Multiple Masses
Multiple masses. Sigh. Do you hate these? Take a deep breath and lean into it. These masses are really not that hard to assess. They are almost always benign, BI-RADS 2, representing multiple cysts or fibroadenomas. This is like a “Get Out of Jail Free” card in Monopoly. Before we use the card though, we need to carefully look at each one to ensure that a cancer is not masquerading as a benign mass. We’ll give you our best tips for figuring out which patients actually need recall and which can be seen next year. Soon you will be thinking, “Bring it on!” instead of putting these cases on your partner’s desk.
The rule of multiplicity in mammography is that multiple and bilateral similar-appearing findings with low-suspicion features have a very high probability of being benign. The basis for this rule is that the genetic, hormonal, and other influences that produce benign findings in one breast tend to produce similar findings in the other, and it is very uncommon for malignant lesions to present simultaneously as similar-appearing findings in multiple regions of both breasts.
When multiple bilateral masses with circumscribed margins are detected by mammography, the rule of multiplicity can be applied and the findings are considered benign. These women can be spared the discomfort, inconvenience, anxiety, and cost of diagnostic mammography, ultrasonography (US), and in some cases, aspiration or biopsy.
However, with multiple masses, it is important to avoid the pitfall of using the rule of multiplicity too soon. Don’t play your “Get Out of Jail Free” card too early. These cases are complex and can be difficult to interpret. Benign masses may obscure other lesions or distract the radiologist from findings that need further evaluation.
Etiology of Multiple Bilateral Masses
Multiple bilateral masses may represent one type of lesion or more than one type. Cysts are the most common lesions contributing to multiple bilateral masses (Figs. 8-1 and 8-2). Cysts can develop at any age, but are most common in premenopausal women. Milk of calcium may be seen mammographically, providing clues to the cystic nature of one or more of the masses.
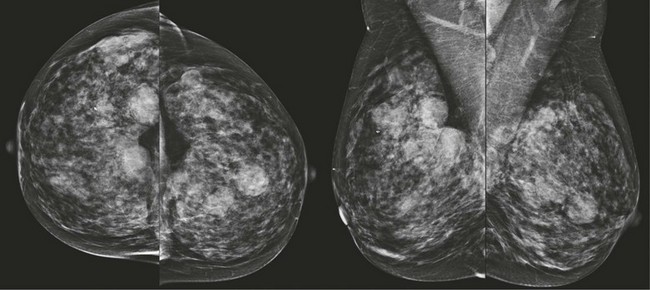
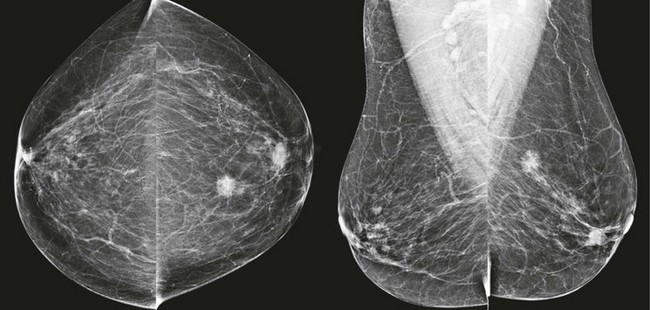
FIGURE 8-1 Multiple Bilateral Benign Masses.
Screening mammogram on a 48-year-old woman showing multiple bilateral similar-appearing masses with partially circumscribed margins. This woman had bilateral cysts previously demonstrated by US. There were no suspicious changes compared with previous mammograms. The patient was assigned BI-RADS 2, and no suspicious changes have occurred in over 2 years on subsequent mammography.
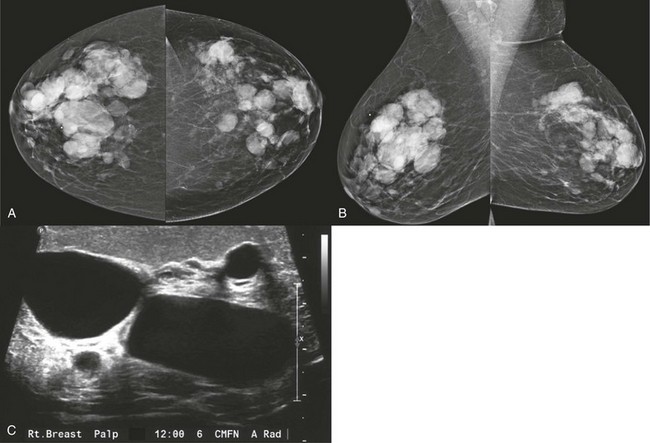
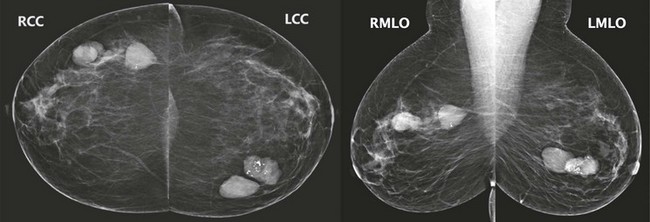
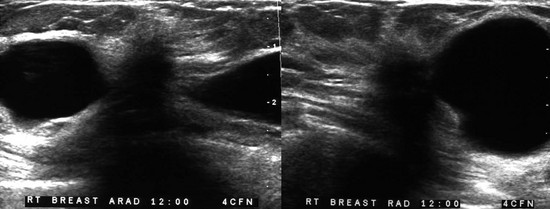
FIGURE 8-2 Multiple Cysts.
A 55-year-old woman with a newly palpable mass in her right breast (marker). A and B, There are multiple bilateral similar-appearing masses with circumscribed margins. When compared with previous mammograms, some masses had decreased in size while others showed enlargement. US targeted to the region of the newly palpable mass reveals multiple cysts (C). Sonographic evaluation of the remaining masses was considered unnecessary, and the patient was assigned BI-RADS 2.
Fibroadenomas are the second most common lesion causing multiple bilateral masses. When coarse calcifications are seen within one or more of the masses, it suggests that other, noncalcified masses may represent fibroadenomas as well (Fig. 8-3).
