Chapter 19 Planning health promotion interventions
Overview
We have seen in Chapter 18 how needs assessment and targeting may be carried out, and the importance of carrying out this process and being clear about the context in which this is done. This chapter builds on the discussion of the first stage of planning – needs assessment – in Chapter 18. Firstly, definitions of planning are given and the reasons for planning discussed. Planning at different levels, from broad strategic planning through project planning to small-scale health education planning, is considered. The Ewles & Simnett (2003) and PRECEDE–proceed models (Green & Kreuter 2005) are reviewed in detail. Quality and audit issues and how this relates to planning are then considered.
Definitions
Planning is one of those terms which is used in many different ways. Other related terms are used in equally imprecise ways, so that often the same activity is labelled in different ways by different people. There are no hard and fast rules about the way terms are used, but the following definitions are presented as a means of clarifying the differences between related activities. These are the definitions we shall be using in this chapter.
 BOX 19.1
BOX 19.1Policy development
Judy has been given a remit to develop a health promotion programme with the aim of reducing the suicide rate. Her health authority’s policy includes a commitment to equal opportunities. She decides her priority will be unemployed people, who are known to be at increased risk of suicide. She consults with stakeholders. Judy’s objectives are: (1) to set up a support group for unemployed people; and (2) to provide specialist counselling services. Her strategy is to network with existing community groups, and to recruit and train volunteer counsellors.
Reasons for planning
Health promoters usually have no problem in finding things to do which seem reasonable. Work areas are inherited from others, delegated from more senior members of the workplace or demanded by clients. It is possible to be kept very busy reacting to all these pressures, and planning health promotion interventions may seem a luxury or a waste of time. However, there are sound reasons for planning health promotion or being proactive in your work practice:
Planning takes different forms and is used at different levels. It may be used to provide the best services or care for an individual client, as in the nursing process, or planning may be for group activities, such as antenatal classes. Planning may also refer to large-scale health promotion interventions targeted at whole populations.
The degree of formality of the planning process also varies. When planning a one-to-one intervention, the process is informal and may involve no one else. Planning for a group intervention may involve liaising with other professionals as well as the target group, to find out what their aims and objectives are and what sorts of methods and resources are available and acceptable. A written plan may be produced to act as a guide and a statement of agreed outcomes and methods. Planning a large-scale intervention will usually involve more long-term collaborative planning. Often a working group (or taskforce or local forum) will be established early on to identify interested groups and gain their support and expertise. A written plan will usually be produced, outlining not only objectives and methods but also a timescale of what is to be achieved when; funding details and a budget; who is responsible for which tasks; and how the intervention will be evaluated and the findings reported back.
There has been much greater emphasis on systematic planning in recent years due to a need for greater economic accountability, more focus on targets and their achievement, and the need to include evidence as part of project development. It is particularly important for practitioners to be clear about the rationale for interventions, the goals and the approach adopted.
Health promotion planning cycle
Planning involves several key stages or logical stepping stones which enable the health promoter to achieve a desired result. The benefit is being clear about what it is you want to achieve, i.e. the purpose of any intervention. Planning entails:
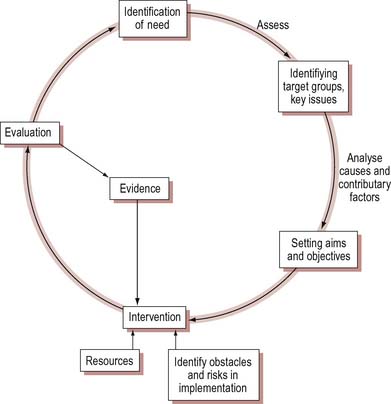
Some planning models are presented in a linear fashion. Others show a circular process to indicate that any evaluation feeds back into the process, as illustrated in Figure 19.1. This seemingly rational and simple approach describes how decisions should be made. It does not take into account that there may not be agreement on objectives or the best way to proceed and that in real life, planning is often piecemeal or incremental. There is no grand design, but circumstances dictate many small reactive decisions.
 BOX 19.2
BOX 19.2What do you think would be the best starting point for planning an intervention or programme? Why?
Think of any planned activities you have been involved with. What was the starting point? Why?
