General Anesthetics
1 Summarize the history of general anesthesia in dentistry.
2 Describe how general anesthesia works and the stages and planes involved.
3 Compare and contrast the classifications of general anesthesia.
4 Discuss the use of nitrous oxide in dentistry, including how it works, the pharmacologic effects, adverse reactions, and contraindications.
5 Name and describe several types of halogenated hydrocarbons.
6 Identify and describe several other types of general anesthesia.
The state of general anesthesia is produced by a heterogeneous group of potent central nervous system (CNS) depressants. They produce a reversible loss of consciousness and insensibility to painful stimuli. Contemporary general anesthetic techniques use balanced anesthesia that uses a combination of drugs to minimize adverse reactions, taking into account the patient’s physical status and preanesthetic and postanesthetic needs. Respiratory depression and loss of protective reflexes are associated with general anesthesia; thus the patient must be constantly monitored and evaluated. Because of the variety of anesthetic agents and techniques used, special training and a complete working knowledge of the pharmacology of each anesthetic is essential.
The hospital operating room provides the optimal setting for procedures requiring general anesthesia because of the ready availability of monitors for vital signs, resuscitative equipment, and trained anesthesia personnel. However, oral and maxillofacial surgeons have used general anesthetic drugs in their offices for many years with an excellent safety record. Nitrous oxide, because it is not a complete anesthetic, is not useful alone as a general anesthetic. In the dental office, it is commonly employed to allay patient anxiety. Other general anesthetic drugs, in less than anesthetic doses, are now used to provide conscious sedation in the dental office. In today’s practice, the dental health team should have an understanding of the principles of general anesthesia because it is an indispensable tool for the needs of special patients and for extensive oral and maxillofacial surgery.
HISTORY
The original methods to produce general anesthesia involved either strangulation or cerebral concussion. Later, opium, belladonna, hemp, and alcohol were used to render patients unconscious. During this time, the surgeries were “quick and dirty.” Nitrous oxide was discovered in 1776, and 20 years later Sir Humphrey Davy suggested that the administration of nitrous oxide might be useful in surgery.
Gardner Quincy Colton, a traveling showman, began giving public demonstrations of “laughing gas” (nitrous oxide) for 25 cents admission (similar to the “hits” of nitrous oxide placed in balloons that are sold in New Orleans). Horace Wells, a dentist, attended one of Colton’s lectures, at which a drug clerk volunteered to receive the gas. A fight commenced, and the clerk gashed his leg; under Wells’ questioning, the clerk said that he felt no pain. The next day Wells extracted one of his own teeth after having administered nitrous oxide and felt no pain.
Wells began using nitrous oxide in his own dental practice. Finally, he persuaded William T. G. Morton, a former dental partner who was studying medicine, to arrange a demonstration of nitrous oxide before the Harvard University medical faculty. During the demonstration, the patient awoke too soon and began screaming. Nitrous oxide’s low potency accounted for its failure (it is an incomplete anesthetic without anoxia).
Soon after, ether was manufactured and ether “jags” (sort of like parties) were held. Morton practiced administering these drugs to himself and the family dogs and cats. His demonstration of the use of ether began with the surgeon turning to Morton and stating, “Well, sir, your patient is ready.” After using ether successfully to anesthetize the patient, Morton said to the surgeon, “Here’s your patient!” The surgeon replied, “Gentlemen, this is no humbug.”
In the following months, Morton attempted to patent ether and spent the remainder of his life futilely trying to collect claims for compensation from the U.S. government. Both Wells and Morton committed suicide because they did not get credit for their “finds.” Although the accomplishments of these dentists were not recognized during their lifetimes, the medical and dental professions today applaud their contribution to methods of alleviating pain.
About the middle of the 1800s, true general anesthetics were discovered in the United States.
MECHANISM OF ACTION
Many theories have been proposed to explain the mechanism of action of the various general anesthetic agents, but unfortunately none of them does so completely. It may seem relatively simple to say that these drugs are CNS depressants. However, the way in which they depress the normal functions of the CNS is complicated by the lack of knowledge of the physiologic and biochemical events of arousal and unconsciousness. Proposed mechanisms for the action of different general anesthetics involve an increase in the threshold for firing, facilitation of inhibitory γ-aminobutyric acid (GABA), and a decrease in duration of opening of nicotinic receptor-activated cation channels. The increase in the threshold or hyperpolarization is a result of the activation of the potassium channels.
Stages and Planes of Anesthesia
The degree of CNS depression produced by general anesthetics must be carefully titrated to avoid excessive cardiorespiratory depression. In 1920, Guedel described a system of stages and planes to describe the effects of anesthetics (Table 10-1). Although Guedel’s classification applied to the effects produced by ether when using the open drop method of administration, modern anesthetic techniques seldom show these exact stages. However, the four stages are briefly described because Guedel’s terminology is still used to describe the depth of anesthesia.
