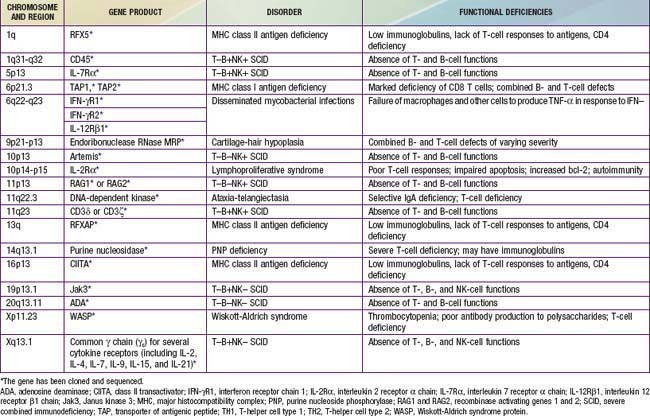
Chapter 120 Primary Combined Antibody and Cellular Immunodeficiencies
Patients with combined antibody and cellular defects have severe, frequently opportunistic infections that lead to death in infancy or childhood unless they are provided hematopoietic stem cell transplantation early in life. These are thought to be rare defects, although the true incidences are unknown because there has been no newborn screening for any of these defects. It is possible that many affected children die of infection during infancy without being diagnosed. The defective gene products for many combined immunodeficiencies are identified (Table 120-1). Because life threatening infection may occur in infancy, screening for SCID has been recommended by the U.S. Secretary of Health and Human Services to be included in the state newborn screening programs. Live, vaccine-derived infections have occurred during this time of life and knowledge of SCID status could prevent these infections. In addition, early identification and subsequent bone marrow transplantation before life-threatening infections and end organ injury is the best approach to therapy.
120.1 Severe Combined Immunodeficiency (SCID)
The syndromes of SCID are caused by diverse genetic mutations that lead to absence of all adaptive immune function and, in some, a lack of natural killer (NK) cells. Patients with this group of disorders have the most severe immunodeficiency.
Pathogenesis
SCID results from mutations in any 1 of 13 known genes that encode components of the immune system crucial for lymphoid cell development (Table 120-2). All patients with SCID have very small thymuses (<1 g) that usually fail to descend from the neck, contain no thymocytes, and lack corticomedullary distinction or Hassall corpuscles. The thymic epithelium appears histologically normal. Both the follicular and paracortical areas of the spleen are depleted of lymphocytes. Lymph nodes, tonsils, adenoids, and Peyer patches are absent or extremely underdeveloped.
Table 120-2 PATHOPHYSIOLOGY MECHANISMS THAT ACCOUNT FOR SEVERE COMBINED IMMUNE DEFICIENCY (SCID)
| DISEASE MECHANISM | GENE DEFECTS |
|---|---|
| Increased apoptosis | |
| • Due to mitochondrial energy failure | AK2 |
| • Due to accumulation of toxic metabolites | ADA |
| • Due to abnormal actin polymerization | CORO1A |
| Impaired cytokine-mediated signaling | |
| • Due to defects of the common γ chain | IG2RG (X-linked SCID) |
| • Due to defects of the IL-7R α chain | IL7R |
| • Due to defects of Jak3 | JAK3 |
| Impaired signaling through the pre–T cell receptor | |
| • Due to defective V(D)J recombination | RAG1, RAG2, DCLRE1C, LIG4,* PRKDC |
| • Due to impaired expression of CD3 subunits | CD3D, CD3E, CD3Z |
| Impaired signaling in the periphery | ORA1 |
| Unknown mechanism | RMRP* |
* These gene defects are most often associated with a milder clinical phenotype than SCID.
From Pessach I, Walter J, Notarangelo LD: Recent advances in primary immunodeficiencies: identification of novel genetic defects and unanticipated phenotypes, Pediatr Res 65:3R–12R, 2009.
Clinical Manifestations
Affected infants present within the 1st few months of life with recurrent or persistent diarrhea, pneumonia, otitis media, sepsis, and cutaneous infections. Growth may appear normal initially, but extreme wasting usually ensues after diarrhea and infections begin. Persistent infections with opportunistic organisms including Candida albicans, Pneumocystis jiroveci, parainfluenza 3 virus, adenovirus, respiratory syncytial virus, rotavirus vaccine virus, cytomegalovirus (CMV), Epstein-Barr virus (EBV), varicella-zoster virus, measles virus, MMR-V vaccine virus, or bacillus Calmette-Guérin (BCG) lead to death. Affected infants also lack the ability to reject foreign tissue and are therefore at risk for severe or fatal graft versus host disease (GVHD) from T lymphocytes in nonirradiated blood products or in allogeneic stem cell transplants or less severe GVHD from maternal immunocompetent T cells that crossed the placenta while the infant was in utero.
Because all molecular types of SCID lack T cells, infants with SCID have lymphopenia (<2,500/mm3) that is present at birth, indicating that the condition could be diagnosed in all affected infants if white blood cell counts with manual differential counts were routinely performed on all cord bloods and the absolute lymphocyte count calculated. These infants also have an absence of lymphocyte proliferative responses to mitogens, antigens, and allogeneic cells in vitro. Patients with adenosine deaminase (ADA) deficiency have the lowest absolute lymphocyte counts, usually <500/mm3. Serum immunoglobulin concentrations are low or absent, and no antibodies are formed after immunizations. Analyses of lymphocyte populations and subpopulations demonstrate distinctive phenotypes for the various genetic forms of SCID (see Table 120-2). T cells are extremely low or absent in all types; when detected, in most cases they are transplacentally derived maternal T cells.
Treatment
SCID is a true pediatric emergency. Unless immunologic reconstitution is achieved through stem cell transplantation, death usually occurs during the 1st yr of life and almost invariably before 2 yr of age. If diagnosed at birth or within the 1st 3.5 mo of life, >94% of cases can be treated successfully with HLA-identical or T-cell–depleted haploidentical (half-matched) parental hematopoietic stem cell transplantation without the need for pretransplant chemoablation or post-transplant GVHD prophylaxis. ADA-deficient SCID and X-linked SCID have been treated with somatic gene therapy; although serious adverse events occurred in the case of X-SCID. These successes offer hope for gene therapy eventually becoming the treatment of choice for all forms of SCID for which the gene has been identified. ADA-deficient SCID is also managed with repeated injections of polyethylene glycol modified bovine adenosine deaminase (PEG-ADA).
