Adrenocorticosteroids
1 Define adrenocorticosteroids and describe how the body releases them.
2 Summarize the classification, administration, mechanism of action, and pharmacologic effects of adrenocorticosteroids.
3 Describes the various adverse reactions and uses of adrenocorticosteroids, including their application to dentistry.
The term adrenocorticosteroids (a-dree-noe-KOR-ti-KO-ster-oids) (adrenal corticosteroids, adrenocorticoids, corticosteroids, or steroids) refers to a group of agents secreted by the adrenal cortex. The dental team should be aware of the effects, adverse reactions, and dental implications of these agents for at least the following reasons:
• Use in dentistry: These compounds are used topically or systemically for the treatment of oral lesions associated with inflammatory diseases.
• Long-term therapy: The adrenocorticosteroids, or steroids as they are commonly called, are prescribed for many patients with chronic systemic diseases such as asthma or arthritis. If taken chronically in high enough doses, these agents can cause a variety of adverse reactions that may influence the patient’s dental treatment.
MECHANISM OF RELEASE
The adrenocorticosteroids are naturally occurring compounds secreted by the adrenal cortex. Their release is triggered by a series of events (Figure 19-1). First, a stimulus such as stress (1) causes the hypothalamus (2) to release corticotropin-releasing hormone (CRH) (3), which acts on the pituitary gland (4). Under the influence of CRH, the pituitary gland secretes adrenocorticotropic hormone (ACTH) (5), which stimulates the adrenal cortex (6) to release hydrocortisone (7). Hydrocortisone then acts on both the pituitary (8) and the hypothalamus (9) to inhibit the release of CRH and ACTH, respectively. This mechanism is called negative feedback. Exogenous steroids act in the same way as hydrocortisone (10); that is, they inhibit the release of CRH and ACTH. With long-term administration of steroids, ACTH release is suppressed and the adrenal gland atrophies. If the administration of the exogenous steroid is then abruptly stopped, a relative steroid deficiency results. This can cause severe problems, including adrenal crisis.

CLASSIFICATION
The adrenocorticosteroids can be divided into two major groups: the glucocorticoids, which affect intermediate carbohydrate metabolism, and the mineralocorticoids, which affect the water and electrolyte composition of the body. The major glucocorticoid present in the body is cortisol (hydrocortisone). Without stress, the normal adult secretes about 20 mg of hydrocortisone daily. A tenfold increase can occur with stress. Maximal secretion occurs between 4 am and 8 am in people with a normal schedule. The chemical structures of the synthetic agents and the naturally occurring adrenocorticosteroids, such as hydrocortisone, are similar. Many chemical modifications have been made in an attempt to produce synthetic glucocorticoids with fewer adverse reactions and more specific activity.
Although the term adrenocorticosteroids refers to those steroids secreted by the adrenal cortex and includes both the glucocorticoids and the mineralocorticoids, this chapter discusses primarily the action of glucocorticoids because of their more frequent use.
DEFINITIONS
The following terms are used in this chapter:
• Addison’s disease: Disease/condition produced by a deficiency of adrenocorticosteroids
• Adrenocorticosteroids/corticosteroids/steroids: Steroidal components released from the adrenal cortex, including glucocorticoids and mineralocorticoids
• Adrenocorticotropic hormone (ACTH): Agent secreted by the pituitary that causes the release of hormones from the adrenal cortex
• Cushing’s syndrome: Disease/condition produced by an excess of adrenocorticosteroids
• Glucocorticoids: Adrenocorticosteroids that primarily affect carbohydrate metabolism
• Mineralocorticoids: Adrenocorticosteroids that affect the body’s sodium and water balance (fluid levels)
ROUTES OF ADMINISTRATION
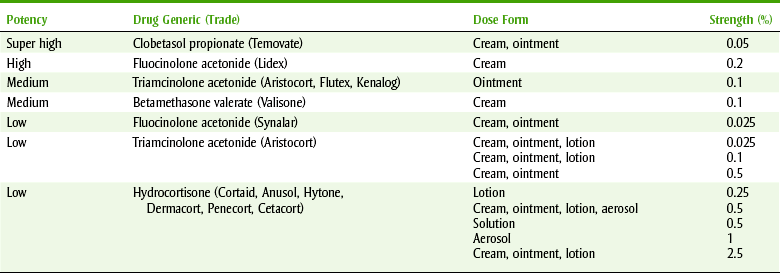
Glucocorticoids are available in a wide variety of dose forms. They are routinely used topically, orally, intramuscularly, and intravenously. Systemic effects are commonly obtained when the drug is administered orally or parenterally, but topical administration may rarely cause systemic effects. If a large quantity of a steroid is applied topically, especially if the skin is denuded or an occlusive dressing such as plastic wrap is applied, systemic effects can occur. Table 19-1 shows the relative potency of selected topical corticosteroid products.
