Emergency Drugs
1 Summarize the general measures a dental professional should follow to train for an emergency and the preparation for treatment in the event of an emergency.
2 Name and describe several categories of emergencies and provide common examples within each category.
3 List the critical drugs to include in a dental office emergency kit and several examples of second- or third-level drugs that would be optional.
4 Name several pieces of equipment that would be included in the emergency kit.
An increasing number of older patients who are taking multiple drugs seek dental treatment each year. The demographics of our population, the use of fluorides, and management of periodontal disease has increased the age of the average dental patient. Dental offices are administering more complicated drug regimens; dental appointments are taking longer; and dental patients are on average getting sicker. With these changes, the chance of an emergency occurring in the dental office continues to increase. Both the dentist and the dental hygienist should become familiar with the most common emergency situations, their management, and the drugs used to treat these conditions. When an emergency occurs, working together can increase the chance of producing the best outcome. Many emergency situations can be handled correctly with adequate knowledge. Lack of this knowledge during an emergency may cause panic in a dental office. If the dental office and its personnel are prepared for an emergency, handling one will be easier. Before treating patients who might be at risk for an emergency, the treatment of a potential emergency related to their disease should be reviewed. It is the responsibility of each dental health care worker to make sure the members of the team can act in a coordinated manner.
GENERAL MEASURES
To prepare the dental office for an emergency, the following steps should be taken:
• Training: All office personnel should be trained and retrained in emergency procedures before an emergency occurs. They should practice for an emergency at least once every 6 months.
Basic cardiac life support (cardiopulmonary resuscitation [CPR]) training (required)
Advanced cardiac life support (ACLS) training (optional, unless performing conscious sedation)
• Phone number: One should post the telephone number of the closest physician, emergency room, and ambulance service (often 911). The number(s) should be programmed into the speed dial function of the phone.
• Emergency kit: One should select the items for the office’s emergency kit, including the drugs and the devices (nondrug items) needed. The kit should be checked every 3 months to make sure that the drugs are not out of date. Some companies have this service by subscription.
To minimize the chances of an office emergency, the procedures listed in Box 23-1 should be performed on each new dental patient. It is easier to prevent rather than treat a dental emergency. If an emergency occurs in the dental office, the steps listed in Box 23-2 should be taken.
Preparation for Treatment
Before any emergency treatment can be administered, investigation of the patient’s signs and symptoms must lead to a diagnosis of the problem. In most cases, the maintenance of the airway (A), respiration (breathing, B), and circulation (C) are of primary importance. The use of drug therapy in these situations is only ancillary to the primary measures of maintaining adequate circulation and respiration. One should remember that drugs are not necessary for the proper management of most emergencies. Whenever there is doubt as to whether to give the drug, it should not be given.
In the dental office, each health care worker should be certified. The legal implications of lack of CPR training could be serious. ACLS training can be helpful in certain rural situations or if the technique of preoperative sedation or conscious sedation is used in the dental office.
The categories of emergencies are discussed in the next section. The most commonly used drugs and the choice of drugs and equipment for a dental office emergency kit are addressed.
CATEGORIES OF EMERGENCIES
This section discusses the signs, symptoms, and treatment of the most common emergency situations, dividing them into changing consciousness; respiratory, cardiovascular, and other emergencies; and drug-related emergencies.
Lost or Altered Consciousness
Many common dental emergencies involve either unconsciousness or altered consciousness. Dental office personnel should be ready to handle these emergencies and determine the best course of treatment.
 SYNCOPE
SYNCOPE
The emergency most often encountered in the dental office is simple syncope (fainting, also known as vasomotor collapse) or transient unconsciousness. The skin takes on an ashen-gray color, and diaphoresis occurs. The release of excessive epinephrine results in a pooling of the blood in the peripheral muscles (β effect, vasodilation), a decrease in total peripheral resistance, and a sudden fall in blood pressure. A reflex tachycardia follows, but soon, decompensation results in severe bradycardia. These effects are brought about by anxiety, fear, or apprehension, all of which are common in a dental situation. Treatment involves placing the patient in the Trendelenburg position (head down) (Figure 23-1), causing blood to rush to the head, which has the effect of giving the patient a transfusion of whole blood.