X-Linked Severe Combined Immunodeficiency (SCIDX1) Due To Mutations in the Gene Encoding the Common Cytokine Receptor γ Chain (γC)
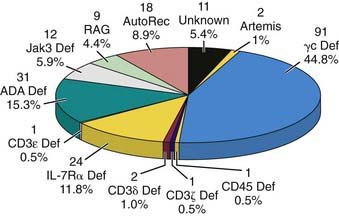
X-linked SCID (X-SCD) is the most common form of SCID in the USA, accounting for 47% of cases (Fig. 120-1). Clinically, immunologically, and histopathologically, affected individuals appear similar to those with other forms of SCID except for having uniformly low percentages of T and NK cells and an elevated percentage of B cells (T−, B+, NK−), a characteristic feature shared only with Janus kinase 3 (Jak3)–deficient SCID. The abnormal gene in X-SCD was mapped to Xq13, cloned, and found to encode the common γ chain (γc) for several cytokine receptors, including IL-2, IL-4, IL-7, IL-9, IL-15, and IL-21. The shared γc functions both to increase the affinity of the receptor for the respective cytokine and to enable the receptors to mediate intracellular signaling. Incapacitation of the receptors for all of these developmentally crucial cytokines by genetic mutations in γc provides an explanation for the severity of the immunodeficiency in SCIDX1. In the 1st 136 patients studied, 95 distinct mutations spanning all 8 IL2RG exons were identified, most of them consisting of small changes at the level of 1 to a few nucleotides. These mutations resulted in abnormal γc chains in two thirds of the cases and absent γc protein in the remainder. Carriers can be detected by demonstrating nonrandom X-chromosome inactivation or the deleterious mutation in their T, B, or NK lymphocytes. Unless donor B or NK cells develop, patients with X-SCID lack B- and NK-cell function after bone marrow transplantation because the abnormal γc persists in those host cells, despite excellent reconstitution of T-cell function by donor-derived T cells.
Autosomal Recessive Severe Combined Immunodeficiency
This pattern of inheritance of SCID is less common in the USA than in Europe. Mutated genes on autosomal chromosomes have been identified in 12 forms of SCID: ADA deficiency; Jak3 deficiency; IL-7 receptor α chain (IL-7Rα) deficiency; RAG1 or RAG2 deficiency; Artemis deficiency; ligase 4 deficiency; DNA–protein kinase catalytic subunit (DNA-PKcs) deficiency; CD3δ, CD3ε, CD3ζ deficiency; and CD45 deficiency (see Fig. 120-1).
ADA Deficiency
An absence of the enzyme adenosine deaminase (ADA) is observed in approximately 15% of patients, the second most common form of SCID, resulting from various point and deletional mutations in the ADA gene on chromosome 20q13-ter. Marked accumulations of adenosine, 2′-deoxyadenosine, and 2′-O-methyladenosine lead directly or indirectly to T-cell apoptosis, which causes the immunodeficiency. ADA-deficient patients usually have a much more profound lymphopenia than do infants with other types of SCID, with mean absolute lymphocyte counts of <500/mm3; the absolute numbers of T, B, and NK cells are very low. NK function is normal. After T-cell function is conferred by hematopoietic stem cell transplantation without pretransplant chemotherapy, there is generally excellent B-cell function despite the fact that the B cells are of host origin. This is because ADA deficiency affects primarily T-cell function. Milder forms of ADA deficiency have led to delayed diagnosis of immunodeficiency, even to adulthood. Other distinguishing features of ADA-deficient SCID include the presence of rib cage abnormalities similar to a rachitic rosary and numerous skeletal abnormalities of chondro-osseous dysplasia, which occur predominantly at the costochondral junctions, at the apophyses of the iliac bones, and in the vertebral bodies where a “bone-in-bone” effect is observed.
As with other types of SCID, ADA deficiency can be cured by HLA-identical or haploidentical T-cell–depleted stem cell transplantation without the need for pre- or post-transplant chemotherapy; this remains the treatment of choice. Enzyme replacement therapy should not be initiated if stem cell transplantation is possible because it confers graft-rejection capability. Enzyme replacement provides protective immunity but over time there is a decline of lymphocyte counts and mitogenic proliferative responses. Fifteen infants with ADA deficiency have become immune reconstituted by gene therapy; in all cases, PEG-ADA was withheld. Spontaneous reversion to normal of a mutation in the ADA gene has also been reported.
Jak3 Deficiency
Patients with this autosomal recessive defect resemble all other types of SCID patients clinically. They have a lymphocyte phenotype similar only to that of patients with X-SCID, with an elevated percentage of B cells and very low or no T and NK cells. Because Jak3 is the only signaling molecule known to be associated with γc, it was a candidate gene for mutations leading to autosomal recessive SCID. Jak3 deficiency accounts for 6% of SCID cases. Even after successful T-cell reconstitution by transplantation of haploidentical stem cells, patients with Jak3-deficient SCID fail to develop NK cells or normal B-cell function owing to the defective function of those host cells that bear abnormal cytokine receptors that share γc.
IL-7Rα Deficiency
Patients with IL-7Rα-deficient SCID have a distinctive lymphocyte phenotype in that, though lacking T cells, they have normal or elevated numbers of both B and NK cells (T−, B+, NK+). This is the third most common form of SCID, accounting for 12% of cases in the USA (see Fig. 120-1). In contrast to patients with γc- and Jak3-deficient SCID, the immunologic defect in these patients is completely correctable by bone marrow stem cell transplantation, as the host B and NK cells appear to be normal.
RAG1 or RAG2 Deficiencies
Infants with these causes of SCID have a different lymphocyte phenotype from those of patients with SCID due to γc, Jak3, IL-7Rα, or ADA deficiencies in that they lack both B and T lymphocytes and have primarily NK cells in their circulation (T−, B−, NK+). This suggested a problem with their antigen receptor genes, which led to the discovery of mutations in recombinase-activating genes, RAG1 or RAG2. Such mutations result in a functional inability to form antigen receptors through genetic recombination. Omenn syndrome is an autosomal recessive, fatal condition characterized by profound susceptibility to infection with clonal T-cell infiltration of skin, intestines, liver, and spleen leading to an exfoliative erythroderma, lymphadenopathy, hepatosplenomegaly, and intractable diarrhea. Mutations in the recombinase activating genes, RAG1 and RAG2, have also been found in patients with this condition. These infants have persistent leukocytosis with marked eosinophilia and lymphocytosis; elevated serum IgE; low IgG, IgA, and IgM; and low or absent B cells. There is dominance of clonal TH2-like cells with severely impaired T-cell function due to the restricted heterogeneity of the host T-cell repertoire.
