Chapter 381 Bronchomalacia and Tracheomalacia
Chondromalacias of the trachea or of a main bronchus occur when there is insufficient cartilage to maintain airway patency throughout the respiratory cycle and are common causes of persistent wheezing in infancy. Tracheomalacia and bronchomalacia can be either primary or secondary (see Table 381-1 on the Nelson Textbook of Pediatrics website at www.expertconsult.com). Although primary tracheomalacia and bronchomalacia are often seen in premature infants, most affected patients are born at term. Secondary tracheomalacia and bronchomalacia refers to the situation in which the central airway is compressed by adjacent structure (e.g., vascular ring, Chapter 426) or deficient in cartilage due to tracheoesophageal fistula. Laryngomalacia can accompany primary bronchomalacia or tracheomalacia. Involvement of the entire central airway (laryngotracheobronchomalacia) is also seen.
Table 381-1 CLASSIFICATION OF TRACHEOMALACIA
PRIMARY TRACHEOMALACIA
SECONDARY TRACHEOMALACIA
From McNamara VM, Crabbe DC: Tracheomalacia, Paediatr Respir Rev 5:147–154, 2004.
Clinical Manifestations
Primary tracheomalacia and bronchomalacia are principally disorders of infants, with a male:female ratio of 2 : 1. The dominant finding, low-pitched monophonic wheezing, is most prominent over the central airways. Parents often describe persistent respiratory congestion even in the absence of a viral respiratory infection. When the lesion involves only one main bronchus (more commonly the left), the wheezing is louder on that side. In cases of tracheomalacia, the wheeze is loudest over the trachea. Hyperinflation and/or subcostal retractions do not occur unless the patient also has asthma or another cause of small airways obstruction. In the absence of asthma, patients with tracheomalacia and bronchomalacia are not helped by administration of a bronchodilator. Acquired tracheomalacia and bronchomalacia are seen in association with vascular rings or tracheoesophageal fistula (and may persist after surgical correction) and cardiomegaly and after lung transplantation.
Diagnosis
The definitive diagnoses of tracheomalacia and bronchomalacia are established by flexible or rigid bronchoscopy (Fig. 381-1). The lesion is difficult to detect on plain radiographs, but fluoroscopy can demonstrate dynamic collapse and can avoid the need for invasive diagnostic techniques. Pulmonary function testing can show a pattern of decreased peak flow and flattening of the flow-volume loop. Other important diagnostic modalities include MRI and CT scanning. MRI with angiography is especially useful when there is a possibility of vascular ring and should be performed when a right aortic arch is seen on plain film radiography.
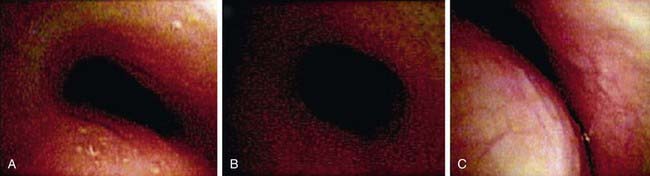
Figure 381-1 Images of tracheomalacia taken 10 mm from site. A, Saber-shaped or triangular appearance. B, Circumferential appearance. C, Crescent (lunate) appearance.
(From Masters IB, Zimmerman PV, Pandeya N, et al: Quantified tracheobronchomalacia disorders and their clinical profiles in children, Chest 133:461–467, 2008.)
Treatment
Postural drainage can help with clearance of secretions. β-Adrenergic agents should be avoided in the absence of asthma, because they can exacerbate poor airway tone. Nebulized ipratropium bromide may be useful. Endobronchial stents have been used in severely affected patients but have a high incidence of complications, ranging from airway obstruction due to granulation tissue to erosion into adjacent vascular structures. Continuous positive airway pressure (CPAP) via tracheostomy may be indicated for severe cases. Surgical approach (aortopexy and bronchopexy) is rarely required and only for patients who have life-threatening apnea, cyanosis, and bradycardia (“cyanotic spells”) from airway obstruction.
Prognosis
Primary bronchomalacia and tracheomalacia have excellent prognoses, because airflow improves as the child and the airways grow. Patients with primary airway malacia usually take longer to recover from common respiratory infections. Wheezing at rest usually resolves by age 3 yr. Prognosis in secondary and acquired forms varies with cause. Patients with concurrent asthma need considerable supportive treatment.
Anton-Pacheco JL, Cabezali D, Tejedor R, et al. The role of airway stenting in pediatric tracheobronchial obstruction. Eur J Cardiothorac Surg. 2008;33:1069-1075.
Boogaard R, Huijsmans SH, Pijnenburg MW, et al. Tracheomalacia and bronchomalacia in children: incidence and patient characteristics. Chest. 2005;128:3391-3397.
Carden KA, Boiselle PM, Waltz DA, et al. Tracheomalacia and tracheobronchomalacia in children and adults: an in-depth review. Chest. 2005;127:984-1005.
Masters IB, Chang AB, Patterson L, et al. Series of laryngomalacia, tracheomalacia, and bronchomalacia disorders and their associations with other conditions in children. Pediatr Pulmonol. 2002;34:189-195.
Masters IB, Zimmerman PV, Pandeya N, et al. Quantified tracheobronchomalacia disorders and their clinical profiles in children. Chest. 2008;133:461-467.
McNamara VM, Crabbe DC. Tracheomalacia. Paediatr Respir Rev. 2004;5:147-154.
Yalcin E, Dogru D, Ozcelik U, et al. Tracheomalacia and bronchomalacia in 34 children: clinical and radiologic profiles and associations with other diseases. Clin Pediatr. 2005;44:777-781.