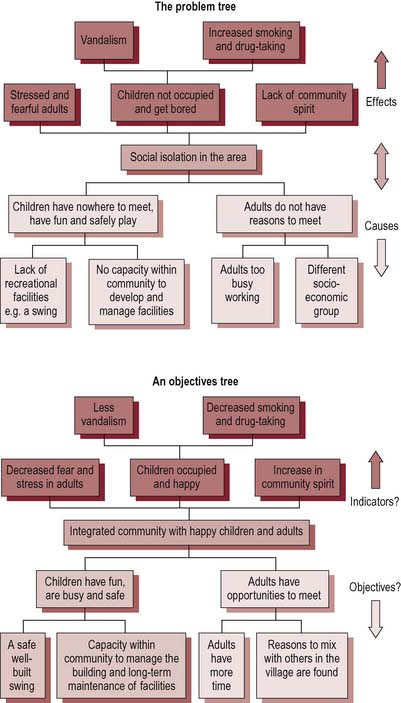
Figure 19.1 suggests that the planning cycle begins with a needs assessment through which the programme’s focus and any specific target groups may be identified. The underlying causes and contributory factors that led to the problem and the areas that will need to be addressed are then identified. Figure 19.2 shows how understanding the effects of a problem can help to identify indicators and desired outcomes from an intervention. Turning the problem, in this case antisocial activity by young people in a neighbourhood, into a positive statement gives a purpose for the intervention. Addressing the causes of the problem identifies outputs and activities. The aims and objectives can then be clearly stated. This provides a number of options for intervention and at this point many other issues come into play such as resource availability, capacity and potential obstacles. These issues will then be considered alongside any evidence of effective interventions. The actual intervention or programme and its methods can then be selected. The practicalities of implementation will need to be explored and the evaluation and monitoring plans put in place. This simple model can be applied to all levels of planning activities, from large-scale strategic planning, to middle-scale project planning and small-scale interventions with clients.
Strategic planning
Strategy tends to be used as an umbrella term to cover a broad programme. It may therefore have several different objectives and projects. Practitioners often do not start with a blank sheet and have to work in a wider policy context where issues are determined nationally. For example, all primary care trusts are required to have a strategy to tackle obesity. Strategies may be local as well as national and involve many stakeholders. A stakeholder analysis helps to identify relevant partners and their interests regarding the issue. For example, local area agreements (LAAs) require consultation between statutory and voluntary agencies and local populations to draw up agreed plans to promote health in a defined locality. LAA plans include:
Developing a local obesity strategy
Read the extract below from a local obesity strategy. What actions can you identify?
To ensure the long-term commitment of all stakeholders and to try to develop a robust action plan, an extensive consultation process has been undertaken within Torbay during the development of this strategy. Opinions have been sought with regards to both the prevention and management of obesity from stakeholders and members of the general public living in Torbay. Furthermore, a resource mapping exercise has also been undertaken. Alongside the mapping of current practice and the recording of both public and stakeholder opinion regards priorities for action, the evidence for the effectiveness of a broad spectrum of interventions was researched at length. This, alongside local and national policy, was used to help prioritise potential actions. Furthermore, those actions known to have evidence of effectiveness reaching those individuals at greatest potential risk were given largest priority … Work to improve the health of the population is by no means the sole responsibility of the health service and increasingly local responsibility for the health of communities is being shared between the agencies that make up Local Strategic Partnerships (LSPs) and with the communities themselves (Torbay Care Trust 2006).
There are several stages in developing a strategy:
These stages correspond to those of a rational planning model: assess–plan–do–evaluate.
Project planning
Project planning is a smaller-scale activity and refers to planning a specific project which is time-limited and aims to bring about a defined change. Examples of small-scale health promotion projects include a project to raise the awareness of university students about meningitis, a project to train school nurses in presentation skills and a project to map safe routes to school for young children.
You are involved in a working group drawing up a local strategy to reduce alcohol use. Who would you want to be involved in the working group? What broad goals would be appropriate?
Broad goals might be framed in terms of:
The working group would need to involve a variety of partners in order to maximize its effectiveness. You might have identified representatives from the local authority, mass media, occupational health services covering workplaces, primary health care practitioners, mental health practitioners, teachers and youth workers, licensed victuallers, magistrates, the police service and voluntary agencies dealing with alcohol-related problems. The success of this strategy will depend on the different partners working together to achieve aims.