Artemis Deficiency
Another cause of SCID is a deficiency of a novel V(D)J recombination/DNA repair factor that belongs to the metallo-β-lactamase superfamily, which is encoded on chromosome 10p by a gene called Artemis. Deficiency of this factor results in an inability to repair DNA after double-stranded cuts by the RAG1 or RAG2 gene products in rearranging antigen receptor genes from their germ line configuration. Similar to RAG1- and RAG2-deficient SCID, this defect results in failure to develop T and B cells and is, therefore, another form of T−, B−, NK+ SCID, also called Athabascan SCID. There is increased radiation sensitivity of both skin fibroblasts and bone marrow cells of those affected with this type of SCID as well as with DNA-PKcs deficiency.
CD45 Deficiency
Other molecular defects causing SCID are mutations in the gene encoding the common leukocyte surface protein CD45. This hematopoietic cell–specific transmembrane protein tyrosine phosphatase functions to regulate src kinases required for T- and B-cell antigen receptor signal transduction. A 2 mo old male infant presented with a clinical picture of SCID and was found to have a very low number of T cells but a normal number of B cells. The T cells failed to respond to mitogens, and serum immunoglobulins diminished with time. He was found to have a large deletion on 1 CD45 allele and a point mutation causing an alteration of the intervening sequence 13 donor splice site on the other allele. A 2nd case of SCID due to CD45 deficiency has been reported, and the author has evaluated and treated a 3rd case.
CD3δ, CD3ε, and CD3ζ Deficiencies
Other causes of autosomal recessive SCID are deficiencies of components of the T-cell receptor (CD3δ, CD3ε, and CD3ζ chains). Mutations in the portions of these genes that encode the extracellular components of the proteins result in a profound deficiency of circulating mature CD3 T cells. Thus, CD3δ, CD3ε, and CD3ζ appear to be essential for intrathymic development of T cells. Since only T-cell development is affected in these defects, both B and NK cells are normal. Thus, the lymphocyte phenotype resembles that of SCID infants with IL-7Rα chain deficiency (T−B+NK+).
Reticular Dysgenesis
Reticular dysgenesis was 1st described in identical twin boys who exhibited a total lack of both lymphocytes and granulocytes in their peripheral blood and bone marrow. Of 8 infants with this defect, 7 died between 3 and 119 days of age as a result of overwhelming infections; 7 infants have been cured by bone marrow transplantation. The thymus glands have all weighed <1 g, have no Hassall corpuscles, and have few or no thymocytes. Reticular dysgenesis is considered a variant of SCID. The molecular basis of this autosomal recessive disorder has recently been found to be due to mutations in the gene encoding adenylate kinase 2.
120.2 Combined Immunodeficiency (CID)
CID is distinguished from SCID by the presence of low but not absent T-cell function. Similar to SCID, CID is a syndrome of diverse genetic causes. Patients with CID have recurrent or chronic pulmonary infections, failure to thrive, oral or cutaneous candidiasis, chronic diarrhea, recurrent skin infections, gram-negative bacterial sepsis, urinary tract infections, and severe varicella in infancy. Although they usually survive longer than infants with SCID, they fail to thrive and die early in life. Neutropenia and eosinophilia are common. Serum immunoglobulins may be normal or elevated for all classes, but selective IgA deficiency, marked elevation of IgE, and elevated IgD levels occur in some cases. Although antibody-forming capacity is impaired in most patients, it is not absent.
Studies of cellular immune function show lymphopenia, profound deficiencies of T cells, and extremely low but not absent lymphocyte proliferative responses to mitogens, antigens, and allogeneic cells in vitro. Peripheral lymphoid tissues demonstrate paracortical lymphocyte depletion. The thymus is very small with a paucity of thymocytes and usually no Hassall corpuscles. An autosomal recessive pattern of inheritance is common.
Purine Nucleoside Phosphorylase Deficiency
More than 40 patients with CID have been found to have purine nucleoside phosphorylase (PNP) deficiency. Point mutations identified in the PNP gene on chromosome 14q13.1 account for these deficiencies. In contrast to ADA deficiency, no characteristic physical or skeletal abnormalities have been noted, but serum and urinary uric acid are usually markedly deficient. Deaths result from generalized vaccinia, varicella, lymphosarcoma, or GVHD mediated by allogeneic T cells in nonirradiated blood or bone marrow. Two thirds of patients have neurologic abnormalities, and one third of patients have autoimmune diseases. Lymphopenia is striking, primarily because of a marked deficiency of T cells; T-cell function is decreased to various degrees. The proportion of circulating NK cells is increased. Prenatal diagnosis is possible. Bone marrow transplantation is the only successful form of therapy.
Interleukin 2 Receptor α Chain (IL-2Rα [CD25]) Mutation
An infant boy born of a consanguineous union developed CMV pneumonia, persistent candidiasis, adenoviral gastroenteritis, failure to thrive, lymphadenopathy, hepatosplenomegaly, and chronic inflammation of his lungs and mandible. Biopsy specimens revealed extensive lymphocytic infiltration of his lung, liver, intestines, and bone. Serum IgA level was low. He had T-cell lymphopenia, and the T cells responded poorly to anti-CD3, phytohemagglutinin (PHA) and other mitogens, and IL-2. He was found to have a mutation in the gene encoding the IL-2 receptor α chain (IL-2Rα [CD25]), leading to truncation of the protein. He had no CD1 in his thymus, and an elevation of the anti-apoptotic protein bcl-2. This defect reveals that some components of cytokine receptors normally serve a negative regulatory role. Mutations in those components can result in unchecked lymphoproliferation and autoimmunity in addition to immunodeficiency.
Cartilage Hair Hypoplasia
Cartilage hair hypoplasia (CHH) is an unusual form of short-limbed dwarfism with frequent and severe infections. It occurs predominantly among the Pennsylvania Amish, but non-Amish patients have been described.
Genetics and Pathogenesis
CHH is an autosomal recessive condition. Numerous mutations that co-segregate with the CHH phenotype have been identified in the untranslated RNase MRP gene, which has been mapped to chromosome 9p21-p13 in Amish and Finnish families (see Table 120-1). The RNase MRP endoribonuclease consists of an RNA molecule bound to several proteins and has at least two functions: cleavage of RNA in mitochondrial DNA synthesis and nucleolar cleaving of pre-RNA. Mutations in RMRP cause CHH by disrupting a function of RNase MRP RNA that affects multiple organ systems. In vitro studies show decreased numbers of T cells and defective T-cell proliferation due to an intrinsic defect related to the G1 phase, resulting in a longer cell cycle for individual cells. NK cells are increased in number and function.
