Technologies That Aid Transportation
SAFE TRANSPORTATION FOR CHILDREN
Vehicle Restraint Systems for Children
Vehicle Restraint Systems for Children With Disabilities
SAFE TRANSPORTATION OF INDIVIDUALS IN WHEELCHAIRS
Crashworthiness of Wheelchairs and Seating Systems
Wheelchair Tie-Down and Occupant Restraint Systems
On completing this chapter you will be able to do the following:
1 Describe the correct use of child restraint systems for passenger safety
2 Describe the correct use of child restraint systems designed for children with special needs
3 Understand the basic features of standards for crashworthiness of wheelchairs and seating systems
4 Understand the use and basic features of standards for wheelchair tie-downs and occupant restraint systems
5 Identify the major components of driver evaluation
6 Identify the major components of driver retraining programs
7 Discuss major design features to consider when making a vehicle purchase
8 Discuss vehicle access issues for individuals with disabilities
9 Describe vehicle modifications to promote access for individuals with disabilities
Robert Murphy, a social anthropologist who described his experience with a spinal tumor in the book The Body Silent, eloquently describes how the loss of the ability to drive deprived him of the spontaneity to go places when he wanted. This chapter explores issues and technologies related to transportation.
The inability to drive was more than a retreat from mobility, for it was one step away from spontaneity and the free exercise of will. Where as I could once act on whim and fancy, I now had to exercise planning and foresight. This was true of even the simplest of actions. (Murphy, 1990)
Chapter 12 focused on personal mobility systems, specifically manual and electrically powered wheelchairs, that afford individuals the ability to move within their immediate environments and for short distances between local environments. This chapter considers mobility systems that afford movement over longer distances, such as movement between home, school, work, and community sites such as shopping and leisure venues, as well as travel between communities. Our focus is on safe personal (car, van, etc.) and public transportation across the life span, including travel as a passenger or a driver. The technology aspects of driving will be considered here, but this chapter is not intended to provide a comprehensive discussion of driving assessment and rehabilitation.
SAFE TRANSPORTATION FOR CHILDREN
Legislation exists in most jurisdictions that requires children of certain weights and heights to travel in a child vehicle restraint system. The majority of jurisdictions require children weighing less than or equal to 40 pounds to be properly secured in a vehicle restraint system. An increasing number are also requiring the use of booster seats for children who weigh more than 40 pounds (e.g., the majority of the United States, three provinces in Canada, and the United Kingdom; legislation is pending in Australia). Many children with mild to moderate seating needs can safely sit in vehicle restraint systems that are produced for typical children who have no special seating needs, so these products will be discussed first, including their proper use and installation. The array of products is vast and constantly changing. The following discussion is general and readers should review specific requirements in their own jurisdictions, particularly those related to booster seats.
Vehicle Restraint Systems for Children
There are three main types of vehicle restraint systems for children: rear-facing infant seats, forward-facing child seats, and booster seats. A number of Web sites provide access to up-to-date information on the proper use and installation of these devices for their specific jurisdictions (Box 13-1). The Canada Safety Council has the Buckle Up Bears education program. Daimler-Chrysler offers the Fit for a Kid program that provides free car seat inspections and determination of whether the vehicle restraint system is properly installed. In the United States, the National Highway Traffic Safety Association maintains current information on vehicle restraint systems. The American Academy of Pediatrics also provides current information on vehicle restraint systems, including those specifically for children with disabilities. Federal regulations exist that govern the structure and testing of vehicle restraint systems, including those for children with disabilities. In the United States, the Federal Motor Vehicle Safety Standards (FMVSS) group produces these regulations and in Canada they are produced by the Canadian Motor Vehicle Safety Standards (CMVSS) organization. Restraint systems that meet these regulations are labeled with a sticker identifying either FMVSS or CMVSS and the specific standard that the system has met. These regulations can be found athttp://www.nhtsa.dot.gov/cars/rules/rulings/ChildRestrSyst/Index.html and http://www.tc.gc.ca/acts-regulations/GENERAL/M/mvsa/regulations/rssr/rssr.htm for U.S. or Canadian standards, respectively.
Rear-facing infant seats (Figure 13-1, A) are intended for use from the time the infant leaves the hospital after birth to the time he or she reaches 12 months and 22 pounds (10 kg). Although most vehicle restraint systems indicate a height and weight limit for the child, rear-facing infant vehicle restraint systems have an age and weight limit, which means that the child must be 12 months of age before he or she is turned to the forward-facing position. Infants younger than this age do not have sufficient head control and their bones are not sufficiently developed to withstand even a minor crash (American Academy of Pediatrics, 1996). A common error on the part of parents is to move a child to the next type of child vehicle restraint system too early (Ebell et al, 2003; Winston et al, 2000; Winston et al, 2004; Yakupcin, 2005). Many children reach the 22 pound/10 kg weight limit well before their first birthdays. In this instance, they should be moved to a vehicle restraint system that will accommodate their heavier weight but will allow them to remain in the rear-facing position. Rear-facing infant seats are typically not left in the vehicle. Rather, the child is transported in the infant seat between the vehicle and destination. The car seat belt system provides restraint for the child and the seat inside the vehicle. Some seats secure into a base that remains installed in the vehicle over the long term.

Figure 13-1 A, Rear-facing infant restraint system. B, Forward-facing child restraint system. (Courtesy of Dorel Juvenile Group.)
Forward-facing vehicle restraint systems (Figure 13-1, B) are intended to be installed in a vehicle and remain for the long term. These systems accommodate children up to and including 40 pounds and 40 inches. Proper installation of these systems is critical. A biomechanical study of the demands of installation of a forward-facing vehicle restraint system found that proper installation required efforts that exceeded maximal force output for many participants and postures that limited the force that could be produced, particularly in the shoulder. Further, the configuration of the vehicle interior resulted in postures that put parents at risk for low back injury (Fox, Sarno, and Potvin, 2004; Sarno, Fox, and Potvin, 2004).
