Antianxiety Agents
1 Discuss the value of patient relaxation in dentistry.
2 Describe the mechanism of action, interactions, and dental relevance of the benzodiazepines and barbiturates.
3 Name and briefly describe the mechanism of action of the nonbenzodiazepine-nonbarbiturate sedative-hypnotics and the nonbenzodiazepine-nonbarbiturate receptor agonists.
4 Name a melatonin receptor agonist and summarize its actions.
5 Explain the workings of the centrally acting muscle relaxants and how they are used.
6 Discuss some general precautions about which the dental practitioner should be aware with the use of antianxiety agents.
Both the dentist and the dental hygienist recognize the value of a relaxed patient. Often, patient anxiety is sufficiently reduced by a calm, patient, confident, and understanding attitude on the part of the dental health care workers. However, individual responses to dental treatment vary widely, ranging from total relaxation and even sleeping to severe apprehension and the inability to approach the dental office, much less the dental chair. Each dental patient should be provided with the most pleasant experience possible within the limits of safety. When the patient is relaxed, appointments can be more productive, and the dentist, hygienist, and patient all benefit.
Dental professionals, because of their familiarity with all of dentistry’s components and ramifications, often do not understand the basis of anxiety in the dental patient. Often, dental health care workers lack empathy and even commonly blame or fault the patient for his or her discomfort. Members of the dental team often become defensive because they do not feel comfortable and do not know how to manage these intense feelings. By acting perturbed, the dental team reinforces the patient’s negative feelings about the dental appointment. A dental practitioner who decides that anxiety control is only necessary for the first third of a dental appointment does not understand patient anxiety and its treatment.
Many patients who require dental care never go to the dental office because of fear and apprehension. A common misconception is that dental patients who express anxiety are just “looking for drugs.” The average dental patient who is being treated for dental anxiety during the appointment does not get the opportunity to abuse antianxiety agents. The appropriate use of antianxiety agents might encourage more patients to seek needed dental treatment. If, to treat many nervous dental patients, an occasional patient who was “seeking” antianxiety agents obtains them, that is an appropriate balance in the use of antianxiety agents. It would be unlikely for a person in search of drugs to sit for an hour in the dental chair, have dental treatment performed, and then pay for the treatment just to obtain one tablet of an antianxiety drug that was taken in the dental office. However, prescribing 20 tablets of an antianxiety drug for a patient nervous about getting dentures would be inappropriate.
It is necessary to objectively assess the patient’s anxiety on both the first and subsequent visits. A patient who is clutching the dental chair arms and has white knuckles is not in a relaxed state (Figure 11-1). By questioning and observing the patient, a determination can be made about the need for antianxiety agents. Thus the patient can feel comfortable and relaxed during subsequent dental appointments. The dental health professional should remember that whatever procedure is performed, he or she has performed it many times. However, for many patients, this may be their first experience with the procedure, and their reactions may be altered by their interpretation of what is happening (e.g., “that sharp, pointy thing is going to hurt!” or “what are those gunlike weapons?”).

FIGURE 11-1 White-knuckle syndrome indicates that a patient is not in a relaxed state. (From Clark MS, Brunick A: Handbook of nitrous oxide and oxygen sedation, ed 3, St Louis, 2008, Mosby.)
Of the agents discussed in this chapter, the dental team will most commonly use orally administered drugs to provide relaxation for the anxious patient. Intravenous (IV) administration is used infrequently because it requires more training and experience than most general dentists possess. Most states require a separate certificate to administer IV agents or to provide conscious sedation, and the malpractice insurance is much more expensive. Although orally administered sedatives provide inconsistent or poorly predictable results, practitioners should become familiar with one or two drugs and use them repeatedly. In the long run, this practice will produce greater benefits than changing from drug to drug.
The dose of a particular antianxiety agent effective for a particular patient is vastly variable, involving both intrapatient and interpatient variation. Predicting the correct dose is a guess at best. The amount needed is poorly related to the degree of the patient’s anxiety or the dental procedure to be performed. The normal sedative dose (calms normal patient without dental appointment) is not expected to produce calmness in a dental patient, but the hypnotic dose (that which induces sleep in the normal patient) can often produce the desired degree of sedation before dental treatment.
This chapter discusses some of the agents that can be used to allay anxiety—primarily, the benzodiazepines. Nitrous oxide, which is used in dentistry as an antianxiety agent, is discussed in Chapter 10 because it is classified as a general anesthetic. It is very useful in decreasing apprehension during the dental appointment and is underused in many dental practices. Some drugs with properties of both the antihistamines and phenothiazines, such as hydroxyzine and promethazine, have weak antianxiety properties and are discussed in Chapter 18.
DEFINITIONS
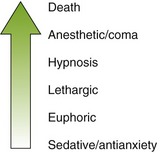
The sedative-hypnotic agents can produce varying degrees of central nervous system (CNS) depression, depending on the dose administered. A small dose will produce mild CNS depression described as sedation (reduction of activity and simple anxiety). This level of CNS depression has some anxiolytic effects. A larger dose of the same drug, the hypnotic dose (inducing sleep), will produce greater CNS depression. Thus the same drug may be either a sedative or a hypnotic, depending on the dose administered. In even larger doses, sedative-hypnotics may produce anesthesia and eventually death (Figure 11-2).
This chapter discusses the benzodiazepines, barbiturates, and the nonbenzodiazepine-nonbarbiturate sedative-hypnotics. The benzodiazepines are discussed first because they are used most often.
BENZODIAZEPINES
The benzodiazepines (ben-zoe-dye-AZ-e-peens) are the most commonly prescribed antianxiety drugs. The members of this group differ mainly in their onset and duration of action, dose, and dose forms available.
Chemistry
These drugs are named benzodiazepines because of their structure: a 1,4-benzodiazepine nucleus. Chlordiazepoxide (klor-dye-az-e-POX-ide) (Librium), the first derivative, was synthesized in 1955. After its success, thousands of other benzodiazepine derivatives were screened for psychopharmacologic activity. As a result of this search, diazepam (Valium) was synthesized in 1959 and marketed in 1963. Many benzodiazepines are now available (Table 11-1).