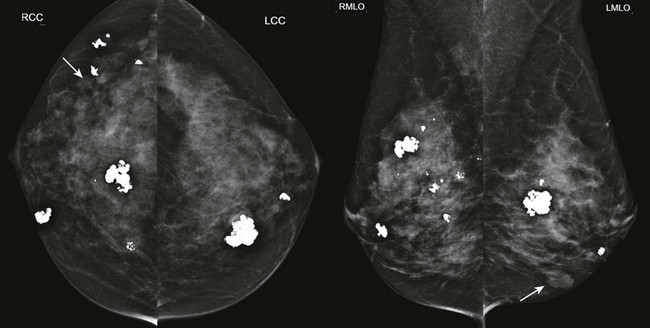
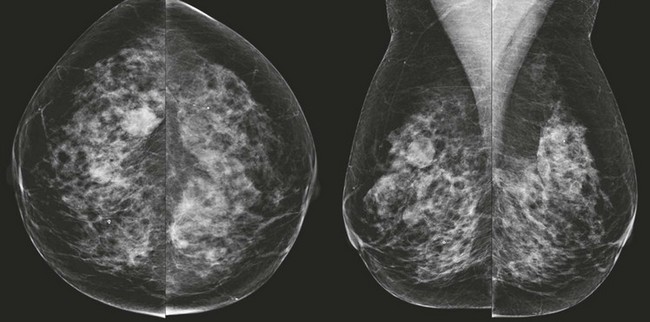
FIGURE 8-3 Multiple Fibroadenomas.
Screening mammogram on a 50-year-old woman. There are multiple bilateral masses, most with coarse calcifications typical of fibroadenomas. The noncalcified masses (arrows) likely represent fibroadenomas as well. The findings showed no suspicious changes for over 4 years.
Peripheral papillomas uncommonly present as multiple bilateral masses. Multiple papillomas are usually round or oval masses with circumscribed margins and are associated with an increased risk for breast cancer. Papillary carcinoma commonly presents as multiple circumscribed masses with segmental distributions on mammography.
Malignant multiple bilateral masses are very uncommon. Nevertheless, metastatic disease should still cross your mind when evaluating multiple bilateral breast masses (Fig. 8-4). Most women with breast metastases have a known history of malignancy. Unfortunately, breast involvement may be the first sign of recurrent disease in a woman thought cured of a malignant disease. Melanoma is the most common nonbreast primary neoplasm to metastasize to the breast. The appearance of the mammogram is usually different from that seen in the benign causes of multiple masses. The masses are typically denser than cysts or fibroadenomas, and the margins are often ill defined. Metastatic lesions of the breast are typically located throughout the organ, including the fatty tissue in the inframammary fold and axilla, whereas cysts and fibroadenomas are located within the breast tissue. Metastatic disease to the breast is often associated with axillary adenopathy, and some of the breast masses may represent metastatic intramammary lymph nodes. Lymphoma, leukemia, and rhabdomyosarcoma are rare in the breast and will be covered in more detail in Chapter 11, Expanding the Differential Diagnosis.
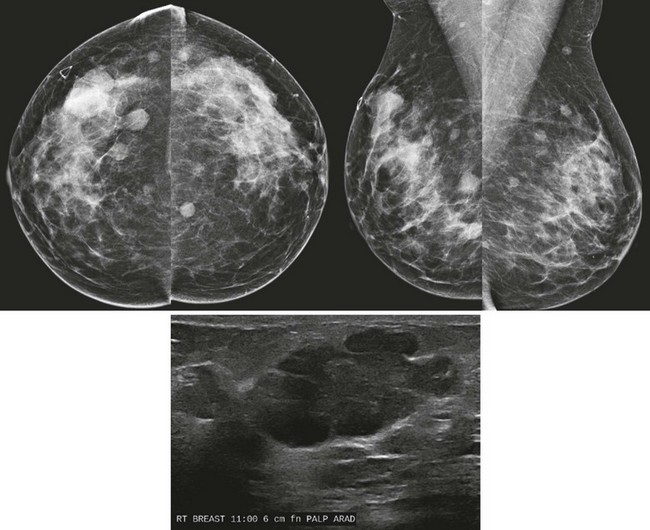
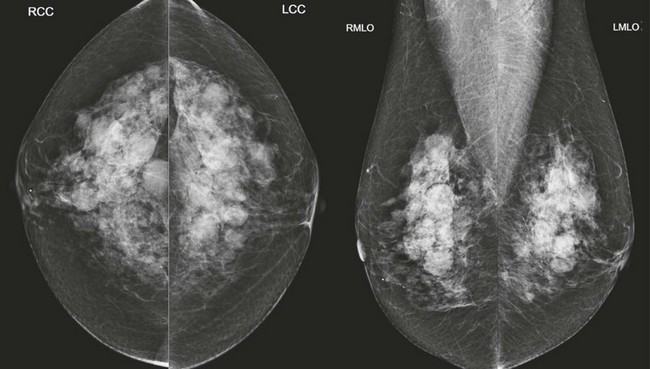
FIGURE 8-4 Metastatic Lesions in the Breasts.
This 47-year-old woman presented with a palpable lump in the right breast (marker). There are multiple circumscribed masses in both breasts. Note that the masses are primarily located in the retromammary fat and even in the axillary fat. US shows a solid hypoechoic mass with microloculated margins. Ultrasound-guided core biopsy samples were black in appearance. The patient subsequently gave a history of ocular melanoma 5 years earlier. Biopsy showed metastatic melanoma.
Intramammary lymph nodes typically demonstrate a lucent notch representing the fatty hilum. However, if the lucent notch is not visible, lymph nodes may contribute to the pattern of multiple bilateral masses. When lymph nodes have a characteristically benign appearance, we do not consider them one of the multiple bilateral masses. For example, if there are two indeterminate circumscribed masses in one breast and a typical intramammary lymph node in the other, the findings are not considered as multiple bilateral masses.