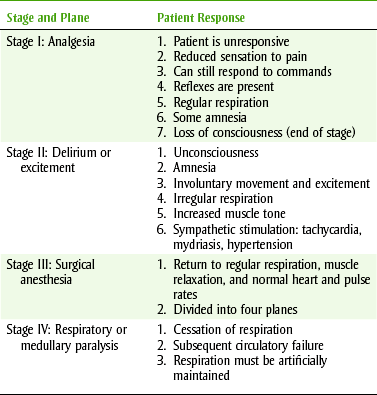
Induction is the term used to refer to the quick change in the patient’s state of consciousness from stage I to stage III, as follows:
1. Stage I analgesia is characterized by the development of analgesia or reduced sensation to pain. The patient is conscious and can still respond to command. Reflexes are present, and respiration remains regular. Some amnesia may also be evident. Nitrous oxide, as used in the dental office, maintains the patient in stage I. The end of this stage is marked by the loss of consciousness.
2. Stage II delirium or excitement begins with unconsciousness and is associated with involuntary movement and excitement. Respiration becomes irregular, and muscle tone increases. Sympathetic stimulation produces tachycardia, mydriasis, and hypertension. This can be an uncomfortable time for the patient because emesis and incontinence can occur. As the depth of anesthesia increases, the patient begins to relax and proceeds to stage III. To ensure the patient’s comfort and safety, it is important to have a smooth and rapid induction. The ultrashort-acting barbiturates accomplish this readily. When balanced anesthesia is used, the patient does not pass through each stage as listed. Adjunct drugs reduce the side effects of each of the drugs used during surgery.
3. Stage III surgical anesthesia is the stage in which most major surgery is performed. This stage is further divided into four planes that are differentiated based on eye movements, depth of respiration, and muscle relaxation. The onset of stage III (planes I and II) is typically characterized by the return of regular respiratory movements, muscle relaxation, and normal heart and pulse rates. Reflexes associated with the eye disappear during planes I and II. Vomiting reflex stops during stage II, but swallowing reflex is maintained until stage III, plane I. Plane III is associated with decreased skeletal muscle tone, dilated pupils, tachycardia, and hypotension. Beginning in plane III and progressing to plane IV, stage III is characterized by intercostal muscle paralysis (diaphragmatic breathing remains), absence of all reflexes, and extreme muscle flaccidity. If the depth of anesthesia is allowed to increase, the patient will rapidly progress to the last stage with cessation of all respiration.
4. Stage IV respiratory or medullary paralysis is characterized by complete cessation of all respiration (diaphragmatic respiration is the last to go) and subsequent circulatory failure. At this point, pupils are maximally dilated and blood pressure falls rapidly. If this stage is not reversed immediately, the patient will die. Respiration must be artificially maintained.
Modern anesthetic techniques now use more rapidly-acting agents than those associated with the four stages of Guedel. Flagg’s approach, used to describe the levels of anesthesia (Figure 10-1), includes the following categories:
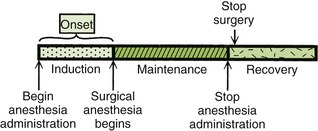
1. Induction: The induction phase encompasses all the preparation and medication necessary for a patient up to the time the operation begins, including preoperative medications, adjunctive drugs to anesthesia, and anesthetics required for induction.
2. Maintenance: The maintenance phase begins with the patient at a depth of anesthesia sufficient to allow surgical manipulation and continues until completion of the procedure.
3. Recovery: The recovery phase begins with the termination of the surgical procedure and continues through the postoperative period until the patient is fully responsive to the environment.
ADVERSE REACTIONS
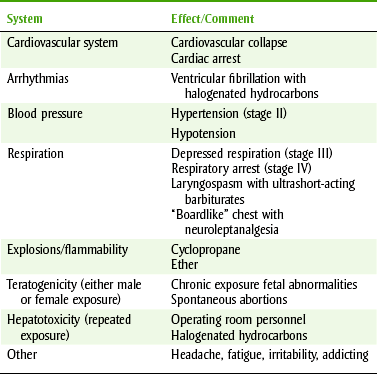
The goals of surgical anesthesia are good patient control, adequate muscle relaxation, and pain relief. To produce anesthesia, potent CNS depressants are given in relatively high doses, and many combinations of drugs are used in balanced anesthesia. The hazards encountered with the administration of general anesthetics are summarized in Table 10-2.
GENERAL ANESTHETICS
Classification of Anesthetic Agents
The general anesthetic agents can be classified according to their chemical structure or route of administration. Table 10-3 categorizes the agents according to their routes of administration.