TABLE 11-1
BENZODIAZEPINES AND MISCELLANEOUS SEDATIVE-HYPNOTIC AGENTS
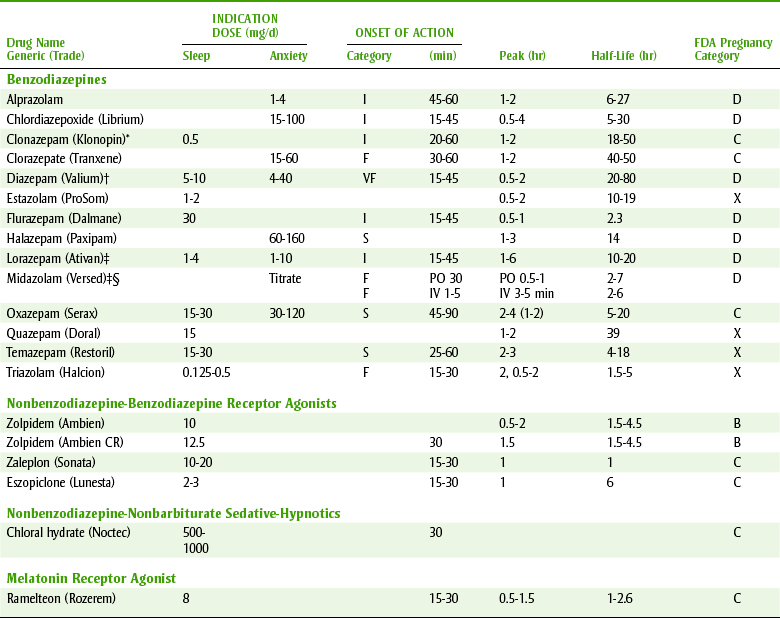
I, Intermediate; F, fast; VF, very fast; S, slow.
*Used as an adjunct to treat certain kinds of seizures.
†Injectable form contains propylene glycol—can produce thrombophlebitis.
‡Available parenterally.
§Midazolam administered intravenously in United States; intravenous form can be given orally.
Pharmacokinetics
The benzodiazepines are well absorbed when administered by the oral route. The rapid onset of action of the benzodiazepines is related to their lipid solubility. Diazepam, which is highly lipid soluble, has a quick onset and is concentrated in the adipose tissue. Storage in adipose tissue prolongs the action of lipid-soluble benzodiazepines. The benzodiazepines are available in the following dose forms: tablets, capsules, oral solution, rectal gel, and injectable forms. The intramuscular (IM) route, for benzodiazepines other than midazolam, gives slow, erratic, and unpredictable results. In contrast, the IV route, for those available in parenteral form, produces a rapid, predictable response that makes them ideal for conscious sedation. Once a benzodiazepine is absorbed, the rate at which it crosses into the cerebrospinal fluid (CSF) through the blood-brain barrier depends on protein binding, lipid solubility, and the ionization constant of the compound. Most benzodiazepines are highly protein bound and are present in the un-ionized, lipid-soluble form. They easily cross the blood-brain and placental barriers to produce an effect in the CNS and on the fetus (Food and Drug Administration [FDA] categories D or X), where they can accumulate with repeated doses.
After absorption, the benzodiazepines are metabolized in the liver by either phase II metabolism or phase I followed by phase II metabolism. Phase I metabolism is decreased in the elderly, in patients taking certain drugs that inhibit hepatic metabolism, and in the presence of hepatic disease. Phase I metabolism results in active metabolites that, with repeated administration, can accumulate. The half-lives of these drugs range from 2 to 200 hours (see Table 11-1).
Benzodiazepines that undergo only phase II metabolism are much less affected by drugs or hepatic disease. Age does not seem to affect phase II metabolism. However, caution should still be used when prescribing these drugs for elderly persons.
Mechanism of Action
Benzodiazepines enhance or facilitate the action of the neurotransmitter γ-aminobutyric acid (GABA), a major inhibitory transmitter in the CNS. It acts in the limbic, thalamic, cortical, and hypothalamic levels of the CNS. Benzodiazepines act as agonists at the benzodiazepine receptor site, thereby reducing the symptoms of anxiety.
Pharmacologic Effects
The pharmacologic effects of the benzodiazepines have qualitatively similar actions but vary in potency.
 BEHAVIORAL EFFECTS
BEHAVIORAL EFFECTS
The clinical effects of these agents in humans are anxiety and panic reduction at lower doses and production of drowsiness and sleep at higher doses. Repeated doses of benzodiazepines reduce rapid eye movement (REM) sleep. Usual doses produce a marked reduction in stages 3 and 4 sleep (deep sleep), which, after long-term use, can interfere with restorative sleep.
ANTISEIZURE EFFECTS
The benzodiazepines, such as diazepam, have antiseizure activity (i.e., they increase the seizure threshold). Diazepam, used parenterally, has been shown to be an effective antiseizure drug for the prevention of seizures associated with local anesthetic toxicity and for the treatment of status epilepticus. Clonazepam, an oral benzodiazepine, is used in combination with other antiseizure drugs to manage partial seizures. The benzodiazepines prevent the spread of seizures in tissues surrounding the anatomic seizure focus (when such a focus exists) but have little effect on the discharges at the focus itself.
MUSCLE RELAXATION
Like all CNS depressants, benzodiazepines can produce relaxation of skeletal muscles. Some studies show benzodiazepines to be superior to other skeletal muscle relaxants for relief of musculoskeletal pain; other studies show the pain relief effect to be no better than aspirin or placebo. Benzodiazepines are effective for muscle spasticity secondary to pathologic states such as cerebral palsy or paraplegia.
Adverse Reactions
In general, benzodiazepines used alone have a wide margin of safety. They all have similar adverse effects but differ in their frequency. Agents with long-elimination half-lives tend to accumulate and produce more side effects.
CENTRAL NERVOUS SYSTEM EFFECTS
The most common side effect attributed to benzodiazepines is CNS depression manifested as fatigue, drowsiness, muscle weakness, and ataxia. These side effects are more likely to occur in elderly persons. The patient may also experience lightheadedness and dizziness. Tolerance to this effect occurs over time. Paradoxical CNS stimulation that produces talkativeness, anxiety, nightmares, tremulousness, hyperactivity, and increased muscle spasticity can occur. This reaction is more common in psychiatric patients, and benzodiazepines should be discontinued if this reaction occurs.