Skin lesions, such as nevi or neurofibromas, can mimic multiple bilateral breast masses. Ideally, your technologists will help you by noting them on the clinical history sheet (Box 8-1).
Management of Multiple Bilateral Masses
“Multiple bilateral masses” refers to asymptomatic women whose mammograms show a minimum of three masses, with at least one mass in each breast. These findings occur in 0.5% to 1.7% of patients in a screening population.
Management recommendations for multiple bilateral masses with benign features differ among radiologists. Many assign BI-RADS 2 and recommend annual screening mammography. Some radiologists recommend bilateral US after the initial mammogram, to serve as a baseline for future studies, while others assign BI-RADS 3 on the initial mammogram and recommend a 6-month bilateral follow-up study to evaluate stability. Our preference is to assign BI-RADS 2 and recommend annual mammographic screening. However, if any of the masses has suspicious features, we have a low threshold for recalling the patient for targeted diagnostic evaluation, as we demonstrate in some of the cases in this chapter.
Why not bring them all in for US? The use of US to evaluate multiple bilateral masses with benign mammographic features yields frequent false-positive findings. As a group, these women do not appear to be at increased risk for developing breast cancer. In women with fibrocystic changes, complicated cysts or complex masses are frequently detected. Benign solid masses, which also frequently occur in these patients, often have indeterminate sonographic features. A degenerating fibroadenoma may have shadowing on US. When masses other than simple cysts are identified by US, they often prompt a recommendation for aspiration, biopsy, or short-term follow-up studies. In addition, when a mass is seen by US, it may be difficult or impossible to identify a corresponding mammographic finding with certainty, unless a localizing intervention is performed.
What Is the Evidence?
There is strong support in the literature, when certain criteria are met, to consider multiple bilateral masses benign, even when there are no previous mammograms for comparison. Leung and Sickles (2000) studied 1440 women with multiple bilateral masses, with circumscribed margins, whose mammograms were prospectively interpreted as benign, irrespective of the availability of prior mammograms. In fact, no comparison studies were available in almost half of the cases. The interval cancer rate for women with multiple bilateral masses was 0.14%, which is similar to previously reported interval cancer rates for the general population and lower than the incident cancer rate in the United States. In an earlier study (Sickles, 1991), 1 cancer was found at follow-up of 253 women (0.4%) with multiple bilateral well-defined solid masses. In the ACRIN 6666 trial, none of 39 women with multiple bilateral circumscribed masses on mammography had cancer. Likewise, none of 48 women with multiple solid masses with benign features on whole breast US had cancer.
Criteria for Assigning BI-RADS 2 Category to Multiple Masses
Multiple circumscribed masses in one breast do not fulfill the multiplicity rule and cannot be considered benign at screening. Unilateral masses with benign features are still most likely to represent cysts or fibroadenomas, and sometimes papillomas. However, the risk of carcinoma is higher than when the masses are bilateral (Fig. 8-5). Suspicion for malignancy is increased if the masses are in a segmental distribution.

The Masses Must Be Multiple
Because the masses must be bilateral, the minimum number of masses present is three; two in one breast and one in the other breast.
The Margins Must Be Circumscribed
A circumscribed margin is a benign feature. When multiple masses are present, some of the mass margins may be obscured. The BI-RADS lexicon defines “circumscribed” as having at least 75% of the margin visible as circumscribed. If a mass is not obscured and most of the mass is circumscribed but the remainder of the margin is ill defined, irregular, or spiculated, then diagnostic evaluation is needed.
Evaluating Multiple Bilateral Masses
The presence of multiple bilateral masses can often be appreciated on an overview of the case images. Are you finished? Sorry, but no. You can’t use the “Get Out of Jail Free” card until you really look! There is no evidence that the presence of multiple bilateral circumscribed masses reduces the chance that a malignant lesion will also develop. To find her cancer, look for mass features that distinguish one from the others. Next, ignore all those masses and look at everything else. Last, be aware of new or changing clinical findings described by the patient or her health care provider.
Which One of These Is Not Like the Others?
Do you remember playing that game when you were a kid? You had to figure out which of several very similar objects was different. We’ll bet that you were really good at that game because you are a radiologist now!
When multiple bilateral masses are present, their size, shape, density, and margins should be individually examined. Is one mass substantially larger than the others (dominant)? Search for masses that stand out from others, such as those that are very dense, irregular in shape, or have indistinct, microlobulated, or spiculated margins (Figs. 8-6 to 8-8, and Box 8-2). Search for associated suspicious findings such as calcifications, architectural distortion, adenopathy, skin thickening, or nipple retraction.
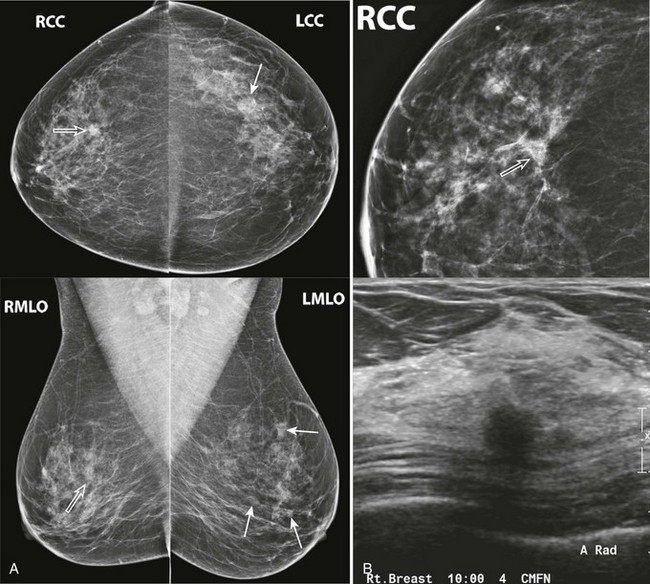
FIGURE 8-6 Multiple Masses with Malignancy.
