Other Hormones
1 Outline the functions of the anterior and posterior glands.
2 Provide an overview of the thyroid hormones and the conditions known as hypothyroidism and hyperthyroidism and the antithyroid drugs.
3 Define diabetes mellitus, list and describe the two types of this disease, its complications, issues involving dentistry, cautions and contraindications in the treatment of patients with diabetes, and the effects of drugs on complications of diabetes.
4 Name and describe the types of drugs used to treat diabetes.
5 Summarize the major female and male sex hormones and name and describe several types of hormonal contraceptives.
Hormones are secreted by endocrine glands and transported by the blood to target organs, where they are biologically active. Endocrine glands include the pituitary, thyroid, parathyroids, pancreas, adrenals, gonads, and placenta (Figure 20-1). They help maintain homeostasis by regulating body functions and are controlled themselves by feedback systems. In most of these systems, the hormone released has a negative feedback effect on the secretion of the hormone stimulating substance. Patients being treated in the dental office may be taking these hormones to treat various diseases.
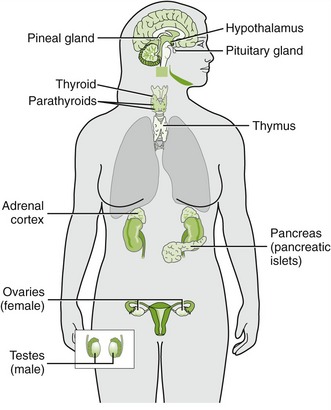
FIGURE 20-1 Locations of the major endocrine glands. (From McKenry L, Tessier E, Hogan MA: Mosby’s pharmacology in nursing, ed 22, St Louis, 2006, Mosby.)
Drugs that affect the endocrine system include the hormones secreted by the endocrine glands, synthetic hormone agonists and antagonists, and substances that influence the synthesis and secretion of hormones. The most important clinical application of these drugs is their use in replacement therapy such as in the treatment of diabetes mellitus (DM) (insulin) and hypothyroidism (levothyroxine). Additional applications include diagnostic procedures, contraception, and the treatment of glandular hyperfunction, cancer, and other systemic disorders.
PITUITARY HORMONES
The pituitary gland (hypophysis) is a small endocrine organ located at the base of the brain. It has been called the master gland because of its regulatory effect on other endocrine glands and organs of the body. It secretes peptide hormones that regulate the thyroid, adrenal, and sex glands; the kidney and uterus; and growth.
In addition to their regulatory effect, the pituitary hormones have a trophic effect that is necessary for the maintenance of many systems. For example, without the gonadotropins, the entire reproductive system fails; without growth hormone and thyrotropin, normal growth and development are impossible.
The secretion of pituitary hormones is influenced by peripheral endocrine glands via hormonal feedback mechanisms and by neurohumoral substances from the hypothalamus. When the hypothalamus releases specific hormone-releasing substances, the specific pituitary hormone is released.
Pituitary deficiency (hypopituitarism) can produce a loss of secondary sex characteristics, decreased metabolism, dwarfism, diabetes insipidus, hypothyroidism, Addison’s disease, loss of pigmentation, thinning and softening of the skin, decreased libido, and retarded dental development. Hypersecretion of pituitary hormones can produce sexual precocity, goiter, Cushing’s disease, acromegaly, and giantism. There are two parts to the pituitary gland: the anterior lobe (adenohypophysis) and the posterior lobe (neurohypophysis).
Anterior Pituitary
The anterior lobe of the pituitary gland secretes growth hormone, or somatotropin; luteinizing hormone (LH); follicle-stimulating hormone (FSH); thyroid-stimulating hormone (TSH), or thyrotropin; adrenocorticotropic hormone (ACTH), or corticotropin; and prolactin (Figure 20-2). β-Lipotropin, secreted by the pituitary, is a precursor to β-endorphin (see Chapter 6).
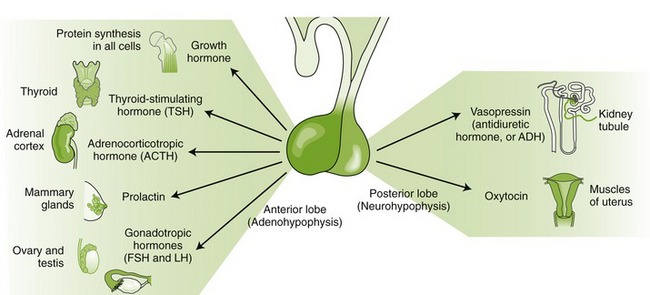
FIGURE 20-2 Pituitary hormones. Some of the major organs of the anterior and posterior lobes and their principal target organs. (From McKenry L, Tessier E, Hogan MA: Mosby’s pharmacology in nursing, ed 22, St Louis, 2006, Mosby.)
Genetic engineering has been able to produce human growth hormone since 1987. Human growth hormone is used medically to treat children who lack it and illicitly by body builders and weight lifters to develop muscles. (Some say that in athletic events at which the contestant’s urine is tested, for example, the Olympics, growth hormone cannot be detected as easily as the androgenic steroids.)
Pharmaceutical gonadotropin-releasing hormone (GnRH) is a synthetic analog. One example, leuprolide, stimulates the pituitary function and is used to treat infertility. GnRH agonists are used to treat prostate cancer and endometriosis. The secretions from the anterior pituitary that stimulate other glands are used to test the function of the stimulated glands.
FSH-like products, which stimulate follicle growth, and LH-like products, which induce ovulation, are used in the treatment of infertility. Although LH itself is not available, human chorionic gonadotropin (hCG), which is almost identical in structure, can be used as an LH substitute for deficiency. Human menopausal gonadotropin (hMG) contains FSH and LH and is commercially available as menotropin (Pergonal). This preparation is used in infertility to stimulate ovarian follicle development. When follicular maturation has occurred, the hMG is discontinued and hCG is given to induce ovulation.
 BROMOCRIPTINE
BROMOCRIPTINE
Bromocriptine (broe-moe-KRIP-teen) (Parlodel), an ergot derivative, inhibits pituitary function. Although not a hormone, it is a dopamine agonist that suppresses prolactin levels. It is used to treat prolactin-secreting adenomas (hyperprolactinemia), acromegaly, and Parkinson’s disease. In the past, it was used to dry up the milk in a woman who did not want to nurse. It is no longer used for this purpose.
Posterior Pituitary
The posterior pituitary gland secretes two hormones: vasopressin (antidiuretic hormone [ADH]) and oxytocin. Vasopressin (vay-soe-PRES-in) (Pitressin) has vasopressor and antidiuretic hormone activity and is used for treatment of transient diabetes insipidus. Synthetic analogs of vasopressin (desmopressin [DDAVP, Stimate] and lypressin [Diapid]) are used for chronic treatment of pituitary diabetes insipidus and to treat certain clotting disorders (hemophilia A and von Willebrand’s disease). Available as nasal solutions, these two analogs have the same action as vasopressin but are longer acting.
Oxytocin (oks-i-TOE-sin) (Pitocin, Syntocinon), administered either by injection or intranasally, is used to induce labor, control postpartum hemorrhage, and induce postpartum lactation.
THYROID HORMONES
The thyroid gland secretes two iodine-containing thyroid hormones: triiodothyronine (T3) and tetraiodothyronine (T4, thyroxine). Calcitonin, another hormone secreted by the thyroid, regulates calcium metabolism. Thyroid hormones act on virtually every tissue and organ system of the body and are important for energy metabolism, growth, and development. Vulnerability to stress, altered drug response, and altered orofacial development are all possible manifestations of thyroid dysfunction. The head and neck examination performed by dental practitioners can identify some thyroid abnormalities. Swallowing can accentuate the thyroid to allow palpitation. The consistency of the gland varies with the abnormality.
Thyroid hormones are synthesized from iodine and tyrosine and stored as a complex protein until TSH stimulates their release. The actions of the thyroid hormones include those on growth and development, calorigenic effects, and metabolic effects. In frogs, thyroid hormone can transform a tadpole into a frog.
Iodine
Normal function of the thyroid gland requires an adequate intake of iodine (approximately 50 to 125 mg per day). Without it, normal amounts of thyroid hormones cannot be made, TSH is secreted in excess, and the thyroid hypertrophies. This thyroid hypertrophy is called simple or nontoxic goiter. Because iodine is not abundant in most foods, simple goiter is prevalent in some areas of the world. Marine life is the only common food that is naturally rich in iodine. Use of iodized salt (contains potassium iodide [KI]) has decreased the incidence of simple goiter in many countries. Iodine is currently used in conjunction with an antithyroid drug in hyperthyroid patients preparing for surgery.
Iodide in high concentrations suppresses the thyroid in a still poorly understood manner. It may produce gingival pain, excessive salivation, and sialadenitis as side effects.
