Chapter 7 The politics of health promotion
Overview
Politics and health promotion are often thought of as separate activities. However, different approaches to health promotion reflect different political positions. This chapter outlines the diversity of social and political philosophies, which helps us to understand how health promotion has developed in the social and political context of the late 20th and early 21st centuries. Understanding our own values helps us to see the logical consequences for health promotion. The political dimensions of health promotion in relation to its organization, its methods and the content of health promotion activity are then explored.
What is politics?
Heywood (2000) identifies a fourfold classification of politics:
Although these are separate concepts, they are arguably united by the fourth definition – politics as power – that is the main focus of this chapter. In democratic countries, people use their vote to give power to the political party of their choice. The elected party then governs public life and thus wields power on behalf of the populace. Power includes not only material or physical resources, but also psychological and cultural aspects, which may be equally effective in limiting or channelling people.
Power is distributed unequally worldwide, and globalization has contributed to increasing the divide between high-income regions, e.g. Europe, the USA and Canada, and low-income regions e.g. in sub-Saharan Africa. More than 10 million children under the age of 5 die each year, almost all in poor countries or poor areas of middle-income countries (Jones et al 2003). Over half of these deaths are caused by undernutrition and lack of access to safe water and sanitation (Labonte & Schrecker 2007).
Political ideologies
One of the arenas in which power relationships are manifest is social policy, which may be defined as planned government activities designed to maintain, integrate and regulate society. This includes both welfare and economic policies, ranging from national legislation to local policy developments within local authorities. (See Chapter 11 for a discussion of Developing Healthy public policy.)
Government policies are determined according to its beliefs and ideas – its ideological position. Different political positions give rise to certain types of policy interventions. Analysts have identified many different frameworks and have pointed to the shift in ideologies since the 1960s (Bambra et al 2008). The old mid 20th-century spectrum of political belief from the hard-line left (Marxism) via Socialism and Liberalism to the right wing (Conservatism) no longer describes accurately the political beliefs and ideologies of nations and parties. Globalization, the demise of Soviet rule over Eastern Europe, and the permeation of nation boundaries through international trade and the forces of nature have given rise to new political beliefs, in particular, the rise of neoliberalism and neoconservatism. These changes are summarized in Table 7.1.
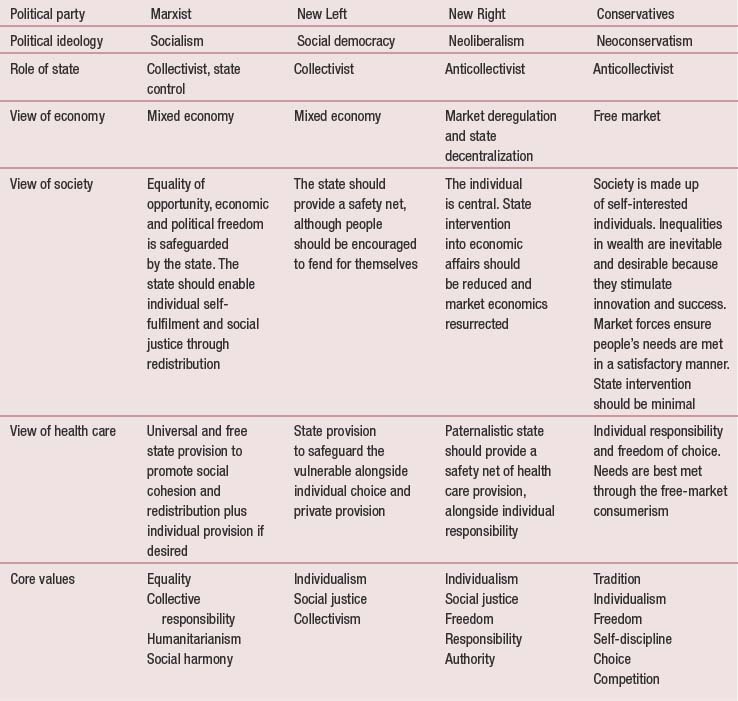
Views on health and health promotion reflect a complex mix of values and beliefs which, in turn, reflect different political ideologies. The central proposition of this chapter is that health, and therefore health promotion, is political. Health promotion takes place in the policy area and embodies ideological values. Ideology is ‘a system of interrelated ideas and concepts that reflect and promote the political economic and cultural values and interests of a particular societal group’ (Bambra et al 2003, p. 18). The ideological viewpoints of different political parties vary widely. Key beliefs in relation to promoting health on which people differ concern:
On the right of the political spectrum there is a belief in individual self-determination and an antipathy to government intervention which not only restricts freedom but also inhibits enterprise. Conservatism sees inequality as inevitable and beneficial, in that differences stimulate people to succeed, resulting in innovation and productivity. Neoconservatism stresses the need to restore traditional values and a shared culture.