Screening mammogram of a 40-year-old woman (A). Multiple masses are seen bilaterally (arrows). A right breast mass is dense for its size (open arrow). The patient was recalled and this mass is shown to have spiculated margins on a craniocaudal (CC) spot compression view (open arrow; B, top). US shows a corresponding hypoechoic solid mass with indistinct margins (B, bottom). Two left breast cysts were also seen. Diagnosis: IDC and ductal carcinoma in situ (DCIS) in the right breast.
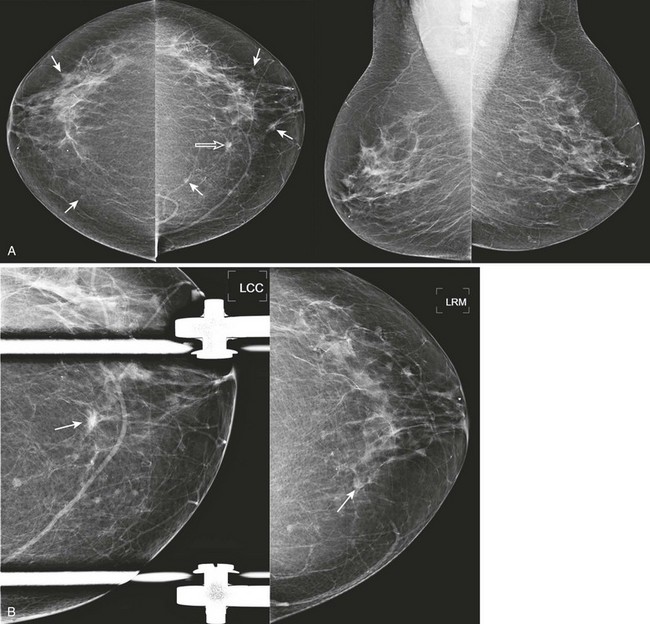
FIGURE 8-7 Multiple Masses and IDC.
Screening mammogram of a 75-year-old woman shows multiple bilateral less-than-1 cm masses (arrows). A, One mass (open arrow), in the medial left breast, is denser than the others and has spiculated margins. B, The appearance remains suspicious on CC spot and CC rolled medial views (arrows). Diagnosis: infiltrating carcinoma with ductal and lobular features and DCIS.
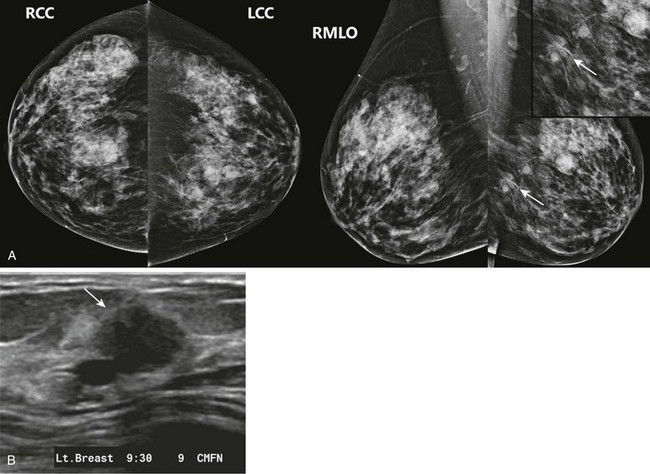
FIGURE 8-8 Multiple Masses and One-View Asymmetry Due to IDC.
A, Screening mammogram on a 64-year-old woman shows multiple bilateral masses. There is an irregular one-view asymmetry in the posterior left breast (arrows). B, US reveals a corresponding solid mass with microlobulated margins (arrow). Multiple cysts were also seen. Core biopsy revealed IDC.
New or Enlarging Masses
When prior mammograms are available, assess how the masses have changed over time. In cases with multiple bilateral circumscribed masses, it is common to observe that some masses are stable while others have decreased or increased in size. Provided the masses have no suspicious characteristics that distinguish them from the others, these cases can still be assigned BI-RADS 2.
Cysts commonly fluctuate in size; they wax and wane (Fig. 8-9). Over half of new cysts will regress within 1 year. After 5 years, about 85% of cysts will either resolve or decrease in size. If a mass has increased dramatically in size, we therefore perform US, even if the patient has a history of cysts.
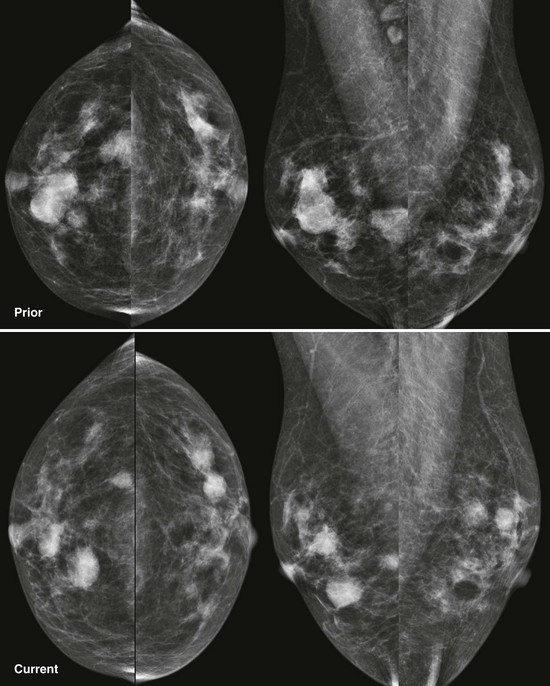
FIGURE 8-9 Waxing and Waning Cysts.
Some masses have enlarged while some have decreased in size. As long as the masses all have benign features and none are dramatically larger, recall is not necessary. This is BI-RADS 2.
Fibroadenomas often enlarge or fluctuate slightly in size in premenopausal women. Aside from the very rapid growth of juvenile fibroadenomas in some young patients, enlarging fibroadenomas usually show fairly gradual increases in size. In postmenopausal women, fibroadenomas regress; it is rare for new fibroadenomas to develop and uncommon for existing fibroadenomas to enlarge. The exception is that fibroadenomas can enlarge significantly in postmenopausal women who are using menopausal hormone therapy.
