27 CHEST PAIN: WHAT TO LOOK FOR
CHEST PAIN—POSSIBLE CAUSES
There are numerous causes for a pain in the chest1-10. They can be sub-divided into non-cardiac causes (common and uncommon), and cardiacoraortic causes. These sub-divisions are shown in Tables 27.1-27.3.
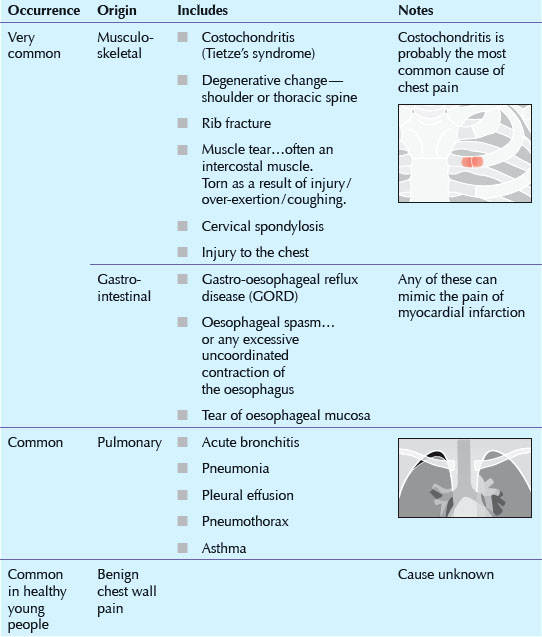
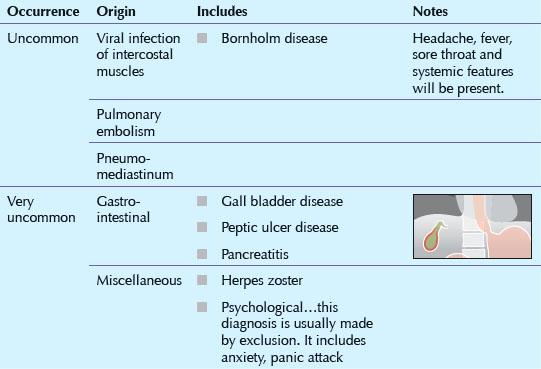
Table 27.3 Cardiac or aortic chest pain.
| Occurrence | Includes | Notes |
|---|---|---|
| Fairly common |
 |
|
| Uncommon | ||
| Often overlooked | Causes cardiac blood vessels to constrict. |

CHEST PAIN—THE ROLE OF THE CXR
The CXR is just one of several diagnostic tools. When a CXR is requested it will:
Sometimes…provide the precise diagnosis (Figs 27.1-27.3).
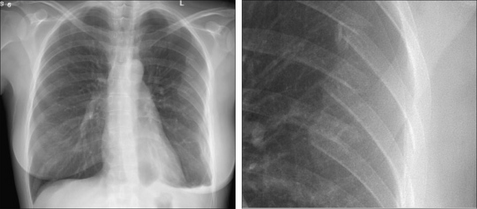
Figure 27.1 Female, 35 years. Drunk and disorderly. Complaining of chest pain. Multiple posterior rib fractures. Note also the shallow left pneumothorax.
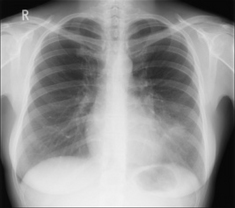
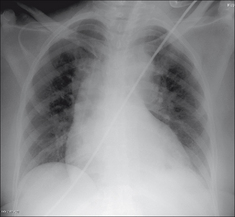
Figure 27.2 Female, 38 years. Chest pain. Silhouette sign...pneumonia in the lingular segments of the left upper lobe.