TABLE 10-3
CLASSIFICATION OF GENERAL ANESTHETICS BY ROUTE OF ADMINISTRATION
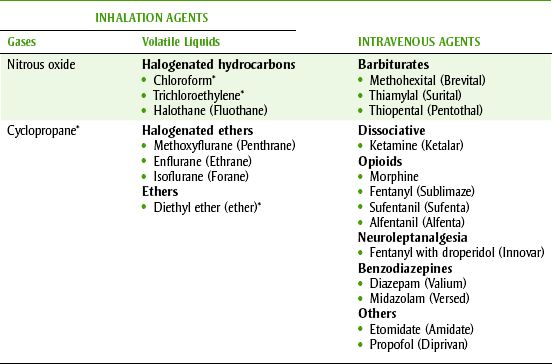
*Of historic interest only.
 INHALATION ANESTHETICS
INHALATION ANESTHETICS
Inhalation agents can be divided into gases and volatile liquids. The liquids are vaporized and carried to the patient in the form of gas. The inhalation agents are often used in combination, using oxygen as a carrier gas.
The volatile general anesthetics are liquids that evaporate easily at room temperature because of their low boiling points. They are classified chemically as halogenated hydrocarbons because they contain fluorine, chlorine, or bromine in their structure. These are potent agents with limited solubility in body tissues, and they have successfully replaced the use of ether in anesthesia. Both methoxyflurane and halothane are used infrequently; enflurane and isoflurane are the more popular volatile liquids in current use.
PHYSICAL FACTORS
The concentration of anesthetic in the inspired mixture is proportional to its partial pressure or tension. The depth of anesthesia produced is a function of the tension (partial pressure) of the anesthetic agent in the brain. The most important physical factors that influence brain anesthetic tension are the tension of the anesthetics in the inspired gases, the rate and volume of delivery of anesthetics to the lungs, and the anesthetic’s solubility in body tissues. Induction can be hastened with high initial anesthetic concentrations and hyperventilation. As anesthesia depth develops, both the concentration and rate of delivery are reduced to maintenance levels.
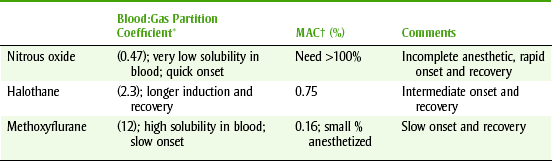
Table 10-4 gives the physical properties of some of the anesthetics. The solubility in blood is expressed by the blood/gas partition coefficient. The less soluble the anesthetic is in body tissues, the more rapid the onset and recovery. The low solubility of nitrous oxide (0.47) correlates well with its rapid onset and recovery. This physical factor allows the anesthesiologist to adjust quickly the desired level of anesthesia. In contrast, halothane, with its higher solubility (2.30), has a longer induction and recovery and changes in level of anesthesia occur more slowly.
TABLE 10-4
PHYSICAL PROPERTIES OF SELECTED INHALATION GENERAL ANESTHETICS
*Partition coefficient (relative distribution by area; blood, brain, gas).
†MAC, Minimal alveolar concentration (amount that anesthetizes 50% of people).
The term minimum alveolar concentration (MAC) is used to compare the potency of general anesthetic inhalation agents. MAC is defined as the minimal alveolar concentration of an anesthetic at 1 atmosphere required to prevent 50% of patients from responding to a supramaximal surgical stimulus. The MAC of nitrous oxide is greater than 100, whereas halothane has a MAC of 0.75, isoflurane of 1.15, and enflurane of 1.68. The lower MAC values indicate the more potent anesthetics. The volatile anesthetics are given in combination with nitrous oxide to reduce the concentration of each while improving MAC values.
INTRAVENOUS ANESTHETICS
The intravenously administered general anesthetics are a diverse group of CNS depressants that include the opioids, the ultrashort-acting barbiturates, and the benzodiazepines. Although most injectable general anesthetics are administered intravenously, one agent, ketamine, can also be given intramuscularly. These drugs find their greatest utility in induction of general anesthesia but may occasionally be used as single agents for short procedures. Although they offer the advantage of convenience, the depth and duration of anesthesia are less easily controlled compared with the inhalation agents. Certain drugs of this group are used in less than anesthetic doses to produce conscious sedation (reflexes retained).
Nitrous Oxide
Nitrous (NYE-trus) oxide (N2O) is a colorless gas with little or no odor and is the least soluble in blood of all the inhalation anesthetics. Because of its low potency (MAC >100), nitrous oxide used alone is unsatisfactory as a general anesthetic agent. However, if anesthesia is first induced with a rapidly acting intravenous (IV) agent and nitrous oxide-oxygen (O2) combination (N2O-O2) is administered in combination with a volatile anesthetic, excellent balanced anesthesia is produced. This synergistic combination permits the use of reduced doses of the more potent inhalation anesthetics. N2O-O2 is given throughout most surgical procedures that necessitate the use of general anesthesia because it reduces the concentration of other agents needed to obtain the desired depth of anesthesia.
