Chapter 1 Concepts of health
Overview
Everyone engaged in the task of promoting health starts with a view of what health is. However, there is a wide variety of these views, or concepts, of health. It is important at the outset to be clear about the concepts of health which are personally adhered to, and to recognize where these differ from those of your colleagues and clients. Otherwise, you may find yourself drawn into conflicts about appropriate strategies and advice that are actually due to different ideas concerning the end goal of health. This chapter introduces different concepts of health and traces the origin of these views. The western scientific medical model of health is dominant but challenged by social and holistic models. Working your way through this chapter will enable you to clarify your own views on the definition of health and to locate these views in a conceptual framework.
Defining health, disease, illness and ill health
Health
Health is a broad concept which can embody a huge range of meanings, from the narrowly technical to the all-embracing moral or philosophical. The word ‘health’ is derived from the Old English word for heal (hael) which means ‘whole’, signalling that health concerns the whole person and his or her integrity, soundness or well-being. There are ‘common-sense’ views of health which are passed through generations as part of a common cultural heritage. These are termed ‘lay’ concepts of health, and everyone acquires a knowledge of them through their socialization into society. Different societies or different groups within one society have different views on what constitutes their ‘common sense’ about health.
 BOX 1.1
BOX 1.1Health has two common meanings in everyday use, one negative and one positive. The negative definition of health is the absence of disease or illness. This is the meaning of health within the western scientific medical model, which is explored in greater detail later on in this chapter. The positive definition of health is a state of well-being, interpreted by the World Health Organization in its constitution as ‘a state of complete physical, mental and social well-being, not merely the absence of disease or infirmity’ (World Health Organization 1946).
Health is holistic and includes different dimensions, each of which needs to be considered. Holistic health means taking account of the separate influences and interaction of these dimensions. Figure 1.1 shows a diagrammatic representation of the dimensions of health.
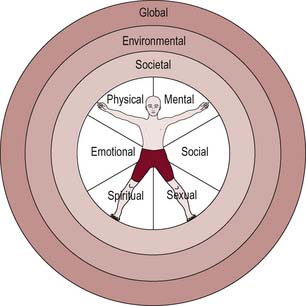
The inner circle represents individual dimensions of health.
The three outer circles are broader dimensions of health which affect the individual. Societal health refers to the link between health and the way a society is structured. This includes the basic infrastructure necessary for health (for example, shelter, peace, food, income), and the degree of integration or division within society. We shall see in Chapter 2 how the existence of patterned inequalities between groups of people harms health. Environmental health refers to the physical environment in which people live, and the importance of good-quality housing, transport, sanitation and pure water facilities and involves caring for the planet and ensuring its sustainability for the future.
 BOX 1.2
BOX 1.2Disease, illness and ill health
Disease, illness and ill health are often used interchangeably, although they have very different meanings. Disease derives from desaise, meaning uneasiness or discomfort. Nowadays, disease implies an objective state of ill health, which may be verified by accepted canons of proof. In our society, these accepted canons of proof are couched in the language of scientific medicine. For example, microscopic analysis may yield evidence of changes in cell structure, which may in turn lead to a diagnosis of cancer or disease. Disease is the existence of some pathology or abnormality of the body which is capable of detection. Disease can be due to exogenous (outside the body, e.g. viral infection) or endogenous (inside the body, e.g. inadequate thyroid function) factors. Health then is the normal functioning of the body as a biological entity.
Illness is the subjective experience of loss of health. This is couched in terms of symptoms, for example the reporting of aches or pains, or loss of function. One way that illness is given meaning is through the narratives we construct about how we fall sick. The process of making sense of illness is a task most sick people engage in to answer the question ‘why me?’ Illness and disease are not the same, although there is a large degree of coexistence. For example, someone may be diagnosed as having cancer through screening, even when there have been no reported symptoms. That is, a disease may be diagnosed in someone who has not reported any illness. When someone reports symptoms, and further investigations such as blood tests prove a disease process, the two concepts, disease and illness, coincide. In these instances, the term ill health is used. Ill health is therefore an umbrella term used to refer to the experience of disease plus illness. Health then is not being ill, the absence of symptoms.
