Chapter 14 Health promotion in the workplace
Overview
The workplace is significant both in affecting people’s health and as a context in which to promote health. Employment rates in the UK have been rising. Statistics for the last quarter of 2007 show that 74.7% of people of working age, or 29.4 million people, were employed (www.statistics.gov.uk). Promoting health in the workplace will therefore reach a large percentage of the adult population, and will have an impact on a setting where many adults spend a considerable amount of their time.
This chapter looks at the workplace as a social system and ways in which it can contribute to ill health and health. It goes on to look at ways in which health promotion has been implemented in the workplace. Most health promotion interventions have tended to focus on individual lifestyle risk factors and employers’ legal responsibilities to provide a safe working environment. Interventions that address the workplace organization and culture as a whole are less common, but evaluation shows they are more effective. The different partners and stakeholders involved in workplace health promotion are identified and their contribution to interventions discussed.
Why is the workplace a key setting for health promotion?
There are four main reasons for prioritizing the workplace. First, the workplace gives access to a target group, healthy adults, especially men, who are often difficult to reach in other ways. Recent projections suggest that by 2020 32.1 million people will be economically active (Madouros 2006), which represents an increase of 6.7% from 2005. Employees in the workplace are a captive audience for health promotion. It is easy to follow up interventions and encourage participation in health programmes because there are established modes of communication. The cohesion of the working community also provides peer pressure and support. The second reason for promoting health in the workplace is to ensure that people are protected from the harm to their health that certain jobs may cause.
 BOX 14.1
BOX 14.1Work-related ill health – U.K. statistics for the year 2006–2007
241 workers were killed at work (an 11% increase on 2005–2006)
141,350 employees suffered serious injuries at work
2.2 million people were suffering from an illness they believed was caused or made worse by their work. Of these, 646,000 were new cases in the last 12 months
36 million days were lost overall (1.5 days per worker), with 30 million due to work-related ill health and 6 million due to workplace injury (Health and Safety Executive (HSE) 2007).
Thirdly, there are economic benefits associated with healthy workplaces (Wanless 2004). American research studies provide evidence that workplace health promotion programmes are associated with lower medical and insurance costs, decreased absenteeism and enhanced performance, productivity and morale (www.uclan.ac.uk/facs/health/hsdu/settings/workplace/htm). The cost of sick leave and incapacity benefit averaged £476 per worker in 2002 (Dooris & Hunter 2007). Research has shown that employees who have three or more risk factors (e.g. smoking, overweight, excessive alcohol intake, physical inactivity) are likely to have 50% more sickness absence from work than employees with no risk factors (Shain & Kramer 2004). Investing in health and preventing ill health increase productivity and staff retention. The average cost–benefit ratio for a variety of health promotion programmes operated by large American companies is significant – just over a fourfold return on each dollar invested (Shain & Kramer 2004). Adopting a healthy workplaces approach therefore makes sound business sense.
Economic benefits of workplace health promotion programmes
Many evaluation studies of workplace health promotion programmes have reported positive results, including the following:
Fourthly, the workplace provides a resource for health that is relevant to a large percentage of the adult population. Creating a healthy environment at work will benefit employees’ health and have positive spin-offs for their families and communities. The traditional focus on the workplace has centred on hazards and illnesses, but a health-promoting approach to the workplace has great potential.
The relationship between work and health
The relationship between work and health is complex. In general, attention has focused on the effects of work on health, although it is also acknowledged that poor health will have negative effects on the capacity for paid employment. There is evidence that paid work is good for your health and unemployment can be linked to ill health (Waddell & Burton 2006). Work is beneficial for health because it provides an income, a sense of self-worth and social networks of colleagues and friends. However, work may also harm health, and most research has concentrated on this aspect of the relationship.
 BOX 14.3
BOX 14.3The workplace can affect health in many different ways. Figure 14.1 provides a means of classifying these different kinds of relationship.