MECHANISM OF ACTION
The mechanism of action of the steroids involves binding to a specific receptor and forming a steroid-receptor complex. The complex then translocates into the nucleus and alters gene expression (turns genes on or off), resulting in the regulation of many cellular processes. Because of the mechanism, a lag time exists in the action of the steroids and the relationship between their effects and blood level is poor. Other effects of glucocorticoids are mediated by catecholamines producing vasodilation or bronchodilation.
The antiinflammatory action of glucocorticoids results from their profound effects on the number, distribution, and function of peripheral leukocytes and to their inhibition of phospholipase A. The use of steroids results in an increase in the concentration of neutrophils and a decrease in the lymphocytes (T and B cells), monocytes, eosinophils, and basophils. Steroids induce the synthesis of a protein that inhibits phospholipase A, decreasing the production of both prostaglandins and leukotrienes from arachidonic acid.
These agents, responsible for the delayed phase of acute inflammation, act synergistically. Steroids also inhibit interleukin-2, migration inhibition factor, and macrophage inhibition factor.
PHARMACOLOGIC EFFECTS
The pharmacologic effects and the adverse reactions of corticosteroids are closely related (Figure 19-2). The effects for which they are used include their antiinflammatory action and suppression of allergic reactions. They also suppress the immune response. Corticosteroids are palliative rather than curative. The glucocorticoid effects and the mineralocorticoid effects are listed in Box 19-1. Many of these effects produce adverse reactions and are discussed in the following section.
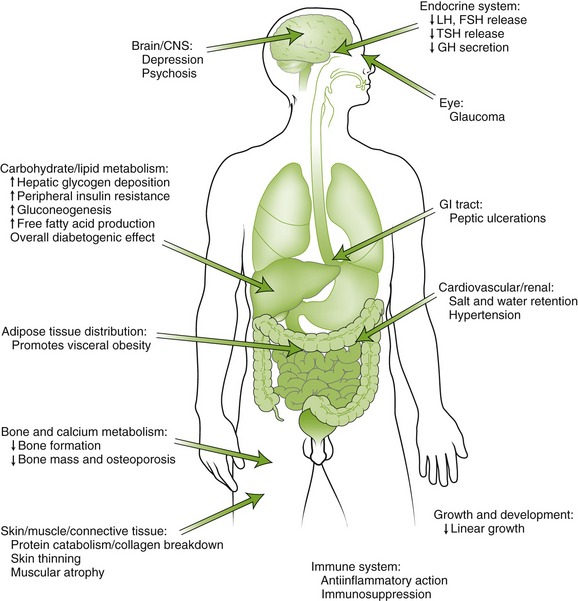
FIGURE 19-2 The principal sites of action of glucocorticoids in humans highlighting some of the consequences of glucocorticoid excess. CNS, Central nervous system; GI, gastrointestinal; FSH, follicle-stimulating hormone; GH, growth hormone; LH, luteinizing hormone; TSH, thyroid-stimulating hormone. (From Kronenberg HM, Melmed S, Polonsky KS, et al: Williams’ textbook of endocrinology, ed 11, Philadelphia, 2008, Saunders.)
ADVERSE REACTIONS
The adverse reactions of corticosteroids are proportional to the dose, frequency and time of administration, and duration of treatment. With prolonged therapy and sufficiently high doses, the following side effects occur.
Metabolic Changes
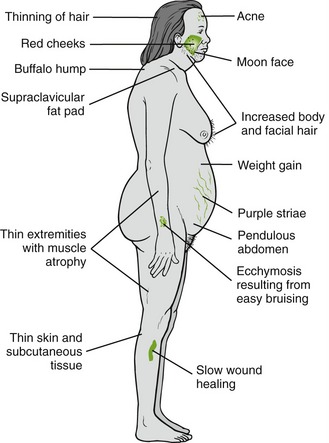
Moon face (round), buffalo hump (fat deposited on back of the neck), truncal obesity, weight gain, and muscle wasting give patients the Cushing’s syndrome appearance (Figure 19-3). Hyperglycemia (diabetes-like) may be aggravated or initiated, especially in prediabetic patients. More antidiabetic medication may be required.