Neoliberalism has evolved since the 1960s as an attempt to combine the twin goals of social justice and economic growth. Neoliberalism is committed towards reducing state intervention in the economy and advocates market deregulation as the means to economic growth and social welfare. Such views are associated with the rugged individualism of Margaret Thatcher who famously asserted: ‘there is no such thing as society, only individuals and their families’.
Socialism is based on a belief in equality, fellowship and community, or a sense of responsibility for others. The government has a key role to play in ensuring everyone’s basic needs are met, redistributing material resources and promoting a sense of social stability and cohesion. Social democracy, whilst embodying the same core beliefs, also embraces the notion of individual choice within a free market.
 BOX 7.1
BOX 7.1In the modern UK, the Labour government elected in 1997 was committed to a ‘third way’ distinct from both liberal capitalism and democratic socialism. The third way was described by the then Prime Minister Blair as ‘rooted in our enduring values of fairness, justice, the equal worth and dignity of all’.
Consider the social policy interventions referred to in these newspaper headlines about particular government policies. What values are being reflected?
At the same time the 1997 election manifesto rejected values and ideology in favour of pragmatism and ‘what works’. It is against this background that recent interventions should be viewed as:
Globalization
Globalization, defined primarily as the economic processes of free trade supporting a global marketplace, is another reason for the shifting positions of political parties. No political party can ignore the immense power of global capitalism, which reaches across the world, ignoring national or regional boundaries. McDonalds, Microsoft and Philip Morris are known worldwide for promotingjunk food, internet communication and tobacco respectively. Proponents of globalization argue it is more efficient and allows poorer countries to benefit from the technological advances of more developed countries. Critics of globalization argue that it destabilizes national economies, reduces everything to a market value and increases inequalities of wealth and health. It has been argued that the socioeconomic determinants of health have become globalized, leading to increased inequalities between rich and poor countries as well as within countries (Labonte & Schrecker 2007). Whatever the stance adopted, health promotion needs to develop and function within an increasingly global economy and world.
Globalization in politics is mirrored by globalization in health. Health risks are now increasingly global in their scope and spread, fuelled by the displacement of people (through war and natural disasters), global trade and movement of people and products. For example, the spread of human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome (AIDS) and severe acute respiratory syndrome (SARS) requires continued vigilance and concerted action by nations and international agencies (Kickbusch & Seck 2007).
There are many important challenges to health and health promotion posed by globalization. Lee (2003) identifies the following:
Equally, globalization opens up new possibilities – of networking, learning from others’ experience and sharing of resources – that could be used positively to promote and protect health. The World Health Organization (WHO) Commission on Macroeconomics and Health in 2001 made the case for a reciprocal relationship between health and development, arguing that not only is development vital for health, but health is vital for development. The political challenge for health promotion is to foreground health as a valued goal and a key component of the global public good.
Health as political
In the WHO Alma Ata declaration (World Health Organization 1978) health was seen as both a human right and a global social issue. The Universal Declaration of Human Rights adopted by the United Nations in 1948 proclaimed that ‘everyone has the right to a standard of living adequate for the health and well-being of oneself and one’s family, including food, clothing, housing, and medical care.’ Economic globalization has threatened these views of health as a human right. The People’s Health Movement (www.phmovement.org) is a group of political activists and advocates opposed to globalization. This group argues that it is health, not the economy, that should be prioritized.
