Chapter 18 Assessing health needs
Overview
The first phase in health promotion planning is an assessment of what a client or population group needs to enable them to become healthier. Health care usually takes the individual as its starting point. Public health concerns the health and welfare of people in groups. Practitioners do not assess individuals in isolation from the communities in which they live. As we have seen in previous chapters the health experiences of individuals are affected by where they reside. The local knowledge of practitioners about the range of local services, facilities and networks is an important part of needs assessment. Within a neighbourhood there will be people in settings such as schools and workplaces and population groups with specific health needs. Practitioners need to know how to assess individuals, how to manage their care and how to encourage healthier lifestyles. They also require an understanding of people’s ways of life and the health problems and opportunities they experience and they need to know how to use this understanding to assess the needs of people in groups systematically. The term needs assessment describes the process of gathering information. It has been defined as a ‘systematic method of reviewing the health needs and issues facing a given population leading to agreed priorities and resource allocation that will improve health and reduce inequalities’ (Cavanagh & Chadwick 2005). The purpose of health needs assessment at national, regional or local level is twofold:
Recognition of the right to participate in defining health needs and health care was acknowledged in the 1978 World Health Organization (WHO) Alma Ata Declaration, and one of the underlying principles of Health For All is community participation (WHO 1985).
National Health Service (NHS) reforms have emphasized the participation of local people in setting priorities, signalling a philosophical shift from a paternalistic medical model to a participatory consumer-led model. This chapter considers the ways in which local health needs are assessed and applied in planning for health promotion. It should be read in conjunction with Chapter 3, which outlines the principal sources of information about health status.
Defining health needs
The concept of need is widely used but often not well understood. People may believe they ‘need’ a new coat because someone observed that their old one is worn out, or because it looks old compared to other people’s coats, or simply because they would like one. A need may thus be something people want or something that is lacking in comparison to others.
 BOX 18.1
BOX 18.1There are two different understandings of what constitutes a health need. It can be seen as:
 BOX 18.2
BOX 18.2Economists tend to avoid the use of the term needs altogether, arguing that it is overlaid with emotion and what is really meant by a health need is actually a matter of people’s wants and demands, and these are limitless (Cohen 2008). Identifying health needs is therefore a question of identifying priorities.
An alternative view is that there are universal needs. Maslow’s hierarchy of needs (Maslow 1954) suggests that all human needs are in fact health needs (Figure 18.1).
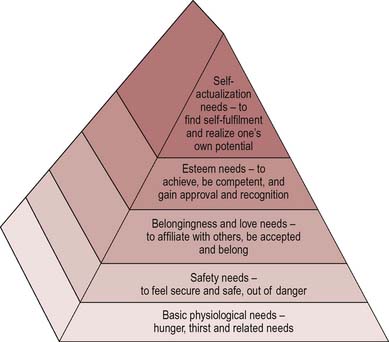
For a person to be self-actualizing, physical, social and emotional needs must be met. Doyal & Gough (1992) have similarly argued that the ultimate goal of human beings is to participate fully in society and to do this the basic needs for physical health and for autonomy must be met. These needs are not relative to a particular country or period of time but are fundamental rights and include the prerequisites for health – peace, shelter, education, food, income, a stable ecosystem, sustainable resources, social justice and equity (WHO 1986). But these needs are not undisputed. How healthy do people have to be before we can say that their needs have been met? Bradshaw (1972), in a widely used taxonomy, distinguished four types of health and social need:
Normative needs
Normative needs are objective needs as defined by professionals, who also identify the ways in which these needs can be met. A normative need reflects a professional judgement that a person or persons deviate from a required standard. This may be against some external criteria such as occupational or legal requirements. Thus the manager of a restaurant is in need of training because she has not completed a course in food hygiene. Or it may be that a person deviates from what is defined by medical staff as the range of ‘clinically normal’ physiological indicators.
 BOX 18.3
BOX 18.3Normative need: child development
A health visitor decides that, according to a growth chart, an infant has failed to gain weight for some time and has fallen below the third centile. She deems the infant to be in need of supplementary feeding and suggests this is done by additional bottle-feeding. Yet expectations of child development vary according to the place and time. This infant would not be regarded as failing to thrive in the USA or in pre-war UK.