Clinical Manifestations
Clinical features include short, pudgy hands; redundant skin; hyperextensible joints of hands and feet but an inability to extend the elbows completely; and fine, sparse, light hair and eyebrows. Severe and often fatal varicella infections, progressive vaccinia, and vaccine-associated poliomyelitis have been observed. Associated conditions include deficient erythrogenesis, Hirschsprung disease, and an increased risk of malignancies. The bones radiographically show scalloping and sclerotic or cystic changes in the metaphyses and flaring of the costochondral junctions of the ribs. Three patterns of immune dysfunction have emerged: defective antibody-mediated immunity, CID (most common), and SCID. The severity of the immunodeficiency varies; in 1 series, 11 of 77 patients died before age 20 yr, but 2 were still alive at age 76 yr. Stem cell transplantation has resulted in immunologic reconstitution in some CHH patients with the SCID phenotype.
Defective Expression of Major Histocompatibility Complex Antigens
The 2 main forms of immunodeficiency and abnormalities of expression of the major histocompatibility complex (MHC) are MHC class I (HLA-A, -B, and -C) antigen deficiency and MHC class II (HLA-DR, -DQ, and -DP) antigen deficiency. The associated defects of both B- and T-cell immunity and of HLA expression emphasize the important biologic role for HLA determinants in effective immune cell cooperation.
MHC Class I Antigen Deficiency
Isolated deficiency of MHC class I (HLA-A, -B, and -C) antigens, the bare lymphocyte syndrome, is rare. The resulting immunodeficiency is much milder than in SCID, contributing to a later age of presentation. Sera from affected children contain normal quantities of MHC class I antigens and β2-microglobulin, but MHC class I antigens are not detected on any cells in the body. There is a deficiency of CD8 but not CD4 T cells. Mutations have been found in 2 genes within the MHC locus on chromosome 6 that encode the peptide transporter proteins TAP1 and TAP2 (see Fig. 118-1). TAP functions to transport antigenic peptides from the cytoplasm across the Golgi apparatus membrane to join the α chain of MHC class I antigens and β2-microglobulin. All these are then assembled into a MHC class I complex that can then move to the cell surface. If the assembly of the complex cannot be completed because there is no antigenic peptide, the MHC class I complex is destroyed in the cytoplasm.
MHC Class II Antigen Deficiency
Many affected with MHC class II (HLA-DR, -DQ, and -DP) deficiency are of North African descent. Patients present in early infancy with persistent diarrhea that is often associated with cryptosporidiosis and enteroviral infections (e.g., poliovirus, coxsackievirus). They also have an increased frequency of infections with herpesviruses and other viruses, oral candidiasis, bacterial pneumonia, P. jiroveci pneumonia, and septicemia. The immunodeficiency is not as severe as in SCID, as evidenced by their failure to develop disseminated infection after BCG vaccination or GVHD from nonirradiated blood transfusions.
Four different molecular defects resulting in impaired expression of MHC class II antigens have been identified (see Table 120-1 and Fig. 118-1). One form is a mutation in the gene on chromosome 1q that encodes a protein called RFX5, a subunit of RFX, which is a multiprotein complex that binds the X box motif of MHC-II promoters. A second form is caused by mutations in a gene on chromosome 13q that encodes a second 36-kD subunit of the RFX complex, called RFX-associated protein (RFXAP). The most common cause of MHC class II defects is mutation in RFXANK, the gene encoding a 3rd subunit of RFX. In a 4th type, there is a mutation in the gene on chromosome 16p13 that encodes a novel MHC class II transactivator (CIITA), a non–DNA-binding co-activator that controls the cell-type specificity and inducibility of MHC-II expression. All 4 of these defects cause impairment in the coordinate expression of MHC class II molecules on the surface of B cells and macrophages.
MHC class II–deficient patients have a very low number of CD4 T cells but normal or elevated numbers of CD8 T cells. Lymphopenia is only moderate. The MHC class II antigens HLA-DP, DQ, and DR are undetectable on blood B cells and monocytes, even though B cells are present in normal number. Patients are hypogammaglobulinemic owing to impaired antigen-specific responses caused by the absence of these antigen-presenting molecules. In addition, MHC antigen-deficient B cells fail to stimulate allogeneic cells in mixed leukocyte culture. Lymphocyte proliferation studies show normal responses to mitogens but no response to antigens. The thymus and other lymphoid organs are severely hypoplastic, and the lack of class II molecules results in abnormal thymic selection with circulating CD4 T cells that have altered CDR3 profiles.
Immunodeficiency with Thrombocytopenia and Eczema (Wiskott-Aldrich Syndrome)
Wiskott-Aldrich syndrome, an X-linked recessive syndrome, is characterized by atopic dermatitis, thrombocytopenic purpura with normal-appearing megakaryocytes but small defective platelets, and undue susceptibility to infection.
Genetics and Pathogenesis
The abnormal gene, on the proximal arm of the X chromosome at Xp11.22-11.23 near the centromere, encodes a 501–amino acid proline-rich cytoplasmic protein restricted in its expression to hematopoietic cell lineages. The Wiskott-Aldrich syndrome protein (WASP) (see Fig. 119-1) binds CDC42H2 and rac, members of the Rho family of guanosine triphosphatases. WASP appears to control the assembly of actin filaments required for microvesicle formation downstream of protein kinase C and tyrosine kinase signaling. Carriers can be detected by nonrandom X-chromosome inactivation in several hematopoietic cell lineages or by demonstration of the deleterious mutation.
Clinical Manifestations
Patients often have prolonged bleeding from the circumcision site or bloody diarrhea during infancy. The thrombocytopenia is not initially due to antiplatelet antibodies. Atopic dermatitis and recurrent infections usually develop during the 1st yr of life. Streptococcus pneumoniae and other bacteria having polysaccharide capsules cause otitis media, pneumonia, meningitis, and sepsis. Later, infections with agents such as P. jiroveci and the herpesviruses become more frequent. Survival beyond the teens is rare; infections, bleeding, and EBV-associated malignancies are major causes of death.
Patients with this defect uniformly have an impaired humoral immune response to polysaccharide antigens, as evidenced by absent or markedly diminished isohemagglutinins, and poor or absent antibody responses after immunization with polysaccharide vaccines. IgG2 subclass concentrations, surprisingly, are normal. Anamnestic responses to protein antigens are poor or absent. There is an accelerated rate of synthesis as well as hypercatabolism of albumin, IgG, IgA, and IgM, resulting in highly variable concentrations of different immunoglobulins, even within the same patient. The predominant immunoglobulin pattern is a low serum level of IgM, elevated IgA and IgE, and a normal or slightly low IgG concentration. Because of their profound antibody deficiencies, these patients should be given monthly infusions of intravenous immunoglobulin (IVIG) regardless of their serum levels of the different immunoglobulin isotypes. Percentages of T cells are moderately reduced, and lymphocyte responses to mitogens are variably depressed.