Within nation states, the political context affects all areas of government policy that have an impact on health, both directly and indirectly. Bambra et al (2003) argue that health is political because power is exercised over it and its correlates (such as citizenship and organization). A recent WHO report (Wilkinson & Marmot 2003) identified 10 social determinants of health: social class gradient, stress, early life, social exclusion, work, unemployment, social support, addiction, food and transport. Evidence suggests that these social determinants of health are the best predictors of individual and population health, that they structure lifestyle choices and that they interact to produce health (Raphael 2003). This in turn leads to the notion of health as political and the outcome of national and international policy decisions. A strong welfare state that provides people with access to the social determinants of health is arguably the best means to promote health (Raphael & Bryant 2006).
 BOX 7.2
BOX 7.2The politics of health promotion structures and organization
Internationally and nationally health promotion has enjoyed varying levels of support throughout the 20th and 21st centuries. The first International Conference on Health Promotion in 1986 led to the adoption of the Ottawa Charter for Health Promotion (WHO 1986) whose five action areas (building a healthy public policy, creating supportive environments, developing personal skills, strengthening communities and reorienting health services) are still used widely. This was followed by conferences in Adelaide (1988), Sundsvall (1991), Jakarta (1997) and Mexico (2000) which identified additional areas for action. More recently, the Bangkok Charter (WHO 2005) outlines four key commitments:
 BOX 7.3
BOX 7.3A brief history of health promotion in the UK
1800–1900 Public health movement
Arose out of a conservative tradition of reluctant collectivism, that the state had to intervene to ensure national efficiency, economic advantage and social stability
1900–1940 Health education
A liberal laissez-faire agenda which allowed voluntary organizations to provide preventive health education
1940–1970s Rise of prevention
A broadly conservative ideology with the emphasis on individual responsibility for health with information and advice being provided by health professionals; this was coupled with state intervention to provide a safety net for the most vulnerable
1980s The rise of the individual
Despite calls for a coherent national programme to tackle widespread inequalities in health and the WHO Ottawa Charter, New Right ideology dominates the health service; individual freedom is emphasized
1990s The rise of the market
Several commentators have argued that health promotion in the UK is currently facing a crisis of identity, and is in danger of being subsumed by the new public health (Orme et al 2007; Scott-Samuel & Springett 2007). Health promotion has always struggled to have a visible presence and its position within the National Health Service has led to it being viewed as a ‘Cinderella’ service subordinated to health care provision and the medical model. Since 1997 and the election of the New Labour government, health promotion has been sinking from view, with the disappearance of both its specialist workforce and its lead organization in England (Scott-Samuel & Wills 2007). Health promotion is now just part of the remit of a range of other agencies and staff, including public health practitioners, the National Institute for Health and Clinical Excellence (NICE), health trainers and community development agencies. In many countries the ascendance of neoliberalism combined with traditional biomedical approaches inhibits the wholescale adoption of the Ottawa Charter principles for health promotion (Raphael 2008; Wills et al 2008). For example, in Canada an epidemiological focus on population health has displaced health promotion.
The following example shows how ‘joined-up policy-making’ by different agencies can contribute in a coordinated way to the aim of suicide reduction.
Health promotion activities are structured by the prevailing policy framework, which has the effect of legitimizing certain approaches and excluding others. Until 1997 in the UK a combination of free-market economics with authoritarianism favoured medical preventive approaches and those which focus on individual lifestyles. Health promotion was seen as a means to prevent morbidity and mortality from specified diseases. Education and advice were the key strategies. Primary care practitioners would identify individuals at risk from a database of the practice population and carry out lifestyle interventions.
Neoliberal ideology sees a more interventionist role for government, although the free-market economy is also emphasized as the means to meet needs. There is an emphasis on partnership working and consumer choice, attempting to transfer free-market economic relationships into the service sector. However there is also recognition that state support and intervention are required to mitigate the inequalities in health driven by socioeconomic inequalities (Bambra & Scott-Samuel 2005). This runs parallel to a pervasive life course discourse that locates health in the hands of the individual. (See Chapter 2 for more discussion of socioeconomic inequalities in health.)
