Chapter 370 Nasal Polyps
Etiology
Nasal polyps are benign pedunculated tumors formed from edematous, usually chronically inflamed nasal mucosa. They commonly arise from the ethmoidal sinus and occur in the middle meatus. Occasionally, they appear within the maxillary antrum and can extend to the nasopharynx (antrochoanal polyp).
It is estimated that between 0.2% and 1% of the population will develop nasal polyps at some time; the incidence of nasal polyps increases with age. Antrochoanal polyps represent only 4-6% of all nasal polyps in the general population but account for approximately one third of polyps in the pediatric population. Large or multiple polyps can completely obstruct the nasal passage. The polyps originating from the ethmoidal sinus are usually smaller and multiple, as compared with the large and usually single antrochoanal polyp.
Cystic fibrosis is the most common childhood cause of nasal polyposis and should be suspected in any child <12 yr old with nasal polyps, even in the absence of typical respiratory and digestive symptoms; as many as 30% of children with cystic fibrosis acquire nasal polyps (Chapter 395). Nasal polyposis is also associated with chronic sinusitis and allergic rhinitis. In the uncommon Samter triad, nasal polyps are associated with aspirin sensitivity and asthma.
Clinical Manifestations
Obstruction of nasal passages is prominent, with associated hyponasal speech and mouth breathing. Profuse unilateral mucoid or mucopurulent rhinorrhea may also be present. An examination of the nasal passages shows glistening, gray, grapelike masses squeezed between the nasal turbinates and the septum.
Diagnosis and Differential Diagnosis
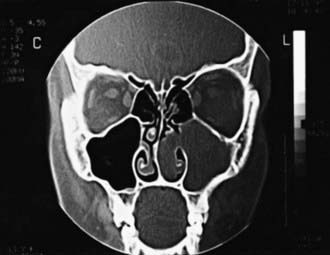
Examination of the external nose and rhinoscopy is performed. Ethmoidal polyps can be readily distinguished from the well-vascularized turbinate tissue, which is pink or red; antrochoanal polyps may have a more fleshy appearance (Fig. 370-1). Antrochoanal polyps may prolapse into the nasopharynx; flexible nasopharyngoscopy can assist in making this diagnosis. Prolonged presence of ethmoidal polyps in a child can widen the bridge of the nose and erode adjacent osseous structures. Tumors of the nose cause more local destruction and distortion of the anatomy. CT scan of the midface is key to diagnosis and planning for surgical treatment (Fig. 370-2).

Treatment
Local or systemic decongestants are not usually effective in shrinking the polyps, although they may provide symptomatic relief from the associated mucosal edema. Intranasal steroid sprays, and sometimes systemic steroids, can provide some shrinkage of nasal polyps with symptomatic relief and have proved useful in children with cystic fibrosis and adults with nasal polyps. Polyps should be removed surgically if complete obstruction, uncontrolled rhinorrhea, or deformity of the nose appears. If the underlying pathogenic mechanism cannot be eliminated (cystic fibrosis), the polyps may soon return. Functional endoscopic sinus surgery provides more complete polyp removal and treatment of other associated nasal disease; in some cases, this has reduced the need for frequent surgeries. Nasal steroid sprays should also be started preventively, once postsurgical healing occurs.
Antrochoanal polyps do not respond to medical measures and must be removed surgically. Because these types of polyps are not associated with any underlying disease process, the recurrence rate is much less than for other types of polyps.
Basik S, Karaman CZ, Akdilli A, et al. Surgical approaches to antrochoanal polyps in children. Int J Pediatr Otorhinolaryngol. 1998;46:197-205.
Magit AE. Tumors of the nose, paranasal sinuses, and nasopharynx. In: Bluestone CD, Stool SE, Kenna MA, editors. Pediatric otolaryngology. ed 3. Philadelphia: WB Saunders; 1996:893-904.
Orvidas LJ, Beatty CW, Weaver AL. Antrochoanal polyps in children. Am J Rhinol. 2001;15:321-325.
Scadding GK, Durham SR, Mirakian R, et al. British Society for Allergy and Clinical Immunology: BSACI guidelines for the management of rhinosinusitis and nasal polyposis. Clin Exp Allergy. 2008;38:260-275.
Stjärne P, Mösges R, Jorissen M, et al. A randomized controlled trial of mometasonc furoate nasal spray for the treatment of nasal polyposis. Arch Otolaryngol Head Neck Surg. 2006;132:179-185.
Thomas M, Yawn BP, Price D, et al. European Position Paper on Rhinosinusitis and Nasal Polyps Group. EPOS Primary Care Guidelines: European Position Paper on the Primary Care Diagnosis and Management of Rhinosinusitis and Nasal Polyps 2007—a summary. Prim Care Respir J. 2008;17:79-89.