Figure 27.3 Male, 54 years. Chest pain, but difficult to localise. Free air under the domes of the diaphragm. Perforated duodenal ulcer.
Occasionally…suggest a possible diagnosis (Fig. 27.4).
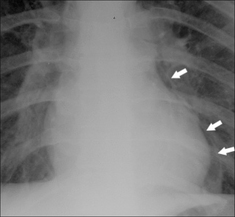
Figure 27.4 Young male. Recent vomiting episode. Now complains of chest pain. Air is present in the mediastinum (arrows). Oesophageal rupture. Boerhaave’s syndrome.
Often…exclude several causes for the pain.
CXR NORMAL—DIAGNOSTIC SIGNIFICANCE
“A normal finding, when assessed quantitatively, can sometimes be extremely valuable in differential diagnosis…only when a normal test result occurs with equal or nearly equal frequency among all the diseases being considered will a negative finding contribute little or nothing to the diagnostic process.”11
A normal CXR will exclude some very common causes of chest pain:

 Pneumothorax and/or pneumomediastinum are recognised complications when smoking cocaine12; or marijuana. The mechanism appears to be use of the valsalva manoeuvre to obtain a high input of the drug into the alveoli. Reflex coughing may raise the intra-alveolar pressure even higher and cause alveolar rupture. 10–30% of patients with chest pain who undergo cardiac catheterisation are found to have normal coronary arteries9. Cough-induced rib fractures. In patients with a chronic cough, 78% of fractures are in women. The lateral aspects of the middle ribs are most commonly affected and the sixth rib is particularly vulnerable10.
Pneumothorax and/or pneumomediastinum are recognised complications when smoking cocaine12; or marijuana. The mechanism appears to be use of the valsalva manoeuvre to obtain a high input of the drug into the alveoli. Reflex coughing may raise the intra-alveolar pressure even higher and cause alveolar rupture. 10–30% of patients with chest pain who undergo cardiac catheterisation are found to have normal coronary arteries9. Cough-induced rib fractures. In patients with a chronic cough, 78% of fractures are in women. The lateral aspects of the middle ribs are most commonly affected and the sixth rib is particularly vulnerable10.
1. Spalding L, Reay E, Kelly C. Cause and outcome of atypical chest pain in patients admitted to hospital. J R Soc Med. 2003;96:122-125.
2. Just RJ, Castell DO. Chest pain of undetermined origin. Gastrointest Endosc Clin N Am. 1994;4:731-746.
3. Crea F, Gaspardone A. New look to an old syndrome: Angina pectoris. Circulation. 1997;96:3766-3773.
4. Minocha A. Noncardiac chest pain. Where does it start? Postgrad Med. 1996;100:107-114.
5. Fam AG. Approach to musculoskeletal chest wall pain. Prim Care. 1988;15:767-782.
6. Wise CM. Chest wall syndromes. Curr Opin Rheumatol. 1994;6:197-202.
7. Hong SN, Rhee PL, Kim JH, et al. Does this patient have oesophageal motility abnormality or pathological acid reflux? Dig Liver Dis. 2005;37:475-484.
8. Chun AA, McGee SR. Bedside diagnosis of coronary artery disease: a systematic review. Am J Med. 2004;117:334-343.
9. Paterson WG. Canadian Association of Gastroenterology Practice Guidelines: management of non-cardiac chest pain. Can J Gastroenterol. 1998;12:401-407.
10. Hanak V, Hartman TE, Ryu JH. Cough induced rib fractures. Mayo Clin Proc. 2005;80:879-882.
11. Gorry GA, Pauker SG, Schwartz WB. The diagnostic importance of the normal finding. N Engl J Med. 1978;298:486-489.
12. Eurman DW, Potash HI, Eyler WR, et al. Chest pain and dyspnea related to “crack” cocaine smoking: value of chest radiography. Radiology. 1989;172:459-462.
13. Richter JE. Oesophageal motility disorders. Lancet. 2001;358:823-828.
14. Adler DG, Romero Y. Primary esophageal motility disorders. Mayo Clin Proc. 2001;76:195-200.
15. Tutuian R, Castell DO. Review article: oesophageal spasm — diagnosis and management. Aliment Pharmacol Ther. 2006;23:1393-1402.