Normative needs are not absolute or objective ‘facts’ – they reflect the judgement of professionals which may be different from that of their clients. Health care workers will judge a need relative to what they are able to provide. The ability to judge normative needs also contributes to the notion of professionalism and the authority and status of professionals.
Felt needs
Felt needs are what people really want. They are needs identified by clients themselves which may relate to services, information or support which can be termed service needs. Moves towards bottom-up approaches in health and social care have meant a greater acceptance of service users’ views. (Chapter 6 in our companion volume (Naidoo & Wills 2005) discusses some of the policy drivers to patient and public involvement.) Needs may be limited by the perceptions of an individual. Individuals may not believe themselves to be in need simply because they do not know what is available in terms of treatment or services.
A GP practice is aware that a lot of patients are seeking consultations for their concerns about not getting pregnant. The practice decides to hold an evening talk on preconceptual care. The talk is advertised in the surgery. No one attends.
This is an example of a need identified by professionals. No consultation was involved. The intervention was planned in the expectation that it would result in a saving of GP time, not as part of a programme to prioritize infertility. The intervention was poorly presented with no marketing, and no attempt to make it accessible for clients.
Expressed need
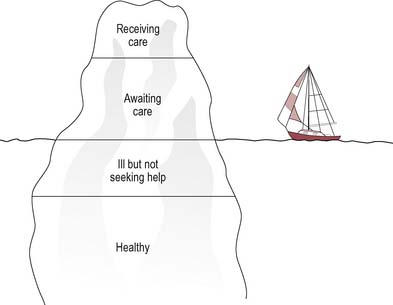
Expressed need arises from felt needs but is expressed in words or action – it has become a demand. Thus clients or groups are expressing a need when they ask for help or information, or when they make use of a service. Expressed need is often used to measure the adequacy of service provision, even though it is not a comprehensive or complete measure. There are also objective needs which exist but are not expressed. Only a proportion of patients make contact with health services and they are merely the tip of an iceberg of potential need, as illustrated in Figure 18.2.
Sometimes people will use a service because it is all that is available, even if it does not adequately meet needs. The best example of expressed need (and unmet demand) is the waiting list. Some needs are not expressed, perhaps because of an inability or unwillingness to articulate the need. This could be due to language difficulties or a lack of knowledge. Expressed needs should not be taken as an indicator of demand because they also exclude needs which are felt but not expressed. Tudor Hart’s inverse-care law has been of vital importance in showing that just because a service or treatment is used less does not mean that it is needed less (Tudor Hart 1971). Those who could most benefit from a service are often those least likely to use it. People may express different needs, and there is a tendency to listen to those with loud and powerful voices, such as views which come from an established group or views which appear to express a popular need. Responding to expressed needs may also therefore have the effect of increasing inequalities in service provision.
Comparative needs
Individuals or groups are said to be in need if their situation, when compared with that of a similar group or individual, is found wanting or lacking with regard to services and resources. For example, if a person with schizophrenia in area A was living in sheltered accommodation and receiving day care, but in area B this was not available, we would say that schizophrenics in area B were in need. In the NHS, although people may be assessed to be in absolute need (normatively), in practice comparative needs assessment will often dictate whether their needs will be met. Areas may be compared on the basis of provision of services or length of waiting lists to see if the health needs of their populations are being met. In a sense, then, comparative need is about equity. It is about equal provision for equal need. This kind of analysis of need does, of course, assume that those in receipt of a service are receiving adequate provision and that their needs are being met.
Bradshaw’s work (1994) is useful in showing that different groups in society hold different definitions of need. We can see that needs are not objective and observable entities to which we must just match our interventions. The concept of need is a relative one and is influenced both by values and attitudes and by other agendas.
Consider these interventions available to women in childbirth. Has medicine created these needs or are they needed improvements in technology?
At first sight, these developments may be seen as the consequence of medical advances. However, medical interventions in childbirth can also be seen as an attempt to establish doctors’ control over that of midwives. The range of interventions may, on the one hand, alienate women and make childbirth an uncomfortable and distressing experience and, on the other hand, the very availability of these services may create a need for them.