The politics of health promotion methods
The methods used in health promotion are often viewed as a technical choice. Health promotion specialists are seen as possessing the expertise to decide what methods will prove most effective given the circumstances. However, we shall argue that methods imply political perspectives, and that the choice of which methods to use is not a politically neutral decision.
Health promotion has at its disposal a large repertoire of methods. These are discussed in greater detail in Part 2 (Figure 7.1).
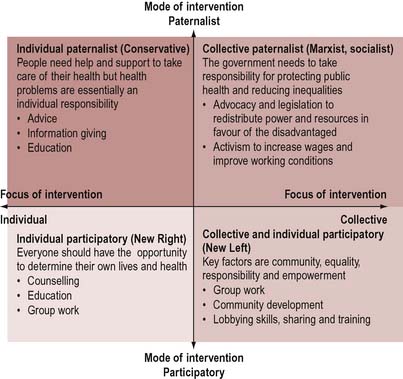
The individual paternalist approach (Conservative)
This approach is expert-led, by professionals, and is focused on the individual. It has a long history, remaining perennially popular. The virtue of professional training is that it gives patients and clients confidence and a clearly demarcated role. Methods focused on the individual send a clear message about individual responsibility for health. Such methods rely on the belief that individuals can make significant changes in their lifestyle or environment. The focus on the individual also implies that everyone has equal resources and means of complying with health promotion messages. This may be viewed as ineffective, or incorrect, and there has been much criticism of these methods as ‘victim-blaming’ and misconceived (Naidoo 1986). However, such a viewpoint is also politically inspired, which may go some way to explaining its endurance.
By ignoring structural factors which affect the life chances and perceptions of different groups of people, the fact that people’s personal identity is bound up with their membership of such groups is obscured. Such an approach also ignores the structured inequalities in health status that are linked to socioeconomic status. This approach reinforces professional power by stating that individuals need to comply with expert advice.
The notion of individual free choice is a central tenet of the free-market economy. In economic terms, individualism becomes translated into consumerism, or the right to purchase goods. This approach is linked to the commodification of health, which becomes advertised as a tangible asset that can be bought. For example, sales of organic food and health club memberships have risen sharply in the UK, due in large part to their promotion as routes to health and well-being. This process in turn further exacerbates inequalities in health, as only the richest people can afford these healthier lifestyle choices.
The individual participatory approach (New Right)
Neoliberalism emphasizes the role of the individual in determining their own choices. The individual participatory approach differs from the paternalistic individual approach by being premised on a different, and more equal, relationship between the health promoter and the client. This approach includes negotiated methods such as counselling, education and group work which take into account people’s beliefs, attitudes and knowledge. The client is an active partner in the process and the end goal is enhanced client autonomy. Many professional groups have shifted their practice in recent years and tried to become more client-centred. Many health promoters feel more comfortable using these methods.
It may be argued that individually negotiated methods are most used and valued by the relatively privileged, healthy and articulate sections of society. Those with the greatest need are least likely to be able to access this kind of health promotion intervention. The focus on the individual maintains the free-market consumerist ethos criticized above.
The collective and individual participatory approach (New Left)
Methods which focus on the collectivity are more likely to be allied to social democratic or socialist political ideologies. The emphasis here is on understanding the processes which shape health outcomes, and assisting people to develop the skills to shape and challenge these processes. The New Left neoliberalist ideology retains a belief in the supremacy of the free market, leading to a focus on individuals and consumerism. The unifying factor is a stress on participation and active involvement, whether of communities or individual consumers. Collective participation, or social capital, is increasingly recognized as an independent source of health as well as self-esteem (Wilkinson 1996). Governments have sought to encourage collective participation through neighbourhood and community initiatives, for example neighbourhood regeneration and renewal interventions. Individual participation is encouraged through patient choice and shared decision-making in relation to treatment and care. Underlying the commitment to equality is a parallel strand of responsibility.
