Chapter 656 Disorders of the Mucous Membranes
The mucous membranes may be involved in developmental disorders, infections, acute and chronic skin diseases, genodermatoses, and benign and malignant tumors.
Cheilitis
Inflammation of the lips (cheilitis) and angles of the mouth (angular cheilitis or perlèche) (Fig. 656-1) are most commonly due to dryness, chapping, and lip licking. Excessive salivation and drooling, particularly in children with neurologic deficits, may also cause chronic irritation. Lesions of oral thrush may occasionally extend to the angles of the mouth. Protection can be provided by frequent applications of a bland ointment such as petrolatum. Candidosis should be treated with an appropriate antifungal agent, and contact dermatitis of the perioral skin should be treated with a low-potency topical corticosteroid ointment preparation and frequent use of petrolatum or a similar emollient.

Fordyce Spots
Fordyce spots are asymptomatic, minute, yellow-white papules on the vermilion border of the lips and buccal mucosa. These ectopic sebaceous glands may be found in otherwise normal individuals and require no therapy.
Mucocele
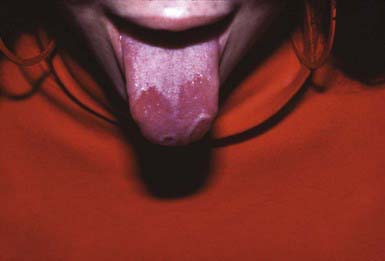
Mucus retention cysts are painless, fluctuant, tense, 2- to 10-mm, bluish papules on the lips (Fig. 656-2), tongue, palate, or buccal mucosa. Traumatic severance of the duct of a minor salivary gland leads to submucosal retention of mucus secretion. Those on the floor of the mouth are known as ranulas when the submaxillary or sublingual salivary ducts are involved. Fluctuations in size are usual, and the lesions may disappear temporarily after traumatic rupture. Recurrence is prevented by excision of the mucocele.

Aphthous Stomatitis (Canker Sores)
Aphthous stomatitis consists of solitary or multiple painful ulcerations occur on the labial (Fig. 656-3), buccal, or lingual mucosa and on the sublingual, palatal, or gingival mucosa (Chapter 307). Lesions may manifest initially as erythematous, indurated papules that erode rapidly to form sharply circumscribed, necrotic ulcers with a gray fibrinous exudate and an erythematous halo. Minor aphthous ulcers are 2-10 mm in diameter and heal spontaneously in 7-10 days. Major aphthous ulcers are >10 mm in diameter and take 10-30 days to heal. A third type of aphthous ulceration is herpetiform in appearance, manifesting as a few to numerous grouped 1- to 2-mm lesions that tend to coalesce into plaques that heal over 7-10 days. Approximately 30% of patients with recurrent lesions have a family history of the disorder (Chapter 307 for differential diagnosis).