A very different list of needs may be compiled by pregnant women, including for example:
These felt or expressed needs may or may not be acknowledged and provided for by service providers. Consider the following questions:
What is clear from the above discussion is that definitions of need vary depending on whose interpretation and values are used. People’s health needs are not the same as those of 20 years ago – the nature and prevalence of diseases may change, as do the expectations of the population and the capacity of health services to meet them. The NHS uses the term health gain in association with health needs to signal that the meeting of needs is related to a person’s ability to benefit. Health gain is defined as:
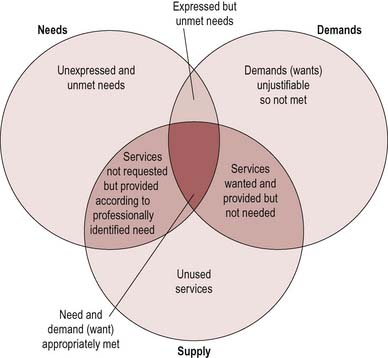
The concept of health gain is rooted in a medical model which sees health as the absence of disease. Consequently, health needs tend to be defined as problems which may be successfully met by services or treatment. Because need is seen as infinite and resources as limited, health authorities confine themselves to what is known to be effective care. Yet community surveys often show that the public define ill health far more broadly than simply problems requiring treatment by health services. Many priorities for health go beyond the narrow outcomes encompassed by adding ‘years to life’ and require health authorities to take account of the structural influences on health, such as housing, community safety and transport links. The meeting of needs is also related to what can be offered (what the state can supply). These differing interpretations are illustrated in Figure 18.3.
The purpose of assessing health needs
The process of assessing needs is nothing new. As we shall see in the next chapter, understanding needs is integral to a basic process approach to planning. Needs assessment including the collection of data is the first step, from which subsequent aims will be derived. Assessing the health and social needs of local populations is a means of obtaining accurate and appropriate information on which to base priorities and ensures that decisions are based on solid information and evidence. This overall purpose can be broken down into different stages as follows.
First stage: help in directing interventions appropriately
Within clinical practice assessing needs is routine and accepted. Assessment takes place to determine what care is required through the gathering of data about:
An integrated care pathway gives a single record of assessment for all the many professionals and agencies who may be involved with a patient but it also provides a map of care for all patients with a similar set of symptoms or diagnosis. It is intended to reduce variations in interpretations of need and treatment offered.
For those practitioners who work with individual clients, there is increasing recognition of the importance of client participation in the assessment of needs. Nursing practice, for example, has frequently been criticized for being too inflexible and routine – doing things to people rather than with them. Prescription has now given way to negotiation alongside the move from sick nursing to health nursing. Understanding the thoughts, feelings and experiences of individuals has become an important part of the therapeutic and nursing process.
Increasingly, health care workers seek to identify clients’ views and perceptions about their health as part of their assessment. What they often find is that their perception differs from that of the client. Clients’ need for information is often underestimated and in health care settings this may mean that information is confined to ward or clinic routines. Despite the greater emphasis on being client-centred, practitioners tend to assess needs in relation to the service they provide. Practitioners may interpret client needs as information needs because it is possible to provide this, whereas the satisfaction of physical needs (as in Maslow’s hierarchy) may seem beyond their scope.
A male patient who is young and fit has a heart attack. The nurse on the ward offers the patient advice on cardiac rehabilitation and information on healthy eating, exercise and safe drinking.
The medical and individualistic approach is adopted because it is a well-understood part of the nurse’s professional role. The nurse understands coronary heart disease prevention as focusing on risk factors even though they are not relevant to this situation. The patient may have other health needs such as a concern about getting back to work or when he might be sexually active again. Assessing individual health needs means starting with the patient’s own concerns.
Second stage: identifying population needs and reducing inequalities
To meet community health needs it is essential to have a clear understanding of what the needs are, what capacity communities have for addressing these needs, and whether particular groups face specific challenges in meeting their needs. Health equity audit is a requirement of planning in which local strategic partnerships and other organizations systematically review the role of inequities in the causes of ill health and the access to services for defined population groups. Health equity audits show whether different categories of people (categorized by socioeconomic group, geographical area, age, sex, disability or minority ethnic group) are having their needs met in an equal manner and whether the most appropriate services are being provided (http://www.nice.org.uk/niceMedia/documents/equityauditfinal.pdf).