Choosing Health: Making Healthier Choices Easier Choices (Department of Health 2004) refers to a contract between individuals, communities and the state. Given a goal of increasing physical activity, what might each party be expected to contribute?
Methods of health promotion that encourage participation include individually focused programmes centred on making informed choices and collective approaches that seek to redistribute power by empowering disadvantaged groups through such means as skills-sharing and training and lobbying.
The collective paternalist approach (Marxist, Socialist)
The collective paternalist methods of working are associated with Marxist and socialist political beliefs. These beliefs include the primacy of social class, determined by economic status, in predicting social status, culture and life chances. Socialism sees individual identity as shaped by social interaction and membership of social groups. The owners of the means of production (the middle class) and those who only have their labour power to sell (the working class) have conflicting economic goals (to maximize profits or maximize wages accordingly). Class conflict is seen as inevitable according to this perspective.
Karl Marx’s (1875) famous phrase ‘from each according to his ability, to each according to his need’ sums up the socialist goal of equality and social solidarity. Appropriate action uses methods such as the active redistribution of power in favour of the disadvantaged. Such action can be top-down (e.g. advocacy on behalf of lower socioeconomic groups or equity audits to expose inequalities) or bottom-up (e.g. trade union activism to increase wages and improve working conditions). Other methods may include promoting social cohesion through community development (see Chapter 10).
The methods adopted by practitioners in response to particular issues reflect political values about:
Consider the following methods which might be adopted in an HIV and sexually transmitted infection (STI) prevention programme with vulnerable young people:
This discussion has presented the view that the methods chosen to promote health are not politically neutral. Certain methods fit into, maintain and reproduce the ideological assumptions of certain political perspectives. However, it is important not to overstate this view. Methods and ideology are not deterministically linked in a cause-and-effect manner. A variety of methods across all four ideological perspectives may be used by health workers who espouse a particular political viewpoint. There may be convincing reasons for adopting an eclectic methodology to promote health. But it is a fallacy to assume that methods are a technically neutral aspect of the health promoter’s activity.
The politics of health promotion content
The previous sections have examined the view that the structure, organization and methods used in health promotion have a political dimension. It is sometimes argued that, although the process of promoting health is a political activity, the content of health promotion is neutral. Our position is that health promotion content is inevitably political. The framing of suitable agendas and the construction of what information is relevant are not value-neutral activities. On the contrary, they imply certain political values.
The Jakarta Conference (WHO 1997) identified the following priorities for worldwide health:
Perhaps the clearest example of the political nature of health promotion is the ongoing debate surrounding the social determinants of health. Whilst there is a wealth of research evidence linking poverty and disadvantage with ill health (Davey Smith 2003; Marmot & Wilkinson 2006), different governments have reacted differently. For almost two decades (1979–1997) a Conservative government refused to recognize the evidence on social inequalities and health, referring instead to ‘variations in health status between different socio-economic groups within the population’ (Department of Health 1992, p. 121). By denying the evidence, a non-interventionist policy could be adopted which argued that the free market is the best means of meeting health needs. By contrast, the Labour government elected in 1997 acknowledges the link between social inequalities and disadvantage and health and has commissioned reports and adopted targets to reduce health inequalities (Department of Health 2003).
Several research studies have confirmed that social democratic countries with strong welfare states, egalitarian ideologies and redistributive policies produce healthier populations, as indicated by lower infant mortality and low-birth-weight rates and increased life expectancy (Navarro & Shi 2001; Chung & Muntaner 2006, 2007; Navarro et al 2006).
Globalization creates new challenges for health promotion to widen its scope of action beyond national boundaries. Creating sustainable healthy environments requires international action. This may appear to be unrealistic for health promoters employed and working in a locality. However international networking, modern forms of communication using the internet and transnational policy-making have increased rapidly in recent years, opening up the possibility for more global health-promoting activity.