When benzodiazepines are used in dentistry to produce conscious sedation, this side effect of CNS depression is used as the primary effect. The amount of the benzodiazepine used to provide conscious sedation is titrated to the patient’s response. The appearance of ptosis is used as an initial endpoint for the dose administered. These agents have a rapid onset of action and an initial effect of 45 minutes to 1 hour.
Diazepam was the most common benzodiazepine used parenterally until newer benzodiazepines were developed. Diazepam’s long half-life and its metabolism to an active metabolite prolonged its duration of action. Its effect lasted past the dental appointment time and even into the next day.
Midazolam, a water-soluble benzodiazepine, is metabolized primarily to inactive metabolites. This produces an advantage for its IV use over diazepam in conscious sedation. Because these benzodiazepines are inactivated either by metabolism or by metabolism of their active metabolites, the duration and depth of sedation can be magnified by administration of drugs that inhibit the hepatic microsomal enzymes. Agents that inhibit these enzymes include cimetidine and erythromycin.
A potent benzodiazepine named flunitrazepam (flew-nye-TRAY-ze-pam) (Rohypnol) is a benzodiazepine available in Europe but not the United States. Acquired illegally from Europe or Mexico, this benzodiazepine, nicknamed “roofies,” is being used inappropriately in the United States and has been secretly administered to women who were then “date raped.” The muscle flaccidity and amnesia produced by this agent make it difficult for the victim to resist or to testify later. Increasing the penalty for possession of this agent is being considered.
ANTEROGRADE AMNESIA
It can be easily demonstrated that parenteral benzodiazepines, such as diazepam and midazolam, produce amnesia beginning when the drug is taken. This effect is used to therapeutic advantage in patients scheduled for an unpleasant dental procedure. Clinical use has produced episodes of amnesia that can sometimes last several hours and can occur with several benzodiazepines. Oral triazolam seems to have a greater likelihood to produce amnesia than other oral benzodiazepines. Patients should be warned not to sign important papers or make important decisions after benzodiazepines are administered. The mechanism of amnesia results from an impairment of consolidation processes that store the information in the brain.
RESPIRATORY EFFECTS
Usual doses of benzodiazepines have no adverse effect on respiration. However, doses of diazepam administered for outpatient dental procedures have been occasionally reported to produce respiratory depression. An isolated case of apnea after IV diazepam has also been observed. These respiratory effects are more common in elderly patients. The minimal respiratory depression can be exacerbated by opioids or alcohol.
CARDIOVASCULAR EFFECTS
Therapeutic doses of benzodiazepines have no adverse effect on circulation. The relief of anxiety may result in a fall in blood pressure and pulse rate. The pulse rate has also been reported to rise (tachycardia) and then return to normal after a few minutes.
VISUAL EFFECTS
Benzodiazepines are contraindicated in angle-closure (narrow angle) glaucoma and can produce other visual changes such as diplopia, nystagmus, and blurred vision. They may be used in treatment of wide-angle glaucoma, which is the most common kind of glaucoma.
DENTAL EFFECTS
The benzodiazepines have been reported to produce xerostomia, increased salivation (note that these are opposite effects), swollen tongue, and a bitter or metallic taste.
THROMBOPHLEBITIS
Parenteral diazepam can produce thrombophlebitis. Because diazepam is poorly soluble in water, the vehicle propylene glycol is used to solubilize it. The vehicle is responsible for the thrombophlebitis. The incidence is lower when the IV infusion is given in the antecubital space rather than the dorsum of the hand (more blood and faster blood flow). Because midazolam is soluble in water and propylene glycol is not used to solubilize it, it is much less likely to produce this effect. With parenteral use, apnea, hypotension, bradycardia, and cardiac arrest have been reported. These are more frequent with rapid administration. Equipment for respiratory and cardiovascular assistance must be available if these agents are to be used parenterally (e.g., conscious sedation in the dental office). Special training of the dental team administering benzodiazepines is required.
OTHER EFFECTS
Benzodiazepines can affect the gastrointestinal tract, producing cramps or pain, and the genitourinary tract, producing difficulty in urination. They can also produce allergic reactions, including skin rash or itching.
PREGNANCY AND LACTATION CONSIDERATIONS
An increased risk of congenital malformation in infants of mothers taking benzodiazepines in the first trimester has been reported. Cleft lip and palate, microencephaly, and gastrointestinal and cardiovascular abnormalities were greater in the group taking benzodiazepines. Most of these agents are classified as FDA pregnancy category D drugs; triazolam and temazepam are in FDA pregnancy category X (see Chapter 24).
Near-term administration of benzodiazepines to the mother has resulted in floppy infant syndrome. This syndrome includes hypoactivity, hypotonia, hypothermia, apnea, and feeding problems. Because these agents are seldom absolutely needed (except for epilepsy), they should be avoided in women who are or may become pregnant and in nursing mothers. Before administering a benzodiazepine, the pregnancy status of the female patient should be determined. The first trimester, often before the patient knows that she is pregnant, is the time benzodiazepines are more likely to be teratogenic or cause problems in the fetus.
Abuse and Tolerance
Benzodiazepines can be abused, and physical dependence and tolerance have been documented. Physiologic addiction can occur if large doses are taken over an extended period. However, their abuse and addiction potential is less than that of the other sedative-hypnotic agents such as the barbiturates.
Prolonged intake of large doses of benzodiazepines can result in a degree of CNS tolerance. Cross-tolerance also exists between the benzodiazepines and other CNS depressants. This may explain why benzodiazepines can be substituted for ethyl alcohol to relieve the symptoms of delirium tremens precipitated by acute alcohol withdrawal.
One advantage of benzodiazepines over barbiturates is their wider therapeutic index, or range of safe dose. Overdose poisoning with these drugs has been rare and appears to be difficult to achieve when used alone, although apnea has rarely been reported. In most instances, excessively large doses must be ingested to produce respiratory or central vasomotor depression. Combining benzodiazepines with other CNS depressants can reduce the safety so that the combination can be lethal. The addition of alcohol can result in coma, respiratory depression, hypotension, or hypothermia.