Consider the following information about a ward (Easttown) in a local borough (Townsville). What are its health needs?
| Rates of mortality (SMR*) | Easttown | Townsville |
|---|---|---|
| All causes | 144.6 | 133.4 |
| Circulatory disease | 201.4 | 153.2 |
| Cancer | 84.5 | 110.4 |
| Coronary heart disease | 244.2 | 153.1 |
* An SMR (standardized mortality rate) of 100 indicates that the ward has average mortality. Higher than 100 indicates higher than average mortality.
A population such as Townsville that has significantly above-average rates of coronary heart disease could be said to be in need of more health service provision, including hospital beds, defibrillators, appropriate medication, e.g. statins and health promotion programmes. On the other hand, such statistics may be interpreted as revealing a community-wide need for an infrastructure to support healthier lifestyles, including aspects such as transport, food security, exercise and access to health services.
Third stage: identifying and responding to the specific needs of minority groups and socially excluded groups
There are recognizable social, demographic or identity-based groups who have traditionally avoided or been excluded from service needs assessments. Such harder-to-reach groups may think that services don’t care about them, don’t listen or are irrelevant. For example, studies of the health of gypsies and travellers have shown that:
There are widespread communication difficulties between health workers and gypsy travellers, with defensive expectation of racism and prejudice. Barriers to health care access were experienced with several contributory causes, including reluctance of GPs to register travellers or visit sites (Parry et al 2004 p 8).
How might health practitioners attempt to meet the needs of hard-to-reach clients?
A first step might be an audit to compare caseloads with the local population. If particular groups are underrepresented, involving members of such groups in discussion about service provision would be useful. This might involve practitioners going out to community venues and networks, e.g. community or religious centres. Other strategies might involve addressing obvious barriers such as language by the translation of information materials or the use of interpreters. If particular groups have specific health risks (e.g. coronary heart disease amongst Asians and stroke amongst African-Caribbeans), opportunistic screening and monitoring might be encouraged. Providing mobile services in people’s communities has also been used successfully, e.g. to provide sexual health services for young people.
Fourth stage: targeting risk groups
Targeting may be done in terms of diseases, life cycles, lifestyles or social groups. The concept of risk groups has emerged as a means of directing health promotion activities to people who are most in need. A risk group may be defined as a population group vulnerable to certain diseases or conditions. A risk group’s vulnerability may be due to genetic, lifestyle, economic, social or environmental characteristics. Normative needs derived from epidemiological research, which identifies groups with poorer than average health, are often used to establish target groups. For example, lower socioeconomic groups at most risk from ill health and premature death are a commonly identified risk group. Comparative need is used to identify at-risk groups who have low take-up rates of services.
However, a focus on high-risk groups can lead to ‘victim-blaming’. Health problems are seen as specific to particular groups who may also be seen as responsible through their behaviour for their own ill health (Naidoo & Wills 2005). For example, young people are the subject of numerous targeted health promotion campaigns. Yet it is not being young that is a risk but certain activities. Many health promoters also reject the notion of targeting because they prefer to work in partnership with groups and communities on the issues they define as important.
Fifth stage: allocating resources
The NHS was predicated on the notion that there was an untreated pool of sickness that, once treated by a national health service, would diminish. Experience shows that there can be unlimited demand for health care. As health care is provided, so expectations rise; as technology improves, people with disabilities and chronic diseases live longer and demand more health care. General improvements in health and living conditions have led to people living longer and an increase in the percentage of older people in the population. It will not be possible to meet all these needs as resources are limited.
Most doctors and health care workers accept that some kind of priority-setting or rationing of health care is inevitable. There have always been waiting lists but rationing is a more far-reaching concept. It entails decisions about how much money should be put into different forms of care or treatment. Not only does this raise issues about justice and equity, it also poses the huge dilemma about who decides the priorities for investment. Public views may be very different from those of doctors. For example, infertility treatment may have a high value to individuals but not to society as a whole. Osteoporosis screening (bone density measurement) may be rated highly by the public but not by doctors who have access to more information and are therefore able to question its effectiveness.
While the ‘postcode lottery’ of accessing drugs such as Herceptin on the NHS is frequently highlighted, there are also considerable variations in spending by primary care trusts (PCTs). This is only partly explained by the age and needs of the population and the local cost of services. For example, Islington PCT in inner-city London spends four times as much as Bracknell PCT on the outskirts of London on mental health, even after adjustment for needs (Kings Fund 2006).