Two errors are common when installing the forward-facing car seat: (1) nonuse or misuse of the tether strap and (2) improper use of the strapping system of the restraint system (Kohn, Chausme, and Flood, 2000; Lang, Lui, and Newlin, 2000). These seats all fasten to the vehicle frame with a tether strap. All new vehicles are equipped with tether anchors. The tether strap must be fastened and tightened so that an excursion of the restraint system of no more than ½ inch is allowed. The strapping component of the restraint system should be snug to the seat with the chest buckle about two fingerwidths below the child’s neck. Often these straps are loose, allowing the child to wiggle free of them. Since 2002 vehicles have been equipped with Lower Anchor Tethers of Children (U.S. name) and lower universal anchorage systems (Canadian name) that make installation of forward-facing car seats simpler. Clasps attached to the restraint system are attached to anchors that are fixed at the level of the seat. These systems are tested to a weight of 48 pounds (21 kg).
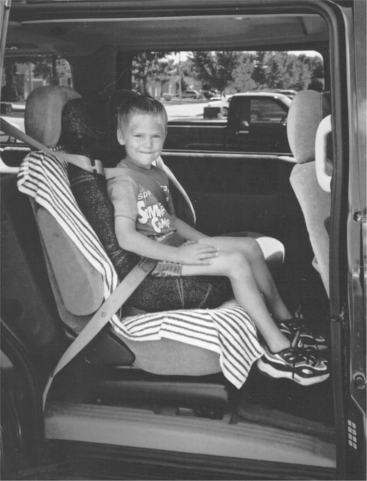
Once a child reaches 40 pounds and 40 inches, he or she can be moved to a booster seat. These seats position the child so that the vehicle seat belts fit properly. The vehicle seat belt provides restraint when a booster seat is used. Figure 13-2 shows the proper positioning of the seat belt, coming over the shoulder, not across the neck, and across the lap, not the abdomen. Booster seat laws are relatively recent and do not necessarily have the same provisions for when the child is ready to move to use the vehicle seatbelt assembly alone. Usually, a child is ready to move to use of the vehicle seat belt only when he or she reaches 80 pounds and is at least 4 feet 9 inches in height.
Location in the Motor Vehicle
The safest location for the child in a motor vehicle is the center rear seat (American Academy of Pediatrics, 1996, 1999a). When this seat is not available, the right outboard seat is preferred because this seat is usually on the side of the lane that borders the road shoulder rather than the side that faces oncoming traffic. Booster seats require the use of a three-point seat belt assembly (i.e., one that has both a shoulder and a lap portion), which sometimes precludes locating the child who uses a booster seat in the rear center seat because the restraint system in this location does not always include the shoulder portion. Children under the age of 12 years should not travel in the front passenger seat of a vehicle that has passenger side airbags. The airbags can seriously injure or kill a young child when they deploy. Some auto manufacturers have “smart” airbags that sense the weight of the occupant of the front passenger seat and either adjust the force of the airbag deployment or turn it off.
Vehicle Restraint Systems for Children With Disabilities
As previously mentioned, some children with mild to moderate seating needs are able to use a car seat that is designed for children without disabilities. This option is preferred when possible because of the costs of vehicle restraint systems that are designed specifically for children with disabilities. In some cases, the child may be able to use the child restraint system without any modification. When modifications are required, elements of the system that are provided by the original equipment manufacturer (OEM) cannot be altered or removed because the system was crash tested with those elements present. Alteration or removal may limit the ability of the seat to protect the child in a crash. Similarly, nothing can be placed underneath the padding or the straps. In the case of the strapping system, placing something underneath alters the direction of the pull on the child’s body and may cause him or her to be ejected from the seat in a crash. However, rolls can be placed alongside the child’s legs, trunk, or head to help maintain an upright position. A roll can also be placed under the child’s knees to reduce extensor tone (American Academy of Pediatrics, 1999b).
Some children with disabilities cannot be safely transported in a child vehicle restraint system that is designed for children without disabilities or they do not have sufficient postural control to be safely secured by the vehicle seat belt assembly once they become too heavy to safely use other restraint systems. Some indicators of the need for a vehicle restraint system that is specifically designed for children with disabilities are children with tracheostomies, children with either excessive high or low tone for whom the typical restraint system does not provide sufficient support, and children who have a spica cast after hip surgery.
Commercial child restraint systems for children with special needs accommodate children up to 130 pounds and 56 inches (142 cm). The weight limit varies on these products so the assistive technology practitioner (ATP) needs to check to determine that the child can be accommodated safely. In addition to accommodating children who are heavier than 100 pounds, these systems provide more postural support and have the option for greater tilt of the system. Postural control may be achieved by the form of the seat shell, providing contouring of the seat and more integral fit with the child’s body, or by padding that is supplied by the manufacturer. Some of these products have the option for the addition of a pommel to maintain leg abduction. Tilt in the system helps maintain postural control in a manner similar to that provided in mobility systems described in Chapter 12. These systems must meet federal safety standards and be crash tested for use as a vehicle restraint system.
Transportation for children who are unable to maintain a sitting position is difficult. Federal regulations exist for car beds but the companies that manufactured or distributed these devices no longer produce them. The E-Z ON Vest remains on the market as a product that will help restrain the child in the supine position. Box 13-2 lists Web sites of companies that manufacture child safety systems for children with disabilities.
SAFE TRANSPORTATION OF INDIVIDUALS IN WHEELCHAIRS
A person who routinely uses a wheelchair for mobility is safest in a motor vehicle when he or she is able to transfer into the vehicle seat and use the belt restraint systems that are supplied by the OEM. When transfers are not possible, the individual may travel in a motor vehicle while remaining seated in the wheelchair. Three factors collectively influence the increasing number of individuals who remain seated in their wheelchairs while riding in a motor vehicle: (1) legislation that promotes the rights of individuals with disabilities, (2) standards that are applied to wheelchairs and tie-down systems that relate to the design and testing of these devices for use in a motor vehicle, and (3) the increased availability of vehicle modifications that allow the wheelchair to be secured safely.