The etiology of aphthous stomatitis is multifactorial; the condition probably represents an oral manifestation of a number of conditions. Altered local regulation of the cell-mediated immune system, after activation and accumulation of cytotoxic T cells, may contribute to the localized mucosal breakdown. It is a common misconception that aphthous stomatitis is a manifestation of herpes simplex virus infection. Recurrent herpes infections remain localized to the lips and rarely cross the mucocutaneous junction; involvement of the oral mucosa occurs only in primary infections.
Treatment of aphthous stomatitis is palliative. The majority of mild cases do not require therapy. Relief of pain, particularly before eating, may be achieved with the use of a topical anesthetic such as viscous lidocaine or an oral rinse with a combined solution of elixir of diphenhydramine, viscous lidocaine, and an oral antacid. Care must be taken to avoid hot food and drink after the use of a topical anesthetic. A topical corticosteroid in a mucosa-adhering agent may help reduce inflammation, and topical tetracycline mouthwash may also hasten healing. In severe, debilitating cases, systemic therapy with corticosteroids, colchicine, cimetidine, or dapsone may be helpful.
Cowden Syndrome (Multiple Hamartoma Syndrome)
Cowden syndrome is an autosomal dominant condition that usually manifests in the 2nd or 3rd decade with smooth, pink or whitish papules on the palatal, gingival, buccal, and labial mucosae. Mutations in the tumor suppressor gene PTEN cause Cowden syndrome. The benign fibromas characteristic of the syndrome may coalesce into a cobblestone appearance. Numerous flesh-colored papules also develop on the face, particularly around the mouth, nose, and ears. These papules are most commonly trichilemmomas, a benign neoplasm of the hair follicle. Associated findings may include acral keratotic papules, thyroid goiter, gastrointestinal polyps, fibrocystic breast nodules, and carcinoma of the breast or thyroid.
Epstein Pearls (Gingival Cysts of the Newborn)
Epstein pearls are white keratin-containing cysts on the palatal or alveolar mucosa of approximately 80% of neonates. They cause no symptoms and are generally shed within a few weeks.
Geographic Tongue (Benign Migratory Glossitis)
Geographic tongue consists of single or multiple sharply demarcated, irregular, smooth red plaques on the dorsum of the tongue caused by transient atrophy of the filiform papillae and the surface epithelium, often with elevated gray margins composed of intervening filiform papillae that are increased in thickness (Fig. 656-4). Symptoms of mild burning or irritation may occasionally be bothersome. Onset is rapid, and the pattern may change over hours to days. Some patients feel that the condition is exacerbated by stress or by hot or spicy foods. The histology of geographic tongue is similar to that of pustular psoriasis. No therapy other than reassurance is necessary.
Scrotal (Fissured) Tongue
Approximately 1% of infants and 2.5% of children have many folds with deep grooves on the dorsal tongue surface, known as fissured tongue. These impart a pebbled or wrinkled appearance. Some cases are congenital, caused by incomplete fusion of the two halves of the tongue; others develop in association with infection, trauma, malnutrition, or low vitamin A levels. Many patients with fissured tongue also have geographic tongue. Food particles and debris may become trapped in the fissures, resulting in irritation, inflammation, and halitosis. Careful cleansing with a mouth rinse and soft-bristled toothbrush is recommended.
Black Hairy Tongue
Black hairy tongue is a dark coating on the dorsum of the tongue caused by hyperplasia and elongation of the filiform papillae; overgrowth of chromogenic bacteria and fungi and entrapped pigmented residues that adsorb to microbial plaque and desquamating keratin may contribute to the dark coloration. Changes often begin posteriorly and extend anteriorly on the dorsum of the tongue. The condition is most common in adults but may also manifest during adolescence. Poor oral hygiene and bacterial overgrowth, treatment with systemic antibiotics such as tetracycline (which promotes the growth of Candida spp.), and smoking are predisposing factors. Improved oral hygiene and brushing with a soft-bristled toothbrush may be all that is necessary for treatment.
Oral Hairy Leukoplakia
Oral hair leukoplakia occurs in approximately 25% of patients with AIDS but is rare in the pediatric population. It manifests as a mostly asymptomatic white thickening and accentuation of the normal vertical folds of the lateral margins of the tongue. The mucosa is white and irregularly thickened but remains soft. The condition may spread occasionally to the ventral tongue surface, the floor of the mouth, the tonsillar pillars, and the pharynx. The condition is due to Epstein-Barr virus, which is present in the upper layer of the affected epithelium. The plaques have no malignant potential. The disorder occurs predominantly in HIV-infected patients but may also be found in individuals who are immunosuppressed for other reasons, such as organ transplantation, leukemia, chemotherapy, and long-term use of inhaled steroids. The condition is generally asymptomatic and does not require therapy.
Acute Necrotizing Ulcerative Gingivitis (Vincent Stomatitis, Fusospirochetal Gingivitis, Trench Mouth)
Acute necrotizing ulcerative gingivitis manifests as punched-out ulceration, necrosis, and bleeding of interdental papillae. A grayish white pseudomembrane may cover the ulcerations. Lesions may spread to involve the buccal mucosa, lips, tongue, tonsils, and pharynx and may be associated with dental pain, a bad taste, low-grade fever, and lymphadenopathy. It occurs most commonly in the 2nd or 3rd decade, particularly in the context of poor dental hygiene, scurvy, or pellagra.
Noma
Noma is a severe form of fusospirillary gangrenous stomatitis that occurs primarily in malnourished children 2-5 yr of age who have had a preceding illness such as measles, scarlet fever, tuberculosis, malignancy, or immunodeficiency. It manifests as a painful, red, indurated papule on the alveolar margin, followed by ulceration and mutilating gangrenous destruction of tissue in the oronasal region. The process may also involve the scalp, neck, shoulders, perineum, and vulva. Noma neonatorum manifests in the first month of life as gangrenous lesions of the lips, nose, mouth, and anal regions. Affected infants are usually small for gestational age, malnourished, premature, and frequently ill, particularly with Pseudomonas aeruginosa sepsis. Care consists of nutritional support, conservative debridement of necrotic soft tissues, empirical broad-spectrum antibiotics such as penicillin and metronidazole, and, in the case of noma neonatorum, antipseudomonal antibiotics (Chapter 43).
Altenburg A, Zouboulis CC. Current concepts in the treatment of recurrent aphthous stomatitis. Skin Therapy Lett. 2008;13:1-4.
Bischoff EWMA, Uijen A, van der Wel M. Aphthous ulcers. BMJ. 2009;339:345-346.
Gonsalves WC, Chi AC, Neville BW. Common oral lesions: part 1. Superficial mucosal lesions. Am Fam Physician. 2007;75:501-507.
Nico MM, Park JH, Lourenco SV. Mucocoele in pediatric patients. Pediatr Dermatol. 2008;25:308-311.
Piperi E, Omile J, Pambuccian S, et al. Oral hairy leukoplakia in HIV-negative patients: report of 10 cases. Int J Surg Pathol. 2008. epub doi:10.1177/1066896908327865