In Oregon in the USA a health commission of health care workers and the public devised a complex formula to prioritize health services and decided there were certain services that they would not provide (www.oregonhealthdecisions.org/index.htm#welcome). In the UK health care may no longer be free and available to all who need it. PCTs are beginning to consider particular services which will not be provided as part of the NHS. Cosmetic surgery, for example, is not provided free for cosmetic reasons alone, but may be allowed for the correction of congenital abnormalities and injuries and other special criteria determined by PCTs locally. Many primary care organizations elicit public views on health care priorities and changing provision to primary care, day-case surgery and the care of the mentally ill in the community.
PCTs have limited resources. Consider the following typical costs of interventions (not actual amounts). What factors would you take into account in deciding priorities?
| Home visit by community psychiatric nurse | £50 |
| Tonsillectomy | £250 |
| Hip replacement | £1000 |
| Place in group home for someone with learning difficulties | £30 000 per year |
| Pregnancy termination | £200 |
| Brief intervention of psychotherapy (10 weeks) | £1500 |
| Day care for an older person with mental ill health | £200 per week |
Some of the factors you might take into account are:
Health needs assessment
Needs assessment can be carried out from the perspectives of professionals, the lay public and key informants (members of the community with a particular viewpoint, such as teachers or police officers). It can be carried out at different levels from that of the individual to specific groups (e.g. population groups, such as older people or people with specific health problems) to local geographic communities to national populations. It can inform general practice profiles, community profiles, intervention planning or service design.
Wright (1998) describes three approaches to health needs assessment:
In all cases health needs assessment is a systematic and explicit process identifying issues affecting a population that can be addressed.
Health needs assessment should be guided by these common questions:
What information is needed?
The first step in a needs assessment is to define the relevant population group or community, including its demographic and social characteristics; behaviours, values and lifestyles; cultural environment and historical circumstances. Community nurses are often involved in compiling community profiles to identify the health of a community and what resources are needed to enable the community to achieve health and stay healthy. A community profile has been described as:
A comprehensive description of the needs of a population that is defined, or defines itself, as a community, and the resources that exist within a community, carried out with the active involvement of the community itself, for the purpose of developing an action plan or other means of improving the quality of life in the community (Hawtin & Percy Smith 2007, p. 5).
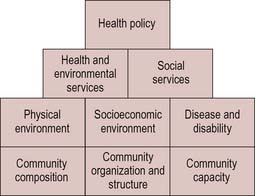
Community profiles do not follow a standard format. Figure 18.4 shows a schematic representation of the main elements:
For each of these elements, list the main sources of information that would need to be accessed to complete a community profile. What are the strengths and limitations of each information source in providing a picture of the community?
Information that is required for planning will include indicators of the state of health and well-being of the population, the factors that determine or influence health and the capacity of the population to meet identified needs. Some of this information is routinely collected and already exists, some will be known by stakeholders (e.g. health professionals, policy-makers, key members of the community) and the community members themselves will have views on what their needs are and how they wish them to be met. Chapter 3 outlined some of the indicators of health status and where this information is available, including:
Gathering information
Routine information that is already available (e.g. census, NHS and local authority data) will give a picture of the potential needs of a community and what is available to meet those needs. It may give an idea of areas of unmet need and identify groups experiencing inequities of health care provision. Information on effective interventions is also available (see Chapter 20). The community’s perceptions of its own health needs and expectations of services or interventions are a vital part of planning, as are the views of professionals about the nature of health needs, best practices and existing service delivery.
The NHS reforms of the 1990s emphasized the need to involve local people in the shaping of local services. Our companion volume (Naidoo & Wills 2005) discusses this shift to patient and public involvement. There are many reasons for this:
The gathering of community knowledge can take place in different ways. Chapter 10 discusses this in more detail. There may be a formal exercise of consultation conducted in a top-down way. Frequently the consultation is confined to issues relating to patient satisfaction with services and particularly the hotel aspects of care.
Ong & Humphris regard this as inadequate:
It is not sufficient to see users as consumers who are satisfied or dissatisfied with services. The place of users is in the joint definition of need, priority setting and evaluation. This approach means a paradigm shift whereby the community perspective will be used as the guiding principle for setting priorities in health care (Ong & Humphris 1994, p. 80).