Crashworthiness of Wheelchairs and Seating Systems
Voluntary standards have been developed by the American National Standards Institute (ANSI)/Rehabilitation Engineering Society of North America (RESNA) and the International Standards Organization (ISO) that make provisions for the testing of wheelchairs and seating systems to determine their performance in a 21 g/48k m frontal impact crash simulation. These standards are ISO 7176-19 Wheeled Mobility Device for Use in Motor Vehicles (2001a) and ANSI/RESNA Wheelchairs/Volume 1: Requirements and Test Methods for Wheelchairs (including Scooters) (2000) and ISO 16840: Seating Devices for use in Motor Vehicles (2004). See Box 13-3 for a summary of the ANSI/RESNA WC-19 standard. The first two standards identify crash test procedures and manufacturer requirements for labeling and provision of information for a wheelchair and its dedicated seating. The use of an after-market seating system invalidates the wheelchair crash testing. Because many consumers purchase a wheelchair from one manufacturer and a seating system from another, ISO 16840 makes provisions for testing of a seating system independent of a specific wheeled mobility base. These standards are specific to a frontal impact; further development is required to test crashworthiness in side and rear impact crashes. Similar standards for wheelchair transportation exist or are being developed for Canada (Z605), Australia (AS-2942), and other parts of the world (ISO 10542, Parts 1 to 5). More information can be found on standards for wheelchair transportation at the Web site for the University of Pittsburgh’s RERC (www.rerc.pitt.edu).
In addition to describing the crash test procedure, the standards set peak excursion limits for the head, the pelvis, and the hip in the anteroposterior plane. They place restrictions on the condition of the wheelchair and seating system after the crash test and provide a rating system for the ease of use and the fit of the vehicle restraint system on the consumer’s body. It is important to remember that the vehicle restraint system (i.e., the vehicle seat belt) provides restraint for the wheelchair occupant, not the straps that are fixed to the wheelchair (Bertocci, Karg, and Fuhrman, 2005; Schneider and Manary, 2006). The rating system that evaluates use of the vehicle restraint system considers the following factors: the size of the opening through which the vehicle restraint system is threaded, the contact of the system with the consumer’s body and where that contact is made, the angle of the pelvic portion of the restraint system, and whether the vehicle restraint system comes into contact with any sharp surfaces (ISO 2001, 2004). As was described earlier for positioning of the vehicle restraint system for a child in a booster seat, the vehicle restraint system must sit across the pelvis, not the abdomen, and rest on the shoulder, not on the neck. Further, the vehicle restraint system must not be held away from the user’s body by any part of the wheelchair or seating system.
ISO 7176-19 and the corresponding ANSI/RESNA standard require manufacture of a frame that has four securement points for a wheelchair tie-down system. These standards apply to manual and electrically powered wheelchairs and scooters. Wheelchairs that have been successfully crash tested are commonly referred to as WC-19 chairs. As noted initially, these standards are voluntary, with the result that only a small percentage of wheelchairs have been crash tested. A number of reasons for this small proportion were identified at a recent State of the Science Workshop on Wheelchair Transportation Safety (Karg, Schneider, and Hobson, 2005). These reasons included the concern of manufacturers to assume legal liability of marketing a wheelchair as conforming to WC-19 standards, the lack of knowledge of safe transportation requirements and issues on the part of many ATPs and consumers, the added expense of purchasing a WC-19 chair, the voluntary nature of the standards, and the fact that the standards are more rigorous and conflict with federal regulations for safe transportation in a public vehicle (Schneider, Manary, and Bunning, 2005).
The requirements for manufacturers to warn users of potential hazards provide useful information regarding safe transportation for persons who travel seated in their wheelchairs. The most protected position is for individuals to be seated forward facing, yet on many public transit vehicles, the configuration for securement of a wheelchair seats the individual sideways. In addition to being unsafe in a crash, the individual feels less secure because he or she is required to adjust to the acceleration and deceleration of the vehicle. Any peripheral devices such as a communication system or a lap tray need to be removed from the chair and stored securely. Chest harnesses are recommended only when they have a quick release mechanism. Although they may be useful in aiding proper positioning of the shoulder component of the vehicle restraint system, they do have the potential to restrict the user’s airway if they become loose (Bertocci, Karg, and Fuhrman, 2005). A head restraint is also recommended (Bertocci, Karg, and Fuhrman, 2005).
Wheelchair Tie-Down and Occupant Restraint Systems
The person with a disability is best protected from injury if he or she transfers to the vehicle seat and uses the standard OEM’s restraint system (see Box 13-4 for summary; J2249 Guideline, version June 9, 1999, http://www.wheelchairstandards.pitt.edu/WCS_T/WCS_T_SAE/WCS_T_SAE_Restraints/WCS_T_SAE_Restraints.html). However, for many individuals with disabilities, transferring to the seat of a vehicle is not possible or practical. For these individuals, the wheelchair functions as the vehicle seat. Once the person is inside a personal or public vehicle as either a passenger or a driver, both the person and the wheelchair need to be properly restrained for safety. The four-point strap tie-down system with the three-point occupant restraint system is considered to be the standard means of securing a passenger who is seated in a wheelchair in a vehicle (van Roosmalen and Hobson, 2005). It is important to view wheelchair tie-down and occupant restraint systems (WTORS) as separate parts of a total system designed to protect the passenger or driver who uses a wheelchair (Thacker and Shaw, 1994). The system that secures the wheelchair to the vehicle should be separate from the restraint that protects the occupant (which is the vehicle seat belt assembly as described above). The standards that specify the design, testing, and manufacturer labeling and information are: ISO 10542, Parts 1-5 Wheelchair tiedowns and occupant restraint systems. Tie-down systems secure the wheelchair to the vehicle floor (Figure 13-3). There are two types of tie-downs that have been crash tested: four-point strap and docking types (ISO 2001b, 2001c Hobson, 2005). The four-belt type of tie-down, the most commonly used system in public transit vehicles, secures the wheelchair at each corner of the frame. In front the belts are attached to the frame (not the leg rests) just above the front caster pivot. WC-19 chairs have very obvious locations for the attachment of these straps. The strapping system and buckles are similar to those used in the aircraft industry for securing cargo. The major advantage of belt systems is low cost and their ability to secure most types of wheelchair frames. Their disadvantage is that use is time consuming and cumbersome and cannot be done independently by the wheelchair rider.