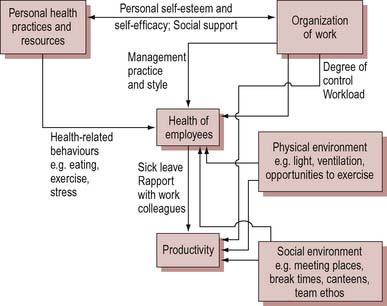
Figure 14.1 The relationship between health and productivity in the workplace. From Shain & Kramer (2004).
 BOX 14.4
BOX 14.4Hazards tend to be what people think of first when health in the workplace is mentioned. Most legislation is directed towards the containment of hazards, and safety legislation has been enshrined in numerous Factory Acts since the mid 19th century. Work that involves handling hazardous or toxic materials may have a direct negative effect on health (e.g. cancers caused by asbestos or occupational asthma). Work which provides easy access to hazardous substances is also linked to associated ill health. For example, doctors and pharmacists have high rates of suicide associated with drug overdose. In 2000 the government set out, for the first time, overarching targets for significant improvements in workplace health and safety. The statistics for workplace deaths and injuries for 2006–2007 are mixed (HSE 2007; Health and Safety Commission 2007). Overall there has been progress in major injury reduction, but an increase in workplace deaths. Almost one-third of deaths occur in the construction sector, with agriculture, waste and recycling industries also implicated.
The workplace is characterized by fragmented information which is collected by different bodies (including the HSE and occupational health services). This poses obvious difficulties when trying to plan and implement a health promotion intervention. Health is often affected through risky behaviour or changed routines. Risky behaviour is the preferred explanation for most official accounts of accidents and injuries sustained in the workplace. There are extensive regulations to cover manual handling (Manual Handling Operations Regulations, amended in 2002) which require employers to provide training and equipment. Nevertheless, employees are expected to ‘take reasonable care for the health and safety of themselves and any others who may be affected by their acts and omissions’. This approach extends to the workplace the victim-blaming ideology of some brands of health promotion. Behaviour which carries health risks may be an integral part of the job or part of the work culture. For example, bartenders have high rates of alcohol-related ill health because drinking heavily is associated with work (Wilhelm et al. 2004).
The general work environment and its effects on health are the most neglected aspects of the work–health relationship. This is due in part to ideological or political reasons, and in part to the fact that such a generalized relationship is hard to research or prove. Because the relationship between work and health is to a large extent indirect, it is often difficult to trace ill health to what happens in the workplace. This in turn leads to the true impact on health from work being underestimated. Focusing on the work environment instead of individual workers’ behaviour shifts responsibility on to the employer and has resource implications.
Although the relationship is difficult to quantify, strong evidence implicating the importance to health of the general work environment is becoming available (Marmot & Wilkinson 2006). There is a body of research demonstrating that certain factors associated with some types of work, such as repetitive tasks, lack of autonomy and pressures to meet deadlines, have harmful effects on health. In particular, low control by workers over what they do and how they do it is associated with increased risk of ill health (Wilkinson 2006). Long-term exposure to stress results in poor health and may also lead to less healthy lifestyle choices, such as smoking. There is a growing acknowledgement of the impact of workplace stress on health:
In response to this situation, the HSE (2005) has produced management standards to support employers who wish to tackle this issue.
Stress in the workplace
A focus on individual stress can be counterproductive, leading to a failure to tackle the underlying causes of problems in the workplace. Evidence has shown that poor working arrangements, such as lack of job control or discretion, consistently high work demands and low social support, can lead to increased risks of CHD [coronary heart disease], musculoskeletal disorders, mental illness and sickness absence. The real task is to improve the quality of jobs by reducing monotony, increasing job control, and applying appropriate HR [human resources] practices and policies – organisations need to ensure they adopt approaches that support the overall health and well being of their employees (Department of Health 2004, Chapter 7 para 16).