Consultation in this way is not always successful. It often views people as the passive providers of information and not as active participants in the process. The results of consultations may seemingly be ignored. The timing, location and publicity for public meetings may lead to a poor turnout. Those consulted may not be representative of the community or may be token representatives of particular groups.
Many health and local authorities are using a range of methods to achieve a wider picture of community needs than one-off consultations. These approaches represent a move away from traditional epidemiological data-gathering towards techniques which reflect the importance of social and environmental factors and the involvement of the community in data collection. These include:
Rapid appraisal is a research technique applied to both urban and rural settings. It is geared to quickly identifying the health needs and priorities of a target population without great expense. It uses secondary data already available and then researchers interview people with knowledge of the area to identify problems and solutions. Key informants are:
List some of the advantages and disadvantages of rapid appraisal as a method of community needs assessment.
Rapid appraisal is useful if virtually nothing is known about the needs and priorities of the target population. It can give a deep understanding of the problems and issues in a community and provide a sense of local ownership. But it does not provide the quantitative analysis of the size of the problem which many public health departments require. It may also be difficult to get beyond personal agendas to find out the community’s views.
Participatory appraisal uses members of the community as data-gatherers. A range of methods may be used to capture the ways in which people describe local issues, e.g. mapping, community walks, timelines, photography, life histories. These techniques focus on mapping community assets and resources.
Whose needs count?
Moves to participation either in community affairs or health care cannot involve everyone. There will be individuals and groups who are not able to take advantage of opportunities for expression. These include potential and future users of a service; those who are not part of an established group; and those who are not deemed sufficiently rational to have a view, e.g. children, people with mental ill health and people with learning difficulties. Participation obviously favours those with the most influence and loudest voices.
It is very difficult to get a cross-section of a community and there are some groups of people who are harder to reach. These include homeless people, unemployed people and people from Black and minority ethnic groups. Some groups comprise individuals who may have a similar experience of health services because of a defining characteristic of being unemployed or homeless, but who do not have a collective voice or means of expressing their views. Other groups may be informal with no recognized meeting place. Many groups may be wary of formal and statutory bodies.
Setting priorities
Within the NHS the criteria used for setting priority areas are:
In addition, there may be locally determined priorities of specific health issues, such as diabetes, or particular population groups, such as older people.
We have seen in this chapter that people’s identified needs may also be taken as the first step in the planning process. However, this subjective interpretation may be tempered by economic priorities. People may express a need for interventions or treatment, the effectiveness of which is in doubt, e.g. antibiotics for simple colds or ear infections. For health promoters, therefore, a simple needs assessment may not be an adequate basis for setting priorities. There is a range of other influences which may determine what is included in a local health promotion plan:
Questions to ask when planning a needs assessment: guide for practitioners
Conclusion
There are many ways of measuring needs and no consensus as to the best method. The selection of a method or methods to measure needs will depend on the purpose and context. The process of encouraging consumerism and participation in public services by identifying and understanding individual and community needs has led to attempts to make such services more flexible. So we find, as part of the nursing process, clients being encouraged to identify aspects of their situation that they deem harmful to their health. We find health organizations using a variety of methods to ascertain the views, beliefs and health behaviours of their population in addition to the objective measures yielded by epidemiology. We find voluntary and community groups being required as part of their funding to monitor not only their clients’ use of the service but also their health needs.
The public sector, including the NHS, is seeking to integrate public views into the planning process. However, most of the information used to assess needs is gathered from a professional perspective which assumes a direct relationship between certain indicators and needs and which is embedded in a medical model of health. For example, if health statistics show an above-average incidence of coronary heart disease, local health planners may well assume a need for greater provision of cardiac treatment and rehabilitation services and a health promotion programme to address risk factors for coronary heart disease. Health promoters have an important role to play in ensuring that needs assessment which feeds into planning takes account of public views and self-defined needs, and uses indicators to measure a social model of positive health.
For those with client caseloads, it is a vital task to know the health status of patients/clients and how this may differ from the broader community in order to plan appropriate interventions.
Assessing health need is important then both in terms of promoting health and in determining priorities. For health promoters the process of identifying needs is not however the only basis for setting priorities. Resource constraints will limit what is available and what is deemed amenable to change. Professional views, practice wisdom and existing activity will provide boundaries to what is considered possible.