Figure 13-3 Wheelchair tie-down securement system for use of wheelchair in a vehicle. Q-Straint wheelchair tie-down system.
Docking systems have two components: a bracket that is secured to the vehicle floor and a component that is fixed to the lower portion of the wheelchair that couples with the bracket. These systems are specific to each model of wheelchair, thus limiting their use in public transit vehicles. Figure 13-4 shows the E-Z Lock system. Some of these devices have an auto engage feature; all have some feedback mechanism that tells the user that the wheelchair is properly secured (Schneider and Manary, 2006). A switch control that is either activated by the wheelchair rider or by another vehicle occupant disengages the wheelchair from the docking component. The major advantages are quick and easy connection and independent use by the wheelchair rider. The disadvantage is that they require adding hardware to the wheelchair (which adds weight), and they are two to five times as expensive as belt systems.
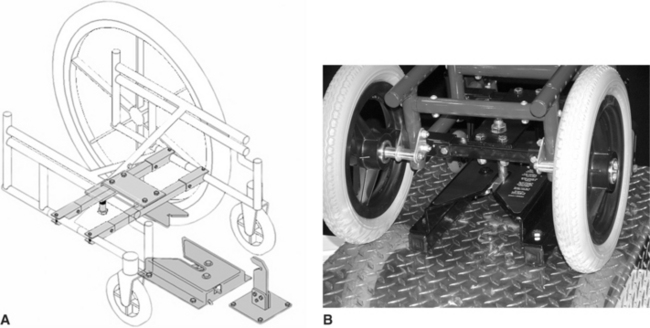
Figure 13-4 A, Schematic depicting the components of the E-Z lock system. B, Wheelchair connected to E-Z lock system in vehicle. (From Pellerito J: Driver rehabilitation and community mobility: principles and practice, St. Louis, 2005, Mosby.)
For occupant restraint, variations of seat and shoulder belts used in passenger cars can be coupled with the four-belt and docking tie-downs to form a complete WTORS. The occupant restraint can be attached either directly to the van floor or to a point that is common to the tie-down attachment point. It is less likely that the wheelchair and occupant will move different distances during a collision if the occupant restraint is attached to the latter point. If they are not attached at the same point, it is likely that the wheelchair will move farther, forcing the occupant into the restraint and causing injury (Thacker and Shaw, 1994). Both the four-point strap tie-down and the docking systems described above have disadvantages. Strap systems cannot be used independently by the wheelchair rider. Current docking systems are wheelchair specific, limiting their use to private vehicles. The ISO 10542-3 describes specifications for a universal docking interface geometry (ISO, 2005). This standard specifies the dimensions and shape of the adaptor, location on the rear of the wheelchair and dimensions of space required around the adaptor (ISO, 2005). Researchers at the Rehabilitation Engineering Research Center on Wheelchair Transportation Safety (www.rercwts.pitt.edu/) are in the process of developing and testing a universal adapter that meets these criteria.
Another advancement in the technology for securing wheelchairs in a vehicle is a passive, rear-facing system that is being introduced in Canada, Australia, and Europe for large accessible transit vehicles. This technology uses a securement station based on external structures, rather than straps, to protect the passenger in the event of a crash. A padded structure that fits closely to the person’s back and head protects in forward motion, the wall of the vehicle and a bar on the opposite side limit lateral movement, and the brakes of the wheelchair and the user’s ability to grasp a bar limit rearward movement (van Roosmalen and Hobson, 2005). Wheelchair riders prefer this system because they can use it independently. However, problems remain, most notably the unreliability of many manual wheelchair brakes and the great variance in the ability of individuals to grasp and hold the barrier to stabilize themselves (Hobson, 2005). No industry standards exist for these stations.
EVALUATION AND TECHNOLOGIES FOR TRANSPORTATION AND DRIVING
Driving is a valued activity, particularly in North America where people depend more on private vehicles than on public transportation. Driving affords independence and spontaneity. People are often very reluctant to give up their driver’s license even when they realize that they can no longer drive safely (Vrkljan and Miller Polgar, 2006). It is estimated that in 1997 70% of women and 92% of men over the age of 65 years held valid driver’s licenses. By 2012, these numbers will change to 100% of men and 90% of women (Rosenbloom, 2004).
Evaluation for Driving
An individual may require a driving evaluation for a variety of reasons, including physical disability such as spinal cord injury, impairments resulting from a cerebral vascular accident or traumatic head injury, or age-related changes such as vision loss. A driving evaluation may be used to determine whether an individual whose license has been removed because of an illness, such as a stroke, is safe to return to driving or whether an individual who is currently driving remains safe to do so. The decision to recommend to a regulatory body that an individual is no longer safe to drive is a difficult one for two reasons: the knowledge that removing a person’s driver’s license frequently results in withdrawal from social activities and depression (Marottoli et al, 2000) and the concern that this conclusion is based on sound assessment procedures. Two consensus conferences on driving evaluation recently published their findings (Korner-Bitensky et al, 2005; Stephens et al, 2005). These conferences were prompted by concern that a common driving evaluation was not used.