Because cysts and fibroadenomas account for most multiple bilateral masses, search for findings that do not fit well with these diagnoses (Box 8-3). Look for one mass that has increased rapidly or substantially in size, especially if enlargement has occurred while other masses have been stable or have regressed. These masses warrant diagnostic evaluation. US is also indicated for patients of any age who have not had masses on prior mammograms and now have multiple masses. When new or enlarging masses are shown to be solid or complex by US, biopsy is indicated.
Clinical Factors
History can be very helpful in evaluating multiple bilateral masses. If previous US, aspiration, or biopsy has been performed, these studies should be reviewed. The use of hormone replacement therapy predisposes to cyst formation and enlargement. When there is a history of malignancy, the possibility of bilateral metastatic lesions should be considered.
When a clinically suspicious palpable abnormality develops in a woman with multiple bilateral masses on mammography, it should be evaluated by US even if the mammographic findings are stable. An exception occurs when mammography demonstrates a typically benign lesion, such as a calcified fibroadenoma or hamartoma, which corresponds to the palpable finding.
Key Points
 Multiple masses (a minimum of three masses with at least one mass in each breast) that have benign features, are similar in appearance, and show no suspicious changes from previous studies are considered benign and can be assigned BI-RADS 2.
Multiple masses (a minimum of three masses with at least one mass in each breast) that have benign features, are similar in appearance, and show no suspicious changes from previous studies are considered benign and can be assigned BI-RADS 2.
If any of the masses appear different from the others (dominant in size, higher density) or have suspicious features (ill-defined margin, associated concerning calcifications), then further evaluation should be considered.
The presence of multiple masses makes these mammograms more complex. After looking at the masses, force yourself to look at everything else to identify other abnormalities such as calcifications or architectural distortion.
At follow-up, BI-RADS 2 can still be used if some or all of the masses are a little bigger. If one mass is enlarging while the rest are stable or regressing, recall should be considered.
Berg, WA, Zhang, A, Adams, A, Mendelson, E. Multiple Bilateral Similar Findings on Mammography: Results of ACRIN 6666 Trial. Presented at Radiological Society of North America Meeting. 2010.
Berg, WA, Zhang, A, Adams, A, Mendelson, E. Multiple Bilateral Similar Masses on Ultrasound: Results of ACRIN 6666 Trial. Presented at Radiological Society of North America Meeting. 2010.
Brenner, RJ, Bein, ME, Sarti, DA, Vinstein, AL. Spontaneous regression of interval benign cysts of the breast. Radiology. 1994;193:365–368.
Cardenosa, G, Eklund, GW. Benign pap illary neoplasms of the breast: Mammographic findings. Radiology. 1991;181:751–755.
Chung, SY, Oh, KK. Imaging findings of metastatic disease to the breast. Yonsei Med J. 2001;42:497–502.
Fornage, BD, Lorigan, JG, Andry, E. Fibroadenoma of the breast: Sonographic appearance. Radiology. 1989;172:671–675.
Gordon, PB, Gagnon, FA, Lanzkowsky, L. Solid breast masses diagnosed as fibroadenoma at fine-needle aspiration biopsy: Acceptable rates of growth at long-term follow-up. Radiology. 2003;229:233–238.
Kopans, D. Breast Imaging, 2nd ed. Philadelphia: Lippincott Williams & Wilkins; 1998.
Leung, JW, Sickles, EA. Multiple bilateral masses detected on screening mammography: Assessment of the need for recall imaging. AJR. 2000;175:23–29.
Liberman, L, Giess, CS, Dershaw, DD, et al. Non-Hodgkin lymphoma of the breast: Imaging characteristics and correlation with histopathologic findings. Radiology. 1994;192:157–160.
McCrae, ES, Johnston, C, Haney, PJ. Metastases to the breast. AJR. 1983;141:685–690.
Meyer, JE, Frenna, TH, Polger, M, et al. Enlarging occult fibroadenomas. Radiology. 1992;183:639–641.
Mitnick, JS, Vazquez, MF, Harris, MN, et al. Invasive papillary carcinoma of the breast: Mammographic appearance. Radiology. 1990;177:803–806.
Muttarak, M, Lerttumnongtum, P, Chaiwun, B, Peh, WCG. Spectrum of papillary lesions of the breast: Clinical, imaging, and pathologic correlation. AJR. 2008;191:700–707.
Rahbar, G, Die, AC, Hansen, GC, et al. Benign versus malignant solid breast masses: US differentiation. Radiology. 1999;213:889–894.
Sickles, EA. Periodic mammographic follow-up of probably benign lesions: Results in 3,184 consecutive cases. Radiology. 1991;179:463–468.
Toombs, BD, Kalisher, L. Metastatic disease to the breast: Clinical, pathologic, and radiographic features. AJR. 1977;129:673–676.
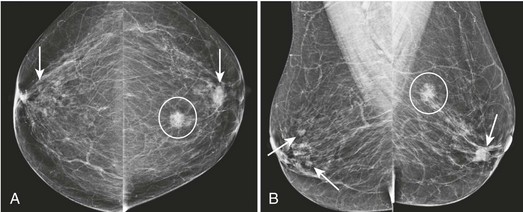
CASE 8-1. A 40-year-old woman has her first screening mammogram. What are the findings? What BI-RADS category would you assign?
CASE 8-2. Screening mammogram of a 55-year-old woman. What are the findings? What is your BI-RADS assessment? The right clip is from previous core biopsy of a benign mass.
