Chapter 620 Abnormalities of the Lens
Cataracts
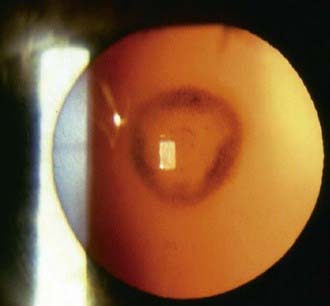
A cataract is any opacity of the lens (Fig. 620-1). Some are clinically unimportant; others significantly affect visual function. The incidence of infantile cataracts is approximately 2-13/10,000 live births. An epidemiologic study of infantile cataracts published in 2003 suggests that approximately 60% of cataracts are an isolated defect; 22% are part of a syndrome; and the remainder is associated with other unrelated major birth defects. Cataracts are more common in low birthweight infants. Infants at or below 2,500 g have a 3- to 4-fold increased odds of developing infantile cataracts. Some cataracts are associated with other ocular or systemic disease.

Differential Diagnosis
The differential diagnosis of cataracts in infants and children includes a wide range of developmental disorders, infectious and inflammatory processes, metabolic diseases, and toxic and traumatic insults (Table 620-1). Cataracts may also develop secondary to intraocular processes, such as retinopathy of prematurity, persistent hyperplastic primary vitreous, retinal detachment, retinitis pigmentosa, and uveitis. A portion of cataracts in children are inherited (Fig. 620-2).
Table 620-1 DIFFERENTIAL DIAGNOSIS OF CATARACTS
DEVELOPMENTAL VARIANTS
Prematurity (Y-suture vacuoles) with or without retinopathy of prematurity
GENETIC DISORDERS
Simple Mendelian Inheritance
Major Chromosomal Defects
Multisystem Genetic Disorders
Inborn Errors of Metabolism
ENDOCRINOPATHIES
CONGENITAL INFECTIONS
OCULAR ANOMALIES
MISCELLANEOUS DISORDERS
IDIOPATHIC
Developmental Variants
Early developmental processes may lead to various congenital lens opacities. Discrete dots or white plaquelike opacities of the lens capsule are common and sometimes involve the contiguous subcapsular region. Small opacities of the posterior capsule may be associated with persistent remnants of the primitive hyaloid vascular system (the common Mittendorf dot), whereas those of the anterior capsule may be associated with persistent strands of the pupillary membrane or vascular sheath of the lens. Congenital cataracts of this type are usually stationary and rarely interfere with vision; in some, progression occurs.
Prematurity
A special type of lens change seen in some preterm newborn infants is the so-called cataract of prematurity. The appearance is of a cluster of tiny vacuoles in the distribution of the Y sutures of the lens. They can be visualized with an ophthalmoscope and are best seen with the pupil well dilated. The pathogenesis is unclear. In most cases, the opacities disappear spontaneously, often within a few weeks.
Mendelian Inheritance
Many cataracts unassociated with other diseases are hereditary. The most common mode of inheritance is autosomal dominant. Penetrance and expressivity vary. Autosomal recessive inheritance occurs less frequently; it is sometimes found in populations with high rates of consanguinity. X-linked inheritance of cataracts unassociated with disease is relatively rare.
Congenital Infection Syndrome
Cataracts in infants and children can be a result of prenatal infection. Lens opacity may occur in any of the major congenital infection syndromes (e.g., toxoplasmosis, cytomegalovirus, syphilis, rubella, herpes simplex virus). Cataracts may also occur secondary to other perinatal infections, including measles, poliomyelitis, influenza, varicella-zoster, and vaccinia.
Metabolic Disorders
Cataracts are a prominent manifestation of many metabolic diseases, particularly certain disorders of carbohydrate, amino acid, calcium, and copper metabolism. A primary consideration in any infant with cataracts is the possibility of galactosemia (Chapter 81.2). In classic infantile galactosemia, galactose-1-phosphate uridyl transferase deficiency, the cataract is typically of the zonular type, with haziness or opacification of 1 or more of the perinuclear layers of the lens Haziness or clouding of the nucleus also often occurs. In its early stages, the cataract generally has a distinctive oil droplet appearance and is best detected with the pupil fully dilated. Progression to complete opacification of the lens may occur within weeks. With early treatment (galactose-free diet), the lens changes may be reversible.