Treatment
Good supportive care includes appropriate nutrition, routine IVIG, use of killed vaccines, aggressive management of eczema and associated cutaneous infections, platelet transfusion for serious bleeding episodes, splenectomy, and high-dose IVIG with systemic steroids for autoimmune complications. Bone marrow or cord blood transplantation is the treatment of choice and is usually curative.
Ataxia-Telangiectasia
Ataxia-telangiectasia is a complex syndrome with immunologic, neurologic, endocrinologic, hepatic, and cutaneous abnormalities.
Genetics and Pathogenesis
The mutated gene responsible for this defect, ataxia telangiectasia mutation (ATM), was mapped to the long arm of chromosome 11 (11q22-23) and has been cloned (see Fig. 119-1). The gene product is a DNA-dependent protein kinase localized predominantly to the nucleus and involved in mitogenic signal transduction, meiotic recombination, and cell cycle control. Cells from patients as well as those of heterozygous carriers have increased sensitivity to ionizing radiation, defective DNA repair, and frequent chromosomal abnormalities.
In vitro tests of lymphocyte function have generally shown moderately depressed proliferative responses to T- and B-cell mitogens. Percentages of CD3 and CD4 T cells are moderately reduced, with normal or increased percentages of CD8 and elevated numbers of Tiγ/δ T cells. Studies of immunoglobulin synthesis have shown both T-helper-cell and intrinsic B-cell defects. The thymus is very hypoplastic, exhibits poor organization, and lacks Hassall corpuscles.
Clinical Manifestations
The most prominent clinical features are progressive cerebellar ataxia, oculocutaneous telangiectasias, chronic sinopulmonary disease, a high incidence of malignancy, and variable humoral and cellular immunodeficiency. Ataxia typically becomes evident soon after these children begin to walk and progresses until they are confined to a wheelchair, usually by the age of 10-12 yr. The telangiectasias begin to develop at 3-6 yr of age. The most frequent humoral immunologic abnormality is the selective absence of IgA, which occurs in 50-80% of these patients. Hypercatabolism of IgA also occurs. IgE concentrations are usually low, and the IgM may be of the low molecular weight variety. IgG2 or total IgG levels may be decreased, and specific antibody titers may be decreased or normal. Recurrent sinopulmonary infections occur in approximately 80% of these patients. Although common viral infections have not usually resulted in untoward sequelae, fatal varicella has occurred. The malignancies associated with ataxia-telangiectasia are usually of the lymphoreticular type, but adenocarcinomas also occur. Unaffected relatives have an increased incidence of malignancy.
120.3 Defects of Innate Immunity
A number of defects in non–antigen-specific immunity (innate immunity) affect antigen-specific immune responses, as there is interaction between the adaptive and innate immune systems.
Interferon-γ Receptor 1 and 2 and IL-12 Receptor β1 Mutations
Disseminated BCG and other severe nontuberculosis mycobacterial infections (sepsis, osteomyelitis) occur in patients with severe T-cell defects; however, no specific host defect is identified in approximately half of such cases. The 1st report was a 2.5 mo old Tunisian girl with fatal idiopathic disseminated BCG infection; 4 children from Malta had disseminated atypical mycobacterial infections in the absence of a recognized immunodeficiency. There was consanguinity in all, and all had a functional defect in the upregulation of tumor necrosis factor α (TNF-α) production by their blood macrophages in response to stimulation with interferon-γ (IFN-γ). All also had a mutation in the gene on chromosome 6q22-q23 that encodes the IFN-γ receptor 1 (IFN-γR1). IFN-γR1 deficiency may be inherited as a complete autosomal recessive (early onset ≈3 yr of age, more episodes, more severe disease, and higher mortality) or partial dominant (onset ≈10 yr of age) disease. Patients with mutations in the IFN-γR2 have also been identified. A 3rd type of defect was found in other patients who had disseminated mycobacterial infections, who have mutations in the β1 chain of the IL-12 receptor (IL-12Rβ1). IL-12 is a powerful inducer of IFN-γ production by T and NK cells, and the mutated receptor chain gene resulted in unresponsiveness of the cells of these patients to IL-12 and inadequate IFN-γ production. The children deficient in IFN-γR1, IFN-γR2, or IL-12Rβ1 appeared not to be susceptible to infection with many agents other than mycobacteria (occasionally Salmonella, Listeria, Histoplasma). TH1 responses appeared to be normal in these patients, and the susceptibility to mycobacterial infections thus apparently results from an intrinsic impairment of the IFN-γ pathway response to these particular intracellular pathogens, showing that IFN-γ is obligatory for efficient macrophage antimycobacterial activity.
Germ Line Stat 1 Mutation
Interferons induce the formation of 2 transcriptional activators: gamma-activating factor (GAF) and interferon-stimulated gamma factor 3 (ISGF3). A natural heterozygous dominant germ line STAT-1 mutation associated with susceptibility to mycobacterial but not viral disease was found in 2 unrelated patients with unexplained mycobacterial disease. This mutation caused a loss of GAF and ISGF3 activation but was dominant for 1 cellular phenotype and recessive for the other. The mutation impaired the nuclear accumulation of GAF but not of ISGF3 in cells stimulated by interferons, implying that the antimycobacterial but not the antiviral effects of human interferons are mediated by GAF. More recently, 2 patients have been identified with homozygous STAT-1 mutations who developed both post–BCG vaccination disseminated disease and lethal viral infections. The mutations in these patients caused a complete lack of STAT-1 and resulted in a lack of formation of both GAF and ISGF3.
IL-1R–Associated Kinase 4 (IRAK4) Deficiency
Members of interleukin-1 receptor (IL-1R) and the Toll-like receptor (TLR) superfamily share an intracytoplasmic Toll-IL-1 receptor (TIR) domain, which mediates recruitment of the interleukin-1 receptor-associated kinase (IRAK) complex via TIR-containing adapter molecules. Three unrelated otherwise healthy children with recurrent pyogenic infections due to pneumococci and staphylococci had normal immunocompetence by standard immune studies. They had normal titers of anti-pneumococcal antibodies. Their blood and fibroblast cells did not activate nuclear factor κB (NF-κB), and mitogen-activated protein kinase (MAPK) and failed to induce downstream cytokines in response to any of the known ligands of TIR-bearing receptors. All were found to have an inherited deficiency of IRAK-4. The TIR-IRAK signaling pathway appears to be crucial for protective immunity against specific bacteria but is redundant against most other microorganisms.