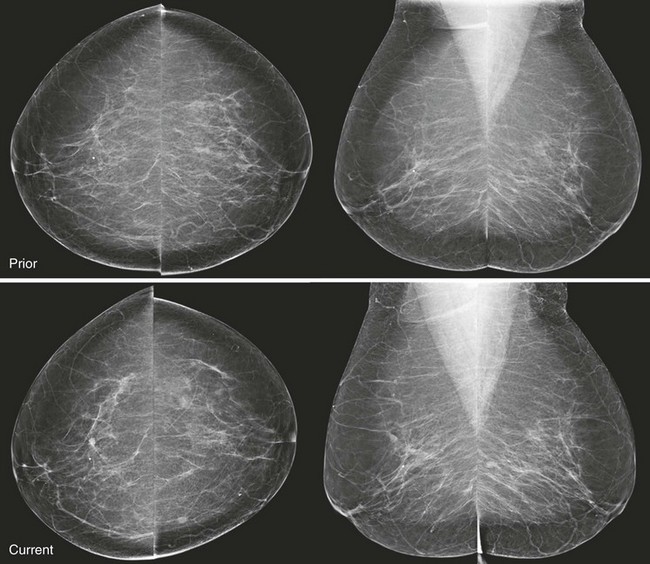
CASE 8-3. Screening mammogram on a 55-year-old woman. On comparison with previous mammograms, some of the masses were bigger and some were smaller. Can the rule of multiplicity be applied? What is the most likely cause of the findings? BI-RADS assessment?
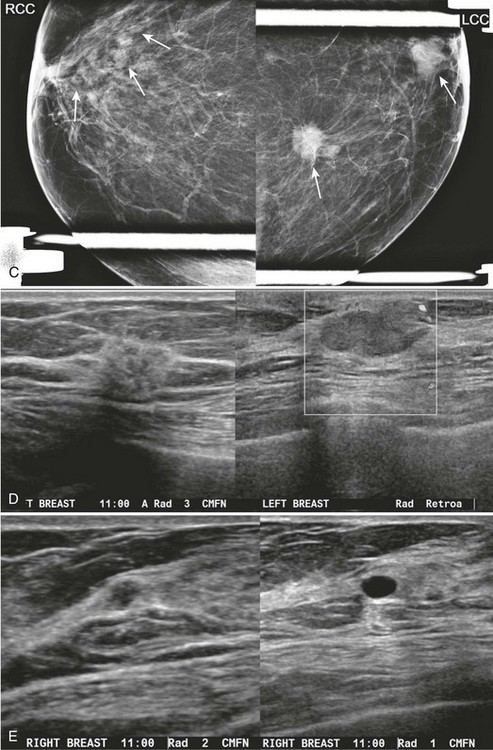
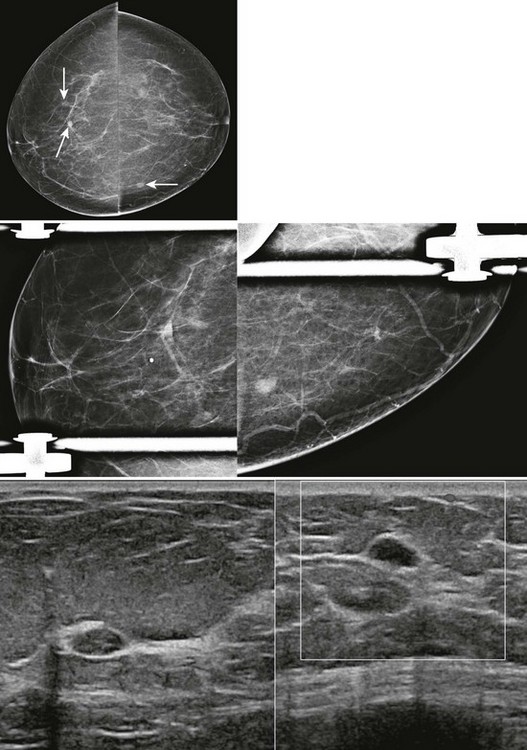
CASE 8-4. Screening mammogram of a 62-year-old woman. No previous mammograms are available. What are the significant findings? What management do you recommend? Can the rule of multiplicity be applied?
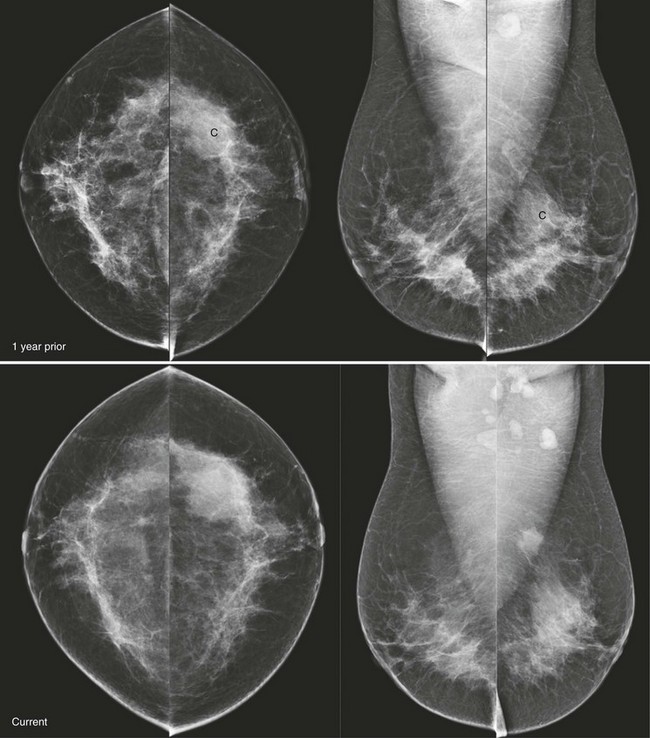
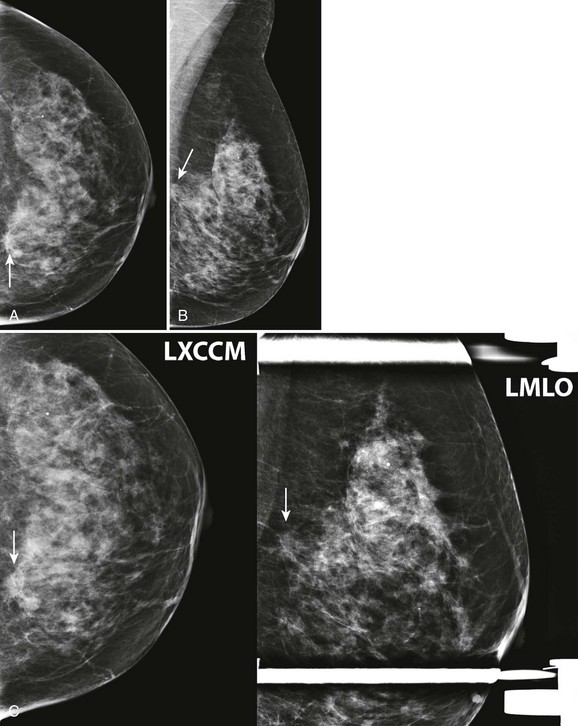
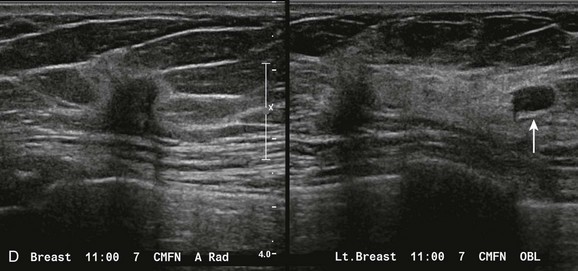
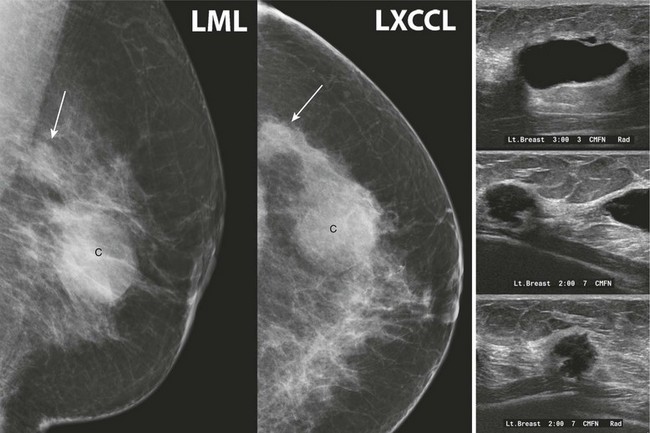
CASE 8-5. Screening mammogram of a 49-year-old woman with a comparison study from 1 year prior. A left breast cyst (C) was diagnosed by previous US. Can the rule of multiplicity be applied? What do you recommend?
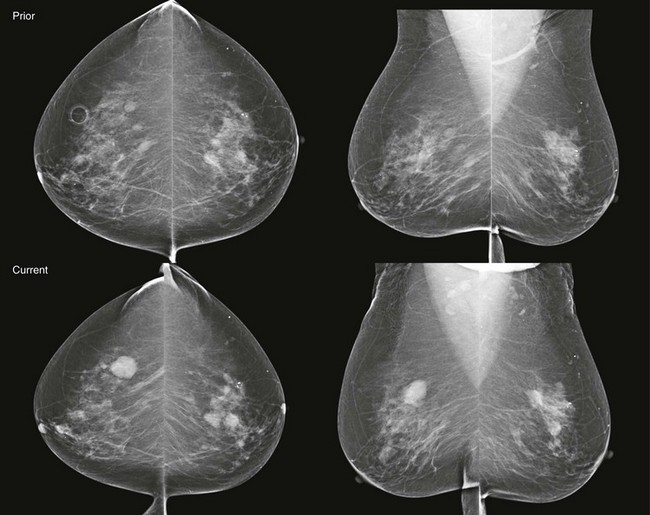
