Chapter 141 Ocular Allergies
The eye is a common target of allergic disorders because of its marked vascularity and direct contact with allergens in the environment. The conjunctiva is the most immunologically active tissue of the external eye. Ocular allergies can occur as isolated target organ disease or more commonly in conjunction with nasal allergies. Ocular symptoms can significantly affect quality of life.
Clinical Manifestations
There are a few distinct entities that constitute allergic eye disease, all of which have bilateral involvement. Sensitization is necessary for all of these except for giant papillary conjunctivitis. Vernal keratoconjunctivitis and atopic keratoconjunctivitis are potentially sight-threatening.
Allergic Conjunctivitis
Allergic conjunctivitis is the most common hypersensitivity response of the eye, affecting approximately 25% of the general population and 30% of children with atopy. It is caused by direct exposure of the mucosal surfaces of the eye to environmental allergens. Patients complain of variable ocular itching, rather than pain, with increased tearing. Clinical signs include bilateral injected conjunctivae with vascular congestion that may progress to chemosis, or conjunctival swelling, and a watery discharge (Fig. 141-1). Allergic conjunctivitis occurs in a seasonal or, less commonly, perennial form. Seasonal allergic conjunctivitis is typically associated with allergic rhinitis (Chapter 137) and is most commonly triggered by pollens. Major pollen groups in the temperate zones include trees (late winter to early spring), grasses (late spring to early summer), and weeds (late summer to early fall), but seasons can vary significantly in different parts of the country. Mold spores can also cause seasonal allergy symptoms, principally in the summer and fall. Seasonal allergy symptoms may be aggravated by coincident exposure to perennial allergens. Perennial allergic conjunctivitis is triggered by allergens such as animal danders or dust mites that are present throughout the year. Symptoms are usually less severe than with seasonal allergic conjunctivitis. Since pollens and soil molds may be present year round while exposure to perennial allergens such as furred animals may be intermittent, classification as intermittent (i.e., symptoms present <4 days a week or for <4 weeks) and persistent (symptoms present >4 days a week and for >4 weeks) has been proposed.

Vernal Keratoconjunctivitis
Vernal keratoconjunctivitis is a severe bilateral chronic inflammatory process of the upper tarsal conjunctival surface that occurs in a limbal or palpebral form. It may threaten eyesight if there is corneal involvement. Although vernal keratoconjunctivitis is not IgE mediated, it occurs most frequently in children with seasonal allergies, asthma, or atopic dermatitis. Vernal keratoconjunctivitis affects boys twice as often as girls and is more common in persons of Asian and African origin. It affects primarily children in temperate areas, with exacerbations in the spring and summer. Symptoms include severe ocular itching exacerbated by exposure to irritants, light, or perspiration. In addition, patients may complain of severe photophobia, foreign-body sensation, and lacrimation. Giant papillae occur predominantly on the upper tarsal plate and are typically described as cobblestoning (Fig. 141-2). Other signs include a stringy or thick, ropey discharge, cobblestone papillae, transient yellow-white points in the limbus (Trantas dots) and conjunctiva (Horner points), corneal “shield” ulcers, and Dennie lines (Dennie-Morgan folds), which are prominent symmetric skinfolds that extend in an arc from the inner canthus beneath and parallel to the lower lid margin. Children with vernal keratoconjunctivitis have measurably longer eyelashes, which may represent a reaction to ocular inflammation.
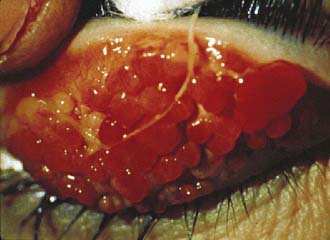
Figure 141-2 Vernal keratoconjunctivitis. Cobblestone papillae and ropey discharge are seen on the underside (tarsal conjunctiva) of the upper eyelid.
(From Adkinson NF Jr, Bochner BS, Busse WW, et al, editors: Middleton’s allergy principles and practice, ed 7, vol 2, Philadelphia, Mosby/Elsevier, p 1224.)
Atopic Keratoconjunctivitis
Atopic keratoconjunctivitis is a chronic inflammatory ocular disorder most commonly involving the lower tarsal conjunctiva. It may threaten eyesight if there is corneal involvement. Almost all patients have atopic dermatitis, and a significant number have asthma. Atopic keratoconjunctivitis rarely presents before late adolescence. Symptoms include severe bilateral ocular itching, burning, photophobia, and tearing with a mucoid discharge that are much more severe than in allergic conjunctivitis and persist through-out the year. The bulbar conjunctiva is injected and chemotic; cataracts may occur. Eyelid eczema can extend to the periorbital skin and cheeks with erythema and thick, dry scaling. Secondary staphylococcal blepharitis is common because of eyelid induration and maceration.
Giant Papillary Conjunctivitis
Giant papillary conjunctivitis has been linked to chronic exposure to foreign bodies, such as contact lenses, both hard and soft, ocular prostheses, and sutures. Symptoms and signs include mild bilateral ocular itching, tearing, a foreign body sensation, and excessive ocular discomfort with mild mucoid discharge with white or clear exudate on awakening, which may become thick and stringy. Trantas dots, limbal infiltration, bulbar conjunctival hyperemia, and edema may develop.
Diagnosis
Non-allergic conjunctivitis can be viral, bacterial, or chlamydial in origin. It is typically unilateral but can be bilateral with symptoms initially developing in one eye (Chapter 618). Symptoms include stinging or burning rather than itching and often a foreign body sensation. Ocular discharge can be watery, mucoid, or purulent. Masqueraders of ocular allergy also include nasolacrimal duct obstruction, foreign body, blepharoconjunctivitis, dry eye, uveitis, and trauma.