Social scientists view health and disease as socially constructed entities. Health and disease are not states of objective reality waiting to be uncovered and investigated by scientific medicine. Rather, they are actively produced and negotiated by ordinary people. In Cornwell’s (1984) study of London’s Eastenders, they referred to three categories of health problems:
Illness has often been conceptualized as deviance – as different from the norm and a source of stigma. Goffman (1968) identifies three sources of stigma:
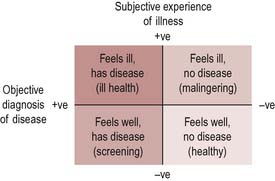
The subjective experience of feeling ill is not always matched by an objective diagnosis of disease. When this happens, doctors and health workers may label such sufferers ‘malingerers’, denying the validity of subjective illness. This can have important consequences, for example a sick certificate may be withheld if a doctor is not convinced that someone’s reported illness is genuine. The acceptance of a behaviour as an illness then becomes an issue of how to manage it. Several conditions, such as chronic fatigue syndrome and repetitive strain injury (RSI), have taken a long time to be recognized as illnesses.
Homosexuals, formerly considered to be sinners, were labelled as ill – not bad but mad. Commitments to mental institutions, hormonal treatments, and castrations were used to deal with unwanted sexual behaviour…. treatments for homosexual men – such as aversion therapy – continued until, and beyond, 1973, when the American Psychiatric Association redesigned homosexuality as non-pathological (Hart & Wellings 2002).
Can you think of other examples of a condition or behaviour where its medicalization has led to its acceptance or otherwise?
It is also possible to experience no symptoms or signs of disease, but to be labelled sick as a result of examination or screening. Hypertension and precancerous changes to cell structures are two examples where screening may identify a disease even though the person concerned may feel perfectly healthy. Figure 1.2 gives a visual representation of these discrepancies. The central point is that subjective perceptions cannot be overruled, or invalidated, by scientific medicine.
The western scientific medical model of health
In modern western societies, and in many other societies as well, the dominant professional view of health adopted by most health care workers during their training and practice is labelled western scientific medicine. Western scientific medicine operates within a medical model of explanation using a narrow view of health, which is often used to refer to no disease or no illness. In this sense, health is a negative term, defined more by what it is not than by what it is.
This view of health is extremely influential, as it underpins much of the training and ethos of a wide variety of health workers. These definitions become powerful because they are used in a variety of contexts, not just in professional circles. For example, the media often present this view of health, disease and illness in dramas set in hospitals or in documentaries about health issues. By these means, professional definitions become known and accepted in society at large.
The scientific medical model arose in western Europe at the time of the Enlightenment, with the rise of rationality and science as forms of knowledge. In earlier times, religion provided a way of knowing and understanding the world. The Enlightenment changed the old order, and substituted science for religion as the dominant means of knowledge and understanding. This was accompanied by a proliferation of equipment and techniques for studying the world. The invention of the microscope and telescope revealed whole worlds which had previously been invisible. Observation, calculation and classification became the means of increasing knowledge. Such knowledge was put to practical purposes, and applied science was one of the forces which accompanied the Industrial Revolution. In an atmosphere when everything was deemed knowable through the proper application of scientific method, the human body became a key object for the pursuit of scientific knowledge. What could be seen, and measured, and catalogued, was ‘true’ in an objective and universal sense.
This view of health is characterized as:
Health is predominantly viewed as the absence of disease. This view sees health and disease as linked, as if on a continuum, so that the more disease a person has, the further away he or she is from health and ‘normality’.
The pathogenic focus on finding the causes for ill health has led to an emphasis on risk factors. Antonovsky (1993) has called for a salutogenic approach which looks instead at why some people remain healthy. He identifies coping mechanisms which enable some people to remain healthy despite adverse circumstances, change and stress. An important factor for health, which Antonovsky labels a ‘sense of coherence’, involves the three aspects of understanding, managing and making sense of change. These are human abilities which are in turn nurtured or obstructed by the wider environment.
The medical model focuses on aetiology and the belief that disease originates from specific and identifiable causes. The causes of contemporary long-term chronic diseases in developed countries are often ‘social’. Medicine and medical practice thus recognize that disease and the diseased body must be placed in a social context. Nevertheless the professional training of many health care workers provides an exaggerated view of the benefits of treatment and pays little attention to prevention. In part this is due to the dominant concern of the biomedical model with the organic appearance of disease and malfunction as the cause of ill-health.
John is 19 and cannot go to the local college because he uses a wheelchair. He is given a place at a day centre because it is thought that this will suit his needs better.
Table 1.1 contrasts the traditional views of a medical model with that of a social model of health.