TREATMENT OF OVERDOSE
Rarely does the ingestion of a benzodiazepine alone result in severe symptoms. Supportive therapy should be undertaken if symptoms result. With recent ingestion, emesis may be induced. Activated charcoal and a saline cathartic may be administered. The patient’s respiration and blood pressure should be monitored.
To reverse some of the effects of a benzodiazepine, flumazenil (floo-MA-zee-nill) (Romazicon), a benzodiazepine antagonist available for IV administration, may be used. It has been shown to reverse the sedating and psychomotor effects, but reversing the respiratory depression produced by the benzodiazepines is incomplete. The amnesia is not consistently reversed. It has an initial half-life of about 10 minutes and a terminal half-life of about 60 minutes. Side effects include pain at the injection site, agitation, and anxiety. An increase in inadequate analgesia does not occur. Some patients became resedated before the end of 3 hours when high doses of long-acting benzodiazepines were ingested (the antagonist wore off before the agonist had been metabolized and excreted). Administering flumazenil to benzodiazepine-dependent individuals could precipitate withdrawal symptoms (similar to naloxone to opioids).
Drug Interactions
Like other antianxiety agents, benzodiazepines interact in an additive fashion with other CNS depressants, notably alcohol, barbiturates, anticonvulsants, and phenothiazines. Because diazepam and desmethyldiazepam are cytochrome P-450 2C enzyme substrates, enzyme inducers may increase their metabolism and enzyme stimulators may decrease their metabolism.
Smoking reduces the effectiveness of the benzodiazepines. The tars produced by smoking cigarettes stimulate the hepatic microsomal enzymes in the liver. The increased number of liver enzymes increases the rate of metabolism of the benzodiazepines, so a higher dose of a benzodiazepine is required to produce the same effect.
Drugs, such as cimetidine, disulfiram, isoniazid, and omeprazole, may increase the effects of benzodiazepines. Valproic acid may displace diazepam from binding sites, which may result in an increase in sedative effects. Selective serotonin reuptake inhibitors (e.g., fluoxetine, sertraline, or paroxetine) have greatly increased diazepam levels by altering its clearance. Benzodiazepines may reduce the effectiveness of levodopa, and parkinsonism has been exacerbated in these patients. Benzodiazepines may increase the effect of digoxin, phenytoin, and probenecid.
Medical Uses
Benzodiazepines are useful in short-term treatment of anxiety, panic attacks, insomnia, and alcohol withdrawal. They are used for the acute treatment of seizures. Some neuromuscular diseases can be treated with the benzodiazepines. They are used in conscious sedation, general anesthesia, or during surgery.
ANXIETY CONTROL
Generalized anxiety disorder and panic disorder are common indications for use of benzodiazepines in general medicine. Anxiety produces a physiologic response resembling fear, with manifestations including restlessness, tension, tachycardia, and dyspnea. Most well-controlled clinical trials have shown that the antianxiety effect of benzodiazepines is better than those of placebo, barbiturates, and meprobamate. Benzodiazepines also produce less sedation than the classic sedative-hypnotic agents.
INSOMNIA MANAGEMENT
If insomnia is a manifestation of anxiety, sleep will usually improve when a benzodiazepine is administered at bedtime as an antianxiety drug. The benzodiazepines are preferable to the barbiturates as hypnotics because the risk of physical addiction or serious poisoning is much less. The efficacy of the benzodiazepines in the treatment of chronic insomnia has not been demonstrated past 1 month.
The occasional use of the benzodiazepines within controlled limits can be useful. For example, limiting the number of tablets to 10 per month for insomnia will limit tolerance, dependence, and withdrawal. Underlying causes of insomnia, such as depression or alcoholism, should be identified and treated. Nonaddicting agents, such as trazodone, may be useful in the treatment of insomnia, and unlike the benzodiazepines, no tolerance or dependence is produced even with chronic use. Nonpharmacologic management of sleep disorders (Box 11-1) should be instituted before any benzodiazepine is prescribed. Several patients with new prescriptions for “sleeping pills” have discussed the pot of coffee they drink after dinner. (What is wrong with this picture?)
TREATMENT OF EPILEPSY (SEIZURES)
Diazepam or lorazepam is the drug of choice for treatment of repetitive, intractable seizures (status epilepticus) that require IV therapy. They are also used for treatment of seizures caused by local anesthetic toxicity. Orally administered diazepam is of little value, even as a maintenance anticonvulsant. Oral clonazepam is used as an adjunct to other anticonvulsants for some difficult-to-control types of seizures. It is also used in the management of mood disorders.
TREATMENT OF ALCOHOLISM
The benzodiazepines are used in the treatment of the alcohol withdrawal syndrome. Administration of an adequate amount of a benzodiazepine can prevent the emergence of the signs and symptoms of acute alcohol withdrawal, such as agitation and tremor. It has not been shown that they prevent hallucinations or delirium tremens.
CONTROL OF MUSCLE SPASMS
Benzodiazepines are used to control the muscle spasticity that accompanies various diseases such as multiple sclerosis and cerebral palsy. They are used for the relief of pain and spasm of back strain. Studies have suggested that the benzodiazepines are more effective than other muscle relaxants such as methocarbamol, carisoprodol, and chlorzoxazone.
Management of the Dental Patient Taking Benzodiazepines
The dental implications of the benzodiazepines are described in Box 11-2.
DENTAL PROCEDURES
Orally administered diazepam has been shown to be more effective than placebo in allaying apprehension in patients undergoing restorative procedures. It is used in combination with other agents such as opioids and anticholinergic agents. If diazepam is used for the initial treatment of patients with dental anxiety, it is hoped that future appointments may be completed successfully without benzodiazepine increases. For preoperative dental anxiety, a benzodiazepine should be chosen that has a fast onset of action and a relatively short half-life. This reduces the patient’s waiting time and allows resumption of normal functions as soon as possible. The dose used should be in the range of the usual hypnotic dose (see Table 11-1). Examples of agents used for dental anxiety might include triazolam (trye-AY-zoe-lam) (fast onset and short half-life) and diazepam (very fast onset but long half-life). Lorazepam (lor-A-ze-pam) or alprazolam (al-PRAY-zoe-lam) (intermediate onset but relatively short half-lives) could also be used, especially in the elderly. Midazolam (MID-ay-zoe-lam) is available for parenteral (Versed injection) and oral (Versed syrup) use in the United States and is used to sedate children. The parenteral midazolam product can be administered orally to sedate children. Patients given either oral or parenteral benzodiazepines should not be allowed to operate a motor vehicle, and the dental staff should ensure that a driver is present before dismissing the patient.