FIGURE 23-1 In the Trendelenburg position, the individual should be tilted back even further in the dental chair so that the head is below the level of the heart and turned to one side. (From Malamed SF: Medical emergencies in the dental office, ed 6, St Louis, 2007, Mosby.)
The most important component in the treatment of syncope is for the dental health care worker to exhibit confidence in action and voice. If the hygienist shows control over the situation, the patient will be less anxious and apprehensive and less likely to repeat the syncopal attack.
Spirits of ammonia can be administered by inhalation. The old practice of putting the head between the legs should be avoided because venous return is cut off by the slumped position.
HYPOGLYCEMIA
The most common cause of hypoglycemia is an excessive dose of insulin in a patient with diabetes. The medical history in this case is important, so the dental health care worker can determine the dose and type of insulin and food intake before the appointment. Often, patients inject their usual daily dose of insulin but fail to eat before coming to the dental office. If this is the case, then patients should be asked to eat before any dental procedures are begun. The time of the hypoglycemia can be estimated by knowledge of the peak effect of the particular insulins used (see Chapter 20).
The patient with hypoglycemia has a rapid pulse and decreased respiration and is very talkative. Hunger, dizziness, weakness, and occasionally tremor of the hands can occur. Diaphoresis, nausea, and mental confusion are other signs of hypoglycemia. If the signs of hypoglycemia are recognized before they become severe, the patient can be given a sugary drink or oral glucose. If the patient lapses into unconsciousness and has no swallowing reflex, dextrose must be given intravenously.
DIABETIC COMA
Less common than hypoglycemia, the diabetic coma is caused by elevated blood sugar. Symptoms of frequent urination, loss of appetite, nausea, vomiting, and thirst are seen. Acetone breath; hypercapnia; warm, dry skin; rapid pulse; and a decrease in blood pressure can occur. Treatment is undertaken only in a hospital setting and includes insulin after proper laboratory results are obtained (blood sugar).
CONVULSIONS OR SEIZURES
Convulsions are most commonly associated with epilepsy, especially the grand mal type (see Chapter 16), but can also result from a toxic reaction to a local anesthetic agent. Convulsions are abnormal movements of parts of the body in clonic and/or tonic contractions and relaxations. The patient may become unconscious. Generally, convulsions are self-limiting, and treatment should include protecting the patient from self-harm, moving any sharp objects out of the patient’s reach, and turning the patient’s head to the side to prevent aspiration. In some situations, diazepam may be administered intravenously, but observation of the patient is often sufficient.
Respiratory Emergencies
Respiratory emergencies involve difficulty in breathing and exchange of oxygen. They include hyperventilation, asthma, anaphylactic shock, apnea, and acute airway obstruction.
HYPERVENTILATION
Hyperventilation is one of the most common dental emergency situations. The increased respiratory rate is often brought on by emotional upset associated with dental treatment. Tachypnea, tachycardia, and paresthesia (tingling of the fingers and around the mouth) have been reported. Nausea, faintness, perspiration, acute anxiety, lightheadedness, and shortness of breath can also occur. The treatment is calm reassurance. The dental professional should encourage patients to hold their breath or “rebreathe” into a paper bag or an unconnected face mask (occasionally portrayed in movies).
ASTHMA
Normally, patients who have acute asthmatic attacks have a history of previous attacks and carry their own medication. The most common sign of an asthmatic attack is wheezing with prolonged expiration (squeak). The patient’s own medication (multidose inhalers containing β2-agonist such as albuterol) should be used first. The dose should be repeated several times. If there is no response to these, hospitalization for administration of aminophylline (parenteral or oral) and parenteral corticosteroids and epinephrine should be considered. Oxygen should also be administered.
ANAPHYLACTIC SHOCK
The most common cause of anaphylactic shock is an injection of penicillin, although anaphylactic reactions have also been caused by many other agents. Examples include eating peanuts or being exposed to latex rubber items. The reaction usually begins within 5 to 30 minutes after ingestion or administration of the antigen. Usually, a weak, rapid pulse and a profound decrease in blood pressure occur. There is dyspnea and severe bronchial constriction.
