Chapter 15 Enterobacteria
Most of the commensal Gram-negative rods that inhabit the normal gastrointestinal tract, and sometimes cause disease, belong to the family Enterobacteriaceae. All species belonging to this family are Gram-negative, facultative anaerobes that ferment glucose. The major medically important species are listed in Table 15.1.
Table 15.1 Enterobacteria commonly causing human disease
| Genus | Representative species (no. of species) | Disease |
|---|---|---|
| Escherichia | E. coli (5) | Gastroenteritis, wound and urinary tract infection |
| Shigella | S. dysenteriae | Dysentery |
| S. flexneri | ||
| S. boydii | ||
| S. sonnei | ||
| Salmonella | S. typhi | Enteric fever (typhoid) |
| S. typhimurium (7 subgroups) | Food poisoning | |
| Klebsiella | K. pneumoniae (7) | |
| Morganella | M. morganii (2) | Urinary tract infection and other types of sepsis |
| Proteus | P. mirabilis (4) | |
| Providencia | P. stuartii (5) | |
| Yersinia | Y. pestis (11) | Plague, septicaemia, enteritis, etc. |
| Citrobacter | C. freundii (4) | Low pathogenicity, opportunistic infections |
| Enterobacter | E. cloacae (13) | |
| Serratia | S. marcescens (10) |
General characteristics of enterobacteria
Habitat
Found in the human gut, at a density of approximately 109 cells per gram of faeces. However, the predominant species in the gut is Bacteroides. Up to 15% of the population may harbour enterobacteria in the oral cavity, mostly as transient commensals. Their oral carriage rate may increase in old age, and in states leading to reduced salivary flow (xerostomia).
Characteristics
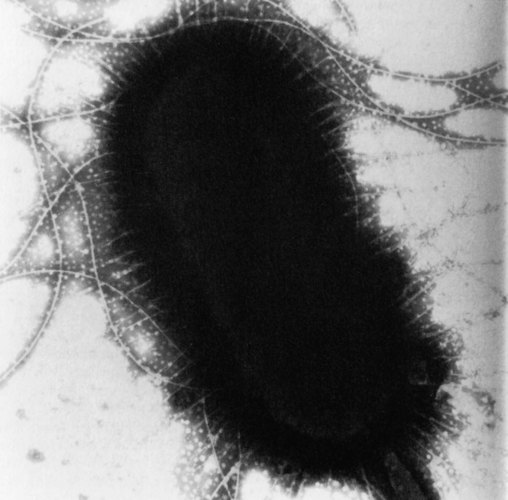
Rapidly growing cells 2 × 0.4 µm in size; may appear coccobacillary. Many species are motile and possess a capsule, especially on initial isolation. All species are endotoxigenic because of the lipopolysaccharide outer cell wall. They also possess pili and flagella, which mediate adhesion and locomotion, respectively (Fig. 15.1).
Culture and identification
Grow well on ordinary media (e.g. blood agar, MacConkey’s agar), producing characteristic circular, convex and glistening/mucoid colonies. Some motile species form swarming patterns on agar cultures. Most species are non-pigmented; a few produce red, pink, yellow or blue pigments.
Enterobacteriaceae ferment a large number of carbohydrates. This property, together with other biochemical tests, is used to identify and differentiate species.
Lactose fermentation
Growth on indicator media is used for the initial categorization of Enterobacteriaceae into two groups: lactose fermenters and lactose non-fermenters. Several selective media, such as MacConkey’s and cystine-lactose-electrolyte-deficient (CLED) media, are available for this purpose. On MacConkey’s agar, the lactose fermenters appear as pink colonies, while on CLED medium, the colour of lactose fermentation is yellow.
Other biochemical tests
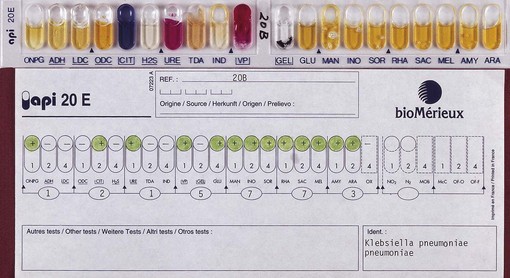
Commercially available kit systems are routinely used to identify species of enterobacteria. The commonly available test systems are based on 10 (API 10E) or 20 (API 20E, Rapid E) biochemical tests (Fig. 15.2).
Serological tests
These are based on the antigens of the organisms. All species have the somatic (O) antigen, and most have the flagellar (H) antigen. The capsular (K) antigen is seen in some species. The antigens are useful in the classification of species and invaluable for epidemiological investigation of outbreaks of disease. Identification of strains within a species can also be done by bacteriophage typing, bacteriocin typing, plasmid analysis and polypeptide analysis.
Pathogenicity
All Enterobacteriaceae are potentially pathogenic. Patients who are immunosuppressed, undergoing mechanical or medical manipulation, and have underlying disease are most susceptible to infection.
Endotoxin shock
This can be precipitated in humans by the lipopolysaccharide, which all Enterobacteriaceae release when they are destroyed. Toxic lipopolysaccharide comprises lipid A, the core polysaccharide and the O antigen; the lipid A is responsible for most of the symptoms associated with endotoxic shock. The toxic effects of lipopolysaccharide are many and include fever, hypotension, intravascular coagulation and effects on the immune system. Large doses of endotoxin may cause death.
Eschericheae
The tribe Eschericheae includes five genera: Escherichia, Salmonella, Shigella, Edwardsiella and Citrobacter. The most important human pathogens in this group, Escherichia coli and the Salmonella and Shigella species, are described here.
Escherichia coli
Habitat and transmission
Indigenous commensal of the human intestinal tract; transmission is either endogenous or exogenous.