There are two main ways in which workplace stress is being addressed. The traditional approach has been to see the individual as unable to cope with the demands and pressures and therefore in need of support. Many large workplaces offer stress management courses, counselling services and employee assistance programmes to help people adjust to new skills.
Organizational approaches to stress are still rare despite a growing literature linking stress with organizational factors, such as lack of control or lack of consultation over changes. These approaches start from the view that illness and stressed behaviour are responses to factors in the workplace, and of which individuals may not even be aware.
Task and work reorganization is the most successful form of intervention. It describes various system solutions to improve communication, the creation of autonomous work groups and whole-organization interventions to restructure relations between management and unions. These interventions do not obviate the need for individual support, but follow an earlier stage of raising staff awareness of stress and its causes.
Responsibility for workplace health
The relationship between work and health may appear substantial but it is viewed in different ways by different groups of people. One of the defining characteristics of the workplace setting is that it brings together a variety of groups who have different agendas with regard to work and health. The key parties are workers or employees and their trade unions or staff associations, employers and managers, occupational health staff, health and safety officers, public health specialists and environmental health officers.
Workers
It has always been a priority for workers’ organizations to ensure that employees are working in safe and healthy conditions. Membership of trade unions has, however, declined since the mid-1970s, when membership was just under two-fifths, to just over a quarter in 2006 (Department of Trade and Industry 2007). Changing patterns of employment also mean that part-time (mainly female) workers make up a significant percentage of the working population. So, although consultation with unions is an important means of reaching workers, it does not reach everyone. As the key target group, workers need to be fully involved as partners in decision-making processes. This is recognized by the European Network for Workplace Health Promotion (ENWHP), who state that effective workplace health promotion involves employees in decision-making processes and develops a working culture based on partnership (www.enwhp.org).
Employers and managers
Employers and managers have as their first priority the viability of the organization. Health is relevant in so far as it can be shown to be linked to organizational goals. Examples of ‘hard’ benefits are improvements in productivity due to lower rates of sickness, absenteeism and staff turnover, and improved recruitment and retention of trained staff. ‘Soft’ benefits, such as enhanced corporate image, are also influential.
Employers are responsible for the health, safety and welfare of all their employees under the Health and Safety at Work Act (1974). There is evidence of a shift in attitudes and awareness of health and safety issues in the workplace. A recent survey (Elgood et al 2004) found that between two-thirds and three-quarters of employees felt that employers take their responsibilities seriously. There was a high level of awareness and understanding about the HSE and its role, although this was less true within smaller organizations. The Investors in People standard is an example of the government’s strategy to use awards to provide incentives for employers, and has been widely adopted. The Improving Working Lives standard is another example that sets a model of good human resources practice against which National Health Service employers can be measured. Leadership and commitment at senior management level have been shown to be vital for effective health promotion initiatives and the creation of healthy workplaces (Faculty of Public Health and Faculty of Occupational Medicine 2006).
Occupational health staff
In many European countries occupational health is a statutory part of health care. In the UK there is no requirement for employers to provide an occupational health service, other than first aid. A recent survey (Institute of Occupational Medicine 2002) found that only 15% of all British firms provided basic occupational health support, and only 3% offered comprehensive support. Occupational health nurses (OHNs), who are specialist nurses with postqualification training, form an important element of the occupational health staff. OHNs are responsible for the health and well-being of employees in the workplace.
The main functions of an occupational health service are:
The workplace has experienced considerable change and uncertainty in the last 20 years. There has been a rapid growth in the service sector, a fragmentation of large organizations and a huge increase in information technology. The provision for health in companies thus needs to be seen alongside policies on employment, the work environment and overall company policy.
Health and Safety Officers and Environmental Health Officers
Health and safety officers and environmental health officers are responsible for ensuring that workplaces conform with safety legislation. They have powers to force workplaces to comply with health and safety regulations, and to impose penalties in the case of non-compliance. Responsibility for workplaces is divided between the HSE and environmental health officers employed by local authorities. There is now a developed body of European Union (EU) occupational health and safety legislation.