Administration of N2O-O2 has become a primary part of dental office anxiety reduction procedures. This use should not be confused with general anesthesia because the intent is to provide for a lightly sedated and relaxed patient. When nitrous oxide is properly administered, the patient remains conscious with the protective reflexes intact. Nitrous oxide provides anxiety relief coupled with analgesia. Thus the N2O-O2 sedation technique may be adopted to offer increased patient cooperation and comfort in a wide range of dental office procedures. The dental practitioner should be thoroughly familiar with this use of nitrous oxide. The dentist (and in some states the hygienist) may legally administer nitrous oxide.
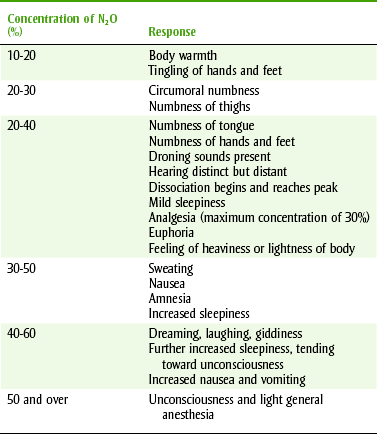
N2O-O2 sedation technique involves increasing the concentration of nitrous oxide to titrate the patient to a desired level of sedation. The gas mixture is delivered to the patient by flowmeters that control both the volume flow and the ratio of nitrous oxide to oxygen. Starting with 100% oxygen for 2 to 3 minutes, nitrous oxide is gradually added in 5% to 10% increments until the patient response indicates that the desired level of sedation has been achieved. Once the nitrous oxide is added, onset occurs rapidly within 3 to 5 minutes. Table 10-5 shows the typical responses observed with increasing concentrations of nitrous oxide. The percent of nitrous oxide required for patient comfort is variable and may range from 10% to 50% (average 35%).
TABLE 10-5
SIGNS AND SYMPTOMS IN RESPONSE TO NITROUS OXIDE AND OXYGEN CONSCIOUS SEDATION
From Clark M, Brunick A: Handbook of nitrous oxide and oxygen sedation, ed 3, St. Louis, 2008, Mosby.
At the termination of a N2O-O2 sedation procedure, the patient should be placed on 100% oxygen for at least 5 minutes. Recovery occurs rapidly as nitrous oxide is quickly removed from the tissues. If the mask is removed without the oxygen recovery period and the patient allowed to breathe room air, a phenomenon known as diffusion hypoxia may result. This occurs because of the rapid outward flow of nitrous oxide accompanied by oxygen and carbon dioxide. The loss of carbon dioxide, a stimulant to respiratory drive, could decrease ventilation with resultant hypoxia. Patients may complain of headache or other side effects if this occurs. Recovery with 100% oxygen avoids this problem.
As has been implied, the N2O-O2 technique has sufficient advantages to recommend its consideration in many dental procedures. Among its advantages are the following:
• Rapid onset: Because of the poor solubility of nitrous oxide in blood, it has a rapid onset of action (<5 minutes).
• Easy administration: No injection is required to obtain an effect. The patient merely breathes through his or her nose.
• Close control: The proper depth of sedation can be maintained by adjusting the percentage of nitrous oxide administered.
• Rapid recovery: Recovery is obtained rapidly with a full return to presedative psychomotor capacity. Thus the need for the patient to be accompanied to the dental appointment can often be eliminated.
• Acceptability for children: Nitrous oxide is a valuable adjunct in managing some apprehensive children. However, it cannot be used when a child’s behavior is openly defiant or hysterical, and it is not a substitute for good behavioral management techniques. The analogy of “going into space” can be effective.
• Relaxed dental team: The N2O-O2 technique not only will offer comfort to the patient and increase the acceptance of dental procedures but also will afford more relaxed treatment, that is, the dental team should be less tense and fatigued at the end of the office day.
PHARMACOLOGIC EFFECTS
Central Nervous System Sedation: Sedation is the main pharmacologic effect of nitrous oxide on the CNS, resulting in analgesia and amnesia. Although there is sensory depression, auditory perception is not affected to the same degree. Therefore a tranquil, quiet environment is required for N2O-O2 analgesic procedures. The use of personal audio input may be useful.
Cardiovascular Effects: Peripheral vasodilation is produced by nitrous oxide administration. This property may facilitate venipuncture should an IV route be desired after starting the N2O-O2.
Gastrointestinal Effects: Nausea and vomiting with N2O-O2 analgesia are uncommon but can occur. The patient should eat a light meal before the appointment but should be warned to avoid a large meal within 3 hours of the appointment.
Changing the concentration of nitrous oxide slowly and monitoring the patient closely can minimize this response. When nitrous oxide is administered slowly, its effects may be evaluated according to Table 10-5 and are summarized as follows:
• The best indicator of the degree of sedation is the patient’s response to questions. The patient may exhibit slurred speech or a slow response. One should not evaluate only as anesthesia is adjusted. The dental practitioner should perform repeated evaluations throughout the dental procedure. Examples of evaluations are asking the patient to “open your mouth” or “move one finger” and noting the patient’s response (can be slow, but the patient should respond).