Infections
Corticosteroids decrease resistance to infection. Because of their antiinflammatory action, they may also mask its symptoms. Patients taking long-term glucocorticoid therapy are given isoniazid, an antituberculosis agent, to prevent tuberculosis.
Central Nervous System Effects
Changes in behavior and personality, including euphoria (with increasing dose), agitation, psychoses, and depression (with decreasing dose), can occur.
Peptic Ulcer
Because corticosteroids stimulate an increase in production of stomach acid and pepsin, they may exacerbate peptic ulcers. Healing is impaired, and the ulcer may perforate.
Impaired Wound Healing and Osteoporosis
The catabolic effects of steroids that result from impaired synthesis of collagen can impair wound healing. This same process can cause osteoporosis or impair growth in children. If the osteoporosis affects alveolar bone, it could result in tooth loss. Thinning bones can also result in fractures in patients on chronic steroids without trauma. Muscle wasting, bruising, and abdominal striae are other symptoms associated with catabolism.
Ophthalmic Effects
Because corticosteroids can increase intraocular pressure, glaucoma may be exacerbated. Cataracts are also associated with steroids.
Electrolyte and Fluid Balance
Glucocorticoids that possess some mineralocorticoid action can produce sodium and water retention. Hypertension or congestive heart failure may be exacerbated. Hypokalemia may also result.
Adrenal Crisis
With prolonged use, adrenal suppression can occur. If a stressful situation arises, the adrenal gland cannot respond adequately. Symptoms of adrenal crisis include weakness, syncope, cardiovascular collapse, and death.
Dental Effects
Oral tissue changes may occur in patients taking corticosteroids. Their mucosal surfaces heal more slowly, are more likely to have infection, and are more friable. With the use of oral steroid inhalers for asthma, oral candidiasis may result. This may be prevented by rinsing the mouth after inhaler use.
USES
There are many conditions for which corticosteroids may be administered (Box 19-2). Patients with these conditions should be questioned about past use of systemic steroids.
 REPLACEMENT
REPLACEMENT
Patients with hypofunction of the adrenal cortex (Addison’s disease) need replacement of glucocorticoid and mineralocorticoid activity. Usually, hydrocortisone is used to restore glucocorticoid activity and desoxycorticosterone is used to restore mineralocorticoid activity. Patients with a hyperfunctioning adrenal cortex (Cushing’s syndrome) may have a majority of the gland removed surgically. In this case, replacement therapy is needed.
EMERGENCIES
Corticosteroids are used in emergency situations for the treatment of shock or adrenal crisis, as discussed in Chapter 23.
INFLAMMATION/ALLERGY
The most extensive use of the corticosteroids in both medicine and dentistry is in the treatment of a wide variety of inflammatory and allergic conditions. These agents are not curative but merely ameliorate symptoms because of their antiinflammatory activity. Some conditions that have been treated with corticosteroids are rheumatoid arthritis, rheumatic fever, systemic lupus erythematosus, scleroderma, inflammation of the joints and soft tissues, acute bronchial asthma, severe and acute allergic reactions, and severe allergic dermatoses. Prednisone (PRED-ni-sone) is the most common corticosteroid used orally.
Topical corticosteroids are used for a variety of skin conditions, which involve various dermatoses or “irritations.” The steroids can be divided into several classes depending on their relative maximum potency*: the least efficacious to the most efficacious and in between. An example of the weakest is hydrocortisone (hye-droe-KOR-ti-sone), an example of an “in between” is triamcinolone (trye-am-SIN-oh-lone) acetonide, and an example of the most potent is augmented betamethasone (bay-ta-METH-a-sone) dipropionate.
Dental Uses
Because of the adrenocorticosteroids’ antiinflammatory action, they are administered topically, intraarticularly, or orally in several dental situations. The use of steroids in dentistry has had mixed success and double-blind controlled studies are needed to determine unequivocally their proper place in the therapeutic armamentarium.
ORAL LESIONS
Systemically administered steroids are often effective in the treatment of oral lesions associated with noninfectious inflammatory diseases, including erythema multiforme, lichen planus, pemphigus, desquamative gingivitis, and benign mucous membrane pemphigoid. It is imperative that an infectious etiology, such as herpes, be ruled out.
APHTHOUS STOMATITIS
The evidence for the benefit of adrenocorticosteroids in the treatment of aphthous stomatitis seems clear. Triamcinolone acetonide (Kenalog in Orabase) has been advocated. Orabase is a mineral oil gel base that sticks to the oral mucosa, forming a plasticlike surface. Other topical steroids, such as fluocinonide and fluocinolone (floo-oh-SIN-oh-lone), can be used topically.