Hyper-IgE Syndrome
The hyper-IgE syndrome is a relatively rare primary immunodeficiency syndrome characterized by recurrent severe staphylococcal abscesses of the skin, lungs, and other viscera as well as sinusitis, mastoiditis, and markedly elevated levels of serum IgE (Table 120-3). C. albicans is the second most common pathogen. More than 200 patients with hyper-IgE syndrome have been reported. The most common form of this condition (autosomal dominant) is now known to be caused by mutations in the gene encoding STAT-3. These mutations result in a dominant negative effect on the expression of STAT-3 by the other nonmutated gene. Rarely, autosomal recessive forms of the hyper-IgE syndrome have been reported, mainly in Turkey, and a mutation in the gene encoding Tyk2 was found in one such patient but not in the others.
Table 120-3 CLINICAL FEATURES OF AUTOSOMAL DOMINANT HYPER IgE SYNDROME (AD-HIES)
IMMUNOLOGIC (APPROXIMATE % FREQUENCY)
SOMATIC (APPROXIMATE % FREQUENCY)
From Freeman AF, Holland SM: Clinical manifestations, etiology, and pathogenesis of the hyper-IgE syndromes, Pediatr Res 65:32R–37R, 2009.
Clinical Manifestations
The characteristic clinical features of the autosomal dominant form of the hyper-IgE syndrome are staphylococcal abscesses, pneumatoceles, osteopenia, and unusual facial features. There is often history from infancy of recurrent staphylococcal abscesses involving the skin, lungs, joints, and other sites. Persistent pneumatoceles develop as a result of recurrent pneumonia. The pruritic dermatitis that occurs is not typical atopic eczema and does not always persist. Allergic respiratory symptoms are usually absent. The 1st 2 reported patients were described as having coarse facial features, including a prominent forehead, deep-set wide-spaced eyes, a broad nasal bridge, a wide fleshy nasal tip, mild prognathism, facial asymmetry, and hemihypertrophy. In older children, delay in shedding primary teeth, recurrent fractures, and scoliosis occur.
These patients demonstrate an exceptionally high serum IgE concentration; an elevated serum IgD concentration; usually normal concentrations of IgG, IgA, and IgM; pronounced blood and sputum eosinophilia; abnormally low anamnestic antibody responses; and poor antibody and cell-mediated responses to neoantigens. In vitro studies show normal percentages of blood T, B, and NK lymphocytes, with the exception of a decreased percentage of T cells with the memory (CD45RO) phenotype. Recently, several laboratories have reported that there is an absence or deficiency of TH17 T cells. The latter cells produce IL-17, a cytokine that acts on monocytes to induce secretion of proinflammatory mediators such as IL-8, TNF, and GM-CSF. It is not clear exactly how the STAT3 mutation causes all parts of the syndrome, but it is thought that the IL-17 deficiency may account in part for the susceptibility to infection. Most patients have normal T-lymphocyte proliferative responses to mitogens but very low or absent responses to antigens or allogeneic cells from family members. Blood, sputum, and histologic sections of lymph nodes, spleen, and lung cysts show striking eosinophilia. Hassall corpuscles and thymic architecture are normal. Phagocytic cell ingestion, metabolism, killing, and total hemolytic complement activity are normal in all patients, and results of chemotaxis studies have been mostly normal.
Autosomal recessive hyper-IgE syndrome presents with recurrent viral infections such as molluscum contagiosum, herpes zoster, and herpes simplex infections, in addition to staphylococcal skin infections. Other features that distinguish this form from the autosomal dominant form include frequent central nervous system abnormalities and vasculitis, a higher mortality, a lack of tendency to pneumatocele formation, delayed shedding of the primary teeth, or osteopenia. Distinctive laboratory findings in the autosomal recessive form include poor T-cell responses to mitogens and absent responses to antigens.
The most effective therapy for the hyper-IgE syndrome is long-term administration of therapeutic doses of a penicillinase-resistant antistaphylococcal antibiotic, adding other agents as required for specific infections. IVIG should be administered to antibody-deficient patients, and appropriate thoracic surgery should be provided for superinfected pneumatoceles or those persisting beyond 6 mo. Bone marrow transplantation has been unsuccessful in this condition.
120.4 Treatment of Cellular or Combined Immunodeficiency
Good supportive care including prevention and treatment of infections is critical while patients await more definitive therapy (Table 120-4). Having knowledge of the pathogens causing disease with specific immune defects is also useful (see Table 120-4).
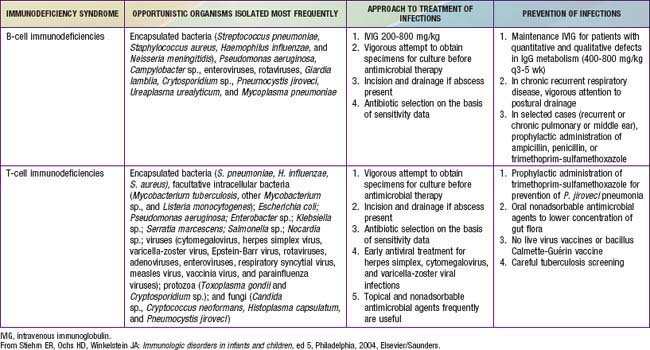
Transplantation of MHC-compatible sibling or haploidentical (half-matched) parental hematopoietic stem cells is the treatment of choice for patients with fatal T-cell or combined T- and B-cell defects. The major risk to the recipient from transplants of bone marrow or peripheral blood stem cells is GVHD. The development of techniques to deplete all post-thymic T cells from donor marrow permits safe and successful use of haploidentical related donor stem cells for the correction of SCID and other fatal immunodeficiency syndromes. Patients with less severe forms of cellular immunodeficiency, including some forms of CID, Wiskott-Aldrich syndrome, cytokine deficiency, and MHC antigen deficiency, reject even HLA-identical marrow grafts unless chemoablative treatment is given before transplantation. Several patients with these conditions have been treated successfully with HLA-identical stem cell transplantation after conditioning.
More than 90% of patients with primary immunodeficiency transplanted with HLA-identical related marrow will survive with immune reconstitution. T-cell–depleted haploidentical related marrow transplants in patients with primary immunodeficiency have a 55% survival rate worldwide. The greatest success has been in patients with SCID, who do not require pretransplant conditioning or GVHD prophylaxis; 80-95% of patients with SCID will survive after T-cell–depleted parental marrow is given without pre-transplant chemotherapy or post-transplant GVHD prophylaxis, depending on whether the transplant can be performed soon after birth when the infant is healthy or after several months when the infant presents with serious infections. Until somatic cell gene therapy is more fully developed, bone marrow transplantation remains the most important and effective therapy for these inborn errors of the immune system. There was remarkable success with gene therapy in immunologically reconstituting 9 infants with X-linked SCID. Unfortunately, leukemic-like clonal T cells or lymphomas developed in 4 of the children. Insertional mutagenesis caused by retroviral insertion of the IL2RG cDNA near the LMO-2 gene produced these serious complications of gene therapy. Efforts are being focused on ways to prevent this problem, but for now gene therapy is on hold except in ADA-deficient SCID, where there has been outstanding success without insertional oncogenesis.