Table 1.1 The medical and social model of health
| Medical model | Social model |
|---|---|
| Health is the absence of disease | Health is a product of social, biological and environmental factors |
| Health services are geared towards treating the sick and disabled | Services emphasize all stages of prevention and treatment |
| High value is placed on specialist medical services | Less emphasis is placed on the role of specialists – there is more attention to self-help and community activity |
| Health workers diagnose and treat and sanction ‘the sick role’ | Health workers enable people to take greater control over their own health |
| The pathogenic focus emphasizes finding biological cause | A salutogenic focus emphasizes understanding why people are healthy |
A critique of the medical model
The role of medicine in determining health
The view that health is the absence of disease and illness, and that medical treatment can restore the body to good health, has been criticized. The distribution of health and ill health has been analysed from a historical and social science perspective. It has been argued that medicine is not as effective as is often claimed. The medical writer, Thomas McKeown, showed that most of the fatal diseases of the 19th century had disappeared before the arrival of antibiotics or immunization programmes. He concluded that social advances in general living conditions, such as improved sanitation and better nutrition made available by rising real wages, have been responsible for most of the reduction in mortality achieved during the last century. Although his thesis has been disputed, there is little disagreement that the contribution of medicine to reduced mortality has been minor, when compared with the major impact of improved environmental conditions.
The rise of the evidence-based practice movement (see Chapter 20) is attributed to Archie Cochrane (1972). His concern was that medical interventions were not trialled to demonstrate effectiveness prior to their widespread adoption. Rather, many procedures rest on habit, custom and tradition rather than rationality. Cochrane advocated greater use of the randomized controlled trial as a means to scientific knowledge and the key to progress.
The role of social factors in determining health
The modern UK is characterized by profound inequalities in income and wealth and these in turn are associated with persistent inequalities in health (Shaw et al 1999). The impact of scientific medicine on health is marginal when compared to major structural features such as the distribution of wealth, income, housing and employment. Tarlov (1996) has claimed that medical services contributed only 17% to the gain in life expectancy in the 20th century. As Chapter 2 will show, the distribution of health mirrors the distribution of material resources within society. In general, the more equal a society is in its distribution of resources, the more equal, and better, is the health status of its citizens (Wilkinson 1996).
Medicine as a means of social control
Social scientists argue that medicine is a social enterprise closely linked with the exercise of professional power (Stacey 1988). This derives from its role in legitimizing health and illness in society and the socially exclusive and autonomous nature of the profession. Medicine is a powerful means of social control, whereby the categories of disease, illness, madness and deviancy are used to maintain a status quo in society. Doctors who make the diagnosis are in a powerful position. The role of the patient during sickness as conceptualized by Parsons (1951) is illustrated in Table 1.2.
| Rights | Responsibilities |
|---|---|
| Patient is relieved of normal responsibilities and tasks | Patient must want to recover as soon as possible and only then can he or she be seen as ‘sick’ |
| Patient is given sympathy and support | Patient must seek professional advice and comply with treatment |
| Patient has the right to a diagnosis, examination and treatment |
Increasingly, too, doctors are involved in decisions relating to the beginning and ending of life (terminations, assisted reproduction, neonatal care). The encroachment of medical decisions into these stages of life subverts human autonomy and gives to medicine an authority beyond its legitimate area of operation (Illich 1975).
The medical profession has long been regarded as an institution for securing occupational and social authority. Access to such power is controlled by professional associations that have their own vested interests to protect (Freidson 1986). The 1858 Medical Act established the General Medical Council which was authorized to regulate doctors, oversee medical education and keep a register of qualified practitioners. The Faculty of Public Health Medicine opened membership to non-medically qualified specialists in 2003, becoming the Faculty of Public Health.
The following is a list of labels which are attached to people at certain stages of their life. Some are universal (everyone is born and dies); others only happen to some people at some stages of their lives. For each label identify:
Medicine as surveillance
Public health medicine has been concerned with the regulation and control of disease. Historically this may have included the containment of bodies, whether those infected with plague, tuberculosis or venereal disease. Mass screening programmes have given rise to what has been called medical surveillance. The wish to identify the ‘abnormal’ few with ‘invisible’ disease justifies monitoring the entire target population. Another critique of the pervasive power of medicine suggests the mapping of disease and identification of risk have subtly handed responsibility of health to individuals. This may invite new forms of control in the name of health, e.g. random drug testing or linking deservedness of surgery to lifestyle factors (Bunton et al 1995). The ability to identify risk also means there can be a moral discourse in which reducing one’s risk factors are seen as a good thing, e.g. eating ‘sensibly,’ living ‘well.’