Characteristics
Gram-negative rods, motile, sometimes capsulate, facultative anaerobe, bile-tolerant.
Culture and identification
Grows well on blood agar; ferments lactose (hence pink colonies on MacConkey’s agar and yellow on CLED agar). Commercial kits, such as API 20E, are used in identification (Fig. 15.2). Biotyping systems are useful for strain delineation.
Pathogenicity
E. coli is a major agent of sepsis; it causes the following diseases.
Urinary tract infection
Young women and elderly adults are the most susceptible. The disease varies from simple urethritis to serious pyelonephritis.
Diarrhoeal diseases
These range from simple diarrhoea to severe disease leading to excessive fluid loss and dehydration, which may be fatal in malnourished infants and elderly debilitated adults. Many strains of enteropathogenic E. coli have powerful toxins and other mechanisms by which they cause diarrhoea:
Based on the above, diarrhoea-producing E. coli can be divided into five types:
Salmonellae
The genus Salmonella has a bewildering spectrum of more than 2000 species living in the intestinal tract of humans, domesticated animals and poultry. Salmonella typhi and Salmonella paratyphi differ from others in that humans are the only known natural host.
Salmonella spp.
Habitat and transmission
Leading sources of salmonella infection are poultry products (i.e. flesh and eggs) and pet turtles (in the USA). Occupational salmonellosis affects veterinary and slaughterhouse workers. Infection is by ingestion of contaminated food, or person-to-person via the faecal–oral route. The carrier state, which develops in some after infection, is an important source of organisms.
Characteristics
Gram-negative, motile, non-sporing rods. All except S. typhi are non-capsulate; facultative anaerobes.
Culture and identification
Culture on MacConkey’s medium or desoxycholate-citrate agar yields non-lactose-fermenting colonies. A combination of biochemical tests and serotyping is required for full identification. The latter is complex as salmonellae have a variety of antigens; notable are the O (somatic) and the H (flagellar) antigens; virulent strains, notably S. typhi, have a capsular polysaccharide antigen designated the Vi (virulence) antigen. There are more than 1700 serotypes of Salmonella enteritidis.
Pathogenicity
The major types of salmonellosis (diseases due to Salmonella) are enteric fever, gastroenteritis and septicaemia.
Shigellae
Shigella species cause bacillary dysentery. The genus is divided into four species (Shigella dysenteriae, Shigella sonnei, Shigella flexneri and Shigella boydii) and a variety of serotypes.
Shigella spp.
Habitat and transmission
The only reservoir is the human intestine. Infection is spread by the faecal–oral route under crowded conditions. A minute dose of the organisms is adequate to cause disease.
Culture and identification
All species grow well on ordinary media and are non-lactose fermenters (except S. sonnei, a slow lactose fermenter). Commercial kits are used in identification.
Pathogenicity
Although shigellae do not invade systemically like salmonellae, they locally invade the intestinal epithelium (ileum and colon). The resultant intense inflammatory response is characterized by bloody, mucopurulent diarrhoea (dysentery). Although no enterotoxin is produced, the exotoxin of Shigella species is neurotoxic.
Treatment and prevention
Severe dysentery is managed by fluid and electrolyte replacement. Antibiotics should be avoided as many strains are resistant to multiple antibiotics. Spread can be controlled by improving sanitation and personal hygiene to interrupt faecal–oral transmission; hand hygiene is critical.
Klebsielleae
A number of species belonging to this tribe, namely Klebsiella, Enterobacter and Serratia, are indigenous to the human intestinal and respiratory tracts. They are also occasionally isolated from the oral cavity and hence are considered transient oral commensals. They cause serious disease in immunocompromised patients, especially in hospital environments (nosocomial infection).
Klebsiella pneumoniae
As the name indicates, Klebsiella pneumoniae may sometimes cause a severe destructive pneumonia. It also causes nosocomial urinary tract infection. The virulence of the organism is mainly due to its large antiphagocytic capsule. This species is isolated from the oropharynx or gastrointestinal tract of about 5% of healthy people, and the isolation rate is higher in the hospitalized.
Enterobacter spp.
Enterobacter species are indigenous to the intestinal tract but can be found on plants and as free-living saprophytes. They may cause nosocomial urinary tract infection and very rarely a primary infection. Enterobacter cloacae and Enterobacter aerogenes are the most frequently isolated as transients in the oral cavity.
Pseudomonads
Pseudomonas species are not enterobacteria, but they are included in this chapter for convenience as they are Gram-negative rods with somewhat similar properties. The genus contains a large number of species, but only a few are human pathogens. They are widely distributed in the environment and may cause disease, especially in hospital settings. Pseudomonas aeruginosa is the most important species to cause such infection and is a special problem in burns patients.
Pseudomonas aeruginosa
Habitat and transmission
Colonizes the human intestine in a few healthy individuals and in a large proportion of hospitalized patients. Colonizes environmental surfaces, especially under moist conditions. Thus, they are found in dental unit water lines, as harmless saprophytes.
Characteristics
Aerobic, Gram-negative rods, motile by means of polar flagella. Grow over a very wide temperature range, including room temperature.
Culture and identification
Grows easily on routine media, producing irregular, moist, iridescent colonies with a characteristic ‘fishy’ aroma. Identified using commercial kits.
Pathogenicity
Virulence factors identified include lipopolysaccharide endotoxin, an exotoxin, extracellular proteases and elastases, and an extracellular ‘slime’ that prevents phagocytosis.
Treatment and prevention
Although this species is resistant to most antimicrobials, it is sensitive to aminoglycosides and certain β-lactams (e.g. acylureidopenicillins), cephalosporins and polymixin. Prevention is by good asepsis in hospitals and rational antibiotic therapy (to prevent emergence of resistant isolates).
Key facts