Hypothyroidism
In the small child, hypofunction of the thyroid is referred to as cretinism. In the adult, this condition is called myxedema or simple hypothyroidism. The main characteristics are mental and physical retardation. Such patients are usually drowsy, weak, and listless and exhibit an expressionless, puffy face with edematous tongue and lips. Oral findings in children usually include delayed tooth eruption, malocclusion, and increased tendency to develop periodontal disease. The teeth are usually poorly shaped and carious. The gingiva is either inflamed or pale and enlarged. The cretin is often uncooperative and difficult to motivate for plaque control. Diagnostic radiographs and routine dental prophylaxis in these patients may require special assistance.
Hypothyroid patients have difficulties withstanding stress and tend to be abnormally sensitive to all central nervous system (CNS) depressants, including the opioids and sedatives. If opioid analgesics are used, their doses should be reduced. Hypothyroid pregnant women tend to produce offspring with large teeth.
Thyroid hypofunction is rationally and effectively treated by oral administration of exogenous thyroid hormones. The most common thyroid hormone used for replacement therapy is levothyroxine (lee-voe-thye-ROX-een). Box 20-1 lists preparations used for thyroid hormone replacement therapy.
Hyperthyroidism
Diffuse toxic goiter (Graves’ disease) and toxic nodular goiter (Plummer’s disease) are the two forms of thyroid hyperfunction. Diffuse toxic goiter is characterized by a diffusely enlarged, highly vascular thyroid gland. It is common in young adults and is considered to be a disorder of the immune response. Toxic nodular goiter is characterized by nodules within the gland that spontaneously secrete excessive amounts of hormone while the rest of the glandular tissue is atrophied. It occurs primarily in older patients and usually arises from long-standing nontoxic goiter.
Hashimoto’s disease, a chronic inflammation of the thyroid associated with an autoimmune response, produces hyperthyroidism. Antithyroglobulin antibody can be detected. It occurs in middle-aged women and often occurs concomitantly with other autoimmune diseases.
Excessive levels of circulating thyroid hormone produce thyrotoxicosis. The adverse effects include excessive production of heat, increased sympathetic activity, increased neuromuscular activity, increased sensitivity to pain, ophthalmopathy, exophthalmos (protruding eyes), and anxiety. Oral manifestations include accelerated tooth eruption, marked loss of the alveolar process, diffuse demineralization of the jawbone, and rapidly progressing periodontal destruction.
The cardiovascular system is especially hyperactive because of a direct inotropic effect, increased peripheral oxygen consumption, and increased sensitivity to catecholamines. Epinephrine is relatively contraindicated in these patients. The potentiating effects of excess thyroid hormone and epinephrine on each other could result in cardiovascular problems such as angina, arrhythmias, and hypertension. β-Blockers, such as propranolol, are used to counteract the tachycardia.
In addition to their increased sensitivity to pain, hyperthyroid persons have an increased tolerance to CNS depressants. They may require higher than usual doses of sedatives, analgesics, and local anesthetics.
No treatment should be begun for any patient with a visible goiter, exophthalmos, or a history of taking antithyroid drugs until approval is obtained from the patient’s physician. Medical management of the condition is important before any elective surgery is performed. A surgical procedure or an acute oral infection could precipitate a crisis. Hydrocortisone should be administered intravenously, and cold towels should be placed on the patient. The use of epinephrine should be avoided in poorly treated or untreated thyrotoxic patients. The cardiac dose of epinephrine can be used carefully. Even in controlled patients who are considered to be euthyroid, stress should be kept at a minimum, preoperative sedation should be considered, and the dental team should be alert for signs of hypothyroidism or hyperthyroidism.
Treatment of hyperthyroidism usually includes one of the options highlighted in Box 20-2. The two most common treatments are radioactive iodine (131I) and thyroidectomy. 131I is usually the drug of choice for patients older than 21 years. It is taken internally and sequestered by the gland; localized destruction of thyroid tissue results. Thyroidectomy is the surgical approach to hyperthyroidism. Both radioactive iodine and thyroidectomy usually result in hypothyroidism because a dose that produces an inadequate effect would require repeating the procedure. If a patient has been adequately treated for hyperthyroidism with either radioactive iodine or thyroidectomy and is taking supplemental thyroid (as needed [prn]), then that patient may be treated like a euthyroid patient.
ANTITHYROID AGENTS
Antithyroid drugs, such as propylthiouracil (PTU) and methimazole (Tapazole), are used in patients who cannot tolerate surgery or treatment with 131I. These drugs interfere directly with the synthesis of thyroid hormones by inhibiting the iodination of tyrosine moieties and the coupling of the iodotyrosines. Adverse reactions associated with PTU include fever, skin rash, and leukopenia. The most serious adverse reaction is agranulocytosis, which can lead to poor wound healing, oral ulcers or necrotic lesions, and oral infections. Paresthesia of facial areas and loss of taste are also seen. Not only are antithyroid drugs used over prolonged periods to bring a hyperactive thyroid to the euthyroid state but they are also given before thyroidectomy to reduce the possibility of thyroid storm, a life-threatening acute form of thyrotoxicosis.
Propranolol, a β-blocker, is often given concomitantly with antithyroid agents. The β-blocker prevents the tachycardia and tremors.
PANCREATIC HORMONES
Two primary hormones secreted by the islets of Langerhans of the pancreas are insulin and glucagon. Insulin promotes fuel storage (pack the bags: glucose out of blood), whereas glucagon promotes fuel mobilization (empty the bags: glucose into blood) in the body. Other hormones secreted by the pancreas are islet amyloid polypeptide (IAPP; amylin) and pancreatic peptide. Their functions have not yet been elucidated.
Diabetes Mellitus
Diabetes mellitus (DM) is a group of metabolic disorders characterized by persistent hyperglycemia. It is thought that the hyperglycemia leads to the many complications of diabetes. DM is currently classified as types I and II (Table 20-1).
Symptoms and complications result, usually from inadequate or poorly timed secretion of insulin from the pancreas and/or insulin resistance of the cells. (Figure 20-3 outlines the body’s physiologic response to changes in blood glucose levels.) The new criterion for the diagnosis of DM is two consecutive fasting blood sugars (FBS) of greater than 126 mg/dl. This will simplify the diagnosis of DM and add many patients to the ranks of people with diabetes.
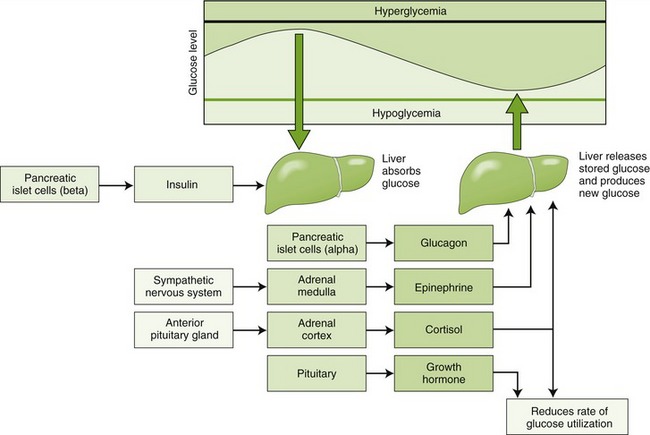
FIGURE 20-3 Physiologic response to changes in blood glucose levels. (From McKenry L, Tessier E, Hogan MA: Mosby’s pharmacology in nursing, ed 22, St Louis, 2006, Mosby.)
Diabetes is primarily characterized by hyperglycemia and glycosuria. Other characteristics include hyperlipemia; azoturia; ketonemia; and, when the deficiency is severe, ketoacidosis. Patients usually experience general weakness, weight loss, polyphagia, polydipsia, and polyuria. Patients with type II diabetes often experience weight gain.
TYPES OF DIABETES
Type I: Type I diabetes usually develops in persons younger than 30 years and results from an autoimmune destruction of the pancreatic β cells. The type I autoimmune response may be in response to an infection, a slow virus, environmental insults, or some as yet unknown factor. It is associated with a complete lack of insulin secretion, increased glucagon secretion, rapid onset of disease, ketosis, and severe symptoms. Without insulin, type I DM is fatal. Type I diabetes must be treated with injections of insulin because the pancreas does not produce any insulin.
Type II: Type II diabetes usually develops in persons older than 40 years. However, more and more cases of type II diabetes are being reported in persons younger than 20 years. This is being attributed to a much more sedentary lifestyle and lack of exercise. Fast foods, video games, and television have replaced physical activity, and as a result, obesity is dramatically on the rise and obesity is a major risk factor for developing type II diabetes. Type II diabetes is associated with the ability of the pancreas to secrete enough insulin to prevent ketoacidosis but not enough to normalize plasma glucose. The insulin secreted does not reduce the glucose levels in the serum to normal levels and could be a result of a variety of reasons (Box 20-3).
