31 SYSTEMIC HYPERTENSION: WHAT TO LOOK FOR
Causes of arterial hypertension:

Normal blood pressure and hypertension: Clinic measurements are often higher than those recorded at home or as 24-hour ambulatory values. There are no universally agreed absolute measurements…but general clinic values:
Coarctation of the aorta: A congenital narrowing of the aortic arch.
 Infantile type: a diffuse aortic narrowing between the left subclavian artery and the ductus arteriosus. Adult type: the narrowing is adjacent or slightly distal to the ductus. The obstruction develops gradually and presentation is commonly due to complications occurring between the ages of 15 and 30 years1.
Infantile type: a diffuse aortic narrowing between the left subclavian artery and the ductus arteriosus. Adult type: the narrowing is adjacent or slightly distal to the ductus. The obstruction develops gradually and presentation is commonly due to complications occurring between the ages of 15 and 30 years1.ESSENTIAL HYPERTENSION—WHAT WILL THE CXR SHOW?
In the vast majority of patients with essential or secondary hypertension the CXR features are unrelated to the underlying cause. The role of the CXR is very basic and simple: to show whether obvious cardiac changes resulting from the raised blood pressure are present. These are:
COARCTATION OF THE AORTA
This is the one cause of systemic arterial hypertension in which evaluation of the CXR must include more than an assessment of cardiac complications. There are two circumstances:
In a particular patient the physician may, on clinical examination, consider that coarctation is possible. The diagnosis may be completely unsuspected. The CXR findings may be the first intimation of coarctation. Most of the coarctations that present after the first year of life are usually post-ductal and these patients are often symptom free. Frequently aortic coarctation is discovered incidentally, not simply because of hypertension or a murmur but serendipitously because of an abnormal CXR.EVALUATING THE CXR3-5
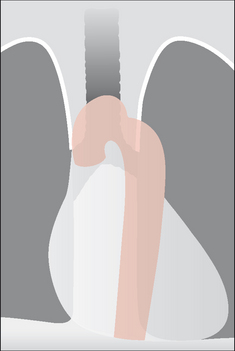
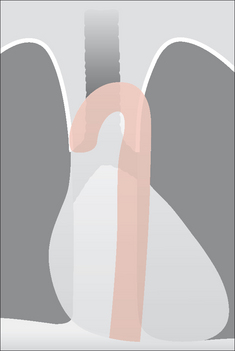
The narrowing of the aorta is shown in Fig. 31.1.
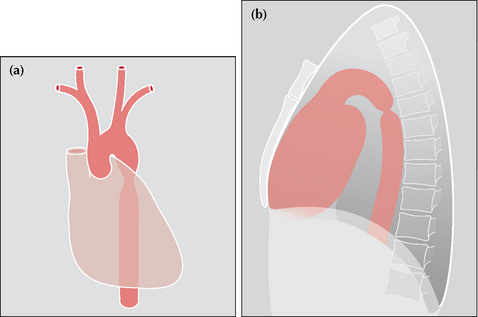
Figure 31.1 Coarctation. To show the site of the aortic narrowing at, or close to, the isthmus of the aorta. (a) Frontal CXR. (b) Lateral CXR. The aortic isthmus is the anatomical site of the junction of the arch and descending aorta.
Look for—rib notching3,5
Resulting from the development of a collateral circulation involving the posterior intercostal arteries. The dilated arteries cause pressure erosion of the posterior and inferior aspects of the ribs. Only ribs 3–9 are affected. Usually bilateral; occasionally unilateral. The notching is often asymmetrical (Fig. 31.2). Notching is rarely evident below the age of five years. The roof of each notch shows some reactive sclerosis5 (i.e. density), because the dilated posterior intercostal arteries exert a longstanding pressure effect on the ribs.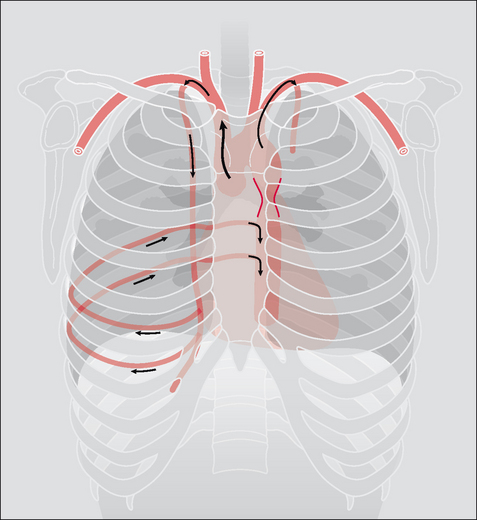
Look for—an abnormal mediastinal shadow3
An abnormal aortic knuckle is usual in adults. It is often evident even in young children. There are a variety of configurations (Figs 31.3-31.6)3.
