Sebaceous and sweat glands – Acne, rosacea and other disorders
Acne
Acne is a chronic inflammation of the pilosebaceous units, producing comedones, papules, pustules, cysts and scars. It affects nearly every adolescent. Acne has an equal sex incidence and tends to affect women earlier than men, although the peak age for clinical acne is 18 years in both sexes. Acne results from:
 increased sebum excretion – seborrhoea (greasy skin)
increased sebum excretion – seborrhoea (greasy skin)
pilosebaceous duct hyperkeratosis and comedone formation
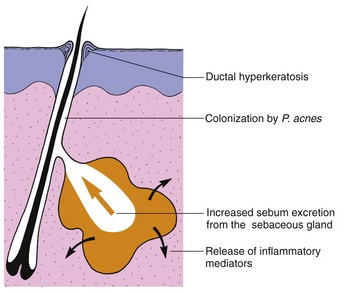
In acne, the androgen-sensitive pilosebaceous unit (p. 4) shows a hyper-responsiveness that results in increased sebum excretion. Factors in sebum induce comedones, and P. acnes initiates inflammation through chemical mediators inducing enzymes (e.g. lipase) and prostaglandins (Fig. 1).
Clinical presentation
Comedones are either open (blackheads: dilated pores with black plugs of melanin-containing keratin) or closed (whiteheads: small cream-coloured, dome-shaped papules). They appear at about the age of 12 years and evolve into inflammatory papules (Fig. 2), pustules or cysts (Fig. 3). The sites of predilection – the face, shoulders, back and upper chest – have many sebaceous glands. The severity of acne depends on its extent and the type of lesion, with cysts being the most destructive.


Acne usually persists until the early twenties, although in a few patients, particularly women, the disease continues into the fifth decade. Scars may follow healing, especially of cysts or abscesses. Scars may be ‘ice-pick’, atrophic (Fig. 4) or keloidal.