Insulin resistance develops because of prolonged hyperglycemia and resulting hyperinsulinemia. Type II diabetes involves a slower onset of disease, less severe symptoms, and lack of ketoacidosis. Tissue insensitivity to insulin, a deficiency of the pancreas’s response to glucose, and obesity results in impaired insulin action. In the presence of hyperglycemia, the resistance of the tissues to insulin and the impaired β cells’ response are exaggerated. Normal serum glucose levels improve these parameters toward normal.
Type II diabetes is treated first with diet and exercise, then with orally acting agents, and if these modalities fail, with insulin. Therefore patients with type II diabetes may be taking insulin either with or without oral agents. Because of the etiology of the hyperglycemia in patients with type II diabetes, moderate improvement of the diet and/or an increase in exercise can produce a large improvement in the glucose levels. Exercise increases the sensitivity of the cells to insulin. Unfortunately, these behavior modifications are difficult to carry out on a routine basis for almost all patients.
COMPLICATIONS OF DIABETES
Uncontrolled diabetes produces a pronounced susceptibility to dental caries. This is caused mainly by decreased salivary flow (xerostomia) related to fluid loss. The loss is secondary to an increase in urination that occurs because of poor use of carbohydrates and the glucose that is excreted via the kidneys (water follows glucose). The complications of xerostomia are a result of the lack of its normal functions: lubricating, cleansing, regulating pH, destroying microorganisms and their products, and maintaining the integrity of the oral structures.
A dry, cracking oral mucosa with the presence of mucositis, ulcers, infections, and an inflamed painful tongue may result. Any change in glucose in saliva probably contributes little to the increased caries rate.
Xerostomia: The small increase in parotid saliva glucose would appear to have little effect on the incidence of caries. In Finland, a recent study was conducted to determine the relationship between dental caries and NIDDM and its control. Over a 15-year period, 25 patients were monitored. The metabolic control of the diabetes was unrelated to dental caries. There was no increase in caries in type II diabetes over control patients. A relationship was found between a reduction in salivary flow and an increase in dental caries. DM can affect the dental development of children. Diabetic children have been shown to differ from normal children in the median ages at which they lose their deciduous teeth and gain their permanent teeth. Tooth eruption is accelerated in children with diabetes.
Periodontal Disease: Patients with uncontrolled or undiagnosed diabetes are more prone to periodontal disease. However, the periodontal status of the patient with well-controlled diabetes has been somewhat more controversial. Despite the fact that some investigators reported a lack of correlation between diabetes and increased periodontal disease, many other studies have resulted in the opposite conclusion. (It may be that if control is good, then there is hardly any effect, whereas if control is poor, then there is a greater effect.)
Periodontal findings include inflammatory and degenerative changes ranging from mild gingivitis to painful periodontitis with a widened periodontal ligament, multiple abscesses, putrescent exudates from periodontal pockets, and increased tooth mobility caused by destruction of supporting alveolar bone. Although it may be more severe, diabetic periodontal disease appears to be similar to that found in nondiabetics. The diabetic state probably serves as a predisposing factor that can accelerate the periodontal destruction originated by microbial agents. The proposed etiology for the periodontal changes seen in the patient with diabetes includes microangiopathy of the tissues, thickening of capillary basement membranes, changes in glucose tolerance factor (more glucose), altered polymorphonuclear leukocyte function, and enhanced collagenase activity.
DENTAL ISSUES
Dental appointments should not interfere with meals and should involve minimal stress. In patients with controlled diabetes, oral surgical procedures should be performed 1.5 to 2 hours after the patient has eaten normal breakfast and taken regular antidiabetes medication. Following surgery, the patient should receive an adequate caloric intake to prevent hypoglycemia. With general anesthesia, patients are often kept nothing by mouth (NPO) and should take half of their usual dose of insulin and receive intravenous 5% glucose in distilled water (D5W).
Patients with diabetes have fragile blood vessels, delayed wound healing, and a tendency to develop infections; therefore surgical therapy should be approached with caution. Scaling and soft tissue curettage usually are tolerated well. The bulk of the literature suggests that prophylactic use of antibiotics should be avoided although many practitioners routinely use antibiotics. If infection is present or if infection ensues, it should be aggressively treated. Measures to reduce the possibility of infection should be used (sterilize instruments, rinse mouth before procedures). The oral complications of diabetes are summarized in Table 20-2.
TABLE 20-2
ORAL COMPLICATIONS OF DIABETES MELLITUS
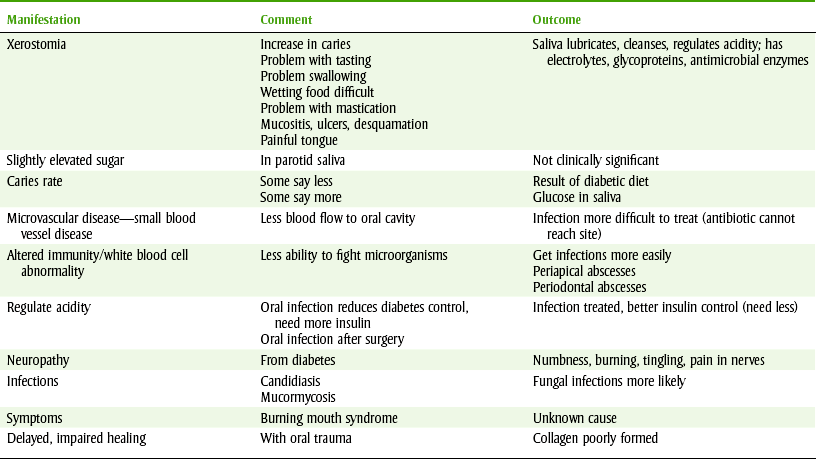
All complications worsen with hyperglycemia, either acute or chronic. Acute fasting glucose (mg/dl) measured by glucose monitor are reflective of glucose at that moment, and chronic glucose levels measured by HgA1c are reflective of glucose control over the previous 2 to 3 months. Oral complications are xerostomia, infection, poor healing, increased caries, candidiasis, gingivitis, periodontal diseases, periapical abscess, and burning mouth syndrome.
CAUTIONS AND CONTRAINDICATIONS
Drugs that may decrease insulin release or increase insulin requirements, such as epinephrine, glucocorticoids, or opioid analgesics, should be used with caution in patients with diabetes. Caution should also be exercised with general anesthetics because of the possibility of acidosis. If diabetes is in good control, then these drugs can be used.
SYSTEMIC COMPLICATIONS OF DIABETES
The systemic complications of diabetes include actions affecting almost all the body tissues and organs.
Cardiovascular System Complications: The incidence of cardiovascular problems is higher in patients with diabetes. Macroangiopathy, microangiopathy, and hyperlipidemia are common. Atherosclerosis is also more common in these patients.
Retinopathy: Because microvascular disease affects the blood supply to the retina, the functioning of the retina is impaired. In fact, diabetes is the major cause of blindness in adults.
Neuropathy: Neuropathy is another complication of diabetes. It leads to reduced and sometimes absent feelings, especially in the lower extremities. A variety of sensations, including pain and burning, have been reported. The oral complaints of pain and discomfort related to the tongue and other oral structures are related to diabetic neuropathy. Drugs used to manage this problem include amitriptyline, carbamazepine, phenytoin, and capsaicin (made from hot peppers). The neurologic problems of diabetes can produce atony of the gastrointestinal (GI) tract (diabetic gastroparesis). Metoclopramide is used to manage this complication.
Infections: Gangrene can occur in the peripheral extremities, especially the feet and legs. This occurs because of the deficiencies of diabetes, depressed immunity, less effective white blood cells, microvascular changes (less blood), and neuropathy (cannot feel the problem).
Healing: Slower healing must be taken into account so that precautions during surgery are taken. Related to this problem is the likelihood of infection, which exacerbates the healing problem.
Summary of Complications: A patient with diabetes has reduced blood flow to the feet because of microvascular disease and reduced sensation because of peripheral neuropathy. The patient has reduced ability to fight infection as a result of altered leukocyte chemotactic properties. The blood does not get to the extremities as easily, so even when antiinfective agents are present in the blood the antibiotics have difficulty reaching the site of action. Neuropathy occurs in the extremities, and these patients cannot easily feel their feet. Because there is lack of feeling, trauma or infections of the feet go unnoticed. Poor circulation, lack of feeling, and inability to fight infection lead to infection of extremities. Couple that with the fact that the patient with diabetes cannot see as well, and the pathway to disaster becomes evident.
Amputations often begin with the toes, progress to ankles and knees, and finally result in amputation of the entire leg. At the same time, microvascular disease reduces the blood supply to the kidneys, producing an increase in protein loss in the urine. Additional reduction in renal function may require dialysis or a kidney transplant. Many of the dialysis beds are filled with patients with diabetes.
