on the frontal CXR can be misleading and spurious. The calcification may be in the descending aorta. In other words, calcification that appears displaced inwards from the lateral wall of the ascending aorta may actually be undisplaced and positioned on the posterior wall of a normal descending aorta (as illustrated in Fig. 24.3).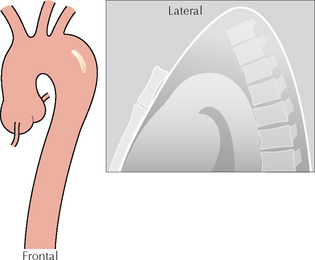
Figure 24.2 Intimal calcification. On the frontal projection the calcification appears to lie more than 1.0 cm from the outer margin of the aorta. The lateral projection does not show any intimal calcification either anteriorly or posteriorly. This appearance provides strong support for the diagnosis of dissection.
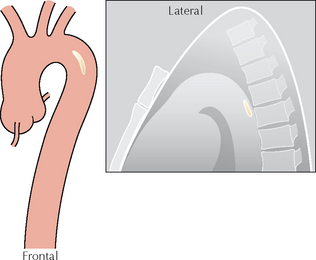
Figure 24.3 Intimal calcification. On the frontal projection the calcification appears to lie more than 1.0 cm from the outer margin of the aorta. However, the lateral projection shows that the calcification is situated posteriorly. This is not evidence of a dissection…the aortic arch is unfolded and the posterior calcification is (misleadingly) projected over the medial wall on the frontal view.
NO CHEST PAIN—BUT THE CXR APPEARANCE IS WORRYING
It is common for CXRs in middle-aged or elderly people to show a widened mediastinum, because the aortic arch gradually unfolds as we get older. But is the widening in a particular patient due to simple aortic unfolding, to a Stanford Type A dissection…or to an aneurysm of the ascending aorta?
Analysis of the CXR appearance will often provide the necessary reassurance that it is unfolding only (Figs 24.4 and 24.5). If there is any persisting doubt then a lateral CXR will provide additional support. A combination of the clinical history, clinical examination, and CXR analysis will almost always remove any worries.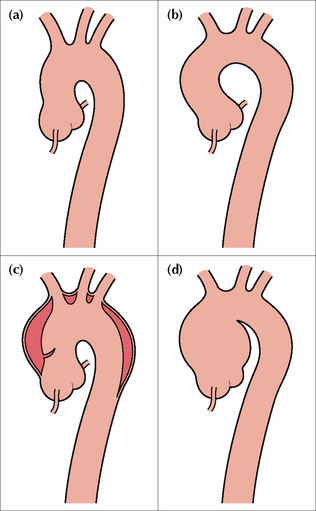
Figure 24.4 A widened mediastinum at the level of the aortic arch may be vascular and due to either age related unfolding of the aorta (b), aortic dissection (c) or an aneurysm (d). A normal aorta—no unfolding—is shown in (a). Age related unfolding of the ascending and descending aorta from early middle age is a common CXR finding. Any unfolding will appear exaggerated, and often worrying, on an AP CXR because of the magnification effect.
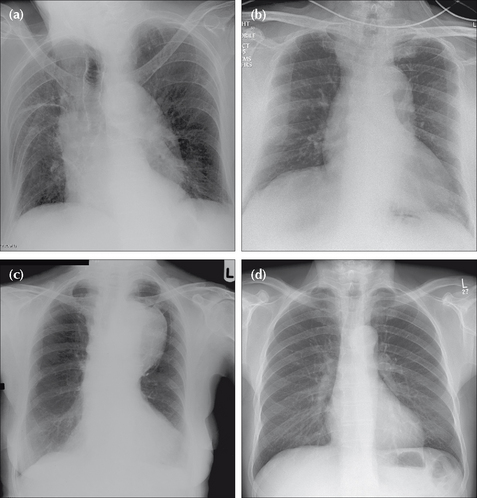
Figure 24.5 Four patients, all middle-aged or elderly. Patient (a): age related aortic unfolding. Patient (b): the aortic shadow at the level of the ascending aorta and aortic arch is prominent in this patient who presented with tearing chest pain. Stanford Type A dissection. Patient (c): the aortic arch and the proximal descending aorta are very prominent and due to aneurysmal dilatation. Patient (d): a normal aortic outline—no unfolding. The amount of age related unfolding of the thoracic aorta shows a wide variation in middle-aged or elderly individuals—compare the CXRs of patient (a) and patient (d). Furthermore, in an elderly or frail patient, rotation (see patient a) is often present and will exaggerate any unfolding.