Parenteral epinephrine is the drug of choice and must be administered immediately in cases of severe anaphylactic shock. It may be given in the deltoid muscle or injected under the tongue. If bronchoconstriction is predominant, albuterol administered by inhalation or nebulization may suffice. After the life-threatening symptoms have been controlled, intravenous corticosteroids, intramuscular diphenhydramine, and aminophylline may also be used.
ACUTE AIRWAY OBSTRUCTION
Acute airway obstruction or aspiration (e.g., aspiration of vomitus) is usually a result of a foreign body (e.g., a crown) in the pharynx or larynx; laryngospasm may be drug induced. Gasping for breath, coughing, gagging, acute anxiety, and cyanosis are signs and symptoms of acute airway obstruction. Treatment begins by placing the patient in a Trendelenburg position on the right side and encouraging coughing. One should not allow the patient to sit up. Clearing the pharynx and pulling the tongue forward before performing the Heimlich maneuver (external subdiaphragmatic compression) should be attempted next. Finally, the Heimlich maneuver should be performed and repeated if needed (Figure 23-2). A cricothyrotomy or tracheotomy, hardly dental office maneuvers, is indicated if the object cannot be dislodged by the other methods.
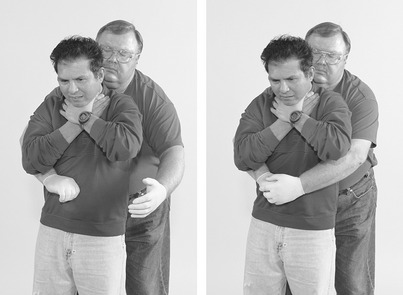
FIGURE 23-2 The proper technique for an abdominal thrust (Heimlich maneuver). (From Chapleau W: Emergency first responder: making the difference, St Louis, 2004, Mosby.)
For aspiration, the use of suction, intubation, and ventilatory assistance is suggested. Steroids, antibiotics, and aminophylline are also administered. When drug-induced laryngospasm is present, succinylcholine, a neuromuscular blocking agent, and positive-pressure oxygen are the agents of choice. The operator must have training and equipment to artificially breathe for the patient before succinylcholine is administered. Prevention of swallowed objects can best be attained by the use of a rubber dam and throat packing, when appropriate.
Cardiovascular System Emergencies
Emergency situations involving the cardiovascular system include angina pectoris, myocardial infarction (MI), cardiac arrest, acute congestive heart failure, arrhythmias, and hypertensive crisis. The primary concern in any cardiovascular emergency is the maintenance of adequate circulation. Administering CPR, calling emergency personnel, and administering oxygen are appropriate for most emergencies. The drugs used in cardiovascular emergencies are discussed individually later in the chapter.
ANGINA PECTORIS
Without a previous history of angina, diagnosis of this condition can be difficult. It often begins as substernal chest pain that radiates across the chest, to the left arm, or to the mandible. It may also produce a feeling of heaviness in the chest. The pulse becomes rapid, and tachypnea can occur. An anginal attack can be brought on by stress from pain, trauma, or fear, especially in a dental situation.
Premedication with sublingual nitroglycerin before a stressful dental situation may prevent an acute anginal attack. Treatment of an acute anginal attack (see Chapter 15) is with sublingual nitroglycerin. Opioids or diazepam are used in hospitalized patients. One should always check and make sure that the patient has not taken a medication used to treat erectile dysfunction within 24 hours of receiving nitroglycerin. If the patient has taken a medication to treat erectile dysfunction, then he should not receive nitroglycerin but should be treated in a hospital for the acute angina attack. Nitroglycerin should not be used to prevent an acute attack if these drugs have been used within 24 hours of the scheduled appointment.
ACUTE MYOCARDIAL INFARCTION
An acute MI (heart attack) often begins as severe pain, pressure, or heaviness in the chest that radiates to other parts of the body. Sweating, nausea, and vomiting can occur. The pain is persistent and unrelieved by rest or nitroglycerin (three doses). In this way, an MI can be differentiated from an anginal attack. An irregular rapid pulse, shortness of breath, diaphoresis, and indigestion can occur. Treatment includes administration of oxygen, an aspirin tablet, and an opioid analgesic agent and transfer to a hospital. The risk of death is greatest within the first 6 hours.