Medicine as harm
According to Illich (1975), doctors and health workers contribute to ill health and create harm (iatrogenesis):
Challenges to medicine
The dominance of medicine has been challenged in recent years by:
These trends are related to wider forces that challenge the expertise of professionals. The response of most professions including medicine has been to introduce democratic decision-making, giving far more credence to lay knowledge. This has led to new concepts such as the ‘expert patient’.
Lay concepts of health
For people concerned with the promotion of health, there is another problem with the dominance of scientific medicine. This is the focus within medicine on illness and disease, and the neglect of health as a positive concept in its own right. Many researchers have studied the general public’s beliefs about health or lay concepts of health. The findings present an interesting picture, where there are continuities in definitions but also differences attributable to age, sex and class.
Blaxter (1990) identified five common concepts of health:
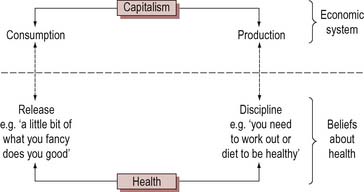
The concepts of ‘control’ and ‘release’ are also commonly found in lay accounts – release is the taking of known risks (e.g. binge drinking) whereas control is the management of health. As illustrated in Figure 1.3 Crawford (2000) suggests that capitalism also requires individuals to be healthy consumers, having fun and seeking immediate gratification. Adherence to healthy lifestyles has to be offset by pleasure or release. In capitalist societies we are encouraged to be disciplined and controlled about pleasures such as alcohol. This is couched as being balanced and moderate.
Researchers have found these issues of control and release in many accounts of health together with a moral view about taking risks. The following extract is from a study of lay men’s views:
I eat healthy food generally and I cheat now and again. Alcohol is bad for you, but we all drink. Mostly everyone I know likes a drink ‘cause its good for you, it actually cheers you up … we’ve got like this throwaway society and I think people’s perceptions are changing, everybody wants everything yesterday … and that’s it, get fit one day, get drunk the next (Robertson 2006, p. 179).
There is often a difference between lay and professional concepts of health. The gap between the two has been identified by health workers as a problem, giving rise to concern. The concern centres around two issues: (1) the perceived lack of communication or poor communication between health worker and client; and (2) clients’ lack of compliance with prescribed treatment regimes. However, there is also a cross-over between lay and professional beliefs about health. Health workers acquire their professional view of health during training. These beliefs overlie their original views of health adopted at an early age from family and society, so professionals are familiar with both. The general public is also aware of, and operates with, both sets of beliefs. In searching for meaning, lay patients frequently adopt professionals’ explanations and interpretations about health and illness. So the two sets of beliefs, scientific medicine and lay public, are not discrete entities but overlap each other and exist in tandem.
Cornwell (1984) describes how people operate with both official and lay beliefs about health. Cornwell’s study of London’s Eastenders found that accounts of health were either public or private. Public accounts are couched in terms of scientific medicine and reflect these dominant beliefs. Health and illness are related to medical diagnosis and treatment, and medical terms and events are used to explain health status. These public accounts were offered first in Cornwell’s interviews. What Cornwell terms private accounts reflect lay views of health, which typically use more holistic and social concepts to explain health and illness. For example, private accounts related health to general life experiences, such as employment, housing and perceived stress. Private accounts were offered in subsequent interviews, when a relationship had been established between Cornwell and the women she was interviewing. Cornwell suggests that people are therefore aware of both systems of beliefs and can use either when asked to talk about health. In encounters with strangers who are perceived as professionals, people use public accounts. However, in more informal settings, people use private accounts.
Cultural views of health
We are able to think about health using the language of scientific medicine because that is part of our cultural heritage. We do so as a matter of course, and think it is self-evident or common sense. However, other societies and cultures have their own common-sense ways of talking about health which are very different. Many cultures view disease as the outcome of malign human or supernatural agencies, and diagnosis is a matter of determining who has been offended. Treatment includes ceremonies to propitiate these spirits as an integral part of the process. Ways of thinking about health and disease reflect the basic preoccupations of society, and dominant views of society and the world. Anthropologists refer to this phenomenon as the cultural specificity of notions of health and disease.