• The patient is relaxed and cooperative and reports a feeling of euphoria. Local anesthetic injections elicit little if any response at this time. Analgesia produced by nitrous oxide is variable but can be equivalent to morphine injection in patients.
• The patient is easily able to maintain an open-mouth position in the desired plane.
• The patient’s eyes may be closed but can be opened easily.
• The respiration, pulse rate, and blood pressure are within normal limits.
In addition to the features already mentioned, the patient often indicates that the time frame the procedure occupied in his or her consciousness has been dramatically decreased. The operating time may appear to the patient to be one-third or one-half as long as it is in reality. This can be especially beneficial in long procedures, particularly in dental schools. Interesting audio input acts as a distractor for both hearing and feeling sensations.
ADVERSE REACTIONS
Invariably, complications that have occurred with the use of N2O-O2 techniques have been the result of misuse or faulty installation of equipment. Obviously, an installation that crossed oxygen and nitrous oxide lines could be disastrous if nitrous oxide were given under the assumption that it was oxygen. (This has occurred, and taking off the mask would have saved the patient’s life.) Cases of dentists abusing N2O, including use of solely N2O, and taping the mask to the face have resulted in reported deaths.
All cylinders are now colored in a standardized manner. Nitrous oxide cylinders are blue, and oxygen cylinders are green. The cylinders are also “pin coded” to prevent inadvertent mixing of cylinders and lines.
Equipment with built-in safety features is now available. Modern equipment has built-in features that allow no more than 70% of N2O to be dispensed. Oxygen, in the gaseous mixture, must be dispensed at concentrations of 30% or higher during the sedation period. The inhalation administration equipment in every dentist’s office should automatically limit the percentage of nitrous oxide that can be administered and have a fail-safe system that shuts down the nitrous oxide if the oxygen runs out.
The combination of nitrous oxide with other sedative regimens can increase the potential danger of causing a general anesthetic state. The limits of this sedation technique must be understood by every member of the dental health team. If inhalation sedation is combined with other modes of sedation, the entire dental staff must be trained and prepared for the possibility that general anesthesia might be produced.
CONTRAINDICATIONS AND DENTAL ISSUES
Respiratory Obstruction: Because the nasal passages are used for gaseous exchange, upper respiratory obstruction or a stuffy nose is an absolute contraindication to this technique. Other respiratory diseases must also be carefully evaluated.
Chronic Obstructive Pulmonary Disease: In the normal person, the drive for ventilation (breathing) is stimulated by an elevation in the partial pressure of carbon dioxide (Paco2). The partial pressure of oxygen (Pao2) can vary widely without stimulating ventilation in the normal patient. Patients with chronic obstructive pulmonary disease (COPD) have compromised ventilation; thus they experience a gradual rise in Paco2 over time. Because this mechanism becomes resistant to this stimulus, a new stimulant emerges—the partial pressure of Paco2. The patient’s ventilation is then driven by a decrease in Pao2. If a patient with COPD is given oxygen and the Pao2 rises, the stimulant to breathing is removed and there is the possibility of inducing apnea. For patients with COPD American Society of Anesthesiologists Levels III and IV, it is suggested that oxygen be limited to less than 3 L/min. Another recommendation is that patients with severe COPD should be given oxygen by nasal cannula during a dental appointment, especially if pain or stress is expected (increased oxygen demand).
Emotional Instability: Because patients may experience euphoria or an altered sensorium with nitrous oxide analgesia, a patient’s emotional instability is a relative contraindication to its use. Patients taking psychotherapeutic medication must be carefully evaluated before nitrous oxide is used. These medications include phenothiazines, tricyclic antidepressants, and lithium. Fanciful dreams occurring during a procedure may be interpreted on recovery as having actually occurred; therefore a female staff member must be in attendance when a female patient is being treated by a male dentist or dental hygienist and nitrous oxide is used. Aberrant sensations may lead to unfounded accusations unless this requirement is strictly enforced. This is required to minimize legal liability (record in chart).
Safety of the use of nitrous oxide in pregnant patients or administration by pregnant operators is in question. Although no direct correlation has yet been found, several epidemiologic studies cast doubt on the safety of exposure to nitrous oxide during pregnancy. The incidence of spontaneous abortion or miscarriages is higher in female operating personnel chronically exposed to anesthetic agents or in wives of male operators. Women exposed to high levels of nitrous oxide (>5 hours/week) were significantly less fertile than unexposed women. This is especially important to female dentists and dental hygienists because dental operatories have been found to have higher concentrations of gases than even hospital operating rooms (poorer ventilation).