Hospitalized patients who have suffered an MI are given lidocaine for arrhythmias and vasopressor agents to maintain an adequate blood pressure. New drugs that can dissolve clots are administered soon after the event and may reverse the clot.
CARDIAC ARREST
When cardiac arrest occurs, generally there is sudden circulatory and respiratory collapse. Without immediate therapy, cardiac arrest is fatal. Permanent brain damage occurs in 4 minutes. Pulse is absent, and blood pressure is unobtainable. After a few minutes, the patient becomes cyanotic and the pupils are fixed and dilated. The first and most important treatment is immediate, adequate CPR.
Today, dental practices should have an automated external defibrillator (AED). An AED, if administered within the first 5 minutes of cardiac arrest, can save up to 50% of those experiencing cardiac arrest. In March of 2002, the American Dental Association (ADA) Council on Scientific Affairs recommended that dentists consider purchasing an AED for their dental offices if emergency medical services personnel with defibrillation skills and equipment are not available within a reasonable period of time. In fact, most states require AEDs for dental practices that use general anesthesia and many require them for conscious sedation. Several states require AEDs, or full-function defibrillators, for all dental practices.
Other medications used in a hospital setting for cardiac arrest include epinephrine for cardiac stimulation and lidocaine for arrhythmias. Parenteral opioid analgesics are given for the pain. Defibrillation is used to treat asystole.
OTHER CARDIOVASCULAR EMERGENCIES
Arrhythmias, another cardiovascular emergency, depend on an electrocardiogram for diagnosis before treatment. A cerebrovascular accident (CVA, stroke), resulting in weakness on one side of the body or speech defects, is treated with oxygen administration and immediate hospitalization so “clot busters” can be administered. Hypertensive crisis is treated with antihypertensive agents given intravenously (see Chapter 15). Treatment of these cardiovascular emergencies is undertaken in a hospital setting.
Other Emergency Situations
Some emergency situations involve symptoms that do not fit into the other categories.
EXTRAPYRAMIDAL REACTIONS
The antipsychotic agents (see Chapter 17) can produce extrapyramidal reactions. Parkinson-like movements, such as uncoordinated tongue and muscular movements and grimacing, can occur. Prochlorperazine (Compazine), which is used for nausea and vomiting, can produce this type of reaction. Intravenous diphenhydramine (Benadryl) is the treatment of choice.
ACUTE ADRENOCORTICAL INSUFFICIENCY
Adrenal crisis usually occurs in patients who are taking enough steroids to suppress the adrenal gland. When they are subjected to acute severe stress without increasing their steroid dose, a crisis may occur. Unable to respond to the stress, the patient has an adrenal crisis. Nausea, vomiting, abdominal pain, and confusion may result. Cardiovascular collapse and irreversible shock may result in a fatality. The treatment for adrenal crisis is parenteral hydrocortisone and oxygen by inhalation. After hospitalization, patients receive fluid replacement and vasopressor agents if symptoms dictate.
THYROID STORM
Thyroid storm is a condition in which hyperthyroidism is out of control. Signs and symptoms include hyperpyrexia, increased sweating, hyperactivity, mental agitation, shaking, nervousness, and tachycardia. Congestive heart failure and cardiovascular collapse may follow. Temperature is controlled by tepid baths and aspirin. β-Blockers are given to control the cardiovascular symptoms. Another agent that may be used is hydrocortisone. Aspirin should be avoided in these patients (displaces thyroxine [T4] from binding sites). Sodium iodide and propylthiouracil are given to inhibit the action of the thyroid gland. Untreated severely hyperthyroid patients should not be given atropine or epinephrine because these agents may precipitate a thyroid storm.
MALIGNANT HYPERTHERMIA
Malignant hyperthermia is a genetically determined reaction that is triggered by inhalation general anesthetics or neuromuscular blocking agents such as succinylcholine. The most notable symptom is a rapidly rising temperature. Baths and aspirin are used to control the elevated temperature. Prompt treatment with dantrolene (Dantrium) can control acidosis and body temperature by reducing calcium released into the muscles during the contractile response. Before dantrolene, death was a common outcome. Fluid replacement, steroids, and sodium bicarbonate may be used.