A driving evaluation usually has two components: an off-road assessment that is paper or computer based and an on-road component with a trained evaluator. In some situations, performance on the off-road assessment may indicate that the client is not safe to proceed with an on-road evaluation or that the on-road evaluation should be conducted in a safer environment such as a closed-circuit course.
Both consensus groups recommended that the off-road assessment should include cognitive, physical, visual, and perceptual elements, although these were not necessarily defined in the same way. The international group (Stephens et al, 2005) also included cutaneous sensation as an element and the Canadian group (Korner-Bitensky et al, 2005) included behavior as a component. Cognitive components include attention (e.g., sustained and divided attention), memory, executive functions such as organization and planning, and higher level functions such as impulse control and judgment. Visual components include useful field of view, visual acuity, contrast sensitivity, visual fields, and visual acuity. In many cases a formal visual evaluation by an optometrist or an ophthalmologist was recommended. Motor abilities include range of motion, lower extremity strength, gross motor function, reaction time, and balance. Perceptual functions include visual scanning, proprioception, and spatial relations. The international group made suggestions for specific, standardized assessments for many of these components, with the recognition that there is limited evidence to date that these assessments are predictive of driving ability (Stephens et al, 2005).
The Canadian group went on to make recommendations for an on-road evaluation. They recommended that the individual drive a course that includes many common driving maneuvers such as stopping at a light or stop sign, making right and left hand turns, merging and accelerating into traffic, driving in reverse and driving on roads with a variety of speed limits. Behaviors scored during an evaluation include but are not limited to the ability to drive at a consistent, appropriate speed, stopping when appropriate and continuing when appropriate (i.e., not stopping at a green light), maintaining a safe distance from a lead car and from cars and other objects that are parked on the side of the roadway, proper lane position, and the ability to drive safely when additional cognitive tasks are present, such as when a passenger talks to the driver.
In addition, both groups recommended that a medical history and a driving history be taken. Further, the client’s knowledge of the rules of driving should be tested. The results of these consensus groups provide an excellent start to the recognition of a consistent driving evaluation test battery. Their continued efforts to examine the relationship between driving performance and performance on the standardized tests included in the battery will provide evidence for the validity of this type of evaluation. Administration of this evaluation is very long so there remains a need for a valid screening assessment that would help clinicians determine who should proceed to a more intensive assessment when such a decision is not clear.
On the basis of the results of the evaluation, a recommendation for driving is made. The outcome of the evaluation can be one of the following: (1) the individual has the skills to continue to drive safely, (2) the individual does not have the skills required for safe driving, (3) the individual has the basic skills and continues with a driver training program, or (4) the individual has a specific impairment that limits the ability to drive with typical equipment so the individual must be assessed and trained to use adapted driving controls.
Driver Training or Retraining
Driver education and training give the opportunity for the consumer to relearn driving skills or to learn driving skills in the case of an individual who is learning to drive with hand controls. This training can include classroom activities, use of a driving simulator, and on-road instruction. Many driving schools will provide driving instruction for individuals whose basic skills are no longer safe but who have the potential to regain safe driving skills as determined by an evaluation. Classroom training is competency based and focuses on topics such as emergency driving procedures, defensive driving techniques, purchase of a vehicle, vehicle maintenance, accident responsibilities, and traffic laws. This classroom training is followed by on-road practice of basic driving maneuvers.
One well-developed driver training or refresher program is 55-Alive, which was developed by the American Association of Retired Persons in the United States and adapted for Canada by the Canada Safety Council. This program is specifically targeted to the older driver and provides off-road classes. In addition to discussing rules of the road, the program teaches safe driving strategies such as route planning, not driving at night or in bad weather, and avoiding heavily traveled freeways. Other modules talk about cognitive and visual changes that have the potential to affect safe driving, the effect of medications on driving performance, vehicle safety features, and how to judge personal fitness to drive. Although this program provides excellent information, the lack of an on-road component limits its ability to ensure that participants will be safe drivers in the actual driving situation (Bédard et al, 2004).
Driving simulators allow training of specific driving skills in a safe environment (Stephens et al, 2005). There are many different types of driving simulators. The simplest form consists of one or more computers that display a preprogrammed route. A steering wheel and brake and accelerator pedals are connected to the computer. The client may sit in a regular chair, wheelchair, or a vehicle seat. More sophisticated models project a driving route onto a screen that surrounds a vehicle on three sides. A client sits in the vehicle and uses the vehicle’s controls. The vehicle is usually fixed with this type of simulator. The most complex simulators use a pod that contains a vehicle with route projected onto a screen that surrounds the vehicle. This pod is mounted on a system that provides six degrees of freedom of movement in an attempt to simulate the motion of a vehicle. Although the technology is continually refined, there is concern that the simulated motion is not sufficiently coupled with the projected image, which can produce nausea in the client.
Driving simulators are useful tools for the driver education process (McCarthy, 2005). They allow the instructor to program specific driving elements into a system and vary the demands placed on the client. Routes can be simple, straightforward driving for use when an individual is learning to use hand controls, for example. The complexity increases with the addition of driving elements, interaction with other vehicles and pedestrians, and unexpected hazards. However, there are drawbacks to these systems. One drawback is the validity of these simulations with respect to actual on-road performance. The ability to predict on-road performance from performance on a simulator is not well established (McCarthy, 2005). A major drawback is simulator sickness. Many clients, particularly seniors, cannot tolerate the simulation and develop nausea and dizziness, which obviously limits the device’s usefulness.
Driver assessment and rehabilitation have the primary goals of keeping safe drivers on the road and helping those who have the potential to remain safe to regain necessary skills. Evaluation and retraining are linked components of this process. Because of the increasing prevalence of senior drivers in many developed countries, many resources are available that provide information about remaining safe behind the wheel and identifying signs for when driving is no longer a safe occupation (Box 13-5).