Dental health care workers should be aware of the concentration of nitrous oxide that is present in the dental operatories in which they practice. Machines are available that monitor the concentration of nitrous oxide. Scavenger systems that can retrieve much of the expired gas can be installed, and turnover of the room air can be increased. Checking of the nitrous oxide concentration in the dental operatory should be repeated, especially if the use changes or personnel are pregnant.
Abuse: The dental team should be knowledgeable about the potential hazards associated with the abuse of nitrous oxide. Case histories describing the chronic abuse of nitrous oxide (self-administration) have reported examples of nitrous-induced neuropathy. Symptoms include numbness and paresthesia of the hands or legs that progresses to more severe neurologic symptoms with continued abuse. Nitrous oxide has been shown to reduce the activity of methionine synthetase, the enzyme involved with the function of vitamin B12. Thus it appears that the chronic abuse of nitrous oxide and attendant neurologic symptoms may be related to its effect on the utilization of vitamin B12. Liver and kidney problems have also been mentioned in association with nitrous oxide abuse. The profile of the average dentist who abuses nitrous oxide is male, white, and in his 40s. He has abused many drugs in the past (polydrug abuser) and has previously self-administered nitrous oxide “therapeutically.” As his abuse progresses, he spends more time at the office alone. The number of missed appointments with patients increases, and his attention is focused on issues other than his patients (using the drug again).
Situations that determine that abuse has begun include self-using nitrous oxide, using nitrous oxide for anything other than dental anxiety, using nitrous oxide during lunch or after work, sneaking nitrous oxide use, missing appointments, not keeping promises, and having problems with family or money.
Halogenated Hydrocarbons
Halothane (HA-loe-thane) (Fluothane) has a fruity, pleasant odor and is nonflammable and nonexplosive. Both induction and recovery are relatively rapid. The MAC for halothane is 0.77 but is improved to 0.29 when combined with 70% nitrous oxide. Because halothane is nonirritating to bronchial mucous membranes, it is considered safe for use on asthmatics. As with the other volatile agents, the halothane dose must be carefully regulated to prevent overt respiratory depression. Muscle relaxation is incomplete, and peripheral neuromuscular blocking drugs, such as d-tubocurarine, are required. Halothane also depresses renal function and can cause uterine muscle relaxation.
Halothane’s effects on the cardiovascular system are manifested by increased vagal activity producing bradycardia and peripheral vasodilation that lowers the blood pressure. It sensitizes the myocardium to the cardiac stimulatory effects of injected epinephrine and norepinephrine, leading to serious cardiac arrhythmias such as ventricular fibrillation (Figure 10-2). During surgery, epinephrine is used with halothane and cardiac rhythm is monitored. If arrhythmias occur, antiarrhythmics are administered.
Evidence indicates a causal relationship between halothane use and postanesthetic hepatitis. Approximately 15% of halothane is metabolized in the liver, and these metabolites have been suggested as a cause of liver damage. Although halothane has proved to be a reliable and effective general anesthetic for many years, the occurrence of this adverse effect has diminished its popularity. For this reason, halothane is contraindicated in patients in whom a previous exposure to halothane or other halogenated hydrocarbons has been followed by postanesthetic liver toxicity. Patients with impaired liver function should be treated only with care.
ENFLURANE
Enflurane (EN-floo-rane) (Ethrane) is a halogenated ether anesthetic with a pleasant smell. Induction and recovery are rapid because of its low tissue solubility. The MAC is 0.57 when combined with nitrous oxide. Enflurane depresses respiration, but this effect is controlled with assisted ventilation. It provides good analgesia and muscle relaxation, but supplemental muscle relaxants are still required. The heart is depressed, and blood pressure is reduced. Myocardial sensitization to injected epinephrine is less than that associated with halothane.
Adverse effects associated with enflurane use include alteration in electroencephalographic activity; thus excessive motor activity may occur during anesthesia. Careful regulation of anesthetic depth prevents such muscular activity. Enflurane is metabolized less than other volatile agents, which may account for the absence of hepatotoxicity. Enflurane also produces a transient depression of renal function.
ISOFLURANE
A drug chemically related to enflurane is isoflurane (eye-soe-FLURE-ane) (Forane). Its low tissue solubility allows for rapid induction and recovery. Isoflurane has a slightly pungent smell, limiting the induction concentration, which otherwise could provoke coughing. When isoflurane is combined with 70% nitrous oxide, the MAC is 0.5. The pharmacologic effects of isoflurane are similar to those of the other halogenated ethers and include respiratory depression, reduced blood pressure, and muscle relaxation. Only a small amount of isoflurane undergoes metabolism, and liver toxicity does not seem to be a problem. Limited if any myocardial sensitization to injected epinephrine occurs. Nausea, vomiting, and shivering on recovery are comparable to responses to other anesthetic agents. The most undesirable side effect is respiratory acidosis associated with deeper levels of anesthesia. Isoflurane has proved to be a useful and popular drug for general anesthesia.