CASE 8-6. A screening mammogram on an 80-year-old woman is compared with a previous mammogram from 1 year ago. The patient has a history of multiple bilateral cysts diagnosed by US and core biopsy of a left breast mass revealing fibroadenoma. Can the rule of multiplicity be applied?
CASE 8-7. Screening mammogram of a 72-year-old woman with a history of lumpectomy and radiation therapy for right breast carcinoma. What are the findings? What do you recommend?

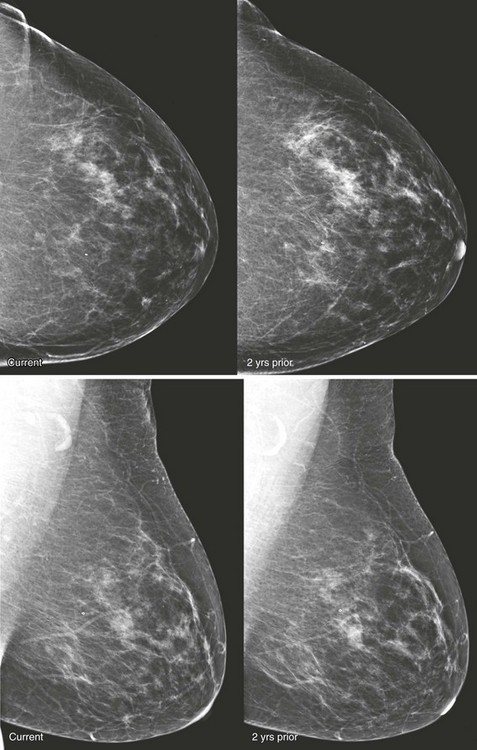
CASE 8-8. Screening mammogram on a 68-year-old woman with a comparison study from 2 years prior. What are the findings? What are your BI-RADS assessment and recommendation?
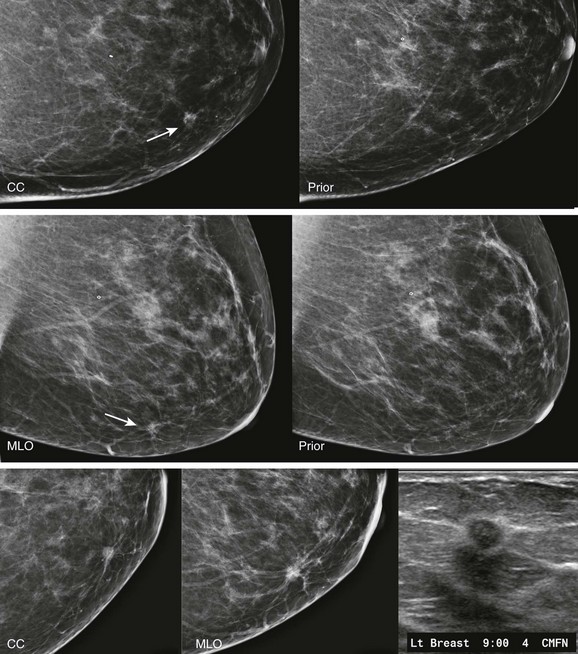
CASE 8-9. A 41-year-old woman with a history of bilateral cysts had screening mammography performed 2 months ago that showed extremely dense tissue with multiple bilateral benign-appearing masses. There were no suspicious findings (BI-RADS 2).