In galactokinase deficiency, cataracts are the sole clinical manifestation. The cataracts are usually zonular and may appear in the 1st months of life, 1st years of life, or later in childhood.
In children with juvenile-onset diabetes mellitus, lens changes are uncommon. Some develop snowflake-like white opacities and vacuoles of the lens. Others develop cataracts that may progress and mature rapidly, sometimes in a matter of days, especially during adolescence. An antecedent event may be the sudden development of myopia caused by changes in the optical density of the lens.
Congenital lens opacities may be seen in children of diabetic and prediabetic mothers. Hypoglycemia in neonates can also be associated with early development of cataracts. Ketotic hypoglycemia is also associated with cataracts.
An association between cataracts and hypocalcemia is well established. Various lens opacities may be seen in patients with hypoparathyroidism.
The oculocerebral renal syndrome of Lowe is associated with cataracts in infants. Affected male children frequently have dense bilateral cataracts at birth, often in association with glaucoma and miotic pupils. Punctate lens opacities are frequently present in heterozygous females.
The distinctive sunflower cataract of Wilson disease is not commonly seen in children. Various lens opacities may be seen in children with certain of the sphingolipidoses, mucopolysaccharidoses, and mucolipidoses, particularly Niemann-Pick disease, mucosulfatidosis, Fabry disease, and aspartylglycosaminuria (Chapters 80 and 82).
Chromosomal Defects
Lens opacities of various types may occur in association with chromosomal defects, including trisomies 13, 18, and 21; Turner syndrome; and a number of deletion (11p13, 18p, 18q) and duplication (3q, 20p, 10q) syndromes (Chapter 76).
Drugs, Toxic Agents, and Trauma
Of the various drugs and toxic agents that may produce cataracts, corticosteroids are of major importance in the pediatric age group. Steroid-related cataracts characteristically are posterior subcapsular lens opacities. The incidence and severity vary. The relative significance of dose, mode of administration, duration of treatment, and individual susceptibility is controversial, and the pathogenesis of steroid-induced cataracts is unclear. The effect on vision depends on the extent and density of the opacity. In many cases, the acuity is only minimally or moderately impaired. Reversibility of steroid-induced cataracts may occur in some cases. All children receiving long-term steroid treatment should have periodic eye examinations.
Trauma to the eye is a major cause of cataracts in children. Opacification of the lens may result from contusion or penetrating injury. Cataracts are an important manifestation of child abuse.
Cataract formation after exposure to radiation is dose and duration dependent. Adult research shows 50% occurrence in lens dose of 15 Gy. Delayed onset is the rule.
Miscellaneous Disorders
The list of multisystem syndromes and diseases associated with lens opacities and other eye anomalies is extensive (see Table 620-1).
Treatment
The treatment of cataracts that significantly interfere with vision includes the following: (1) surgical removal of lens material to provide an optically clear visual axis; (2) correction of the resultant aphakic refractive error with spectacles, contact lenses, or intraocular lens implantation; and (3) correction of any associated sensory deprivation amblyopia. Because the use of spectacles may not be possible in children after cataract removal, the use of contact lenses for visual rehabilitation is sometimes a medical necessity. Intraocular lens implantation has become a mainstay for visual rehabilitation in older children. Patients are currently being recruited into a multicenter trial to help determine visual outcomes with contact lenses versus intraocular lens implants in very young children. Treatment of the amblyopia may be the most demanding and difficult step in the visual rehabilitation of infants or children with cataracts. Not all cataracts require surgical intervention. Cataracts that are not visually significant should be monitored for change and the child should be monitored for development of amblyopia.