DESFLURANE AND SEVOFLURANE
The newest halogenated hydrocarbons include desflurane and sevoflurane. They have the advantage of having low blood/gas partition coefficient so that they have a more rapid onset and a shorter duration of action than the other halogenated hydrocarbon anesthetics. Unfortunately, they have other difficulties. Desflurane’s low volatility requires a special vaporizer. Because it induces cough and laryngospasm, it cannot be used for induction. Its recovery, despite its physical properties, does not appear to be faster than that of older agents. Sevoflurane is chemically unstable when exposed to carbon dioxide absorbents, producing a potentially nephrotoxic compound. Because it releases fluoride (F−) when metabolized, renal damage may occur.
Other General Anesthetics
ULTRASHORT-ACTING BARBITURATES
The ultrashort-acting barbiturates used include methohexital (meth-oh-HEX-i-tal) sodium (Brevital), thiopental (thye-oh-PEN-tal) sodium (Pentothal), and thiamylal (thye-AM-i-lal) sodium (Surital). Although the basic pharmacology of the barbiturates is discussed in Chapter 11, certain facts about these drugs are discussed here.
These ultrashort-acting agents have a rapid onset of action (about 30 to 40 seconds) when given intravenously. Figure 10-3 demonstrates the percentage of the dose in each tissue over time. One should note that the dose begins in the blood, rapidly goes to the brain (lipid soluble), redistributes to lean tissues (muscles with high vascularity), and finally moves to the fat (lipid soluble, but low perfusion). If repeated doses are given, as is often the case during anesthesia, the drug accumulates in body tissues, resulting in prolonged recovery.
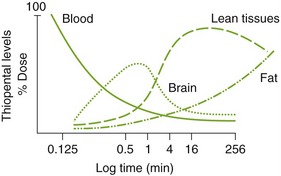
FIGURE 10-3 Thiopental concentrations in various tissues: fat, muscle (lean tissues), blood, and brain.
If these drugs are used as the sole anesthetic for short procedures, the patient will respond to painful stimuli. Because no analgesia is observed with doses that allow the patient to breathe spontaneously, the intravenously administered barbiturates function more effectively when used with a local anesthetic agent as part of a balanced anesthetic technique.
A serious complication with the use of IV barbiturates occurs when the solution is accidentally injected extravascularly or intraarterially. Symptoms with extravascular infiltration can range from tissue tenderness to necrosis and sloughing. Intraarterial injection is extremely dangerous and can lead to arteriospasm associated with ischemia of the arm and fingers and severe pain.
Other complications with ultrashort-acting barbiturates include laryngospasm and bronchospasm. In some patients, hiccoughs, increased muscle activity, and delirium occur on recovery. Premedication with atropine or opioids has proved reasonably effective in reducing these recovery problems.
The absolute contraindications to the use of ultrashort-acting barbiturates include an absence of suitable veins for administration, status asthmaticus, porphyria, or known hypersensitivity. The dose should be adjusted, and caution should be taken in patients with asthma or hepatic, renal, or cardiovascular impairment. These drugs can be used alone by trained and qualified practitioners for very short dental procedures or as part of a balanced anesthesia to induce surgical anesthesia (going from stage I to stage III). Because these drugs are potent anesthetics, they should be administered only by qualified individuals, with resuscitation equipment readily available.
PROPOFOL
One of the general anesthetics unrelated to any other general anesthetic is propofol (PROE-po-fole) (Diprivan). It is an IV anesthetic that produces an onset of anesthesia in 30 seconds (similar to the barbiturates) and a duration of action of about 5 minutes. Patients “feel better” and begin ambulation sooner than with other agents. It produces little vomiting and may have antiemetic effects. Propofol can be used for induction and for maintenance of balanced anesthesia. It is popular for outpatient surgery. Propofol is metabolized in the liver by conjugation to glucuronide and sulfate and excreted in the kidneys with a half-life of 30 to 60 minutes.
Propofol can produce a marked decrease in blood pressure during induction because it produces vasodilation. Apnea occurs in 50% to 80% of patients given propofol. Bradycardia and pain at the injection site can occur. Gastrointestinal adverse reactions have been reported. Hypersensitivity reactions involving hypotension, flushing, and bronchospasm occurred when propofol was dissolved in the original vehicle (polyoxyethylated castor oil) (Cremophor), but this reaction does not occur when it is dissolved in a fat emulsion (Intralipid) or soybean oil. Propofol is a relatively costly anesthetic.
KETAMINE
The anesthetic ketamine (KEET-a-meen) (Ketalar) is related chemically to phencyclidine (PCP), a hallucinogen. The anesthetic state ketamine produces has been given the name dissociative anesthesia because ketamine appears to disrupt association pathways in the brain. Under ketamine, the patient appears to be catatonic and has amnesia; ketamine produces analgesia without actual loss of consciousness.