Treatment
Primary treatment of ocular allergies includes avoidance of allergens, cold compresses, and lubrication. Secondary treatment regimens include the use of oral or topical antihistamines (see Table 142-1) and, if necessary, topical decongestants, mast cell stabilizers, and anti-inflammatory agents (Table 141-1). Drugs with dual antihistamine and mast cell blocking activities provide the most advantageous approach in treating allergic conjunctivitis, with both fast-acting symptomatic relief and disease-modifying action. Children often complain of stinging or burning with use of topical ophthalmic preparations and usually prefer oral antihistamines for allergic conjunctivitis. It is important not to contaminate topical ocular medications by allowing the applicator tip to contact the eye or eyelid. Using refrigerated medications may decrease some of the discomfort associated with their use. Topical decongestants act as vasoconstrictors, reducing erythema, vascular congestion, and eyelid edema, but do not diminish the allergic response. Adverse effects of topical vasoconstrictors include burning or stinging and rebound hyperemia or conjunctivitis medicamentosa with chronic use. Combined use of an antihistamine and a vasoconstrictive agent is more effective than use of either agent alone. Use of topical nasal corticosteroids for allergic rhinoconjunctivitis decreases ocular symptoms, presumably through a naso-ocular reflex.
Table 141-1 TOPICAL OPHTHALMIC MEDICATIONS FOR ALLERGIC CONJUNCTIVITIS
| DRUG AND TRADE NAMES | MECHANISM OF ACTION AND DOSING | CAUTIONS AND ADVERSE EVENTS |
|---|---|---|
| Not for treatment of contact lens–related irritation; the preservative may be absorbed by soft contact lenses. Wait at least 10 min after administration before inserting soft contact lenses. | ||
| Soft contact lenses should not be worn if the eye is red. Wait at least 10 min after administration before inserting soft contact lenses. | ||
| Not for use in patients wearing soft contact lenses during treatment. | ||
| Pheniramine maleate | Antihistamine/vasoconstrictor | Avoid prolonged use (>3-4 days) to avoid rebound symptoms. Not for use with contact lenses. |
| 0.3%/naphazoline hydrochloride | Children >6 yr: 1-2 gtt qid | |
| 0.025% | ||
| Naphcon-A, Opcon-A | ||
| Cromolyn sodium 4% | Mast cell stabilizer | Can be used to treat giant papillary conjunctivitis and vernal keratitis. Not for use with contact lenses. |
| Crolom, Opticrom | Children >4 yr 1-2 gtt q4-6h | |
| Lodoxamide tromethamine 0.1% Alomide | Can be used to treat vernal keratoconjunctivitis. Not for use in patients wearing soft contact lenses during treatment. | |
| Nedocromil sodium 2% Alocril | Avoid wearing contact lenses while exhibiting the signs and symptoms of allergic conjunctivitis. | |
| Not for treatment of contact lens related irritation; the preservative may be absorbed by soft contact lenses. Wait at least 10 min after administration before inserting soft contact lenses. | ||
| Contact lenses should be removed prior to use. Wait at least 15 min after administration before inserting soft contact lenses. Not for the treatment of contact lens irritation. | ||
| Not for treatment of contact lens related irritation; the preservative may be absorbed by soft contact lenses. Wait at least 10 min after administration before inserting soft contact lenses. | ||
| Not for treatment of contact lens related irritation; the preservative may be absorbed by soft contact lenses. Wait at least 10 min after administration before inserting soft contact lenses. | ||
| Ketorolac tromethamine 0.5% Acular | Avoid with aspirin or NSAID sensitivity. Use ocular product with caution in patients with complicated ocular surgeries, corneal denervation or epithelial defects, ocular surface diseases (e.g., dry eye syndrome), repeated ocular surgeries within a short period of time, diabetes mellitus, or rheumatoid arthritis; these patients may be at risk for corneal adverse events that may be sight-threatening. Do not use while wearing contact lenses. |
NSAID, nonsteroidal anti-inflammatory drug.
Tertiary treatment of ocular allergy includes topical or, rarely, oral corticosteroids and should be conducted in conjunction with an ophthalmologist. Local administration of topical corticosteroids may be associated with increased intraocular pressure, viral infections, and cataract formation. Allergen immunotherapy can be very effective in seasonal and perennial allergic conjunctivitis, especially when associated with rhinitis, and can decrease the need for oral or topical medications to control allergy symptoms.
Baroody FM, Foster KA, Markaryan A, et al. Nasal ocular reflexes and eye symptoms in patients with allergic rhinitis. Ann Allergy Asthma Immunol. 2008;100:194-199.
Bielory L. Allergic and immunologic disorders of the eye: II. Ocular allergy. J Allergy Clin Immunol. 2000;106:1019-1032.
Bielory L. Intranasal corticosteroids reduce ocular symptoms of allergic rhinitis as a class effect. J Allergy Clin Immunol. 2008;121:538-539.
Bielory L. Ocular allergy treatment. Immunol Allergy Clin North Am. 2008;28:189-224.
Bielory L, Friedlaender MH. Allergic conjunctivitis. Immunol Allergy Clin North Am. 2008;28:43-58.
Bousquet J, Khaltaev N, Cruz AA, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen). Allergy. 2008;63(Suppl 86):8-160.
Donshik PC, Ehlers WH, Ballow M. Giant papillary conjunctivitis. Immunol Allergy Clin North Am. 2008;28:83-103.
Jun J, Bielory L, Raizman MB. Vernal conjunctivitis. Immunol Allergy Clin North Am. 2008;28:59-82.