Prognosis
Prognosis depends on many factors, including the nature of the cataract, the underlying disease, age at onset, age at intervention, duration and severity of any attendant amblyopia, and presence of any associated ocular abnormalities (e.g., microphthalmia, retinal lesions, optic atrophy, glaucoma, nystagmus, and strabismus). Persistent amblyopia is the most common cause of poor visual recovery after cataract surgery in children. Secondary conditions and complications may develop in children who have had cataract surgery, including inflammatory sequelae, secondary membranes, glaucoma, retinal detachment, and changes in the axial length of the eye. All these should be considered in planning treatment.
Ectopia Lentis
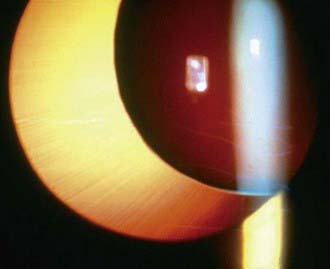
Normally, the lens is suspended in place behind the iris diaphragm by the zonular fibers of the ciliary body. Abnormalities of the suspensory system resulting from a developmental defect, disease, or trauma may result in instability or displacement of the lens. Displacement of the lens is classified as luxation (dislocation–complete displacement of the lens) (Fig. 620-3) or as subluxation (partial displacement–shifting or tilting of the lens) (Fig. 620-4). Symptoms include blurring of vision, which is often the result of refractive changes such as myopia, astigmatism, or aphakic hyperopia. Some patients experience diplopia (double vision). An important sign of displacement is iridodonesis, a tremulousness of the iris caused by the loss of its usual support. Also, the anterior chamber may appear deeper than normal. Sometimes the equatorial region (“edge”) of the displaced lens may be visible in the pupillary aperture. On ophthalmoscopy, this may appear as a black crescent. Also, the difference between the phakic and aphakic portions can be appreciated when focusing on the fundus.
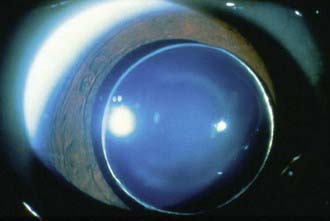
Figure 620-3 Complete dislocation of lens into the anterior chamber seen in Weill-Marchesani syndrome.
Differential Diagnosis
A major cause of lens displacement is trauma. Displacement may also occur as a result of ocular disease such as uveitis, intraocular tumor, congenital glaucoma, high myopia, megalocornea, aniridia, or in association with cataract. Ectopia lentis may also be inherited or associated with systemic disease.
Displacement of the lens occurring as a heritable ocular condition unassociated with systemic abnormalities is referred to as simple ectopia lentis. Simple ectopia lentis is usually transmitted as an autosomal dominant condition. The lens is generally displaced upward and temporally. The ectopia may be present at birth or may appear later in life. Another form of heritable dislocation is ectopia lentis et pupillae. In this condition, both the lens and pupil are displaced, usually in opposite directions. This condition is generally bilateral, with 1 eye being almost a mirror image of the other. Ectopia lentis et pupillae is a recessive condition, although variable expression with some intermingling with simple ectopia lentis has been reported.
Systemic disorders associated with displacement of the lens include Marfan syndrome, homocystinuria, Weill-Marchesani syndrome, and sulfite oxidase deficiency (Chapter 79). Ectopia lentis occurs in approximately 80% of patients with Marfan syndrome, and in about 50% of patients; the ectopia is evident by the age of 5 yr. In most cases, the lens is displaced superiorly and temporally; it is almost always bilateral and relatively symmetric. In homocystinuria, the lens is usually displaced inferiorly and somewhat nasally. It occurs early in life and is often evident by 5 yr of age. In Weill-Marchesani syndrome, the displacement of the lens is often downward and forward, and the lens tends to be small and round.
Ectopia lentis is also associated occasionally with other conditions, including Ehlers-Danlos, Sturge-Weber, Crouzon, and Klippel-Feil syndromes; oxycephaly; and mandibulofacial dysostosis. A syndrome of dominantly inherited blepharoptosis, high myopia, and ectopia lentis has also been described.