Ewles & Simnett (2003) define project stages as:
The start of the project is agreement that the project should take place, its overall aims and the allocation of a budget to support the project. Often the start is signalled by the formal adoption of a project proposal, indicating that an organization has given support for the development and implementation of a project. Specification means setting objectives and quality criteria for how the project is to be delivered. Setting objectives is considered in more detail below. Quality and audit are discussed later in this chapter. Design is the detailed planning of the training intervention. A Gantt chart (set out as an example in Figure 19.3) is a useful tool to use at this stage. A Gantt chart plots tasks and the people responsible for these tasks against a timescale in which these activities need to be undertaken. It portrays in a graphical form the interdependence of project tasks and how each single task contributes to the whole. Implementation is the project activity, e.g. training sessions. Evaluation, review and final completion report on project outcomes and assess whether objectives have been met. It is useful to have a time lag between completing the project and the final review in order to assess long-term as well as immediate outcomes.
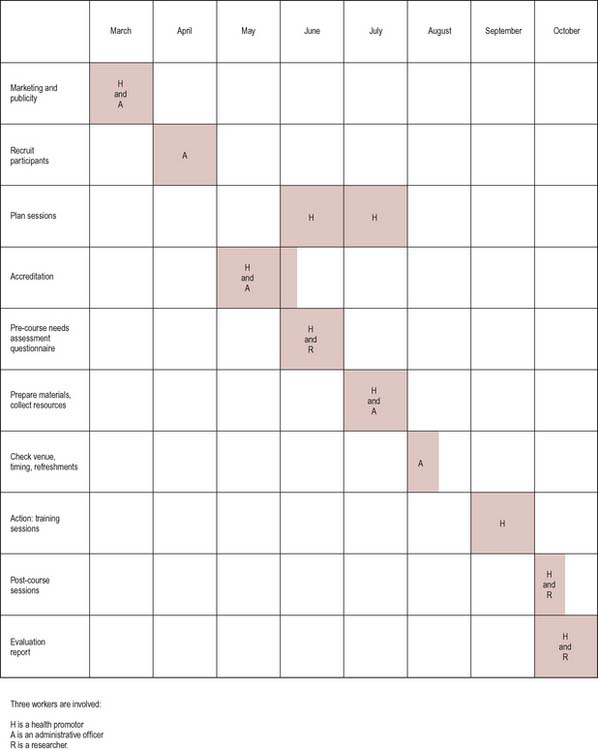
Figure 19.3 Gantt chart: planning training project. Three workers are involved: H, health promotion specialist; A, administrative officer; and R researcher.
The strategy outlined in Activity 19.4 includes a project centred on training GPs and practice nurses to identify problematic use of alcohol at an early stage. This project, which is part of the overall alcohol reduction strategy, would require careful and detailed planning, including:
The kind of planning most health practitioners will be involved in will be on a much smaller scale. For example, you may want to plan a health education session with an individual client, or a series of sessions with a small group around a specific issue. Using the example above, you might want to plan a single session in detail. This would require you to:
Planning models
Planning, whatever the scale of the activity, requires systematic working through a number of stages. There are a number of different planning models that have been developed, two of which are now discussed in greater detail.
Ewles & Simnett (2003) planning framework
The Ewles & Simnett (2003) planning framework (Figure 19.4) is a useful generic framework which can be adapted to a number of situations.
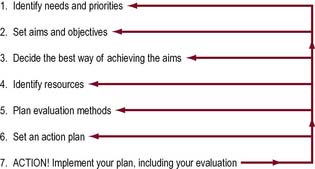
Stage 1: identify needs and priorities
This may need local research and investigation, or may be the selection of particular clients from a caseload. Researching needs may require additional investigation. For example, local community profiles and local agencies might provide information on pressing local needs. Consultation with community members may flag up their felt needs and priorities. Needs may already be defined for you, often on the basis of national or local epidemiological data reporting trends in illness and deaths. Chapter 18 discusses this stage in more detail.
Other planning models start at different points. For example, a stated health promotion goal can be analysed to determine an appropriate educational intervention. This intervention is modified by referring to the characteristics of the target group, and a detailed educational programme planned. For example, an accident reduction programme identifies education about hazards in the home as a priority. The target group is older people. Based on evidence of other interventions with older people, it is decided that interpersonal communication would be the most effective intervention. Specific objectives are formulated concerning education about lighting and mobility aids.