PREMEDICATION
The benzodiazepines have been used before surgical procedures to allay anxiety. They may be used orally or parenterally. The amnesia that occurs with parenteral administration is especially useful during stressful dental procedures. Diazepam is used as a premedication before general anesthesia, endoscopy, cardioversion, gastroscopy, sigmoidoscopy, and cystoscopy.
CONSCIOUS SEDATION
Conscious sedation using the benzodiazepines is usually accomplished by IV administration. Diazepam, lorazepam, or midazolam, given intravenously, provides muscle relaxation and anterograde amnesia (amnesia occurs to events after the injection) during dental procedures. Although amnesia quickly follows the IV injection of diazepam and midazolam, it depends on several variables. Amnesia may be expected to persist for up to 45 minutes; therefore postoperative instructions should be provided in writing. Benzodiazepines available for parenteral administration (diazepam, midazolam, and lorazepam) are used for conscious sedation. The patient maintains reflexes, but time perception is lost and amnesia reduces the patient’s memory. Because parenteral benzodiazepines have been associated with respiratory depression and arrest when used for conscious sedation, they require continuous monitoring of respiratory and cardiac function. Emergency drugs, equipment, and personnel must be available. Because some states and insurance companies are placing controls on the use of IV sedation in dentistry, those dentists without additional training cannot use conscious sedation. Additional training is now a requirement before dentists can administer parenteral benzodiazepines.
BARBITURATES
Barbiturates (bar-BI-tyoo-rates), the original sedative-hypnotic agents, are chemically related to each other and have similar pharmacologic effects. The barbiturates differ from each other mainly in their onset and duration of action (Table 11-2). Because these agents have been used for years, the problems with their use have been well documented. Barbiturates have long been associated with a high rate of abuse and complete cardiovascular and respiratory depression with overdose. Because the benzodiazepines have a much more acceptable safety profile, they have almost completely replaced barbiturates in clinical use for treating anxiety and insomnia. Barbiturates are still used as anticonvulsants and to induce general anesthesia.
TABLE 11-2
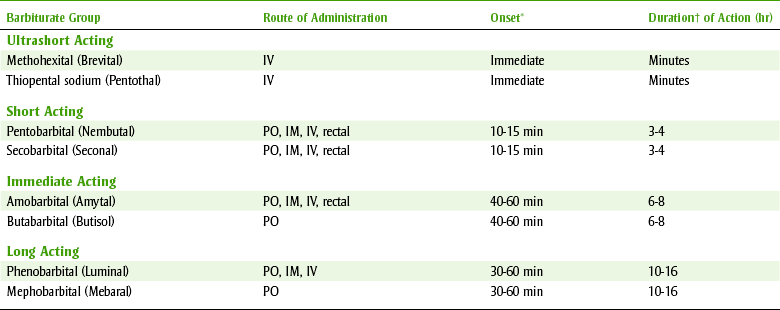
IM, Intramuscular; IV, intravenous; PO, orally.
*Onset = time until the drug’s action begins.
†Duration = length of drug’s action.
Chemistry
The clinically useful barbiturates are formed by substitution of R groups (organic groups) on the barbiturate nucleus sites A and B. Another modification of the barbiturate nucleus involves replacing the oxygen atom with a sulfur atom site C. Compounds with the S-substitution are effective as IV agents such as thiopental.
Pharmacokinetics
Barbiturates are well absorbed orally and rectally. Because the injectable solutions are highly irritating, the IM route is avoided and the drugs are used intravenously. The IV agents are inactivated mainly by redistribution from their site of action in the CNS to the muscles and finally to adipose tissue. The short- and intermediate-acting barbiturates are rapidly and almost completely metabolized by the liver. Long-acting barbiturates are largely excreted through the kidneys as the free drug. Patients with liver damage may have an exaggerated response to short- and intermediate-acting agents, and patients with renal impairment may have an accumulation of the long-acting agents.
Mechanism of Action
Barbiturates produce their effect by enhancing GABA-receptor binding. They prolong the opening of the chloride channels. In higher doses, they may also act directly on the chloride channels without GABA presence. This mechanism is less specific than that of the benzodiazepines, which may account for their ability to induce surgical anesthesia and produce pronounced generalized CNS depressant effects.
Pharmacologic Effects
CENTRAL NERVOUS SYSTEM DEPRESSION
The principal effects of the barbiturates are on the CNS. When normal doses of these agents are administered, relaxation occurs and the electroencephalogram (EEG) speeds up. With larger doses, the inhibitory fibers of the CNS are depressed, resulting in disinhibition and euphoria. If excitation occurs at this point, it is a result of depression of the inhibitory pathways. Anxiety relief cannot be separated from the sedative effects. When higher doses are administered, hypnosis can be produced. The administration of even higher doses can result in anesthesia, with respiratory and cardiovascular depression and finally arrest. This progressive CNS depression parallels that caused by most CNS depressants, including general anesthetics (see Chapter 10).
The CNS depression produced by the barbiturates is additive with other agents that produce this effect. For example, a patient who drinks an alcoholic beverage or is given an opioid analgesic will show additive CNS depression.
ANALGESIA
Barbiturates have no significant analgesic effects. Even doses that produce general anesthesia do not block the reflex response to pain. Patients in pain may become agitated and even delirious if barbiturates are administered without analgesic agents.
ANTICONVULSANT EFFECT
The barbiturates possess anticonvulsant action. The long-acting agents such as phenobarbital are used in the treatment of epilepsy (see Chapter 16).
Adverse Reactions
In the usual therapeutic doses, barbiturates are relatively safe. However, one should be aware that CNS depression may be exaggerated in elderly and debilitated patients or in those with liver or kidney impairment. In some patients, especially the elderly, barbiturates can have an idiosyncratic effect, causing stimulation instead of sedation. Barbiturates can cause fetal harm if administered to a pregnant woman.