EFFECT OF DRUGS ON COMPLICATIONS OF DIABETES
The Diabetes Control and Complications Trial (DCCT) was a randomized, controlled clinical trial conducted at 26 centers, primarily in the United States. The intensive intervention included additional interactions with a health care provider. Data were collected from patient notifications of events and from quarterly interviews. The 1441 volunteers had type I for 1 to 15 years. The average length of follow-up was 6.5 years. Subjects were randomly assigned to conventional or intensive diabetes treatment. Intensive therapy included three or more insulin injections daily or a continuous subcutaneous infusion of insulin (insulin pump) guided by four or more glucose tests per day.
Conventional therapy included one or two insulin injections daily. This study demonstrated that intensive treatment of patients with type I can substantially reduce the onset and progression of diabetic retinopathy, nephropathy, and neuropathy. The major risk associated with the intensive treatment is recurrent hypoglycemia that was three times higher than in those with conventional therapy.
Comparing the intensive therapy with traditional therapy resulted in both “good news” and “bad news”:
EVALUATION OF THE DENTAL PATIENT WITH DIABETES
Asking a patient “How well is your diabetes controlled?” does not often produce useable information. In my experience, the answer patients give to this question does not relate to the actual control of the patient’s diabetes. Some questions for the patient that might provide useful information are “What numbers have you been getting for your blood sugar? What was your test this morning? When did you last test your blood glucose? What were the results?” No matter what the number is, one should not be judgmental.
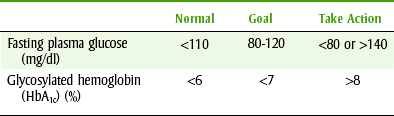
Both the oral and systemic complications of diabetes are exacerbated by poor glucose control. There are two laboratory tests useful to evaluate a patient’s glucose control: serum glucose and glycosylated hemoglobin (Table 20-3). Serum glucose is a measure of the patient’s glucose control at the time that the blood is sampled. It does not reflect the patient’s overall glucose control. The second test is the glycosylated hemoglobin (HbA1c). Because this test reflects the glucose control over a 2- to 3-month period, it more accurately measures the patient’s overall serum glucose control. Of course, a relationship exists between all the blood glucose levels and the glycosylated hemoglobin.
TREATMENT OF HYPOGLYCEMIA
One can prevent hypoglycemia by remembering that “An ounce of prevention is worth a pound of cure.” It is easy to question patients concerning their insulin use and dietary intake. The treatment of hypoglycemia depends on whether a patient retains the swallowing reflex. In the early stages, when the patient is awake, the treatment consists of any of the following: fruit juice, cake icing, glucose gel, or soluble carbohydrates. If the patient is unconscious and lacks a swallowing reflex, treatment consists of intravenous dextrose (50%). Intravenous glucose fluids and glucagon can be given. Because changes in behavior and in vital signs occur with hypoglycemia, dental teams should be able to use an oral product to manage their hypoglycemic patients. One of these items should be readily available in the dental office for emergencies.
Clinically, it is often difficult to distinguish an insulin reaction hypoglycemia (low glucose) from hyperglycemia (high glucose). It is useful to give a patient sugar for two reasons. First, the small amount of sugar used to treat hypoglycemia will produce little additional harm if hyperglycemia is present. Second, the dental office is not equipped to treat hyperglycemia. Insulin should not be administered in a dental office emergency; the patient should be immediately taken to a hospital emergency room.
DRUGS USED TO MANAGE DIABETES
Insulins: Insulin (IN-su-lin) is usually administered by subcutaneous injection because its large molecular size prevents it from being absorbed from the GI tract. The major difference among the currently used types of insulin is their onset and duration of action. The older preparations were prepared from beef or pork pancreases, but human insulin is now used exclusively. Human insulin is produced by two different processes: through recombinant deoxyribonucleic acid (rDNA) synthesis and by modifying porcine (pig) insulin. Both compounds are identical to the human insulin secreted by people. rDNA synthesis produces human insulin by gene splicing carried out by Escherichia coli. The processing of pork insulin involves transpeptidation of the pork insulin until it is the same as human insulin. Pig insulin has only two amino acids that are different from those in human insulin.
Table 20-4 lists insulin preparations, their peak effect, and their duration of action. The most common insulins used in clinical practice are human regular and neutral protein Hagedorn (NPH) (isophane insulin suspension) insulin (Figure 20-4). Lispro is made by exchanging two amino acids in the structure of human insulin. This change results in an insulin with a faster onset of action. Lispro insulin is commonly used to obtain tighter control of blood glucose.
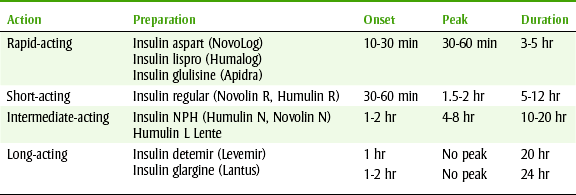
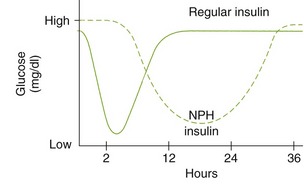
FIGURE 20-4 Serum levels of insulin and its effect on plasma glucose (milligrams per deciliter) levels. NPH, Neutral protein Hagedorn.
The most common adverse reaction associated with any insulin product is hypoglycemia. Besides hypoglycemia, inhaled insulin can cause shortness of breath, dry mouth, and cough.
The dental health care worker should be most concerned about a hypoglycemic reaction (Box 20-4) in the dental patient with diabetes who takes insulin. This can be caused by an unintentional insulin overdose (insulin shock), failure to eat, or increased exercise or stress. Symptoms that can be explained by an increased release of epinephrine from the adrenals include sweating, weakness, nausea, and tachycardia. Symptoms caused by glucose deprivation of the brain include headache; blurred vision; mental confusion; incoherent speech; and eventually, coma, convulsions, and death.
Another side effect associated with insulin is an allergic reaction, usually caused by noninsulin contaminants. Lipodystrophy at the injection site produces atrophy of the subcutaneous fatty tissue. The incidence of these reactions has decreased because the newer insulin preparations are purer and because patient education regarding changing the injection site has improved.
Oral Antidiabetic Agents: There are currently four groups of oral agents used to treat diabetes, referred to as oral antidiabetics. Each group works by a different mechanism and has a different adverse reaction profile. The oldest group of oral antidiabetic agents, the sulfonylureas, are also known as oral hypoglycemic agents. The other three groups are more precisely referred to as the antihyperglycemic agents because they lower an elevated blood sugar but do not produce hypoglycemia by themselves.
Figure 20-5 summarizes the mechanism of action of the various types of antidiabetic agents.
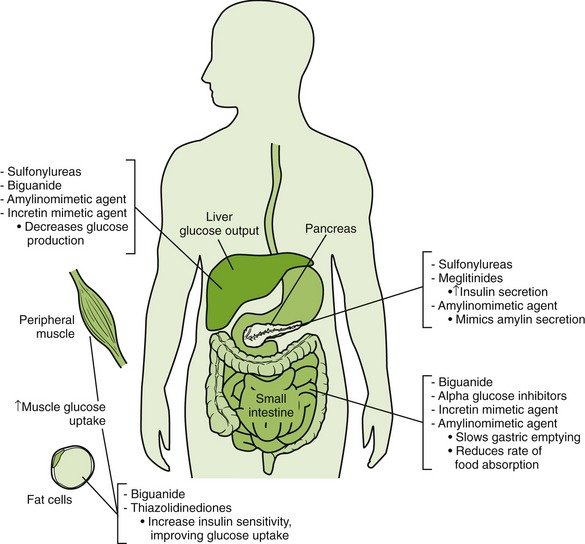
FIGURE 20-5 Mechanisms of action of antidiabetic agents. (From Clayton BD, Stock YN, Harroun RD: Basic pharmacology for nurses, ed 14, St Louis, 2007, Mosby.)
Biguanides: Metformin (met-FOR-min) (Glucophage) is a member of the biguanide group. It lowers blood glucose but, used alone, does not produce hypoglycemia. Metformin increases hepatic and peripheral insulin sensitivity, resulting in decreased hepatic glucose production (by reducing gluconeogenesis). It also increases peripheral skeletal muscle glucose uptake.
Metformin may be used alone, in combination with a sulfonylurea, or with insulin for management of type II diabetes.
Adverse reactions of metformin are primarily related to the GI tract (30%) and include anorexia, dyspepsia, flatulence, nausea, and vomiting. It can produce headache and interfere with vitamin B12 absorption. It accumulates in renal and hepatic impairment. Lactic acidosis, its most serious side effect, is rare. Predisposing factors to lactic acidosis include alcoholism, binge drinking, and renal or hepatic dysfunction. Metformin is contraindicated in patients with these conditions or patients who are fasting because metformin predisposes a patient to lactic acidosis. Oral manifestations include a metallic taste. The dose ranges from 1500 to 2550 mg divided into two or three daily doses.