Lighten the Load
The European Agency for Safety and Health at Work has organized the Lighten the Load campaign to promote an integrated approach to tackling musculoskeletal disorders (MSDs). MSDs are the most common form of work-related illness in Europe. In the EU 25% of workers suffer from backache and 23% from muscular pains. Nine organizations won good-practice awards in 2008. Winning projects included:
A recent consultation paper (Department of Trade and Industry 2007) documented the valuable role played by workplace safety representatives. Safety representatives prevent 8000–13 000 injuries and 3000–8000 work-related illnesses annually. The annual savings to industry and society as a whole are estimated as £578 million per year (at 2004 prices). Yet safety representatives are not universal. Only 46% of workplaces (92% of public sector and 39% of private sector) and 68% of employees (98% of public sector and 59% of private sector) are covered by employee representation.
Health promotion in the workplace
Several policy initiatives target the workplace as a setting for health promotion, e.g. the government’s public health White Paper Choosing Health: Making Healthy Choices Easier Choices (Department of Health 2004) and Health, Work and Wellbeing – Caring for our Future (Department of Work and Pensions 2005). There are two approaches to health promotion in the workplace. The most common approach is to target individual lifestyles and behaviour within a workplace setting. This approach sees the workplace primarily as a site through which programmes can be delivered. The more challenging, but potentially more effective, approach is to target the workplace and its organization and culture. Health promotion in the workplace falls into the following categories:
Examples of healthy workplace initiatives
There is widespread acceptance of the requirement to provide safe working conditions. Health promotion programmes in the workplace are still not widespread and are more likely in large workplaces. Programmes include smoking cessation, alcohol counselling, weight management, exercise and fitness interventions, general health screening and stress management courses.
A ban on smoking in all workplaces was introduced in England in 2007. Is legislation the most appropriate means to a healthy setting?
There is evidence that health promotion targeting the whole organization is more effective than targeting individual lifestyles (Noblet & LaMontagne 2006). Changing organizational culture and practice, through more flexible working hours and break times, for example, has a more significant impact than programmes that assume individuals can make the necessary changes themselves, e.g. offering relaxation classes after working hours.
Workplace health promotion
The Director of Public Health and the Bristol North Primary Care Team worked collaboratively to introduce measures designed to help their staff cycle to work, and thereby embed physical activity in their daily routines. Measures included:
Within 1 year the number of employees cycling to work doubled, from 5% to 10% (Faculty of Public Health and Faculty of Occupational Medicine 2006).
The whole-organization approach has been recognized and endorsed at the highest level and by international bodies. For example, the ENWHP adopted the Luxembourg Declaration on Workplace Health Promotion in 1997. The Declaration states that successful initiatives should follow these guidelines:
In order to maximize the impact of workplace health promotion, the approach needs to shift from an exclusively individually focused lifestyle approach to a more comprehensive approach that includes whole-organization activities as well.
The evidence of effective health promotion interventions in the workplace is building, although it remains rather scanty. The Department of Health (2004) has called for more rigorous evaluation of initiatives. A review of work-based health promotion programmes concluded that they have a positive impact, with a variety of risk factors including smoking being reduced amongst programme participants (Kreis & Bodeker 2004, cited in Department of Work and Pensions 2005).
Conclusion
The workplace is recognized as a key setting in which to promote health, due to both its reach (three-quarters of the working-age population are employed) and its importance in contributing directly and indirectly to people’s health. Traditionally the focus has been on individually targeted programmes centred on hazards and the prevention of ill health. The challenge today is to broaden the focus to include the whole organizational setting and to move from ill health to positive health and well-being. There is a developing evidence base that demonstrates that such a comprehensive and multicomponent approach is effective. The proven benefits include not just better employee health, but also increased productivity and economic benefits to industry and society as a whole. Many different groups have a role to play in promoting health in the workplace, including workers, managers, employers, occupational health staff, health and safety officers and environmental health officers.