ANESTHETIC DOSES
With higher doses, barbiturate concentrations attained in the blood can be lethal. High concentrations are used for intubation or very short procedures. Coughing and laryngospasm have been reported with IV use of barbiturates. High doses may reversibly depress liver and kidney function, reduce gastrointestinal motility, and lower body temperature.
ACUTE POISONING
When barbiturates are prescribed, the possibility that acute poisoning can occur must be considered. Although a lethal dose can only be approximated, severe poisoning will follow the ingestion of 10 times the hypnotic dose, and life is seriously threatened when more than 15 times the hypnotic dose is consumed. The cause of death when an overdose occurs is respiratory failure. The treatment includes conservative management and treatment of specific symptoms.
Chronic Long-Term Use
Chronic use of barbiturates can lead to physical and psychological dependence. Long-term use produces a state similar to alcohol intoxication. The barbiturate addict becomes progressively depressed and is unable to function. Tolerance develops to most effects of barbiturates but not to the lethal dose. Therefore a larger and larger dose must be used to produce an effect, and this dose can approximate the lethal dose. Cross-tolerance occurs among barbiturates and between the barbiturates and nonbarbiturate sedative-hypnotic agents. Chapter 25 discusses the abuse of the barbiturates.
Contraindications
The use of barbiturates is absolutely contraindicated in patients with intermittent porphyria or a positive family history of porphyria. This is because barbiturates can stimulate and increase the synthesis of porphyrins, which are already at an excessive level in this metabolic disease. In fact, the barbiturates have been reported to precipitate an acute attack of porphyria.
Drug Interactions
Because barbiturates are potent stimulators of liver microsomal enzyme production, they are involved in many drug interactions. These enzymes are responsible for the metabolism of many drugs, so an increase in these enzymes could increase the rate of drug destruction and decrease the duration of action. For example, if an epileptic patient who is currently receiving phenytoin (Dilantin) is subsequently given phenobarbital, the phenobarbital stimulates the liver microsomal enzymes that destroy the phenytoin and the phenobarbital more rapidly, which could cause convulsions. This drug interaction requires repeated doses and is not significant with a single dose. Some barbiturate drug interactions are listed in Box 11-3.
Uses
The therapeutic uses of barbiturates are determined by their duration of action (see Table 11-2). The ultrashort-acting agents, such as thiopental (thye-oh-PEN-tal), are used intravenously for the induction of general anesthesia. For very brief procedures, they may be used alone. For more extensive procedures, they are used to induce stage III surgical anesthesia (see Chapter 10).
The short- and intermediate-acting agents have little medical use. Benzodiazepines have replaced them for insomnia and anxiety relief. The short-acting agents were popular agents of abuse because of their fast onset of action.
The long-acting barbiturates, such as phenobarbital (fee-noe-BAR-bi-tal), are used for the treatment of epilepsy.
NONBENZODIAZEPINE-NONBARBITURATE SEDATIVE-HYPNOTICS
Chloral hydrate (KLOR-al HYE-drate) (Noctec) is an inexpensive, orally effective sedative-hypnotic drug with a rapid onset (20 to 30 minutes) and fairly short duration of action (about 4 hours). Therapeutic doses do not produce pronounced respiratory or cardiovascular depression. An exaggerated effect occurs in patients with advanced liver or kidney disease. Large doses or long-term use may produce peripheral vasodilation and hypotension with some degree of myocardial depression. Gastric irritation can be minimized by taking chloral hydrate in diluted solutions with milk or food. The highly irritating effect of chloral hydrate on the mucosa can produce aspiration, especially in struggling children. Its disagreeable odor and taste can be partially masked in a flavored syrup. As with all sedative-hypnotic agents, psychologic or physical dependence may follow prolonged use of this drug.
Chloral hydrate has been used in dentistry for the preoperative sedation of children. The child’s hypnotic dose of chloral hydrate, when used alone, is 50 mg/kg, up to a maximum of 1 gm. Benzodiazepines are a safer choice for sedation of children. Because of its high incidence of gastrointestinal adverse effects and its ability to cause vasodilation and hypotension, this drug is rarely used in children.
Buspirone
Buspirone (byoo-SPYE-rone) (BuSpar) is unique in structure and action. It is the only member of this anxiolytic group. Its onset of action is about 1 week. It is discussed separately because of its unique structure and pharmacology. Its mechanism of action is unknown, but it is believed to be related to interactions with neurotransmitters in the CNS, including serotonin (5-HT1A), dopamine, and cholinergic and α-adrenergic receptors. Buspirone undergoes first-pass metabolism and has a half-life of 2 to 4 hours.
The pharmacologic effect of buspirone is called anxioselective because of its selective anxiolytic action without hypnotic, anticonvulsant, or muscle-relaxant properties. It produces much less CNS depression than other sedative-hypnotic agents and does not affect driving skills. Some patients experience nervousness or insomnia. Buspirone does not produce tolerance or dependence. It does not appear to be addicting and there is no withdrawal syndrome. Because of the mechanism by which buspirone produces its anxiolytic effect, most patients prefer the benzodiazepines.
NONBENZODIAZEPINE-BENZODIAZEPINE RECEPTOR AGONISTS
Zolpidem (Ambien), zaleplon (Sonata), and eszopiclone (Lunesta) are a new class of drugs that are not benzodiazepines but appear to bind to benzodiazepine receptors and decrease sleep latency with little effect on sleep stages. All of these drugs are thought to have agonist effects on GABA. These drugs are used to treat insomnia only. They are controlled substances and have the potential to cause both physical and psychologic dependence.
Zolpidem
Zolpidem (zole-PI-dem) is a hypnotic agent that was recently developed and is indicated for the short-term management of insomnia. Its structure is unlike the benzodiazepines. In contrast to some sedative-hypnotic agents that act at all benzodiazepine (BZ) receptors, zolpidem interacts with the GABAA receptor at the BZ1 receptor. Although zolpidem retains its hypnotic and anxiolytic effects, its receptor specificity gives zolpidem fewer muscle relaxant and anticonvulsant effects. It may be less likely to produce depression of sleep stages 3 and 4. Side effects include headache, drowsiness, dizziness, and diarrhea. Myalgia, arthralgia, sinusitis, and pharyngitis have been reported. Amnesia may also occur. Withdrawal can occur if abruptly stopped after 1 to 2 weeks of use. Rebound insomnia may be experienced. Its quicker onset of action makes it useful to initiate sleep. Because of its fast onset of action, it should be taken immediately before bedtime. Patients should not drive while taking this drug until they see what kind of effect it has on them.