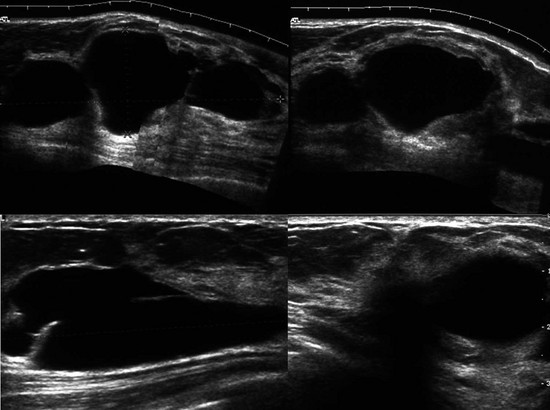
She now presents with a new palpable mass in her upper right breast and is referred for US. Your sonographer brings you the following images from the palpable region. What do you recommend?
CASE 8-10. Screening mammogram showing the left breast of a 64-year-old woman. There are known multiple bilateral masses. The clip is from remote benign core biopsy. What significant change has occurred since the previous study?
CASE 8-1. There are multiple bilateral similar-appearing masses with benign features. There are coarse fibroadenomatous calcifications within masses in each breast, and the remaining masses most likely represent fibroadenomas as well. These findings are benign (BI-RADS 2), and the patient can be recommended for annual screening mammography.
CASE 8-2. The tissue is heterogeneously dense, and there are multiple bilateral masses. There is an irregular focal asymmetry in the posterior medial left breast (arrows; A and B). BI-RADS 0. Recommend diagnostic views and ultrasonography.
On diagnostic views a spiculated mass is confirmed in the retroglandular fat (arrows; C). US shows a corresponding irregular hypoechoic mass with indistinct margins (D). An adjacent oval hypoechoic circumscribed mass is also seen (arrow). Core biopsy of the irregular mass revealed invasive lobular carcinoma with pleomorphic features. Core biopsy of the circumscribed mass showed fat necrosis and LCIS.
CASE 8-3. There are multiple bilateral similar-appearing masses. No single mass is more suspicious than the others. Fluctuation in size is usually indicative of cysts. Yes, we can use the rule of multiplicity. The findings are considered benign (BI-RADS 2).
CASE 8-4. There are two masses in the left breast (upper inner quadrant and subareolar) and at least two much smaller masses in the anterior right breast (arrows; A and B). The rule of multiplicity cannot be applied because the 11 o’clock mass on the left has spiculated margins (circle).
These findings are better seen on spot compression views (arrows; C). US of the left breast reveals a mass with indistinct margins in the 11 o’clock position and a circumscribed mass in the subareolar region (D). US of the anterior right breast shows one hypoechoic solid mass with indistinct margins and one simple cyst (E).
Diagnoses: Left breast: 11 o’clock mass, IDC and DCIS; left subareolar mass, infiltrating carcinoma with mucinous features. Right breast: 11 o’clock mass, multifocal DCIS.
CASE 8-5. There are two masses in the left breast, including the previously documented cyst (C), which has obscured margins. The more posterior mass is excluded from the screening CC view but is confirmed on the exaggerated craniocaudal lateral (XCCL) and mediolateral views (arrows). It has enlarged since the previous mammogram.
The rule of multiplicity should not be applied. The masses are unilateral. The posterior left breast mass has suspicious features (irregular shape, indistinct margins) and has clearly enlarged. There is a dense left axillary lymph node. US shows the known cyst and an adjacent, irregular hypoechoic mass, which was biopsied. Diagnosis: IDC grade 2.
CASE 8-6. There are multiple bilateral masses. However, the findings cannot be considered benign because one mass, in the upper-outer quadrant of the right breast (arrows), has enlarged markedly since the previous mammogram and, therefore, warrants diagnostic evaluation. US shows an oval, circumscribed, solid mass with parallel orientation in the 10 o’clock position. Biopsy is indicated because of the rapid enlargement of the mass. Core biopsy revealed benign phyllodes tumor associated with lobular carcinoma in situ with the same diagnosis at excision.

CASE 8-7. There is postsurgical deformity of the anterior right breast. Multiple masses are present in the right breast. Some of the masses (arrows) have indistinct margins. The findings are suspicious for recurrent carcinoma. Diagnostic views and US are recommended.
Magnification views confirm multiple masses, one with spiculated margins (arrow). US reveals three solid masses. Core biopsies of two masses both revealed IDC and DCIS.

CASE 8-8. There are at least three new bilateral isodense masses with circumscribed margins (arrows). There were no masses on prior mammograms; therefore, diagnostic views and US were performed. CC spot compression views show circumscribed margins. US reveals bilateral oval solid masses. Core biopsy of masses in the 12 o’clock position of the right breast and the 10 o’clock position of the left breast both revealed previously unsuspected extranodal marginal zone B-cell lymphoma.
CASE 8-9. There are multiple cysts. Did you notice the hypoechoic shadowing region on the lower right image? You rescan this region and find a hypoechoic solid shadowing mass with spiculated margins, adjacent to cysts. This is highly suspicious. Diagnosis: IDC.
CASE 8-10. There are multiple masses. One, in the lower inner quadrant of the breast, stands out from the others (arrow). It is irregular in shape and has enlarged.
Spot compression views and US were performed. The mass has spiculated margins. US shows a round mass with an echogenic halo. These features are highly suspicious (BI-RADS 5). Diagnosis: IDC.