Drug-Related Emergencies
Opioids, administered in the dental office or prescribed by the dentist, can produce overdose symptoms. Respiration can be depressed, or respiratory arrest may occur. Illegitimate use of street drugs (e.g., heroin) may also produce overdose symptoms. The most common symptoms of overdose from the opioids are shallow and slow respiration and pinpoint pupils. The drug of choice for opioid overdose is naloxone (Narcan), an opioid antagonist (see Chapter 6).
REACTION TO LOCAL ANESTHETIC AGENTS
Toxic reactions to local anesthetic agents usually result from excessive plasma levels of the anesthetic. Both central nervous system (CNS) stimulation, and CNS depression can occur. The stimulation is exhibited as excitement or convulsions (see Chapter 9). Following stimulation, depression can occur with symptoms of drowsiness, unconsciousness, or cardiac and respiratory arrest. The treatment of this toxic reaction is symptomatic. If convulsions are a predominant feature, diazepam can be administered. If hypotension is predominant, a pressor agent can be given. In the presence of reflex bradycardia, atropine may be administered. Usually, patients who have a toxic reaction to local anesthetics must be watched closely, but drug administration is rarely necessary. This reaction requires a dose of local anesthetic above the maximum dental dose.
Epinephrine
Toxic reactions to epinephrine occur most often after the placement of a gingival retraction cord used before taking impressions. The symptoms range from nervousness to frank shaking and can also include tachycardia. Because epinephrine is quickly metabolized, the main treatment is to remove the cord and reassure the patient. Becoming panicky will cause the patient to release endogenous epinephrine, and the reaction will continue. Above all else, the dental health care worker must remain calm.
EMERGENCY KIT FOR THE DENTAL OFFICE
Although the choice of drugs for a dental office emergency kit will depend on individual circumstances, experience, and personal preference, the dental health care worker should make sure there is an emergency kit in the dental office (Figure 23-3). Table 23-1 lists some emergency drugs, their therapeutic uses, and their usual adult doses. Other drugs that may be included if the office personnel are trained in ACLS include level 2 drugs, atropine and lidocaine, and calcium chloride.
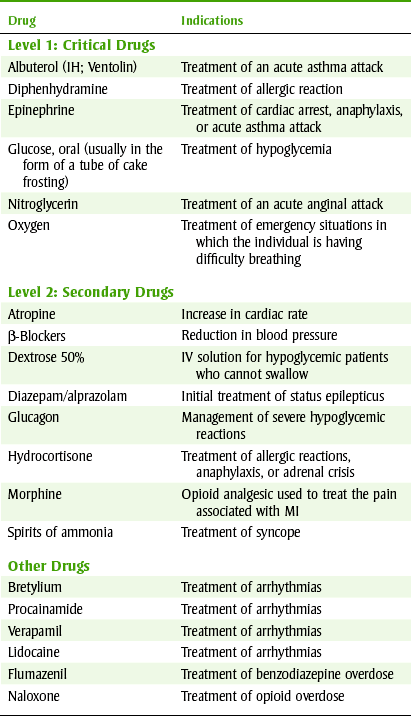
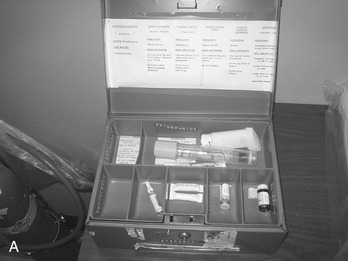
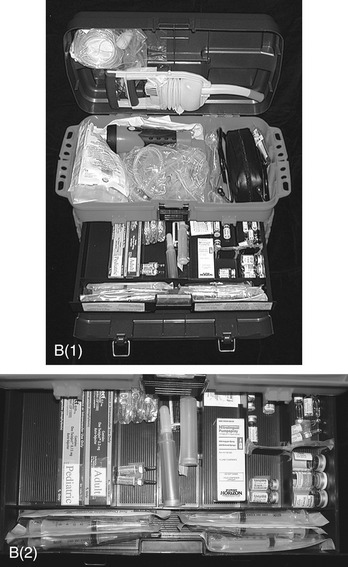
FIGURE 23-3 Examples of self-made emergency kits. A, Simple version with basic items only. B, Large version with many drugs and additional equipment. (From Malamed SF: Medical emergencies in the dental office, ed 6, St Louis, 2007, Mosby.)