Stage 2: set aims and objectives
Aims are broad goals concerned with improving health in a particular area or reducing a health problem, e.g. reducing the amount of alcohol-related ill health. Objectives need to be specific and should be statements that define what participants will have achieved by the end of the intervention. Objectives therefore need to be measurable in some way. There is a balance to be struck between setting objectives which are realistic but also challenging. When writing objectives it is recommended that they are SMART:
Health promotion objectives can refer to educational, behavioural, policy, process or environmental outcomes:
Educational objectives may be divided into three categories:
Setting objectives for a training programme
A project has the overall aim of improving the early identification of alcohol-related problems. One of the objectives is to raise the awareness of GPs and practice nurses to such problems in patients. One activity might involve a training session with the following educational objectives:
Objectives also reflect perspectives about the determinants of health and values about what are the most important things to achieve. These perspectives and values may be your own or may be derived from your organization.
 BOX 19.7
BOX 19.7Stage 3: identify appropriate methods for achieving the objectives
Decisions about how to go about addressing the problem will depend on objectives but also available evidence of effective interventions, available funding and the expertise of practitioners. Certain methods go with certain objectives but would be quite inappropriate for other objectives. For example, participative small-group work is effective at changing attitudes but a more formal teaching session would be more effective if specific knowledge is to be imparted. Community development is effective at increasing community involvement and participation but would not be appropriate if local government policy change is the objective. The mass media is effective in raising people’s awareness of health issues but ineffective in persuading people to change their behaviour. So the next stage in planning is deciding which methods would be the logical choice given your objectives. You may then find you have to compromise owing to constraints of time, resources or skills, but this compromise should concern the amount of input, or the use of complementary methods. It should not mean that you end up using inappropriate methods which are unlikely to achieve your objectives.
A Sun Smart programme in Australia identifies a major health problem in children’s exposure to ultraviolet light. A diagnosis of the risk factors for this identifies children not wearing hats and lack of shade in the playground. The contributory factors for children not wearing hats are their dislike of wearing them and the lack of any requirement to wear them. The contributory factors for the children’s exposure to sun when in the playground are lack of funds to build shelters and lack of awareness by children of the need to keep out of the sun.
Regulating to make the wearing of hats part of school uniform might make the healthy choice easier, so encouraging stakeholder involvement in a review of uniform requirements might be an objective. Making hats a fun and desirable part of clothing and raising funds to build a playground shelter might be other objectives.
Stage 4: identify resources
When objectives and methods have been decided, the next stage is to consider whether any specific resources are needed to implement the strategy. Resources include human resources, financial resources and materials and equipment.
What would you need to include in a budget plan for the training sessions for GPs and practice nurses on early identification of problematic alcohol use discussed in Box 19.4?
Funding is an important issue for larger-scale interventions which require additional inputs over and above existing services and staff. For larger-scale interventions you may need to prepare a budget which is a statement of expected costs. This includes direct costs, which relate to the project, and fixed costs, which happen anyway.
Fixed costs include overheads to cover accommodation, heating, lighting and telephone rental.
A budget control system regularly monitors what is spent and what remains. This is usually done by monit-oring the amount of money allocated, the amount of money spent and the variance between the two (underspend or overspend) under each budget heading every month.
Stage 5: plan evaluation methods
Evaluation must relate to the objectives you have set but can be undertaken more or less formally. For example, in relation to an educational session you might decide to ask participants their views at the end of the session, or spend some time noting your own perceptions of what went well and what could be improved next time. Or you might design a more formal means of evaluation, e.g. a questionnaire for participants to fill in anonymously, which is timetabled into the session. Project evaluation is discussed in more detail in the next chapter.
Stage 6: set an action plan
This is a detailed written plan which identifies tasks, the person responsible for each task, resources which will be used, a timescale and means of evaluation. You might also include interim indicators of progress to show if you are proceeding as planned. Many factors can threaten the sustainability of a project. Being clear about the external factors underlying the structure of the project and what assumptions are being made is a key requirement of most project plans, especially where large sums of money are being allocated. For example, projects may depend on achieving community involvement or successful fund-ing bids.
Log frames (logistical frameworks) are widely used in international development projects to identify the activities of a programme and any inherent risks that might delay completion (see Figure 19.5). The benefit of a log frame is that it tests the assumptions of a project plan. Working from the bottom up, it tests the logic through ‘if–then’, i.e. if we do these activities, then this output will be achieved. If we deliver these outputs, then this purpose will be achieved. If the purpose is achieved then this will contribute to the goal. Flaws in logic might include having a purpose that is too far away from the outputs or a purpose that cannot be assessed.