Zolpidem may be used in dentistry if the patient is having difficulty falling asleep the night before a dental appointment. This drug is usually used for persons with chronic insomnia.
Zolpidem is also available as Ambien CR, a controlled-release dose form. There have been reports of behavioral and emotional changes in patients taking Ambien CR. Patients have reported a decrease in inhibition similar to that seen with alcohol and other CNS depressant drugs. Amnesia, anxiety, and a worsening of depression have been reported in patients taking Ambien CR.
Zaleplon
Zaleplon is a rapid-acting hypnotic that is less potent and has a shorter duration of action than zolpidem. It does not appear to decrease premature awakenings or increase total sleep time, but it appears to have a lower risk of next-day residual effects, even with middle of the night use. It does not appear to affect driving the morning after nighttime administration. Zaleplon can cause anterograde amnesia.
Eszopiclone
Eszopiclone is the newest agent of this class available in the United States. It has the longest half-life of the three, but comparative clinical data are lacking. A 6-month trial with eszopiclone found no development of tolerance. Anterograde amnesia has been reported with this drug. Some patients have reported an unpleasant taste while taking this drug. Because of its long half-life, eszopiclone could impair driving the morning after nighttime administration.
MELATONIN RECEPTOR AGONIST
Ramelteon (Rozerem) has been approved by the FDA for the treatment of insomnia characterized by difficulty falling asleep. This drug is an indenofuran derivative that is highly selective for melatonin type 1 (MT1) and melatonin type 2 (MT2) receptors. Studies in animals indicate that the MT1 receptor regulates sleep and the MT2 receptor may mediate the phase-shifting effects of melatonin on a 24-hour biologic clock. In clinical trials, ramelteon produced small, statistically significant improvements on sleep latency but had little effect on sleep maintenance.
The most common adverse effects reported during clinical trials included somnolence, dizziness, fatigue, headache, and insomnia. It is not a controlled substance like the benzodiazepines and the nonbenzodiazepine-benzodiazepine receptor agonists (NBRAs), and there have been no reports of tolerance, rebound insomnia, or withdrawal effects. The long-term safety of ramelteon is unknown.
CENTRALLY ACTING MUSCLE RELAXANTS
Drugs classified as centrally acting muscle relaxants (Table 11-3) exert their effects on the CNS to produce skeletal muscle relaxation.
TABLE 11-3
CENTRALLY ACTING SKELETAL MUSCLE RELAXANTS
| Drug | Comments | Dose (mg) |
| Carisoprodol (Soma) | Tachycardia, flushing | 350 tid-qid |
| Chlorzoxazone (Parafon Forte DSC) | GI distress, hypersensitivity, CNS depression | 250-750 tid-qid |
| Methocarbamol (Robaxin) | CNS depression, GI distress, rash | 1000-1500 qid |
| Orphenadrine (Norflex) | Xerostomia, GIT, vision changes | 100 bid |
| Cyclobenzaprine (Flexeril) | Sedation (40%), xerostomia (30%) | 10 tid |
| Diazepam (Valium) | Benzodiazepine | 5-10 bid-tid |
bid, Twice per day; CNS, central nervous system; GI, gastrointestinal; GIT, gastrointestinal tract; qid, 4 times per day; tid, 3 times per day.
Pharmacologic Effects
Some degree of sedative effect is exhibited by all the CNS muscle relaxants because their action is on the CNS. Xerostomia is common with these agents.
Clinical tests have shown that the sedative effects dominate over the “selective” muscle relaxant activity. When administered intravenously in humans, these agents have been shown to be useful in treating muscle spasm and producing muscle relaxation for certain orthopedic procedures. When these agents are given orally, they do not produce the flaccidity obtainable with IV administration. Thus, until better studies are produced, the beneficial effects of these drugs can be logically ascribed to their sedative action. They are used for back and neck pain and in patients with muscle spasms related to a car accident.
Individual Centrally Acting Muscle Relaxants
Centrally acting skeletal muscle relaxants exert their muscle-relaxing properties indirectly by producing CNS depression. They act in the CNS and have no direct effect on striated muscle, the motor endplate, or nerve fibers. They do not directly relax tense skeletal muscles.
They share many common side effects, including gastrointestinal upset, sedation, and dizziness (results of CNS depression). All of the muscle relaxants have the potential to produce allergic reactions. Most of these agents can produce xerostomia, and the dental health care worker should question the patient about self-treatment for this adverse effect.
Structurally related to the tricyclic antidepressants, cyclobenzaprine (sye-kloe-BEN-za-preen) (Flexeril) is considered to be the strongest muscle relaxant. Because sedation occurs in about 40% of the patients taking cyclobenzaprine, it is the most sedating muscle relaxant. It also is most likely to produce xerostomia with an incidence of 30%. (This demonstrates typical effects and adverse reactions of drugs: the more pharmacologic effect [wanted], the more adverse reactions [unwanted].)
A relative of meprobamate is carisoprodol (kar-eye-soe-PROE-dole) (Soma). Chlorzoxazone (klor-ZOX-a-zone) (Paraflex) may discolor the urine purple-red. The patient should be warned about this harmless property. Other muscle relaxants include methocarbamol (meth-oh-KAR-ba-mole) (Robaxin) and orphenadrine (or-FEN-a-dreen) (Norflex). Diazepam (Valium), a benzodiazepine, also possesses muscle-relaxant properties and is used for spastic muscles such as occurs in multiple sclerosis. Table 11-3 lists the muscle relaxants that function via the brain and their selected side effects and usual doses.
USE
The muscle relaxants are all indicated as an adjunct to rest and physical therapy for relief of muscle spasm associated with acute painful musculoskeletal conditions. Questions about their efficacy still linger in the literature. They are also used in the treatment of temporomandibular disorder (TMD) because relaxation of the muscles is helpful to the symptoms. The success of muscle relaxants in the management of TMD has not been documented.