Drugs
Table 23-1 lists the drugs that should be considered for inclusion in a simple emergency dental kit. These may vary, depending on the preference and experience of the practitioner. Some equipment and drugs that are not used by dental office personnel are kept in the emergency kit for use by a physician or for those with ACLS training in an emergency.
Obtaining small quantities of these medications may be difficult because they are often sold in packages of 12. A hospital pharmacy may be able to help the practitioner because the pharmacy buys in large quantities and could sell the few ampules that are needed for the dental office emergency kit. The security of the kit should be ensured by the use of a “breakable” lock that can be used to determine whether tampering has occurred. The kit should be stored in a prominent place in the dental office, but control of the agents, such as the diazepam or an opioid, if included, should be ensured.
LEVEL 1 (CRITICAL) DRUGS
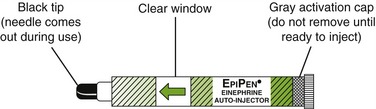
Epinephrine: Epinephrine (Figure 23-4) must be included in the dental office emergency kit for treatment of cardiac arrest, anaphylaxis, or acute asthmatic attack. It should not be used in treatment of shock because it can cause decreased venous return with increased ischemia and can precipitate ventricular fibrillation. The rationale for the use of epinephrine for cardiac arrest is β-stimulation of the myocardium. In the treatment of severe anaphylaxis and acute asthmatic attacks, it acts as a physiologic antagonist to the massive release of mediators that occurs in these conditions. Without epinephrine, these chemicals lead to bronchoconstriction and decreased oxygen exchange. Because epinephrine’s cardiac effects are diminished in the presence of acidosis, adequate mechanical resuscitation and external cardiac massage accompany its administration. Epinephrine may be administered by intravenous or intracardiac routes (by trained personnel). Dental personnel may find injection into the frenulum under the tongue more convenient.
Diphenhydramine: Diphenhydramine (Benadryl), an antihistamine, is used in the treatment of some allergic reactions. Because antihistamines compete with histamine for tissue receptor sites, a rapid reversal of allergic symptoms cannot be expected. For this reason, epinephrine and diphenhydramine are used together in severe allergic reactions or anaphylaxis.
Oxygen: Oxygen is indicated in most emergencies, especially if respiratory difficulty is a problem. Patients with chronic obstructive pulmonary disease (COPD) should be given oxygen with caution because apnea may result. All dental office personnel should know the procedure for administering inhalation oxygen. All potential members of the dental team should review the procedure on a regular basis.
Nitroglycerin: Sublingual nitroglycerin tablets or nitroglycerin spray (see Chapter 15) should be kept in the dental office emergency kit to manage an acute anginal attack. The sublingual spray may be used in place of the tablets (Figure 23-5).

Glucose: Oral glucose (Figure 23-6), or any available liquid carbohydrate, is used to manage hypoglycemia in the conscious or semiconscious patient with diabetes. If the patient can swallow, then the oral route is preferable. A small amount may be placed in the buccal pouch, where it can be slowly swallowed. Tubes of glucose for this purpose are available, or cake frosting in tubes may be used.

LEVEL 2 DRUGS
Benzodiazepines: Diazepam (Valium) and midazolam (Versed) are the drugs of choice for the treatment of most convulsions if a drug is needed. However, in the majority of cases, convulsive episodes are self-limiting and require only supportive care in the form of protecting the patient from physical harm and administering oxygen.
One cause of convulsions in the dental office is a toxic reaction to a local anesthetic from an overdose or an idiosyncrasy (see Chapter 9). Anticonvulsant drugs should be used conservatively because they may enhance CNS depression of the local anesthetic.
Aromatic Ammonia Spirits: Containers of aromatic ammonia spirits, designed to be crushed, can be used to treat syncope (Figure 23-7). Aromatic ammonia acts by irritating the membranes of the upper respiratory tract, resulting in stimulation of respiration and blood pressure. A dental office should have one (unexpired) container near each dental chair for easy access.