TEMPOROMANDIBULAR JOINT
The temporomandibular joint (TMJ) affected with arthritis (inflammation) also responds to the systemic administration of steroids. If only this joint is affected, an intraarticular injection can often decrease the pain and improve the joint movement.
USES IN ORAL SURGERY
The adrenocorticosteroids have been used in oral surgery to reduce postoperative edema, trismus, and pain. Although the decrease in edema with steroid use can be easily documented, the magnitude of the benefit must be weighed against the potential risk of infection and decreased healing. The safety and effectiveness of these agents have not been proved in controlled double-blind studies.
CORTICOSTEROID PRODUCTS
Selected synthetic corticosteroids are arranged in Table 19-2 according to their duration of action: short, intermediate, and long. The relative antiinflammatory and salt-retaining activity and equivalent oral dose are given, with hydrocortisone arbitrarily assigned the value of 1 for each activity. The other agents are then given values in relation to those of hydrocortisone. For example, prednisone, with an antiinflammatory activity of 4, has 4 times as much antiinflammatory action as hydrocortisone. Therefore only one-fourth as much prednisone is required to produce the same effect produced by hydrocortisone. The mineralocorticoid, or salt-retaining, properties of the glucocorticoids are also compared with those of hydrocortisone. For example, triamcinolone does not increase salt retention, whereas hydrocortisone does.
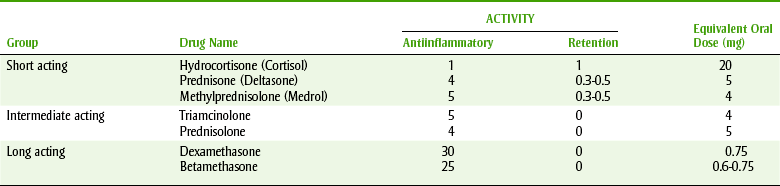
Table 19-2 lists the equivalent oral dose in milligrams based on 20 mg of hydrocortisone, the amount normally secreted daily by an adult without stress. One can see that 0.75 mg of dexamethasone or 5 mg of prednisone is approximately equivalent to 20 mg of hydrocortisone.
DENTAL IMPLICATIONS
Box 19-3 summarizes the management of dental patients taking steroids. Because steroids suppress immune reaction, with chronic administration of steroids, infections are more likely to occur and healing is delayed. These factors are important in dental patients, especially if a surgical procedure is to be performed. Because the symptoms of infection may be masked, the wound site should be carefully examined.
Adverse Reactions
Adrenocorticosteroids stimulate acid secretion; patients taking these agents should be given other ulcerogenic medications, such as the salicylates or the nonsteroidal antiinflammatory agents, with caution.
BLOOD PRESSURE CHANGES
The blood pressure of patients taking corticosteroids should be measured because these agents can exacerbate hypertension. The more mineralocorticoid action, the more likely the agent is to raise blood pressure.
GLAUCOMA
Other agents that can induce or exacerbate glaucoma, such as the anticholinergics, should be used with caution in patients taking adrenocorticosteroids.
BEHAVIORAL CHANGES
A patient’s bizarre behavior may be explained by the presence of, or withdrawal from, adrenocorticosteroids. Psychosis, euphoria, or depression might be seen.
OSTEOPOROSIS
Dental radiographs may demonstrate osteoporosis in patients taking long-term adrenocorticosteroids. More than 50% bone loss is required to observe osteoporosis (radiographically). These patients are more likely to suffer fractures either with or without trauma.
INFECTION
Because of the antiinflammatory activity of the adrenocorticosteroids, they may mask the symptoms of an infection. They decrease a patient’s ability to fight infection by suppression of migration of polymorphonuclear leukocytes, thus reducing lymph system action.
DELAYED WOUND HEALING
Because the adrenocorticosteroids cause delayed wound healing, special precautions should be taken when surgical procedures are performed in the oral cavity. Friability of the tissue also requires special care when closing wounds and extra sutures may be required.
ADRENAL CRISIS
The body releases corticosteroids and epinephrine from the adrenal gland when a person experiences stress. Under normal conditions, when the body sends a message (ACTH) to the adrenal gland, it is stimulated and secretes hydrocortisone. Because the adrenal gland of a normal person is regularly stimulated when the person experiences stress, the adrenal gland stays ready for a message to put out hydrocortisone. The body does not differentiate between the hydrocortisone (endogenous) it secretes and the hydrocortisone or prednisone (exogenous) given to a patient by any route. When a patient is taking chronic prednisone, the steroid provides negative feedback to the hypothalamus (reduces release of CRH) and the pituitary (reduces release of ACTH).