CLINICAL SYNOPSIS: ACUTE CHEST PAIN10,15
In clinical practice the middle-aged or elderly patient presenting with acute chest pain is not only an emergency but frequently a diagnostic dilemma—is it a myocardial infarct or is it a dissection? Wise advice has been provided by Schubert10:
“…acute myocardial infarction (AMI) and aortic dissection can present identically. For patients with chest pain, the most important first step in distinguishing AMI from aortic dissection is to consider both as diagnostic possibilities. After that, the strongest and most reliable indicators for aortic dissection are found in the history. Results of ECG and CXR investigations do not reliably discriminate between aortic dissection and AMI. A careful history focused on the quality of a patient’s pain is the most useful tactic for distinguishing a dissection from AMI.”

GUIDELINES IN RELATION TO USEFULNESS OF THE CXR
The CXR will exclude some of the other causes of chest pain (e.g. pneumothorax, mediastinal emphysema). A completely normal CXR makes the diagnosis of a dissection unlikely in a patient in whom clinical suspicion is low.1. Chen K, Varon J, Wenker OC, et al. Acute thoracic aortic dissection: the basics. J Emerg Med. 1997;15:859-867.
2. Nienaber CA, Eagle KA. Aortic dissection: new frontiers in diagnosis and management. Part 1: From etiology to diagnostic strategies. Circulation. 2003;108:628-635.
3. Wiesenfarth J. Aortic dissection (monograph-on-line). Stanford, CA: Stanford University School of Medicine, 2001. www.emedicine.com/emerg.
4. Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA. 2000;283:897-903.
5. Khan IA, Nair CK. Clinical, diagnostic, and management perspectives of aortic dissection. Chest. 2002;122:311-328.
6. Erbel R, Zamorano J. The aorta. Aortic aneurysm, trauma, and dissection. Crit Care Clin. 1996;12:733-766.
7. Rogers FB, Osler TM, Shackford SR, et al. Aortic dissection after trauma: case report and review of the literature. J Trauma. 1996;41:906-908.
8. Pretre R, Von Segesser LK. Aortic dissection. Lancet. 1997;349:1461-1464.
9. Stultz DB, Gupta SC. Rapid assessment and treatment of aortic dissection. Emerg Med. 2004;36:18-43.
10. Schubert H. Thoracic aortic dissection: distinguishing it from acute myocardial infarction. Can Fam Physician. 2003;49:583-585.
11. Hansell DM, Armstrong P, Lynch DA, McAdams HP. Imaging of Diseases of the Chest, 4th ed. St Louis, MO: Mosby, 2005.
12. Cigarroa JE, Isselbacher EM, DeSanctis RW, et al. Diagnostic imaging in the evaluation of suspected aortic dissection. Old standards and new directions. N Engl J Med. 1993;328:35-43.
13. Jagannath AS, Sos TA, Lockhart SH, et al. Aortic dissection: a statistical analysis of the usefulness of plain chest radiographic findings. AJR. 1986;147:1123-1126.
14. Fisher ER, Stern EJ, Godwin JD. Acute aortic dissection: typical and atypical imaging features. Radiographics. 1994;14:1263-1271.
15. Kelly BS. Evaluation of the elderly patient with acute chest pain. Clin Geriatr Med. 2007;23:327-349.