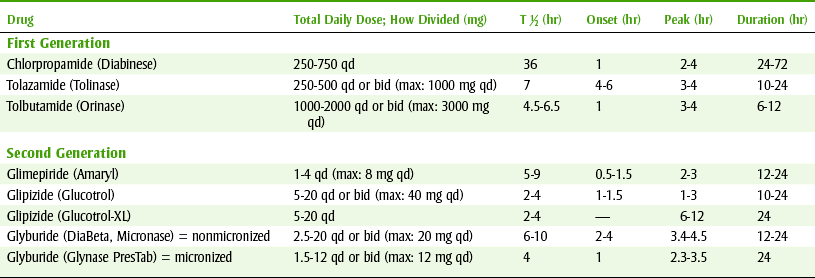
Sulfonylureas: For many years, the sulfonylureas were the only orally active agents used to manage diabetes. There are two major groups: first-generation and second-generation sulfonylureas. Their actions are similar, but the second-generation agents are more potent than the first-generation agents so their doses are smaller. Second-generation sulfonylureas have replaced first-generation sulfonylureas because they are less toxic and easier to dose than first-generation sulfonylureas. Glyburide, one of the most commonly used oral sulfonylureas, is discussed as the prototype.
The mechanism of action of the sulfonylureas (Figure 20-6) includes stimulation of the release of insulin from the β cells of the pancreas, reduction of glucose from the liver, reduction in serum glucagon levels, and increase in the sensitivity of the target tissues to insulin (probably secondary to reduced hyperglycemia).
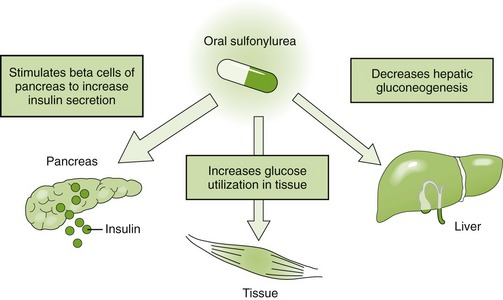
FIGURE 20-6 Mechanism of action of sulfonylureas. (From McKenry L, Tessier E, Hogan MA: Mosby’s pharmacology in nursing, ed 22, St Louis, 2006, Mosby.)
Sulfonylureas are indicated for the treatment of patients with type II diabetes who cannot be treated with diet and exercise alone. Adverse reactions of the sulfonylureas include blood dyscrasias, GI disturbances, cutaneous reactions, and liver damage. Aspirin can interact with the sulfonylureas, producing a decrease in serum glucose levels. This is not clinically significant unless the diabetic patient is especially brittle. Table 20-5 lists the first-generation and second-generation sulfonylureas, their average daily dose, and their duration of action. Tolbutamide (tole-BYOO-ta-mide) is an older first-generation sulfonylurea that was once popular, but most patients currently take a second-generation sulfonylurea.
The first line of treatment of type II diabetes usually involves a sulfonylurea and/or a biguanide. These two agents can be used together to lower the blood level more than either one individually.
In addition to the biguanides, there are two other new antihyperglycemic* drug groups that have become available for the management of diabetes. It has been suggested that rather than being called oral hypoglycemic agents they should be called euglycemic agents. They work to lower blood glucose and glycosylated hemoglobin by different mechanisms. In some instances, combining agents from more than one group can produce a greater reduction in blood glucose than either agent used alone. Table 20-6 lists some properties of these three groups of antihyperglycemic agents.
TABLE 20-6
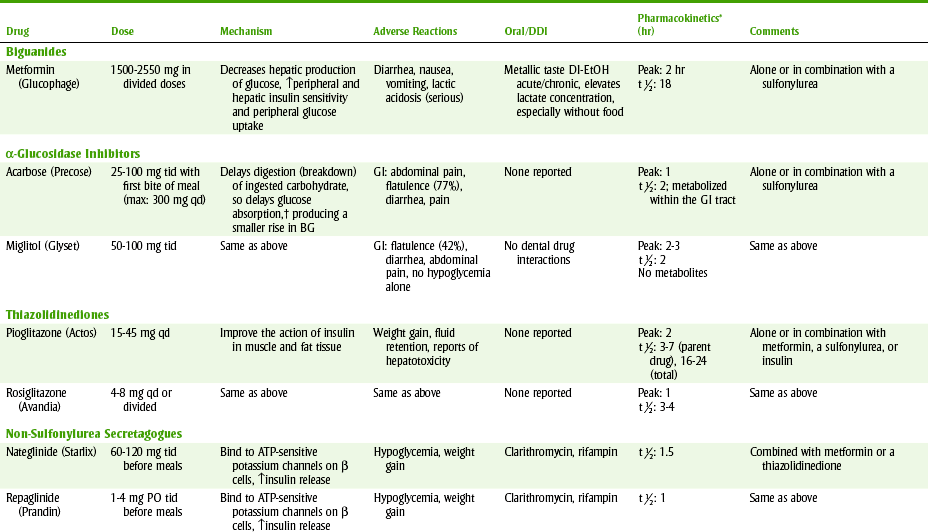
BG, Blood glucose; bid, twice a day; DDI, dental drug interactions; EtOH, alcohol; GI, gastrointestinal; LDL, low density lipoprotein; PO, by mouth; qd, every day; tid, three times a day.
* peak, duration (hr).
peak, duration (hr).
†Does not produce hypoglycemia alone; reduces the insulinotropic and weight-increasing effects of sulfonylureas.
Non-Sulfonylurea Secretagogues: Repaglinide (Prandin) and nateglinide (Starlix), although structurally different from the sulfonylureas, bind to adenosine triphosphate (ATP)–sensitive potassium channels on β cells and increase insulin release. These drugs stimulate the release of insulin from the pancreas. Insulin release is glucose-dependent and requires functioning β cells. These drugs are rapidly absorbed from the GI tract resulting in peak plasma levels of insulin within 30 to 60 minutes and return to baseline before the next meal. They must be taken with meals. If a meal is missed, then the drug should not be taken. Blood glucose control with these drugs is comparable to that of sulfonylureas. Repaglinide may be a useful alternative to a sulfonylurea in patients with renal impairment or in patients who eat sporadically. Both drugs are Food and Drug Administration (FDA) approved for combined use with metformin or a thiazolidinedione.
Hypoglycemia appears to occur less often with repaglinide and nateglinide than with sulfonylureas.
α-Glucosidase Inhibitors: Acarbose (Precose) is an α-glucosidase inhibitor. Simply, it slows the breakdown of ingested carbohydrates so that postprandial hyperglycemia is reduced. It is a competitive, reversible inhibitor of GI tract enzymes: intestinal α-glucosidase and pancreatic α-amylase. The intestinal glucosidases hydrolyze saccharides to glucose or other monosaccharides that can be absorbed. The pancreatic amylase hydrolyzes complex starches to oligosaccharides in the intestine. By inhibiting these enzymes, glucose availability and therefore absorption are delayed and postprandial hyperglycemia is lowered.
Acarbose can be used alone or with other agents, including insulin, sulfonylureas, and biguanides. Its major adverse effect is flatulence (77%), which is produced by bacteria acting on the undigested carbohydrates and producing gas. Other GI tract adverse reactions include diarrhea, abdominal pain, and distention. These effects are often tolerated if the dose of the drug is increased slowly and after using the drug for some time. Anemia and elevated transaminase levels have been reported. The dose of acarbose is 25 to 100 mg two or three times daily, given with the first bite of food.
Thiazolidinediones: Pioglitazone (Actos) and rosiglitazone (Avandia) are the only two thiazolidinediones available in the United States. These drugs increase the insulin sensitivity of adipose tissue, skeletal muscle, and the liver. They can take up to 6 to 14 weeks to achieve maximum effect. Both are FDA approved as monotherapy or in combination with metformin, a sulfonylurea, or insulin. Rosiglitazone is also approved as a third drug with both metformin and a sulfonylurea. Thiazolidinediones have an additive blood glucose–lowering effect when used in combination with metformin, sulfonylureas, or insulin.
Troglitazone (Rezulin), the first thiazolidinedione, was removed from the U.S. market because of a rare, sometimes fatal, hepatic toxicity. Hepatotoxicity has rarely been reported with rosiglitazone and pioglitazone. The FDA recommends checking serum alanine aminotransferase (ALT) levels before starting therapy and periodically thereafter. These drugs should not be used in patients with underlying liver disease or with ALT levels greater than 2.5 times the upper limit of normal. Other common adverse effects include weight gain and fluid retention.