Treatment and Prognosis
Displacement of the lens often results only in optical problems. In some cases, however, more serious complications may develop, such as glaucoma, uveitis, retinal detachment, or cataract. Management must be individualized according to the type of displacement, its cause, and the presence of any complicating ocular or systemic conditions. For many patients, optical correction by spectacles or contact lenses can be provided. Manipulation of the iris diaphragm with mydriatic or miotic drops may sometimes help improve vision. In selected cases, the best treatment is surgical removal of the lens. In many children, treatment of any associated amblyopia must be instituted early. In addition, for children with ectopia lentis, safety precautions should be taken to prevent injury to the eye.
Microspherophakia
The term microspherophakia refers to a small, round lens that may occur as an isolated anomaly (probably autosomal recessive) or in association with other ocular abnormalities, such as ectopia lentis, myopia, or retinal detachment (possibly autosomal dominant). Microspherophakia may also occur in association with various systemic disorders, including Marfan syndrome, Weill-Marchesani syndrome, Alport syndrome, mandibulofacial dysostosis, and Klinefelter syndrome.
Anterior Lenticonus
Anterior lenticonus is a rare bilateral condition in which the anterior surface of the lens bulges centrally. It may be accompanied by lens opacities or other eye anomalies and is a prominent feature of Alport syndrome. The increased curvature of the central area may cause high myopia.
Rupture of the anterior capsule may occur, requiring prompt surgical intervention.
Posterior Lenticonus
Posterior lenticonus, which occurs more commonly than anterior lenticonus, is characterized by a circumscribed round or oval bulge of the posterior lens capsule and cortex, restricted to the 2-7 mm central region. In the early stages, by the red reflex test, this may look like an oil droplet. It occurs in infants and young children and tends to increase with age. Usually the lens material within and surrounding the capsular bulge eventually becomes opacified. Posterior lenticonus usually occurs as an isolated ocular anomaly. It is generally unilateral but may be bilateral. It is believed to be sporadic, although autosomal dominant and X-linked inheritance has been suggested in some cases. Infants or children with posterior lenticonus may require optical correction, amblyopia treatment, and surgery for progressive cataract.
Anteby I, Isaac M, BenEzra D. Hereditary subluxated lenses: visual performances and long-term follow-up after surgery. Ophthalmology. 2003;110:1344-1348.
Bhatti TR, Dott M, Yoon PW, et al. Descriptive epidemiology of infantile cataracts in metropolitain Atlanta, GA, 1968–1998. Arch Pediatr Adolesc Med. 2003;157:341-347.
Chugh KS, Sakhuja V, Agarwal A, et al. Hereditary nephritis (Alport’s syndrome)—clinical profile and inheritance in 28 kindreds. Nephrol Dial Transplant. 1993;8:690-695.
Fallaha N, Lambert SR. Pediatric cataracts. Ophthalmol Clin North Am. 2001;14:479-492.
Léonard A, Bernard P, Hiel AL, et al. Prenatal diagnosis of fetal cataract: case report and review of the literature. Fetal Diagn Ther. 2009;26:61-67.
Levin AV, Edmonds SA, Nelson LB, et al. Extended-wear contact lenses for the treatment of pediatric aphakia. Ophthalmology. 1988;95:1107-1113.
McClatchey SK, Hofmeister EM. The optics of aphakic and pseudophakic eyes in childhood. Surv Ophthalmol. 2009;55:174-182.
Peterseim MW, Wilson ME. Bilateral intraocular lens implantation in the pediatric population. Ophthalmology. 2000;107:1261-1266.
Plager DA, Yang S, Neely D, et al. Complications in the first year following cataract surgery with and without IOL in infants and older children. J AAPOS. 2002;6:9-14.
Russell-Eggit IM. Non-syndromic posterior lenticonus a cause of childhood cataract: evidence for X-linked inheritance. Eye (Lond). 2000;14(Pt 6):861-863.
SanGiovanni JP, Chew EY, Reed GF, et al. Infantile cataract in collaborative perinatal project: prevalence and risk factors. Arch Ophthalmol. 2002;120:1559-1565.
Tesser RA, Hess DB, Buckley EG. Pediatric cataracts and lens anomalies. In: Nelson LB, Olitsky SE, editors. Harley’s pediatric ophthalmology. ed 5. Philadelphia: Lippincott Williams & Wilkins; 2005:255-284.