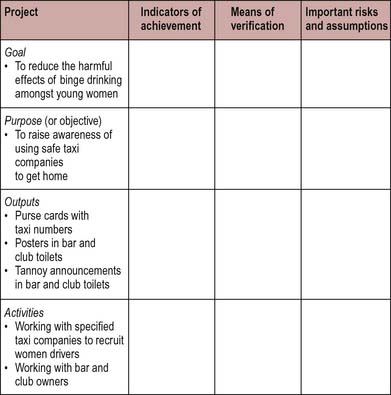
Complete the log frame, in Figure 19.5 above. What are the advantages of using this framework in project management?
Stage 7: action, or implementation of the plan
It is often useful to keep a log or diary to note unexpected problems and how you dealt with them, as well as unintended benefits. This information can then be fed into the evaluation process. You will also want to plan for the documentation and dissemination of the findings from the project, whether in the form of a report, a newsletter or presentation.
PRECEDE–proceed model
Figure 19.6 illustrates the PRECEDE–proceed planning model, one of the earliest and best-known models which has now been revised and simplified (Green & Kreuter 2005). PRECEDE stands for predisposing reinforcing and enabling causes in educational diagnosis. This model recognizes the multiple determinants of health and starts with an assessment of the quality of life, which is the ultimate goal. Health contributes towards quality of life. The model then works backwards in a sequence of diagnostic phases to identify the environmental and organizational factors that influence health behaviour, including health service utilization. It considers the predisposing factors, those personal factors such as individual motivation, knowledge attitudes and beliefs; reinforcing factors, the attitudes and behaviours of role models, peers, employers; and enabling factors, resources and skills that either support or hinder change in behaviour or environment. As well as diagnosing what needs to be addressed, the capacity for implementation of a proposed programme is also considered.
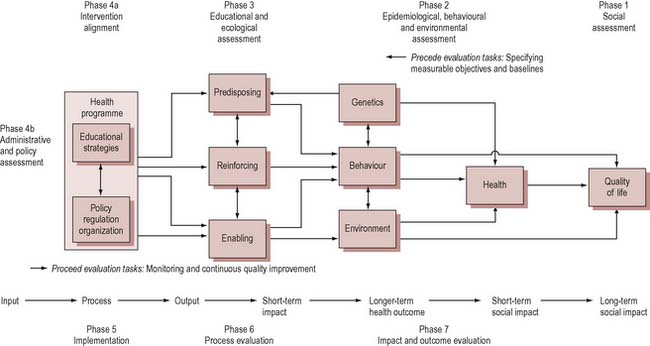
The model may be broken down into phases, as illustrated in Box 19.11. Priority targets for intervention are established through each phase of the assessment process (phases 1–4) on the basis of:
The results of this assessment process guide the development of the intervention (phase 5). The evaluation (phases 6–7) then tracks the impact of the intervention on factors identified as important targets in the assessment process.
Phases of the PRECEDE–proceed model
The intention is that using the PRECEDE–proceed model will guide the health educator to the most effective type of intervention. Using knowledge drawn from epidemiology, social psychology, education and management studies, the health educator can arrive at an optimum intervention. The model is said to be based on a complementary mix of expertise drawn from these different disciplines. In practice, the model is often modified and is rarely used as illustrated (see Green’s own website for an account of the application of the model: http://www.lgreen.net/precede.htm). For example, it is unusual to begin the process of planning with an agenda as open as ‘quality of life’. Priority topics, target groups or settings are more often identified at the outset. For example, the Saving Lives: Our Healthier Nation targets (Department of Health 1998) focus on specific diseases. So in practice the use of the PRECEDE proceed model often begins at the behavioural diagnosis rather than the needs assessment phase.
The PRECEDE–proceed model may be criticized on several grounds. As a health education planning model it mirrors the medical world. The planning process is dominated by experts. The general public may be involved in identifying problems, but the ways and means of tackling these problems are to be determined by experts. The focus is on achieving behavioural change at the level of individuals or groups. The social, political and environmental context of health is systematically screened out by the model in phases 2 and 3. To some extent this may be explained by the PRECEDE proceed model being a health education rather than a health promotion planning model. A model developed specifically for health education cannot be expected to apply to other forms of health promotion but, for most people, education, even if it does not include changing the environment, does include clarifying values, beliefs and attitudes, facilitating self-empowerment and supporting autonomy. Using the PRECEDE–proceed model subordinates these activities to the primary aim of behaviour change. It could be argued that PRECEDE–proceed is a model dominated by social psychology and behavioural perspectives rather than educational perspectives, and that the label is therefore misleading. PRECEDE–proceed is, however, a highly structured planning model which ensures that certain issues are considered. If the objective is behaviour change, then PRECEDE–proceed is a useful model to follow.