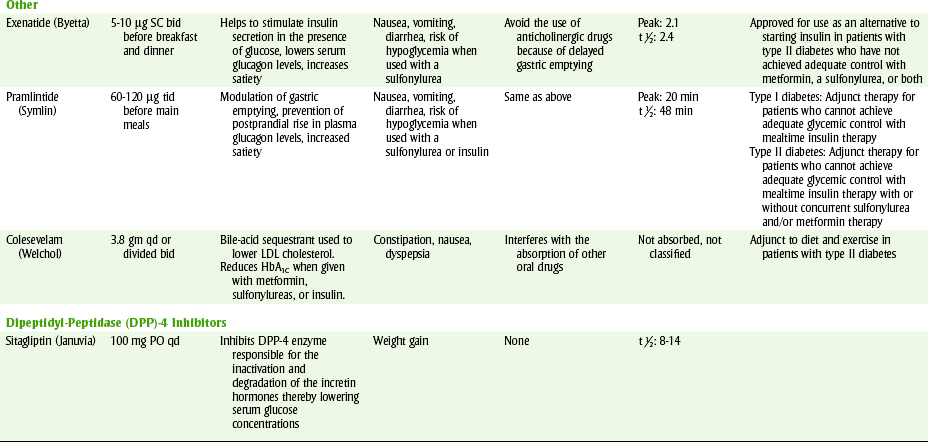
Exenatide: Exenatide (Byetta) is the first in a new class of drugs called incretin mimetics that has an amino acid sequence similar to human glucagon-like-peptide-1 (GLP-1) and in the presence of glucose acts to stimulate insulin secretion. Exenatide is indicated as an alternative to starting insulin in patients with type II diabetes who have not achieved adequate control with metformin, a sulfonylurea, or both. This drug is available as a subcutaneous injection.
The most commonly reported adverse effects include nausea, vomiting, and diarrhea. There have been postmarketing surveillance reports of acute pancreatitis in patients taking exenatide. The FDA is currently considering label changes. There is also a risk for mild-to-moderate hypoglycemia when it is used in combination with a sulfonylurea. The dose of the sulfonylurea may have to be lowered if either of these drugs is started.
Pramlintide: Pramlintide (Symlin) is an amylinomimetic agent that is responsible for modulation of gastric emptying, prevention of the postprandial rise in plasma glucagon, and satiety, which leads to decreased caloric intake and potential weight loss.
It is approved for type I diabetes as an adjunct treatment in patients who use mealtime insulin therapy and who have failed to achieve desired glucose control despite optimal insulin therapy. It is also indicated for type II diabetes as an adjunct treatment in patients who use mealtime insulin therapy and who have failed to achieve desired glucose control despite optimal insulin therapy, with or without a concurrent sulfonylurea agent and/or metformin. Like exenatide, pramlintide is available as a subcutaneous injection and should be given immediately before major meals. The most commonly reported adverse effects include nausea, vomiting, and headache.
Colesevelam: Colesevelam (WelChol) is a bile-acid sequestrant that is used to lower low-density lipoprotein (LDL) cholesterol. Its mechanism of action in treating type II diabetes is unclear. It has been approved by the FDA as an adjunct to diet and exercise for the treatment of type II diabetes. Colesevelam can cause constipation, nausea, dyspepsia, and increase serum triglyceride concentrations. It can interfere with the absorption of other oral drugs.
Dipeptidyl-Peptidase-4 Inhibitors: Sitagliptin (Januvia) is an oral dipeptidyl-peptidase-4 (DPP-4) inhibitor that has been approved for use in the treatment of type II diabetes as monotherapy or in combination with metformin, a sulfonylurea, or a thiazolidinedione, but not with insulin. It inhibits the DPP-4 enzyme that is responsible for the inactivation and degradation of the incretin hormones GLP-1 and glucose-dependent insulinotropic polypeptide. These GI hormones potentiate insulin synthesis and release by pancreatic β cells and decrease glucagon production by pancreatic α cells, thereby lowering serum glucose concentration. Modest weight gain may occur with this drug. The incidence of hypoglycemia increases when used in combination with a sulfonylurea.
Glucagon: Glucagon is a polypeptide hormone produced by the α cells of the pancreas.
Glucagon’s role is as an antagonist to insulin. Higher levels of glucagon are present in the blood of patients with diabetes, even when normal blood glucose levels are maintained. Glucagon may be used parenterally for the emergency treatment of hypoglycemia, but glucose is usually preferred.
FEMALE SEX HORMONES
There are both male and female sex hormones, and most sex hormones occur in both sexes but in different proportions.
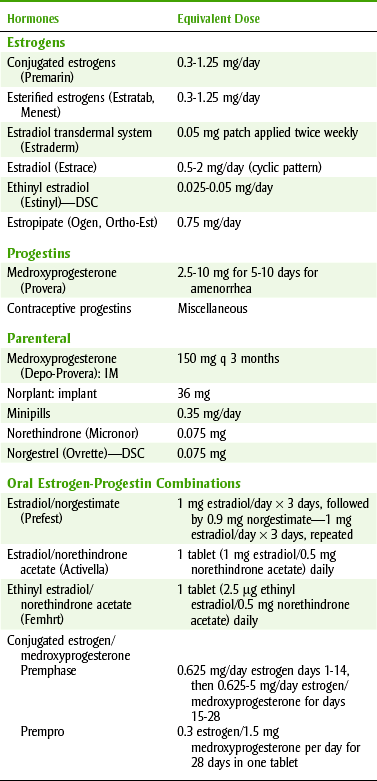
The two major female sex hormones are the estrogens (ES-troe-jenz) and progestins (proe-JES-tins) (e.g., progesterone [proe-JES-te-rone]). Products containing these hormones are listed in Table 20-7. They are secreted primarily by the ovaries but also by the testes and placenta. They are largely responsible for producing the female sex characteristics, developing the reproductive system, and preparing the reproductive system for conception.
Estrogen and progesterone levels vary daily. These changes are dependent on the pituitary gonadotropic hormones FSH and LH. The interrelationship among these hormones during the female sexual cycle is as follows: On day 1 of an average 28-day cycle, when the menstrual flow begins, the secretions of FSH and LH begin to increase. This release is caused by a reduction in the blood levels of estrogen and progesterone, which normally inhibit their release. In response to increased FSH, an ovarian egg matures, and the follicle in which it is contained grows in size and begins to produce and secrete estrogen. For reasons not entirely understood, on approximately day 12, the rate of secretion of FSH and LH increases markedly to cause a rapid swelling of the follicle that culminates in ovulation on day 14.
Following ovulation, LH causes the secretory cells of the follicle to develop into a corpus luteum that secretes large quantities of estrogen and progesterone. This causes a feedback decrease in the secretion of both FSH and LH. On approximately day 26, the corpus luteum completely degenerates. The resultant decrease in estrogen and progesterone leads to menstruation and increased release of FSH and LH. The FSH initiates growth of new follicles to begin a new cycle. Figure 20-7 illustrates the steps in the typical female menstrual cycle.
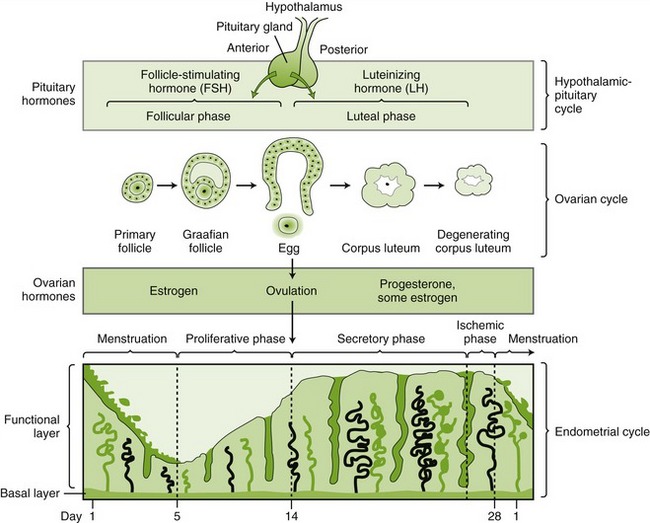
FIGURE 20-7 The menstrual cycle. (From McKenry L, Tessier E, Hogan MA: Mosby’s pharmacology in nursing, ed 22, St Louis, 2006, Mosby.)
Estrogens
In addition to their role in the female sexual cycle, estrogens are largely responsible for the changes that take place at puberty in girls. They promote the growth and development of the vagina, uterus, fallopian tubes, breasts, and axillary and pubic hair. They increase the deposition of fat in subcutaneous tissues and increase the retention of salt and water. They also cause increased osteoblastic activity and early fusion of the epiphyses.