Vehicle Selection
A number of factors are important when selecting a vehicle for a person with a physical disability. Some of these include: whether the person will use the vehicle seat or a wheelchair, vehicle access, visual aspects, location and size of primary and secondary driving controls, and seatbelt and airbag design. Resources are available to assist with the process of selecting a vehicle. Most of these are geared to the elderly population (Box 13-6).
Ingress and egress refer to getting into and out of the vehicle. Miller Polgar and Shaw (2003) conducted semistructured interviews with seniors about their use of vehicle features. Seniors reported a number of factors that made ingress and egress easier, including whether the height of the seat roughly matched the hip, a wide door opening, and some form of handle to help them steady themselves. Seats that have less bucketing also make transfers easy. Figure 13-5 shows an after-market modification of a passenger seat that pivots 90 degrees and then moves forward and down to come out of the vehicle to facilitate transfers. Seniors also reported that the weight of the door affected ingress and egress; a door that was too heavy was a concern because seniors felt less stable when they reached out to close it. Once in the vehicle, the driver should determine access to the steering wheel, pedals, and controls for secondary functions such as windshield wipers.

Figure 13-5 After-market seat modification that rotates seat 90 degrees and moves it toward outside of vehicle to facilitate transfer. (Courtesy Braun Corporation.)
Visual aspects are another consideration when selecting a vehicle. The driver needs to determine the sightlines in the vehicle and whether there is clear visual access to the front, the side, and the mirrors. Further, the driver needs to determine whether he or she can read the information on the dashboard, both during the day and at night. A final aspect of vision relates to the location of various controls. Are controls for important features such as the temperature and wipers located in such a way that a quick glance away from the road is sufficient to guide a reach to use them?
The location and size of the controls have physical as well as visual implications. Consideration should be made of the range of motion required to reach vehicle controls for features such as wipers, turn indicators, temperature, and window defrost. Are they of sufficient size that the driver or passenger can target them accurately when reaching? What force is required to activate them? What action is required to activate them? Modifications to these controls are discussed in a later section.
Seniors who participated in the study by Miller Polgar and Shaw (2003) overwhelmingly indicated that seatbelts were problematic. They were difficult to reach, fasten, and unfasten. Participants had difficulty seeing the coupling mechanism. In some vehicles the location of the receiving part of the seatbelt is very difficult to see. Seatbelts did not fit properly (as described above), often sitting uncomfortably on the neck. Some after-market products are available which attempt to make the seatbelt more comfortable. These devices are not regulated, so there is the potential that they may invalidate any crash testing completed with the seatbelt and limit the potential of the seatbelt to protect the occupant in a crash. After-market devices should not alter the proper fit of the seatbelt.
Consideration should be made of the safe use of airbags. The driver should sit about 10 inches away from the steering wheel to avoid injury from an airbag that is activated at less than that distance. The height and weight of passengers is a further issue. Car manufacturers recommend that children under the age of 12 years should not occupy the front seat in a car equipped with passenger airbags because of the risk of serious injury or death. Adults who are the height or weight as a typical 12-year-old are at similar risk. Many new vehicles have sensors in the seat that vary the force with which the airbag activates or whether the airbag activates in a crash on the basis of the weight of the seat occupant.
Access to storage of a mobility device and any regularly transported equipment should be checked. If a vehicle occupant uses a wheelchair that is transported with the individual, it is important to determine whether the wheelchair will fit in the vehicle and how difficult it is to lift and position in the vehicle. This suggestion seems like a very obvious one, but it is one that can be neglected with a very frustrating outcome.
A final consideration is whether an individual who uses a wheelchair will transfer into the vehicle seat or whether he or she will be transported in the wheelchair. This discussion will focus on the driver because of access issues to driving controls, but many of the comments will be applicable to a passenger who regularly uses a wheelchair. Transfer to the vehicle seat provides the most protection for the occupant because the OEM’s seat belt provides the most effective protection in a crash (Schneider and Manary, 2006). The vehicle seat back and headrest also provide better protection than that of a wheelchair seating system. The vehicle seat should put a driver in a better position to reach necessary controls. However, use of the vehicle seat does require the ability to complete a transfer relatively easily. A seating system will provide the user with a better functional position generally than a vehicle seat will do (Phillips, Fisher, and Miller Polgar, 2005). The most important limitation of using the vehicle seat concerns individuals at risk for pressure ulcers. Vehicle seats are not designed with tissue integrity in mind and over a long trip a pressure ulcer could easily develop.
The benefits and limitations of remaining in a wheelchair during transportation are the reverse of the above with some additional factors. The wheelchair seating system is designed to give better postural control and trunk stability than a vehicle seat, which are important safety considerations for either a driver or a passenger (Phillips, Fisher, and Miller Polgar, 2005; Schneider and Manary, 2006). Any vehicle tie-down system will not be as safe a restraint as the OEM’s system. A less apparent consideration is the suspension system of the wheelchair. Vehicle seats do not have suspension systems, so the seat does not move independently of the vehicle. Such is not the case with a wheelchair with a suspension system. Travel in these chairs may have the uncomfortable side effect of motion sickness (Phillips, Fisher, and Miller Polgar, 2005).
Vehicle Access
Ingress and egress issues for an individual who transfers into a vehicle seat were considered above. This section will discuss access issues for individuals who remain in their wheelchairs for transportation. In these instances, the vehicle will be a modified van. Also considered will be after-market devices that load and store the wheelchair once the user has transferred to a vehicle seat.
Van modifications typically involve provision of a ramp or lowered floor for access and a tie-down system to secure a wheelchair. The latter were discussed in an earlier section of this chapter. These are either side or rear loading, manual or power operated. They provide access through the sliding passenger door or the rear. Figure 13-6 shows a lowered floor that accesses the side sliding passenger door. Newer designs store the lowered floor in a recessed area on the van floor so they do not interfere with access inside the vehicle. Many car manufacturers provide reimbursement for after-market modifications required to make a van accessible. The Web addresses for the main van conversion companies are listed in Box 13-7.