 BOX 1.13
BOX 1.13The Gnau of New Guinea refer to illness and other general misfortunes by the same word, wala. They also use the pidgin English sik to refer to bodily misfortunes. Sickness is a particular type of misfortune which is caused by evil beings or by magic and sorcery. People who are sick act in certain ways (shunning certain foods, eating alone) which oblige others to find out and treat the illness (Lewis 1986).
In any multicultural society such as the UK, a variety of cultural views coexist at any one time. For example, traditional Chinese medicine is based on the dichotomy of yin and yang, female and male, hot and cold, which is applied to symptoms, diet and treatments, such as acupuncture and Chinese herbal medicine. Complementary therapists offer therapies based on these cultural views of health and disease alongside (or increasingly within) the National Health Service, which is based on scientific medicine.
A unified view of health
Is there any unifying concept of health which can reconcile these different views and beliefs? Attempts at such a synthesis have come from philosophers such as Seedhouse (1986) and from organizations concerned with health, such as the World Health Organization.
Figure 1.4 shows four theories of health:
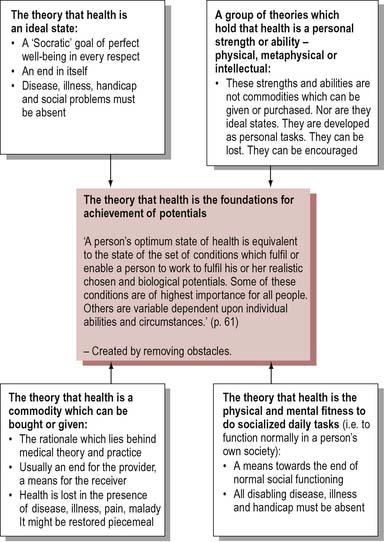
Seedhouse suggests that these four views can be combined in a unified theory of health as the foundation for human achievement. Health is thus a means to an end rather than a fixed state to which a person should aspire.
[Health is] the extent to which an individual or group is able, on the one hand, to realize aspirations and satisfy needs; and, on the other hand, to change or cope with the environment. Health is, therefore, seen as a resource for everyday life, not an object of living; it is a positive concept emphasising social and personal resources, as well as physical capacities (World Health Organization 1984).
Provided certain central conditions are met, people can be enabled to achieve their potential. The task of practitioners working for health is to create these conditions for people to achieve health:
This definition acknowledges that people have different starting points which set limits for their potential for health. It encompasses a positive notion of health which is applicable to everyone, whatever their circumstances. However, it could be argued that this definition does not acknowledge the social construction of health sufficiently. People as individuals have little scope to determine optimum conditions for realizing their potential.
By health I mean the power to live a full, adult, living, breathing life in close contact with what I love … I want to be all that I am capable of becoming (Mansfield 1977, p. 278).
The view of health as personal potential is attractive because it is so flexible, but this very flexibility causes problems. It leads to relativism (health may mean a thousand different things to a thousand different people), which makes it impracticable as a working definition for health promoters.
Health is regarded by the World Health Organization as a fundamental human right and there are certain prerequisites for health which include peace, adequate food and shelter and sustainable resource use.
Looking at health this way establishes it as a social as well as an individual product, and it emphasizes the dynamic and positive nature of health. Health is viewed as both a fundamental human right and a sound social investment. This view has been publicly affirmed by the Jakarta Declaration which linked health to social and economic development (World Health Organization 1997). This definition provides a variety of reasons for supporting health, which are likely to meet the concerns of a range of groups. It establishes a broad consensus for prioritizing health, and legitimizes a range of activities designed to promote health. For example, in addition to the more acceptable strategies of primary health care and personal skills development, the World Health Organization also identified in the Ottawa Charter the more radical strategies of community participation and healthy public policy as essential to the promotion of health (World Health Organization 1986). However, it could still be argued that such a broad definition makes it difficult to identify practical priorities for health promotion activities.
There is no agreement on what is meant by health. Health is used in many different contexts to refer to many different aspects of life. Given this complexity of meanings, it is unlikely that a unified concept of health which includes all its meanings will be formulated.
Conclusion
There are no rights and wrongs regarding concepts of health. Different people are likely to hold different views of health and may operate with several conflicting views simultaneously. Where people are located socially, in terms of social class, gender, ethnic origin and occupation, will affect their concept of health. The medical model has, however, dominated western thinking about health. Yet its value for health promotion is limited:
There is such a range of meaning attached to the notion of health that in any particular situation, it is important to find out what views are in operation. Clarifying what you understand about health, and what other people mean when they talk about health, is an essential first step for the health promoter.