MISCELLANEOUS AGENTS
Baclofen (BAK-loe-fen) (Lioresal) inhibits both monosynaptic and polysynaptic reflexes at the spinal level. It also inhibits GABA, but whether this is related to its action is unknown. It is indicated for spasticity from multiple sclerosis or spinal cord injuries or diseases. Baclofen has been used to treat trigeminal neuralgia, although it is not FDA approved for this purpose. Drowsiness, weakness, headache, and insomnia have been reported. Nausea, dry mouth, taste disorder, and urinary frequency have been seen. Lowering of the seizure threshold and an increase in ovarian cysts in rats have also occurred.
Tizanidine
Tizanidine (tye-ZAN-i-deen) (Zanaflex) is a short-acting muscle relaxant. It is a centrally acting α-adrenergic receptor agonist (like clonidine) that increases presynaptic inhibition of motor neurons. Like clonidine, it can produce sedation, drowsiness, hypotension, and xerostomia.
Dantrolene
Dantrolene (DAN-troe-leen) (Dantrium) affects the contractile response of the skeletal muscle by acting directly on the muscle itself. It dissociates the excitation-contraction coupling, probably by interfering with the release of calcium from the sarcoplasmic reticulum. It is indicated in the treatment of spasticity from upper motor neuron disorders such as spinal cord injury, cerebral palsy, or multiple sclerosis. It is also used orally to prevent and intravenously to treat malignant hyperthermia brought on by succinylcholine or inhalation of general anesthetics. The hepatotoxicity it produces is more common with higher doses and in older female patients taking concomitant medications. This agent may cause drowsiness or photosensitivity.
GENERAL COMMENTS ABOUT ANTIANXIETY AGENTS
Analgesic-Sedative Combinations
The use of an analgesic and a sedative-hypnotic agent to provide concomitant sedation and analgesia is rational for several reasons (Box 11-4).
Both sedation and analgesia can be obtained from the opioid analgesics alone. However, it is not desirable to prescribe an opioid to add sedation to analgesia unless the analgesic potency is required. In cases in which anxiety is an important component in pain relief, either a nonopioid or opioid can be used concomitantly with a sedative. This combination may be prescribed separately, although a few fixed-dose products are available. A combination of a sedative with an analgesic is available in butalbital compound (Fiorinal) or butalbital/acetaminophen (Fioricet). If the patient’s pain is more severe, then an opioid and a sedative-hypnotic agent can be prescribed. The previously mentioned agents are available mixed with codeine (#3 contains 30 mg codeine) to make Fiorinal #3. In a dental patient in whom anxiety is magnifying the pain reaction, the prescribing of a combination agent might be useful.
Special Considerations
Certain generalizations should be kept in mind when discussing the use of the antianxiety agents. The dental practitioner plays an important role in helping the patient understand the possible effects of the drugs used to allay anxiety. The patient may raise questions about these agents, and their effects should be explained. Dental patients who are to use antianxiety agents should be driven to and from the dental appointment.
Drugs are not to be used as a substitute for patient management. The practitioner should not rely exclusively on drugs to provide a calm and cooperative patient. The dental team should exhibit a confident and relaxed manner. A pleasant, soothing office atmosphere is of great importance in relaxing an anxious patient. Appropriate use of music of the patient’s choice can reduce anxiety. Drugs should not be substituted for patient education or for the proper psychological approach to patient care.
When an agent for anxiety relief is required, the selection of the specific drug should be based on knowledge of the advantages and disadvantages of the agents available and an understanding of the needs and contraindications related to the case at hand.
Precautions
Regardless of the antianxiety agent selected, the following precautions pertain:
• Patients with impaired elimination may experience exaggerated effects of these medications. These persons include the young, the elderly, the debilitated, and those with liver or kidney disease.
• Depression caused by all sedative-hypnotics will add to depression caused by other CNS depressants that the patient may be taking. The patient should be made aware of this, particularly in regard to alcohol; over-the-counter (OTC) sleep aids may also be a potential source of hazard.
• The patient should understand that the drug prescribed will make it unsafe to perform acts requiring full alertness and muscle coordination such as driving a car. The patient should be accompanied by a responsible adult who can drive the patient home. The patient should be warned against signing any important papers or documents. These cautions are particularly important if the patient has not taken the drug previously and consequently his or her response is less predictable.
• Psychic and physical dependence has been observed with almost all drugs used to allay anxiety. The dentist should realize that these drugs have abuse potential and should limit their use accordingly. This is particularly important in regard to the treatment of chronic conditions or persons with a history of addiction or alcoholism.
• Suicide may be attempted by taking sedative-hypnotic drugs. Consequently, the amount of drug prescribed should be limited to the minimum required to accomplish the therapeutic objective. With benzodiazepines, the therapeutic index is wide unless mixed with alcohol.
• These drugs should never be administered to pregnant women or those who may be pregnant unless the potential benefit to the mother outweighs the risk to the fetus.
• Sedatives do not provide analgesia. In fact, the use of a sedative without adequate pain control may cause the patient to become highly excited and act irrationally. However, sedatives may potentiate the effect of an analgesic taken concomitantly.
CLINICAL SKILLS ASSESSMENT
1. What are some of the nonpharmacologic methods of helping a patient deal with her anxiety?
2. The dentist decides to prescribe diazepam, which is to be taken the night before her appointment and approximately 1 hour before her appointment. What is the rationale for using benzodiazepines to treat anxiety?
3. What are the adverse reactions associated with benzodiazepines?
4. Is memory loss a problem with benzodiazepines? What should a patient be told?
5. Should a patient be concerned about becoming addicted to benzodiazepines? Why or why not?
6. What should a patient be told about the medication that the dentist has chosen?
7. Name two major pharmacologic effects of barbiturates.
8. Describe the major adverse reactions of barbiturates.
9. Name the one absolute contraindication to the use of barbiturates.
10. Describe the mechanism of the most important drug interaction of barbiturates.
11. State the potential advantages of the NBRAs.
12. Explain why chloral hydrate is still used by some dentists as premedication for children.
13. What is the rationale for combining a sedative-hypnotic drug with an analgesic?
 Please visit http://evolve.elsevier.com/Haveles/pharmacology for review questions and additional practice and reference materials.
Please visit http://evolve.elsevier.com/Haveles/pharmacology for review questions and additional practice and reference materials.