Quality and audit
Assessing the quality of practice through quality assurance, quality management or audit is an important aspect of professional practice. It helps to improve standards, identify cost-effective activities, demonstrate worth to outside agencies and ensure that activities meet stakeholders’ requirements. The introduction of commissioning of services and the placing of contracts have highlighted the need for specification of quality. There has also been an increased emphasis on audit of public sector activities and clinical audit is well established. Frameworks are established such as the protocols established by the National Institute for Health and Clinical Excellence (NICE) as well as National Service Frameworks and the Healthcare Commission in order to ensure high-quality health services. Continuous quality improvement, total quality management and the use of external standards all aim to improve services and also provide answers to the variability in programme development. The core principles of quality interventions in health promotion have been defined as (Speller et al 1997):
Quality expresses a notion of ‘fit for the purpose’ but also conveys a notion of excellence. Applying the notion of quality to work practice is difficult. One means of trying to do this is through quality assurance or audit which is a ‘systematic process through which achievable and desirable levels of quality are described, the extent to which these levels are achieved is assessed, and action taken following assessment to enable them to be realised’ (Wright & Whittington 1992).
Quality assurance is an ongoing process of continual assessment and improvement of practice, and therefore differs from evaluation, which focuses on outcomes at a specific point in time. A quality system may include elements of quality assurance and quality management. Quality assurance involves setting standards which specify quality and ensure consistency. Quality management applies the emphasis on quality to everyone through increasing their control over their performance. Quality assurance in health promotion is defined as:
the process of assessment of a programme or intervention in order to ensure performance against agreed standards, which are subject to continuous improvement and set within the framework and principles of the Ottawa Charter (Speller 1998, p. 79).
Quality is about doing things in the correct manner. Box 19.12 outlines the criteria in the European Quality Instrument for Health Promotion for supporting development of interventions, benchmarking and evaluation (Bollars et al 2005). It states that indicators of quality relate to appropriate design, good management and practice that accord with core principles.
European quality instrument for health promotion
I. Framework of health promotion principles
This approach embraces the principles of health promotion, including a positive and comprehensive approach to health, attention to the broad determinants of health, participation, empowerment, equity and equality.
II. Project development and implementation
III. Project management
IV. Sustainability
The continuation of the project is ensured
(www.nigz.nl/gettingevidence and in full at http://ws5.e-vision.nl/systeem3/images/Annexe%2010%20EQUIHP.pdf).
Audit is a systematic process of scrutinizing a service or programme in order to improve performance. Audit may focus on a particular aspect, e.g. organization and management or training. Part of the purpose of an audit is to build a picture, providing evidence of gaps and areas for improvement by comparing what is done with agreed best practice. A key part of an audit is to see if a service meets the needs of its users, so it may involve gathering and acting on local people’s views. Audit may involve an internal review or scrutiny by an independent external auditor (e.g. the Audit Commission, Ofsted inspectors of schools).
Conclusion
There are sound reasons for adopting a planning model to structure health promotion interventions. Recognizing that health is a complex socially determined concept means that activities to promote health require careful planning, and often collaboration and working together with different agencies. Activities at different levels all benefit from planning, although the factors which need to be considered will vary according to the level of planned intervention.
The rationale for planning is summarized by the Centre for International Development and Training (2006) as follows:
Planning provides a standard framework in which projects/programmes/interventions are developed, implemented and evaluated. The planning cycle ensures that the results of a project are fed back into new projects and programmes. There are a variety of planning models for health promotion and they can help make explicit the various values, rationales and assumptions that are inherent in the decision-making process.
In reality, planning health promotion is a more complex process than the planning models suggest. This is because rational decision-making is only one factor in determining what happens. Many other factors are also important, including historical precedent, enthusiasms of key people and the political context. So it is unlikely that any health promotion intervention proceeds exactly along the lines indicated by a planning model, but this does not mean models are not useful. Models help structure activities and can act as a checklist to ensure that important stages are not missed out. They are there to be modified in the light of experience, not to act as straitjackets.
Chapter 20 goes on to discuss the evaluation stage. Evaluating interventions, and being able to determine to what extent health promotion is successful in achieving its objectives, is the key to establishing health promotion as a central plank of health work.