With prolonged administration of steroids, suppression of the hypothalamic-pituitary-adrenal axis occurs. With suppression, the body does not quickly respond to stress with release of hydrocortisone. Suppression is proportional to the potency of the agent, the dose of the agent, and the duration of administration. The longer the duration, the higher the dose, and the greater the potency of the steroid, the quicker the suppression occurs. Once suppression occurs, it can take weeks or months for the adrenal gland to respond normally. Without the proper response to stress, adrenal crisis is possible. The crisis occurs because of a relative lack of corticosteroids during stress, such as a dental appointment for a patient with dental phobia. It may be necessary to administer adrenal steroids before a stressful dental procedure to prevent crisis. A consultation with the patient’s physician is helpful. Generally, low and very high (mega) doses do not present problems; problems may occur with mid-range doses.
Steroid Supplementation
There are many ways of using supplemental steroids in patients who use chronic steroids and are to undergo a stressful dental procedure. One approach to determine if additional steroids are needed is diagrammed in Figure 19-4. With both low (<20 mg hydrocortisone or 5 mg prednisone) and very high doses (immunosuppressive; >40 to 60 mg hydrocortisone/day or 10 to 15 mg prednisone/day), no additional steroid supplementation is needed. With some intermediate doses of steroids (estimated to be between 20 and 40 mg/day hydrocortisone or 5 and 10 mg prednisone/day), additional steroids may be indicated if the procedure will produce severe stress.
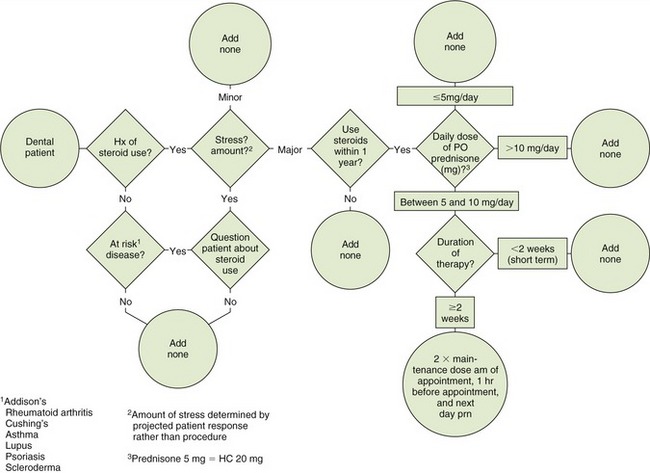
After consultation with the patient’s physician, one suggested regimen is to administer two to three times the patient’s usual daily dose of steroids the day of the procedure and 1 hour before the surgery or procedure. If pain is expected to persist into the next day, then two times the usual daily dose of steroids should also be given the following day. Some authors state that steroid supplementation is only needed if severe stress is expected (evaluate dental anxiety and dental procedure severity). The patient should be evaluated for likelihood to experience stress based on the patient’s degree of anxiety—not the specific procedure planned. Administering additional steroids for 1 or 2 days poses no additional risk above that produced by chronic use of steroids.
Topical Use
Steroids are used in dentistry to manage certain oral conditions, such as aphthous stomatitis, related to inflammatory or immune mechanisms. Both topical and systemic steroids are used in these instances. The relative potencies of selected topical glucocorticoids are listed in Table 19-1.
CLINICAL SKILLS ASSESSMENT
1. Compare and contrast the activity of the glucocorticoids and mineralocorticoids.
2. List the routes of administration for the steroids used in dentistry.
3. What are the dental concerns associated with steroids?
4. Are there any drug interactions to be aware of?
5. Describe the three major uses of the steroids in medicine.
6. Explain how to evaluate a patient undergoing therapy and how to determine whether the patient’s physician should be consulted. State what problems could arise from dental treatment and how these adverse effects could be monitored.
7. Define the terms Cushing’s syndrome and Addison’s disease.
8. Both hypofunctioning and hyperfunctioning of the adrenal cortex require replacement therapy. What are the dental concerns regarding replacement therapy?
 Please visit http://evolve.elsevier.com/Haveles/pharmacology for review questions and additional practice and reference materials.
Please visit http://evolve.elsevier.com/Haveles/pharmacology for review questions and additional practice and reference materials.
*Using the strict definition of potency and efficacy, the term potency as used to refer to topical steroids is really efficacy.