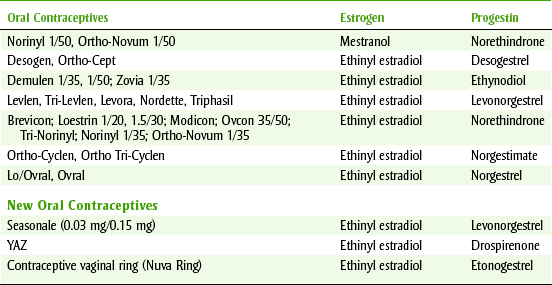
The most potent endogenous estrogen is 17β-estradiol. The liver readily oxidizes it to estrone, which in turn can be hydrated to estriol. Because synthetic estrogens can be administered orally, they are used for therapy and contraception. Table 20-8 lists some estrogens and progestins used for birth control.
In addition to their presence in oral contraceptives, estrogens are used to treat menstrual disturbances (dysmenorrhea, dysfunctional uterine bleeding), osteoporosis, atrophic vaginitis, nondevelopment of the ovaries, hirsutism, cancer, and symptoms of menopause (particularly vasomotor instability [hot flashes and night sweats]). Estradiol transdermal system (Estraderm) is applied to the skin twice a week to treat the vasomotor symptoms of menopause.
The most common side effects of estrogen therapy are nausea and vomiting. With continued treatment, tolerance develops and these symptoms usually disappear. Other side effects include uterine bleeding, vaginal discharge, edema, thrombophlebitis, weight gain, and hypertension. Estrogen therapy may also promote endometrial carcinoma in postmenopausal women. This risk may be canceled out by administration of a progestin (e.g., medroxyprogesterone [Provera]) for the last 10 days of the cycle. A small increase in risk of breast cancer has been demonstrated, but the unusual form is more easily “cured” than the usual breast cancer. The incidence of vaginal and cervical carcinoma has been shown to increase in the female offspring of women given diethylstilbestrol (DES).
EFFECT ON ORAL TISSUES
Estrogens influence the gingival tissues. For example, changes in sex hormone levels during the life of the female are related to the development of gingivitis at puberty (puberty gingivitis), during pregnancy (pregnancy gingivitis), and after menopause (chronic desquamative gingivitis). Conscientious plaque control helps to minimize these conditions. The increase in gingival inflammation may occur even with a decrease in the amount of plaque. This may be a result of increased levels of prostaglandin E (PGE), estradiol, and progesterone in the saliva.
Other side effects of estrogens are discussed in the section on oral contraceptives.
Progestins
The corpus luteum is the primary source of progesterone during the normal female sexual cycle. Progesterone promotes secretory changes in the endometrium and prepares the uterus for implantation of the fertilized ovum. If implantation does not occur by the end of the menstrual cycle, progesterone secretion declines, and the onset of menstruation occurs. If implantation takes place, the developing trophoblast secretes chorionic gonadotropin, which sustains the corpus luteum, thus maintaining progesterone and estrogen levels and preventing menstruation. Other effects of progesterone include suppression of uterine contractility, proliferation of the acini of the mammary gland, and alteration of transplantation immunity to prevent immunologic rejection of the fetus.
Medroxyprogesterone (me-DROKS-ee-proe-JESS-ter-one) (Provera), a progestin, is used orally by postmenopausal women in conjunction with estrogens. It prevents the increase in the risk of uterine cancer that can occur with unopposed estrogen. Women who have had a hysterectomy do not need to take medroxyprogesterone with estrogens.
Progestins alone are used in a variety of dose forms. Parenteral medroxyprogesterone (Depo-Provera) is administered every 3 months as a contraceptive. Progestin-only “minipills” (see Table 20-7) are used orally for contraception in patients in whom estrogens are contraindicated. They must be taken each day of the month and are slightly less effective than the combination oral contraceptive products. They are very infrequently used.
A progestational agent can be administered in the form of an intrauterine device (IUD) impregnated with a progestational agent (Progestasert) or an implant placed under the skin on the arm (levonorgestrel [Norplant]). Norplant provides contraception for at least 5 years. These implants can produce prolonged, spotty, and irregular bleeding or amenorrhea; however, many women find them convenient and problem free. The problem with Norplant seems to be that removing the five containers in which the drug was contained has proved very difficult.
The primary use of the progestins is as one of the ingredients in almost all oral contraception combinations. The second most common use is in combination with estrogen for postmenopausal women. Other uses of the progestational agents include the treatment of endometriosis, dysmenorrhea, dysfunctional uterine bleeding, and premenstrual tension.
Hormonal Contraceptives
Oral contraceptives are the most common dose forms of hormonal contraceptives and consist of estrogens and progestins in various combinations. These are the most common birth control pills and are more than 99% effective (if patient compliance is perfect). Preparations that contain a progestin alone (the minipill) are slightly less effective and produce less regular menstrual cycles but do not have most of the side effects of the estrogen contained in the combination preparation (Box 20-5).
The compounds most commonly found in oral contraceptives are the estrogens, ethinyl estradiol and mestranol, and the progestins, norgestrel, norethindrone, and norethynodrel. The combination type of oral contraceptive is taken for 21 days of each month. With a 28-day pack, the seven pills in the fourth week contain no active ingredient but remind the patient to take a pill every day. After the third week, the menstrual cycle occurs. At least three different formulations exist: the fixed combination, the biphasic (two different strengths of tablets), and the triphasic (three different types of tablets with varying amounts of the estrogenic and progestogenic component). The biphasic and triphasic agents are said to mimic the “natural” hormones more closely. No documented advantage has been demonstrated between these three combinations.
Seasonale (ethinyl estradiol/levonorgestrel) is the newest in combination oral contraceptives. Seasonale is different in that it is an extended-cycle oral contraceptive. Women take Seasonale for 3 months. Seasonale is taken once daily until the last tablet in the extended-cycle tablet dispenser is taken. The active tablets (n = 84) are pink, and the inactive tablets (n = 7) are white. The new dispenser is started the very next day. As a result, women only bleed once every 3 months (4 periods a year).
The contraceptive vaginal ring is a new dose form that introduces hormonal contraception into the body. NuvaRing is the only combination dose form in this group. It contains ethinyl estradiol and etonogestrel. The patient inserts the ring for 3 weeks during which the ring continuously releases low doses of ethinyl estradiol and etonogestrel. The ring is removed at the start of the fourth week, and the patient will then experience bleeding (their period). A new ring is inserted on day 29 of the patient’s cycle after being ring-free for a week. Patients must insert the new ring on the same day each month.
An injectable hormonal contraceptive is also available. Lunelle is a monthly birth control shot that is 99% effective when given as prescribed. It contains the hormones ethinyl estradiol and drospirenone. The injection is given by a health professional on a monthly basis.
Hormonal contraceptives interfere with fertility by inhibiting the release of FSH and LH and therefore preventing ovulation. Early follicular FSH and midcycle FSH and LH increases are not seen. In addition, these contraceptive agents interfere with impregnation by altering the endometrium and the secretions of the cervix.
The side effects associated with hormonal contraceptives include increased tendency to clot (produces thrombophlebitis and thromboembolism) and carcinogenicity. The minor side effects of nausea, dizziness, headache, weight gain, and breast discomfort resemble those during early pregnancy and are mainly attributable to the estrogen in the preparation. These effects usually last only several weeks. Other side effects include blood pressure elevation and liver damage.
The hormones in contraceptives increase gingival fluid, stimulate gingivitis, and are associated with gingival inflammation similar to but not as prominent as that seen in pregnancy. Others have not shown any significant differences between the plaque scores, gingival scores, or loss of attachment when comparing users and nonusers of oral contraceptives. This discrepancy may be based partly on differences in dose between studies. In addition, this effect may not be evident in all users but may be of clinical significance only in those persons who are highly susceptible to oral soft tissue disorders. In any case, the dentist and dental hygienist should be aware that hormonal contraceptives do have the potential to cause or aggravate gingival inflammation.
Hormonal contraceptives are also associated with a significant increase in the frequency of dry socket after extractions. This risk can be minimized by performing extractions during days 23 through 28 of the tablet cycle. For patients taking Seasonale, extractions should be limited to the end of the extended-cycle tablet dispenser when the patient is taking the white tablets. Contraindications for the use of oral contraceptives include thromboembolic disorders, significant dysfunction of the liver, known or suspected carcinoma of the breast or other estrogen-dependent neoplasm, and undiagnosed genital bleeding.
In light of the increased use of antibiotics in periodontal therapy, the importance of the antibiotic hormonal contraceptive interaction must be mentioned (Table 20-9). Certain antibiotics have been said to reduce the effectiveness of hormonal contraceptives. They are thought to do so indirectly by suppressing the intestinal flora and thus diminishing the availability of hydrolytic enzymes to regenerate the parent steroid molecule. Consequently, plasma concentrations of the steroids are said to be abnormally low, and the steroid is cleared more rapidly from the body than under normal circumstances. Some recommend that the patient might want to use an additional method of contraception until the end of her cycle. Other suggestions include the substitution of topical for systemic antibiotics, if possible, and the use of hormonal contraceptives with higher levels of the estrogen component. The latter suggestion should only be undertaken by the patient’s physician. Although all antibiotics have been implicated in this drug interaction, the incidence is indeed rare. If the patient is in the last week (week 3) or the placebo week (week 4), the chance of hormonal contraceptive therapy failure is even slimmer. In our litigation-conscious society, there should be documentation in the dental chart that the patient was informed about the rare chance of a drug interaction between oral contraceptives and antibiotics (see Table 20-9).