Morphine: Morphine and meperidine are opioid analgesics administered to a patient who has suffered an acute MI. These agents relieve pain and allay apprehension. They are used for cases of pulmonary embolism and angina for the same reasons.
Hydrocortisone: A corticosteroid used for allergic reactions, anaphylaxis, and adrenal crisis is hydrocortisone sodium. Even given intravenously, hydrocortisone has a slow onset of action. Epinephrine is still the drug of choice for anaphylaxis and serious allergic reactions because it acts immediately as a physiologic antagonist. Administration of hydrocortisone should follow the use of epinephrine, and it may be given intramuscularly or intravenously.
Dextrose: Intravenous dextrose is used to manage hypoglycemic episodes when a patient with diabetes is unconscious and cannot swallow. Hypoglycemia occurs most commonly when the patient’s insulin, exercise, and food intake are out of balance. In the dental office, all patients with hypoglycemia should be recognized before unconsciousness occurs.
Glucagon: Glucagon is used for the management of severe hypoglycemic reactions. It can be given intramuscularly, intravenously, or subcutaneously. If the patient does not respond to the glucagon, intravenous glucose should be considered.
OTHER DRUGS
Naloxone: Naloxone (Narcan), a pure opioid antagonist, is the drug of choice for opioid-induced apnea. Its use is extremely safe, but more than one administration may be needed because of its short duration of action. The initial dose is 0.4 mg (1 ml) intravenously, but it can also be given subcutaneously or intramuscularly. The onset of action is approximately 2 minutes by the intravenous route. This dose should be repeated several times in case the dose of opioid was high (sometimes a combination of self-administered plus dentist-administered opioids).
Another potential problem with giving naloxone is precipitating withdrawal in an addict (see Chapter 6). Naloxone is effective in reversing the respiratory depression caused by opioid drugs; if no response occurs, other causes for the respiratory depression must be considered. Naloxone should be in a dental emergency kit if patients are given opioids preoperatively or intraoperatively.
Flumazenil: Flumazenil (Romazicon) is a benzodiazepine antagonist used for reversing most of the effects of the benzodiazepines. It may be used after conscious sedation with diazepam or lorazepam. It should be in the emergency kit only if parenteral benzodiazepines are administered in the dental office.
Equipment
An oxygen mask, a manual resuscitation bag, and an oxygen tank with a flow gauge are needed to administer positive pressure oxygen. A sphygmomanometer and stethoscope are used to take a patient’s blood pressure. Disposable syringes, needles, and a tourniquet are used to administer medications. A laryngeal suction cannula is used to suction the throat if aspiration occurs. All dental practices should have an AED in case a patient goes into cardiac arrest. Box 23-3 lists essential equipment for a dental office emergency.
With ACLS training, a more advanced emergency kit can be prepared. Nasal and oral airways are used to maintain an unobstructed airway. Endotracheal tubes and a laryngoscope are required for intubation. Intravenous solutions, tubing, butterfly needles, and adhesive tape are used for intravenously administering drugs. A cricothyrotomy (incision through skin and cricothyroid membrane before performing a tracheotomy) kit can be used for acute airway obstruction when other measures fail.
Many dental offices will not have staff trained to use the more advanced equipment. Without training, attempts to use this equipment may be more harmful than using simple measures. If untrained, stick to CPR.
CLINICAL SKILLS ASSESSMENT
1. State what general measures the dental health care worker should be familiar with to respond to any emergency situation.
2. For each of the following common emergencies, state the signs, symptoms, and treatment (including drugs):
3. List the equipment required to treat the emergencies in question 2 and explain the rationale for the inclusion of each item.
4. Give the names of the drugs required in an emergency kit for the dental office.
5. What drugs should be included in an ideal emergency kit?
6. What are the indications for the drugs most commonly found in an emergency kit for the dental office?
 Please visit http://evolve.elsevier.com/Haveles/pharmacology for review questions and additional practice and reference materials.
Please visit http://evolve.elsevier.com/Haveles/pharmacology for review questions and additional practice and reference materials.