Figure 13-6 Side access lowered floor accessible minivan for transfer with wheelchair into and out of vehicle. (Courtesy Braun Corporation.)
Integration of the wheelchair with the van modifications is critical. A mismatch between these mobility devices is a very expensive mistake. The consumer needs to know the dimensions and configuration of his wheelchair before proceeding with van modifications. The following should be considered: (1) the width of the wheelchair for movement through the opening into the vehicle and maneuvering once inside the vehicle, (2) the height of the wheelchair for head clearance (remember that a tilt chair may increase the overall height, and (3) the length of the wheelchair and consequent turning radius; front rigging and the need for a reclined position will increase the length of the wheelchair. If a person remains in the wheelchair to drive, further considerations are made. He or she must be able to fit into the space allocated for the driver. The seat height must not interfere with the travel of the steering wheel. He or she must be able to reach the necessary controls and finally be able to see out of the front and side windows and access the mirrors. In some situations, if the seat height is too high, the driver will not be able to see out of the front window (Phillips, Fisher, and Miller Polgar, 2005). These are important considerations; a modified van that does not accommodate the user’s wheelchair is of no benefit.
If it is not possible for the individual to load the wheelchair manually into the vehicle, there are powered wheelchair-loading devices that can assist with this function. These devices pick up and store a manual wheelchair in the back seat, in the trunk, or in a carrier attached to the roof or back of the car. Figure 13-7 shows an example of a loading device that folds and stores a conventional wheelchair inside a cover that is mounted on top of the car. The other advantage of this type of loading device is that the wheelchair does not take up room in the trunk or back seat. These devices can be operated either from outside or inside the vehicle.

MODIFICATIONS FOR DRIVING
The driver with a disability needs to be carefully evaluated for any modifications that are being considered. The assessment of an individual for driving modifications progresses in a logical manner, starting with an assessment of ability to operate the primary controls, followed by an assessment of the use of the secondary controls. Once modifications are recommended, only a reputable dealer should install them.
Primary Driving Controls
The primary driving controls are those that are used to stop (brakes), go (accelerator), and steer. Modifications are available to assist the driver to maintain a grip on the steering wheel, to access the pedals, or to control the vehicle with the hands and arms only when the driver does not have use of the legs to control the vehicle. Each of these vehicle modifications will be considered in turn.
There are a number of options to consider for steering for drivers who use one arm or use a prosthetic arm or who have impaired arm and hand function. For a driver who uses one hand to steer, a steering device allows the driver to maintain control of the wheel at all times (Lillie, 1996). Evaluation of the client’s hand function determines both the type and location of the device (Bouman and Pellerito, 2006). Steering devices attach directly to the steering wheel or to a bar that stretches across the inner diameter of the wheel and attach to each side of the steering wheel. These devices are frequently removable so that another person can drive the vehicle (Bouman and Pellerito, 2006). Steering devices (shown clockwise in Figure 13-8) include palm grip, tri-pin, fork-grip or V-grip, spinner knob, and amputee ring (for use with prosthetic hooks). Additional modifications for steering may include a reduced-effort or zero-effort steering mechanism, a steering wheel of reduced diameter, height and angle adjustments to the steering column, and reduced gain (the number of turns of the steering wheel required to pivot the wheels from fully left to fully right). Reduced- or low-effort steering systems reduce the effort required for steering a vehicle by 40%, whereas zero-effort systems are able to reduce the effort required by 70% (Peterson, 1996).
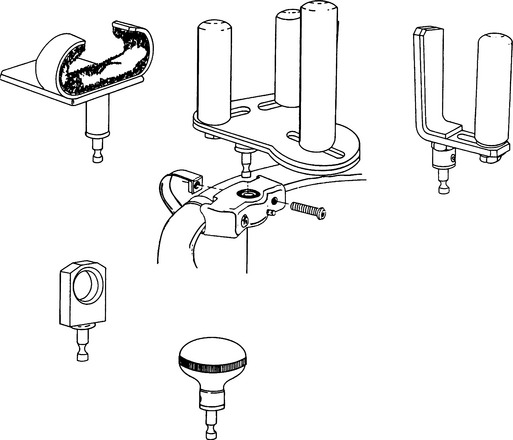
Figure 13-8 Different steering aids that accommodate a variety of consumer needs. (Courtesy Mobility Products and Design.)
Two primary types of pedal adaptations are available: a left foot accelerator and pedal extensions (Bouman and Pellerito, 2006). The latter are available from many OEMs and are used by individuals who are not able to reach the pedals. As the name would indicate, the left foot accelerator allows the driver to control both braking and acceleration with the left foot. This device is also removable for other drivers. It requires an automatic transmission vehicle.
Hand controls for accelerator and brake consist of a mechanical linkage connected to each pedal, a control handle, and associated connecting hardware. There are four common design approaches: push-pull, push-twist, push-right-angle-pull (Bouman and Pellerito, 2006; Lillie, 1996; Peterson, 1996), and push-tilt (Bouman and Pellerito, 2006). In each case the first designation (e.g., push) refers to activation of the brake and the second (e.g., pull or twist) is used for activation of the accelerator. By using a push control (Figure 13-9, A), the consumer activates the brakes by pushing on a lever in a direction directly away from him or her, parallel to the steering column. Acceleration is accomplished either by pulling back on the control, rotating it, or pulling downward at a right angle to the steering column. The weight of the user’s hand is sufficient to maintain a constant velocity. When the accelerator control is released, it returns to the off position. These controls are easily attached to almost any vehicle by the connecting hardware, which clamps a rod to each pedal and stabilizes them by attachment of a mounting bracket to the steering column. The connecting rods are adjustable in length to accommodate different vehicles. They are normally operated with the left hand, and the right hand is used for steering; however, right-hand mounting systems are also available from a variety of manufacturers (Bouman and Pellerito, 2006).