Ketamine may be given intravenously or intramuscularly, with a rapid (1 to 2 minutes) onset of action occurring with either route. It is distributed first to lipid tissues then to more vascular areas. Pharyngeal and laryngeal reflexes remain active, and there is little respiratory change. Ketamine increases cerebral blood flow and stimulates the heart to increase cardiac output. Because excessive salivation is a common finding with ketamine, atropine is a necessary premedication. Muscle tone may increase during its use.
The principal drawback to the use of ketamine is the occurrence of “emergence phenomena,” including delirium and hallucinations during recovery. This happens most often in adults, older children, and drug abusers. Reactions of this type can be minimized if visual and auditory stimuli are reduced during recovery. Small doses of an ultrashort-acting intravenously administered barbiturate or benzodiazepine have been used to control the recovery problem. Specific contraindications include a history of cerebrovascular disease, hypertension, and hypersensitivity to the drug. Psychiatric problems present a relative contraindication. Because protective reflexes of the pharynx and larynx are active, care should be taken not to stimulate the pharynx. This increase in reflexes in the throat may discourage use in dentistry.
OPIOIDS
The opioids (OH-pee-oyds) have long been used as adjunctive drugs to general anesthesia in preanesthetic medication and to provide analgesia during and after a surgical procedure. Now opioids are used as anesthetic agents as well. The opioids used include morphine, fentanyl (Sublimaze), sufentanil (Sufenta), and alfentanil (Alfenta). These drugs do not significantly alter cardiovascular function or peripheral resistance. Prolonged respiratory depression is the major disadvantage and requires careful attention to ventilatory function throughout the anesthetic period. Reversal of this depression can be produced by the opioid antagonist naloxone.
DROPERIDOL PLUS FENTANYL
The term neuroleptanalgesia refers to the so-called wakeful anesthetic state produced by the combination of a neuroleptic drug, droperidol (Inapsine), and a potent opioid analgesic, fentanyl (Sublimaze). Droperidol produces marked sedation and a catatonic state. It is a close relative of haloperidol, an antipsychotic agent. The combination of drugs is marketed as Innovar and is usually given intravenously for a rapid onset. Adding nitrous oxide results in neuroleptanesthesia. Return to consciousness appears to be rapid, but the effects of droperidol are long lasting and recovery is slow.
The adverse effects can be serious and include those that would normally be associated with the opioids and major tranquilizers. Respiratory depression and extrapyramidal tremors have occurred. This combination of drugs should be used with great care, especially in patients with pulmonary insufficiency and parkinsonism. A boardlike chest, associated with intercostal muscle paralysis and requiring ventilatory support, has occurred in some patients using IV opioids. Fentanyl is sometimes used as a sole agent for sedation.
BENZODIAZEPINES
The anxiolytic benzodiazepines have been an integral part of conscious sedation and preanesthetic medication for years. Diazepam (Valium) has been used intravenously for many years. Midazolam (Versed), which is water soluble, does not need a solvent for solution, so one of diazepam’s major side effects, thrombophlebitis, can be avoided. Other advantages include that it has a shorter duration of action and produces more amnesia than diazepam. Parenteral lorazepam is also available for similar uses. The benzodiazepines find their greatest application as adjunctive drugs in the balanced anesthesia technique or for conscious sedation. They are discussed in detail in Chapter 11.
BALANCED GENERAL ANESTHESIA
The goals of surgical anesthesia are good patient control, adequate muscle relaxation, and pain relief. There are many agents that can produce general anesthesia. Each drug has its own adverse reaction profile. The many specific steps in Guedel’s classification were developed for describing the effects obtained when ether was used alone. When balanced anesthesia is used, the patient readily passes from stage I to stage III (surgical anesthesia), skipping over the signs of stage II. The ultrashort-acting IV barbiturates accomplish this readily. These barbiturates are combined with the N2O-O2 in combination, which are then administered along with a volatile inhalation anesthetic (e.g., halogenated hydrocarbons). If local anesthetic blocks are administered before oral surgery procedures, the depth of general anesthesia can be lighter.
CLINICAL SKILLS ASSESSMENT
1. Name and describe the four stages of anesthesia.
2. State the pharmacologic effects of the general anesthetics.
3. Describe the effects observed with varying concentrations of nitrous oxide.
4. What are the adverse reactions associated with nitrous oxide?
5. List the contraindications to the use of nitrous oxide.
6. State the potential hazards associated with the general anesthetic agents.
7. Describe which general anesthetics would be useful in the following situations:
b. A patient requiring oral surgery.
8. Explain the rationale for the use of several agents during general anesthesia.
 Please visit http://evolve.elsevier.com/Haveles/pharmacology for review questions and additional practice and reference materials.
Please visit http://evolve.elsevier.com/Haveles/pharmacology for review questions and additional practice and reference materials.