Food labelling in the European Union
The European Union (EU) agreed in 2008 to impose standard nutritional information in food labelling for all prepackaged food across 27 countries. The new labelling scheme was agreed as a means to curb the rise in obesity in the EU. The scheme falls short of the traffic light system advocated by health charities, but went further than self-regulation, which the food industry had lobbied for (Guardian 31/1/2008, p. 14).
Discuss the claim that evidence-based practice means health promotion is a neutral activity, because scientific methods have been used to determine what works and what doesn’t work.
Increasingly, practitioners are called upon to base their work on evidence. The rise of evidence-based practice can be linked to New Right ideas about the accountability of practitioners and services to the ‘consumer’. It could also be linked to socialist paternal collectivist ideas, identifying what works best and then requiring practitioners to follow set protocols. Evidence-based practice usually refers to a scientific notion of evidence that prioritizes randomized controlled trials as providing the best evidence (see Chapter 3). However this stance may be criticized for ignoring service users, their values, desires and wants. It may also neglect political and social issues that are too complex to factor into this model of decision-making. Evidence needs to engage with people’s views and beliefs rather than pursue abstract notions of health or ill health.
This view of evidence-based practice can also be criticized for adopting a naive view of science as politically neutral. Social scientists (Bauchspies et al 2005, David 2005) point out that science is a social activity like any other, subject to similar constraints. Health-related research does not take place in ivory towers. Researchers have to bid for funds, and provide findings which are acceptable to funders and the academic community. Research indicates that private-sector funding of charitable and non-profit health organizations influences their activities and outputs (Jacobson 2005).
The process of research is therefore not immune to political considerations. What evidence filters through to the general public as the scientific consensus on health topics is also the result of political processes. The very idea of scientific consensus in social science is debatable. There is no issue where there is 100% agreement of the ‘scientific facts’. For example, there is an ongoing debate about whether it is social capital or income that is responsible for the better health status of the more advantaged groups.
Being political
We have seen how health promotion arises from and reinforces political values and beliefs and takes place in a political context. Health promoters hold values and beliefs which are underpinned by established sets of ideas or ideologies. Many health promoters are engaged in practice which accords (more or less) with their personal values. The medical model of health provides a clear role for practitioners because it recognizes their expertise. It also gives a clear role for individuals to act to protect their own health. Some health promoters may find that their professional role at times comes into conflict with their political beliefs and values. A belief in collective health goals and the need to empower people to be involved and take control over factors influencing their health may be at odds with a health promotion role bound by corporate contracts and the need to meet targets.
Should health promotion have a code of practice that incorporates underpinning political principles? If so, what should be included?
The following activity is designed to help health promotion activists identify where they could make changes in their practice.
The following are suggestions for developing radical health promotion practice. How many do you think are feasible for you? Be clear and honest about your own political standpoint.
Conclusion
Politics, or the process and study of the distribution of power in society, underpins all human activities, including health promotion. The political scene is in a state of constant flux, with the early 21st century witnessing the rise of neoliberalist ideology and globalization. These processes and values are embedded in the context in which health promoters practise. An understanding and engagement with politics in its widest sense are necessary in order to practise reflectively and in accordance with one’s personal values and beliefs.
There is often resistance to the idea that health promotion is a political activity. Accepting the premise that politics is involved in health promotion may be experienced as muddying the waters, for it transforms a situation of relative certainty to one of uncertainty. It is no longer sufficient to rely on professional training to ensure effective health promotion. A whole range of different considerations needs to be taken into account, some of which threaten and call into question the whole notion of professional expertise.
However uncomfortable the process may be, an awareness of the political nature of health promotion is vital to its effectiveness (O’Neill 1989). Accepting the status quo is not an apolitical position but a deeply political one. What exists is not inevitable, but the result of complex forces and historical processes. Things might be otherwise. Health promotion is centrally concerned with a vision of better health for all. This vision may be informed by scientific knowledge and technical know-how, but its overall shape is determined by personal values and beliefs. Part of the task of health promoters is to uncover and hold up to scrutiny their values and beliefs. It is hoped that this and Chapter 6 will help health promoters in this task.
The following statements reflect particular political philosophies. Can you identify these political philosophies? Which statements do you agree with?