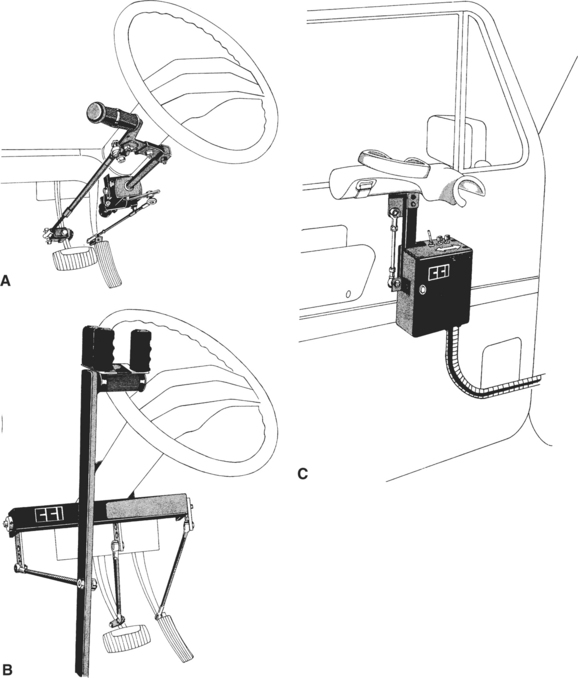
Figure 13-9 Hand control for braking and acceleration. A, A push-twist hand control. Pushing down applies the brakes, and twisting the lever to the left accelerates the vehicle. B, A mechanically assisted manual system. C, An electrically assisted controller and interface. (Courtesy Creative Controls, Inc.)
Additional assistance is required for persons with weak upper extremities (e.g., high-level spinal cord injury). There are two basic approaches: (1) mechanical assist and (2) power assist. Mechanical assist systems use one of the approaches described above, but they provide a lever arm that affords a mechanical advantage (Figure 13-9, B). Instead of connecting the hand control directly to the accelerator and brake pedals, there is a mechanical linkage that magnifies the force applied by the user. Typically this is a long arm, attached to the floor, that is pulled back for acceleration and pushed forward for braking. The arm is also linked to the pedals through connecting hardware. Power-assisted devices use either hydraulic or pneumatic assist (similar to power brakes or steering) or electronic powered systems. Electronically powered systems add servomotors that apply force to the brake and accelerator system. An electronically assisted brake and accelerator control is shown in Figure 13-9, C. One of the most recent developments is the use of a joystick that the driver pushes back for acceleration and pushes forward for braking.
Secondary Driving Controls
In addition to the controls necessary to maneuver the vehicle, secondary driving controls are needed for safe operation of a vehicle. These include turn signals, parking brakes, lights, horn, ignition, temperature control (heat and air conditioning), and windshield wipers. The knobs for operating secondary controls may not be within reach of the driver or may be of such a shape that the driver cannot operate them (Bouman and Pellerito, 2006). These knobs can be adapted by adding extensions or a differently shaped control or by relocating them so the driver can use them. A control panel that contains all these functions can also replace the standard controls. This panel is a special-purpose membrane keyboard that interfaces through a microcomputer to activate the secondary functions. It is mounted to either side of the steering wheel in a location that is within reach of the driver (Figure 13-10). Drivers who only have the use of one hand have an option of a voice-activated control panel that activates the functions above through spoken commands (Bouman and Pellerito, 2006).

SUMMARY
Access to a vehicle affords independence and the ability to participate in community activities. Technology relating to occupant protection and vehicle access, either as a driver or a passenger, needs to be considered in light of its ability to provide safety when traveling in the vehicle. This chapter considered assistive technology that aids safe transportation for individuals with disabilities. A primary concern is occupant protection, which included selection and use of proper vehicle restraint systems for children who are not able to use the vehicle seatbelt assembly and for individuals with mobility impairments who remain seated in a wheelchair while riding in an adapted vehicle. The factors that need to be considered when determining whether an individual can transfer to a vehicle seat or needs to remain in a wheelchair were discussed. Further, the voluntary standards that guide the testing and labeling of wheelchairs for use during transportation and for vehicle tie-down and occupant restraint systems were also discussed. Two further main topics were covered in this chapter: vehicle access and selection and driver evaluation and retraining, including vehicle modifications for driving.
Study Questions
1. What are the three main categories of child restraint systems for vehicles? What are the indications for the use of each category?
2. What modifications can be made to a child restraint system, designed for a typically developing child, that accommodate the positioning needs of a child with a disability? What types of modifications cannot be made to these systems? Why?
3. Describe the advantages and disadvantages of transferring to the OEM vehicle seat for travel in a vehicle, rather than remaining in a wheelchair. Describe the advantages and disadvantages of remaining in a wheelchair when traveling in a vehicle.
4. Name the standards that set the criteria for crash testing and labeling of wheelchairs and seating systems. What are the requirements of these standards?
5. Define a wheelchair tie-down and occupant restraint system.
6. Describe the advantages and disadvantages of each of the two types of wheelchair securement systems for vehicles.
7. What off-road components are recommended for inclusion in a driver evaluation?
8. What on-road components are recommended for inclusion in a driver evaluation?
9. What are the advantages and disadvantages of the use of driving simulators for driving evaluation and retraining?
10. Describe the major considerations for selection of a vehicle for use by an individual with a disability, as either a driver or a passenger.
11. Discuss the elements that need to be considered to ensure that an individual’s wheelchair is compatible with the modified vehicle.
12. What are primary and secondary vehicle controls?
13. How are primary mechanical hand controls designed and operated? What are the major types?