120.5 Immune Dysregulation with Autoimmunity or Lymphoproliferation
Autoimmune Lymphoproliferative Syndrome (ALPS)
ALPS, also known as Canale-Smith syndrome, is a disorder of abnormal lymphocyte apoptosis leading to polyclonal populations of T cells (double-negative T cells), which express CD3 and α/β antigen receptors but do not have CD4 or CD8 co-receptors (CD3 + T cell receptor α/β+ CD4− CD8−). These T cells respond poorly to antigens or mitogens and do not produce growth or survival factors (interleukin 2). The genetic deficit in most patients is a germ line or somatic mutation in the Fas gene, which produces a cell surface receptor of the tumor necrosis factor receptor superfamily (TNFRSF6), which, when stimulated by its ligand, will produce programmed cell death (Table 120-5). Persistent survival of these lymphocytes leads to immune dysregulation and autoimmunity.
Table 120-5 ALPS CASE CRITERIA AND ALPS CLASSIFICATION
REQUIRED
SUPPORTING
ALPS Ia = due to mutation in TNFRSF6
ALPS Ib = due to mutation in the gene for Fas ligand
ALPS II = due to mutation in the gene for caspase 10
ALPS III = ALPS without defined genetic cause
From Straus SE, Sneller M, Lenardo MJ, et al: An inherited disorder of lymphocyte apoptosis: the autoimmune lymphoproliferative syndrome, Ann Intern Med 130:591–601, 1999; Bleesing JJH, Straus SE, Fleisher TA: Autoimmune lymphoproliferative syndrome: a human disorder of abnormal lymphocyte survival, Pediatr Clin North Am 47:1291–1310, 2000.
Clinical Manifestations
ALPS is characterized by autoimmunity, chronic persistent or recurrent lymphadenopathy, splenomegaly, hepatomegaly (in 50%), and hypergammaglobulinemia (IgG, IgA). Many patients present in the 1st yr of life, and most are symptomatic by yr 5. Lymphadenopathy can be striking (Fig. 120-2). Splenomegaly may produce hypersplenism with cytopenias. Autoimmunity also produces anemia (Coombs positive hemolytic anemia) or thrombocytopenia or a mild neutropenia. Lymphoproliferative process (lymphadenopathy, splenomegaly) may regress over time, but autoimmunity does not and is characterized by frequent exacerbations and recurrences. Other autoimmune features include urticaria, uveitis, glomerulonephritis, hepatitis, vasculitis, glomulonephritis, vasculitis, panniculitis, arthritis, and central nervous system involvement (seizures, headaches, encephalopathy).
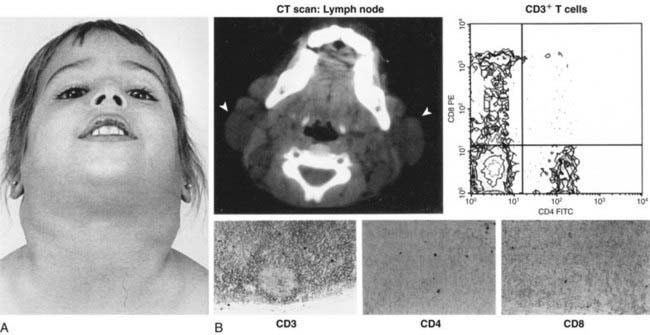
Figure 120-2 Clinical, radiographic, immunologic, and histologic characteristics of the autoimmune lymphoproliferative syndrome. A, Front view of the National Institutes of Health patient. B, Top middle, a CT scan of the neck is shown demonstrating enlarged preauricular, cervical, and occipital lymph nodes. Arrowheads denote the most prominent lymph nodes. The top right panels show the flow-cytometric analysis of peripheral blood T cells from a patient with autoimmune lymphoproliferative syndrome (ALPS), with CD8 expression on the vertical axis and CD4 on the horizontal axis. The lower left quadrant contains CD4-CD8 (double-negative) T cells, which are usually present at <1% of T cells expressing the αβ TCR. The bottom panels show CD3, CD4, and CD8 staining on serial sections of a lymph node biopsy specimen from a patient with ALPS and also shows that large numbers of DNCD3+ CD4-CD8 (double-negative) T cells are present in the interfollicular areas of the lymph node.
(Adapted from Siegel RM, Fleisher TA: The role of Fas and related death receptors in autoimmune and other disease states, J Allergy Clin Immunol 103:729–738, 1999; with permission.)
Malignancies are also more common in patients with ALPS and include Hodgkin and non-Hodgkin lymphomas and solid tissue tumors of thyroid, skin, heart, or lung.
Diagnosis
Laboratory abnormalities depend on the lymphoproliferative organ response (hypersplenism) or the degree of autoimmunity (anemia, thrombocytopenia). There may be lymphocytosis or lymphopenia. Criteria for the diagnosis are noted in Table 120-5. Flow cytometry helps identify the lymphocyte type (see Fig. 120-2). Functional genetic analysis for the TNFRSF6 gene often reveals a heterozygous mutation.
Treatment
Lymphoproliferative manifestations have been managed with corticosteroids and immunosuppressive agents (Cytoxan [cyclophosphamide], methotrexate, azathioprine); once weaned, the manifestation recurs. Hypersplenism may require splenectomy. Malignancies can be treated with the usual protocols used in patients unaffected by ALPS. Stem cell transplantation is another possible option in treating the autoimmune manifestations of ALPS.
Immune-Dysregulation, Polyendocrinopathy, Enteropathy, X-Linked (IPEX) Syndrome
This immune dysregulation syndrome is characterized by onset within the 1st weeks or months of life with watery diarrhea, an eczematous rash, insulin-dependent diabetes mellitus, hyperthyroidism or hypothyroidism, and other autoimmune disorders (Coombs positive hemolytic anemia, thrombocytopenia, neutropenia, alopecia).
IPEX is due to a mutation in the FOXP3 gene, which encodes a forkhead-winged helix transcription factor (scurfin) involved in the function and development of CD4+CD25+ regulatory T cells. The absence of regulatory cells may predispose to abnormal activation of effector T cells.
Clinical Manifestations
Watery diarrhea with intestinal villous atrophy leads to failure to thrive in most patients. Cutaneous lesions (usually eczema) and insulin-dependent diabetes begin in infancy. Lymphadenopathy and splenomegaly are also present. Serious bacterial infections (meningitis, sepsis, pneumonia, osteomyelitis) may be related to neutropenia, malnutrition, or immune dysregulation. Laboratory features reflect the associated autoimmune diseases, dehydration, and malnutrition. In addition, serum IgE levels are elevated with normal levels of IgM, IgG, and IgA. The diagnosis is made clinically and by mutational analysis of the FOXP3 gene.