MALE SEX HORMONES
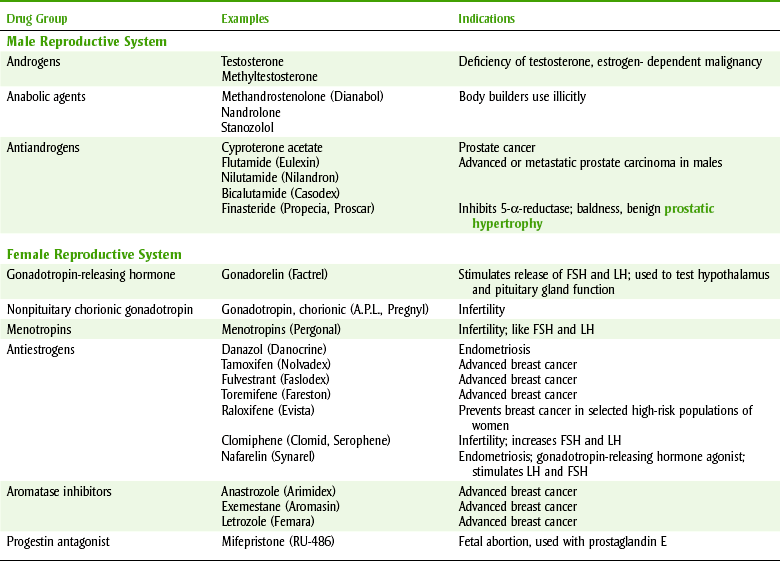
The main androgen, testosterone, has both androgenic and anabolic effects. Because there is overlap between androgens and anabolic steroids, separating them is difficult. Table 20-10 lists the male hormones and their antagonists and the female hormone antagonists. Androgens are responsible for the development of secondary male sex characteristics. Their anabolic action results in an increase in tissue protein and nitrogen retention in the body. Other actions of the androgens include increased osteoblastic activity, epiphyseal closure (cannot grow any taller), and an increase in sebaceous gland activity (increased acne).
Puberty gingivitis can occur related to hormonal changes. Androgenic steroids are used medically in the treatment of breast cancer or for replacement therapy. Treatment includes subgingival debridement and oral hygiene instructions (Box 20-6).
Androgens are used illicitly by body builders, weight lifters, and other athletes for muscle mass gain. Many athletic events now test the urine for the presence of anabolic steroids. Because of their abuse, androgenic steroids are Schedule III controlled substances (same category as Tylenol #3). The side effects of androgenic steroids include nausea, cholestatic jaundice, hepatocellular neoplasms, increased serum cholesterol, habituation, and depression and excitation. In females, virilization (acne, hirsutism, deepening voice, clitoral enlargement, malelike baldness) occurs. Considering the potential for side effects, the illicit use of these agents is difficult to understand.
OTHER AGENTS THAT AFFECT SEX HORMONE SYSTEMS
Other agents that affect sex hormones may either act like the hormones or inhibit the action of the naturally occurring sex hormones (Table 20-11). Hormones from the opposite sex are often used to manage prostate, breast, and uterine cancers because the cancer is often stimulated by the patient’s own sex hormones. For example, prostate cancer is often stimulated by testosterone, so men with prostate cancer are given estrogens to inhibit the cancer’s growth.
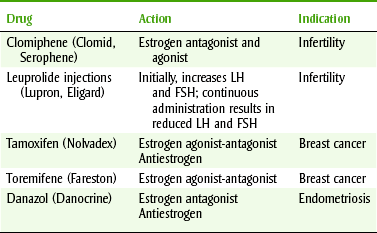
Clomiphene
Clomiphene (KLOE-mi-feen) (Clomid, Serophene) has the ability to induce ovulation in some anovulatory women. Clomiphene reduces the number of estrogenic receptors (antiestrogen) by binding to them. The hypothalamus and pituitary then falsely interpret the situation as estrogen levels that are low and increase their secretion of LH, FSH, and gonadotropins. Because clomiphene is a partial estrogen agonist, it acts as a competitive inhibitor of endogenous estrogen. Ovarian stimulation then results. Its side effects include hot flashes, eye problems, headaches, and constipation. Other side effects result from the symptoms of ovulation. Clomiphene is used to treat infertility in females and has been used experimentally for males also. The chance of multiple pregnancies increases about six times with clomiphene treatment. Female dental patients being treated with clomiphene should be considered to be pregnant, unless known to be not pregnant.
Leuprolide
Leuprolide (loo-PROE-lide) (Lupron) is a GnRH analog used intramuscularly in the management of endometriosis and to treat infertility. It suppresses production of male and female steroids as a result of a decreased level of LH and FSH.
Tamoxifen
Tamoxifen (ta-MOKS-i-fen) (Nolvadex) is a competitive inhibitor of estradiol at the receptor. It is indicated in the palliative treatment of advanced breast cancer in postmenopausal women. A large study recently published determined that the use of tamoxifen as a prophylactic (preventive) for primary breast cancer in women at increased risk reduced the risk by about 50%. A similar new drug is raloxifene (Evista).
Danazol
Danazol (DA-na-zole) (Danocrine) possesses weak progestational and androgenic action. It suppresses ovarian function and prevents LH and FSH midcycle surge. Its side effects include an increase in weight, decrease in breast size, acne, increased hair, lowered voice, headache, and hot flushes. It is used to treat endometriosis and fibrocystic breast disease in women.
Aromatase Inhibitors
Aromatase inhibitors are the newest in a group of drugs to help treat breast cancer. These drugs reduce almost the entire amount of estrogen made in the bodies of postmenopausal women. One of the advantages of aromatase inhibitors is that because they cut off the estrogen supply, they tend to cause fewer side effects than tamoxifen, especially stroke, blood clots, and uterine cancer. However, women taking aromatase inhibitors are at a higher risk for osteoporosis because they have less estrogen to protect bone density. They are indicated for the treatment of advanced breast cancer in postmenopausal women. Anastrozole is also FDA-approved for women with early-stage disease right after surgery, exemestane is FDA-approved for women with early-stage disease that have already received 2 to 3 years of tamoxifen therapy, and letrozole is FDA-approved for women with early-stage disease right after surgery and for women with early-stage disease who have completed 5 years of tamoxifen therapy.
A new indication for Colesevelam (Welchol). Med Lett Drugs Ther. 2008;50:33.
Collin, HL, et al. Caries in patients with NIDDM. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998;85:680–685.
Crofford, OB. Diabetes control and complications. Annu Rev Med. 1995;46:267–279.
Drugs for Type 2 Diabetes. Treatment Guidelines. The Medical Letter. 2008:47–54.
Eurich, DT, et al. Improved clinical outcomes associated with metformin in patients with diabetes and heart failure. Diabetes Care. 2005;28:2345.
Nathan, DM, et al. Management of hyperglycaemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement from the American Diabetes Association and the European Association for the Study of Diabetes. Diabetologia. 2006;49:1711.
The ADVANCE Collaborative Group. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008;358:2560.
The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977–986.
CLINICAL SKILLS ASSESSMENT
1. What is diabetes and what are its signs and symptoms?
2. Compare and contrast Type I and Type II diabetes.
3. What are some of the dental concerns associated with diabetes and how would the dental practitioner counsel a pediatric patient with diabetes?
4. When should a diabetic patient’s dental appointment be scheduled and why?
5. Describe the commonly used types of insulin and state their most common usage pattern.
6. What are the adverse reactions associated with insulin?
7. Name the four oral hypoglycemic agents (from different groups) and state two side effects of this group of drugs.
8. How do oral contraceptives work and what are their clinical uses?
9. What are some of the adverse reactions associated with oral contraceptives?
10. What are the dental concerns associated with oral contraceptives?
11. Describe the dental effects of hypothyroidism and hyperthyroidism.
12. What is the difference between hypoglycemic agents and antihyperglycemic agents?
 Please visit http://evolve.elsevier.com/Haveles/pharmacology for review questions and additional practice and reference materials.
Please visit http://evolve.elsevier.com/Haveles/pharmacology for review questions and additional practice and reference materials.
*Antihyperglycemic refers to agents that prevent an elevation in the blood glucose, whereas hypoglycemic refers to agents that lower blood glucose (sometimes grouped with sulfonylureas as oral hypoglycemic agents). One should note that the former does not produce hypoglycemia, whereas the latter may.