Some variants of acne are seen:
Acné excoriée: due to squeezing, affects depressed or obsessional young women.
Chloracne: caused by systemic toxicity of certain aromatic halogenated industrial chemicals.
Conglobate: a mass of burrowing abscesses and sinuses with scarring.
Cosmetic: pomade and cosmetic-induced comedonal and papular acne (mainly seen in the USA).
Drug-induced: by systemic steroids, androgens and topical steroids.
Infantile: mostly found on the faces of male infants; cause unknown.
Physical: occlusion by the back of a wheelchair or on a violinist’s chin.
Complications and differential diagnosis
Embarrassment, social withdrawal and depression are important sequelae of acne. These can improve with effective treatment. The rare and severe acne fulminans, seen in adolescent males, is associated with fever, arthritis and vasculitis. Long-term antibiotic treatment may induce a Gram-negative folliculitis.
Rosacea can usually be differentiated from acne (see below). Bacterial folliculitis is more acute than acne, but the two may coexist.
Management
Treatment depends on the type and extent of acne and the patient’s psychological state. ‘Over-the-counter’ creams have often already been used.
Local treatment is adequate for mild acne and is used with systemic drugs for more severe cases.
Benzoyl peroxide (Panoxyl, Brevoxyl) cream or gel, applied twice a day, works by reducing the number of P. acnes. It may cause irritation, contact allergy and bleach clothing.
Tretinoin (Retin-A gel) is good at reducing the number of comedones, but may be irritant.
Antibiotics, e.g. clindamycin alone (Dalacin T) or with benzoyl peroxide (Duac), erythromycin alone (Stiemycin) or with zinc (Zineryt), can be used for mild or moderately severe acne.
Other topical agents, e.g. azelaic acid, isotretinoin and adapalene.
Oral treatment with antibiotics, retinoid or hormones is prescribed for moderate or severe acne, acné excoriée and in depressed patients.
Antibiotics
The first-line systemic antibiotic drug is oxytetracycline, 500 mg twice daily (taken half an hour before food with water), given for a minimum of 4 months. Tetracyclines are contraindicated in children and in pregnancy, and may cause Candida albicans infection or photosensitivity. Lymecycline (Tetralysal, 408 mg daily) and doxycycline (Vibramycin, 100 mg once daily) are alternative tetracyclines that are better absorbed.
Erythromycin (500 mg twice daily) and trimethoprim are second-choice antibiotics. Women on oral contraceptives who take an antibiotic are advised that, if diarrhoea develops, additional contraception is needed for the rest of the menstrual cycle.
Antiandrogen
The combination of an antiandrogen and an oestrogen (co-cyprindiol–cyproterone acetate, 2 mg, and ethinylestradiol, 35 mcg: Dianette) is used in females (not males) with moderate to severe acne that is resistant to conventional therapy. The antiandrogen suppresses sebum production. Co-cyprindiol is given for 6–12 months and is also a contraceptive.
Retinoid
Isotretinoin (Roaccutane), which reduces sebum excretion, inhibits P. acnes and is anti-inflammatory, is a very effective treatment for acne. It is used if acne is severe or unresponsive to conventional treatment, or if acne relapses quickly once antibiotics are stopped. A course lasts 4 months and requires the monitoring of liver function and fasting lipids. Isotretinoin is teratogenic. Women given the drug must not be pregnant and need to take the oral contraceptive throughout treatment and for the month before and after. Side-effects include cracked lips, dry skin, nose bleeds, hair loss, muscle aches and mood change.
Rosacea
Rosacea is a chronic inflammatory facial dermatosis characterized by erythema and pustules. The cause of rosacea is unknown. Histologically, dilated dermal blood vessels, sebaceous gland hyperplasia and an inflammatory cell infiltrate are seen. Sebum excretion is normal.
Clinical presentation
Rosacea has an equal sex incidence. Although commonest in middle age, it also affects young adults and the elderly. The earliest symptom is flushing. Erythema, telangiectasia, papules, pustules (Fig. 5) and, occasionally, lymphoedema involve the cheeks, nose, forehead and chin. Rhinophyma, hyperplasia of the sebaceous glands and connective tissue of the nose (Fig. 5), and eye involvement by blepharitis and conjunctivitis are complications. Sunlight and topical steroids exacerbate the condition. Rosacea persists for years, but usually responds well to treatment. Rosacea lacks the comedones of acne and occurs in an older age group. Contact dermatitis, photosensitive eruptions, seborrhoeic dermatitis and lupus erythematosus often involve the face but are more acute or scaly, or lack pustules.

Management
Topically, metronidazole 0.75% cream (Rozex) or azelaic acid may be helpful. If this is ineffective, the usual oral treatment is oxytetracycline, initially 1 g daily, reducing to 250 mg daily after a few weeks and continued for 2–3 months. Erythromycin is an alternative. Repeated treatment is often needed. Isotretinoin can be used but is less effective than in acne. Plastic surgery is required for rhinophyma.
Other disorders
Perioral dermatitis is characterized by papules and pustules that may occur around the mouth and chin of a woman who has used topical steroids. They will clear with steroid cessation and oral tetracycline therapy.
Hidradenitis suppurativa is an unpleasant chronic inflammatory condition of the infundibulum of hair follicles (p. 4) in the apocrine sweat gland areas of the axillae, groin and perineum. Nodules, abscesses, cysts and sinuses form and scarring results (p. 114). Treatment is with topical antiseptics, a prolonged course of a systemic antibiotic or retinoid, surgical excision or infliximab. Conglobate acne may coexist.
Hyperhidrosis (excess sweating) due to eccrine gland overactivity is usually emotional in origin. Twenty per cent aluminium chloride in alcohol is often effective. Iontophoresis is used for the hands (p. 23) and Botox injection for the axillae (p. 114).
Sebaceous and apocrine disorders
Acne
Due to increased sebum excretion, comedone formation, P. acnes and inflammation.
Presentation: comedones, pustules, cysts and scars seen over the face, chest and trunk.
Treatment: topical treatments include benzoyl peroxide and tretinoin; systemic treatments include antibiotics, e.g. tetracyclines or erythromycin, co-cyprindiol and isotretinoin.