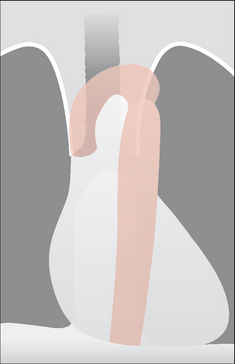
The “figure 3” configuration. The superior bulge is caused by an enlarged left subclavian artery and/or the aortic arch. The inferior bulge is due to post-stenotic dilatation of the aorta (Fig. 31.3).
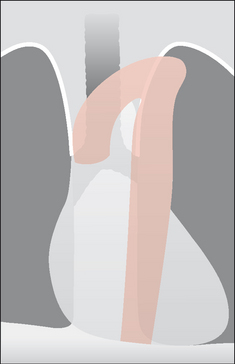
Caused by an enlarged left subclavian artery and/or aortic arch…but there is no appreciable post-stenotic dilatation (Fig. 31.4).
Due to an inconspicuous left subclavian artery, a small aortic arch, and no post-stenotic dilatation (Fig. 31.6).
Look for—cardiac enlargement
In children with coarctation an enlarged heart is common and is due to left ventricular hypertrophy3. Adults with coarctation usually have a normal cardio-thoracic ratio unless there is accompanying aortic valve disease or heart failure.
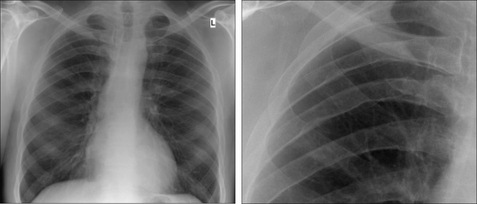
Figure 31.7 Adult. Coarctation. The main finding is the posterior and inferior rib notching. The mediastinum demonstrates a (somewhat) high knuckle appearance.
AN INTERESTING CONDITION—PSEUDOCOARCTATION (AKA KINKED AORTA)6-8
Aetiology/pathology
Closely related to coarctation but there is no pressure gradient across nor obstruction to the aortic lumen. An elongated and high aorta is kinked at the isthmus. There is no collateral circulation and so there is no rib notching.
Clinical features
No abnormal findings attributable to the kink. Often detected solely as an incidental left sided “mediastinal mass” on a CXR.
The CXR
A left-sided “mass” is projected above the aortic arch. A lateral CXR is very useful and will usually suggest that the mass is simply due to the high aortic arch. A CT examination with sagittal reconstruction will exclude a mass lesion or an aortic aneurysm and will confirm the diagnosis of pseudocoarctation.
1. Swanton RH. Pocket Consultant: Cardiology, 5th ed. Oxford: Blackwell, 2003.
2. Rosenthal E. Coarctation of the aorta from fetus to adult: curable condition or life long disease process? Heart. 2005;91:1495-1502.
3. Jefferson K, Rees S. Clinical Cardiac Radiology. London: Butterworth, 1980.
4. Cole TJ, Henry DA, Jolles H, et al. Normal and abnormal vascular structures that simulate neoplasms on chest radiographs: clues to the diagnosis. Radiographics. 1995;15:867-891.
5. Guttentag AR, Salwen JK. Keep your eyes on the ribs: the spectrum of normal variants and diseases that involve the ribs. Radiographics. 1999;19:1125-1142.
6. Hoeffel JC, Henry M, Mentre B, et al. Pseudocoarctation or congenital kinking of the aorta: radiologic considerations. Am Heart J. 1975;89:428-436.
7. Cheng TO. Pseudocoarctation of the aorta. An important consideration in the differential diagnosis of superior mediastinal mass. Am J Med. 1970;49:551-555.
8. Taneja K, Kawlra S, Sharma S, et al. Pseudocoarctation of the aorta: complementary findings on plain film radiography, CT, DSA, and MRA. Cardiovasc Intervent Radiol. 1998;21:439-441.