Treatment
Inhibition of T-cell activation by cyclosporine, tacrolimus, or sirolimus with steroids is the treatment of choice, along with the specific care of the endocrinopathy and other manifestations of autoimmunity. Stem cell transplantation is the only possibility for curing IPEX. Overall, the combination of the risks for serious bacterial infection in the untreated condition and the risks of immunosuppression and bone marrow transplantation gives IPEX a poor prognosis. Untreated, most die by 2 yr of age.
Adeli MM, Buckley RH. Why newborn screening for severe combined immunodeficiency is essential: a case report. Pediatrics. 2010;126(2):e465-e469.
Aiuti A, Cattaneo F, Galimberti S, et al. Gene therapy for immunodeficiency due to adenosine deaminase deficiency. N Engl J Med. 2009;360:447-458.
Bouma G, Burns SO, Thrasher AJ. Wiskott-Aldrich Syndrome: immunodeficiency resulting from defective cell migration and impaired immunostimulatory activation. Immunobiology. 2009;214:778-790.
Buckley RH. Molecular defects in human severe combined immunodeficiency and approaches to immune reconstitution. Annu Rev Immunol. 2004;22:625-655.
Casrouge A, Zhang SY, Eidenschenk C, et al. Herpes simplex virus encephalitis in human UNC-93B deficiency. Science. 2006;314:308-312.
Freeman AF, Holland SM. Clinical manifestations, etiology, and pathogenesis of the hyper-IgE syndromes. Pediatr Res. 2009;6:32R-37R.
Geha RS, Notarangelo LD, Casanova JL, et al. Primary immunodeficiency diseases: an update from the International Union of Immunological Societies Primary Immunodeficiency Diseases Classification Committee. J Allergy Clin Immunol. 2007;120:776-794.
Hacein-Bey-Abina S, Hauer J, Lim A, et al. Efficacy of gene therapy for x-linked severe combined immunodeficiency. N Engl J Med. 2010;363:355-364.
Hacein-Bey-Abina S, Garrigue A, Wang GP, et al. Insertional oncogenesis in 4 patients after retrovirus-mediated gene therapy of SCID-X1. J Clin Invest. 2008;118:3132-3142.
Holland SM, Deleo FR, Elloumi HZ, et al. STAT3 mutations in the hyper-IgE syndrome. N Engl J Med. 2007;357:1608-1619.
Howe SJ, Mansour MR, Schwarzwaelder K, et al. Insertional mutagenesis combined with acquired somatic mutations causes leukemogenesis following gene therapy of SCID-X1 patients. J Clin Invest. 2008;118:3143-3150.
Ku CL, Yang K, Bustamante J, et al. Inherited disorders of human Toll-like receptor signaling: immunological implications. Immunol Rev. 2005;203:10-20.
Lagresle-Peyrou C, Six EM, Picard C, et al. Human adenylate kinase 2 deficiency causes a profound hematopoietic defect associated with sensorineural deafness. Nat Genet. 2009;41:106-111.
Ma CS, Chew GY, Simpson N, et al. Deficiency of Th17 cells in hyper IgE syndrome due to mutations in STAT3. J Exp Med. 2008;205:1551-1557.
Meyer-Bahlburg A, Becker-Herman S, Humblet-Baron S, et al. Wiskott-Aldrich syndrome protein deficiency in B cells results in impaired peripheral homeostasis. Blood. 2008;112:4158-4169.
Minegishi Y, Saito M, Tsuchiya S, et al. Dominant-negative mutations in the DNA-binding domain of STAT3 cause hyper-IgE syndrome. Nature. 2007;448:1058-1062.
Morinishi Y, Imai K, Nakagawa N, et al. Identification of severe combined immunodeficiency by T-cell receptor excision circles quantification using neonatal Guthrie cards. J Pediatr. 2009;155:829-833.
Pannicke U, Honig M, Hess I, et al. Reticular dysgenesis (aleukocytosis) is caused by mutations in the gene encoding mitochondrial adenylate kinase 2. Nat Genet. 2009;41:101-105.
Patel NC, Hertel PM, Estes MK, et al. Vaccine-acquired rotavirus in infants with severe combined immunodeficiency. N Engl J Med. 2010;362:314-319.
Pessach I, Walter J, Notarangelo LD. Recent advances in primary immunodeficiencies: identification of novel genetic defects and unanticipated phenotypes. Pediatr Res. 2009;65:3R-12R.
Railey MD, Lokhnygina Y, Buckley RH. Long-term clinical outcome of patients with severe combined immunodeficiency who received related donor bone marrow transplants without pretransplant chemotherapy post-transplant GVHD prophylaxis. J Pediatr. 2009;155:834-840.
Renner ED, Puck JM, Holland SM, et al. Autosomal recessive hyperimmunoglobulin E syndrome: a distinct disease entity. J Pediatr. 2004;144:93-99.
Roberts JL, Lauritsen JHP, Cooney M, et al. T-B+NK+ severe combined immunodeficiency caused by complete deficiency of the CD3 zeta subunit of the T cell antigen receptor complex. Blood. 2007;109:3198-3206.
Rosenzweig SD, Holland SM. Defects in the interferon-gamma and interleukin-12 pathways. Immunol Rev. 2005;203:38-47.
Routes JM, Grossman WJ, Verbsky J, et al. Statewide newborn screening for severe T-cell lymphopenia. JAMA. 2009;302:2465-2470.
Sarzotti-Kelsoe M, Win CM, Parrott RE, et al. Thymic output, T-cell diversity, and T-cell function in long-term human SCID chimeras. Blood. 2009;114:1445-1453.
Su MA, Anderson MS. Monogenic autoimmune diseases: insights into self-tolerance. Pediatr Res. 2009;65:20R-25R.
Tangye SG, Cook MC, Fulcher DA. Insights into the role of STAT3 in human lymphocyte differentiation as revealed by the hyper-IgE syndrome. J Immunol. 2009;182:21-28.
van der Burg M., Ijspeert H, Verkaik NS, et al. A DNA-PKcs mutation in a radiosensitive T-B- SCID patient inhibits Artemis activation and nonhomologous end-joining. J Clin Invest. 2009;119:91-98.
von Bernuth H, Picard C, Jin Z, et al. Pyogenic bacterial infections in humans with MyD88 deficiency. Science. 2008;321:691-696.
Zhang Q, Davis JC, Lamborn IT, et al. Combined immunodeficiency associated with DOCK8 mutations. N Engl J Med. 2009;361:2046-2054.